

Abstract
Background
Upper arm development in children is different in different ethnic groups. There have been few reports on upper arm circumference (UAC) at different stages of development in children and adolescents in China. The purpose of this study was to provide a reference for growth with weighted assessment of the overall level of development.
Methods
Using a pooled analysis, an authoritative journal database search and reports of UAC, we created a new database on developmental measures in children. In conducting a weighted analysis, we compared reference values for 0~60 months of development according to the World Health Organization (WHO) statistics considering gender and nationality and used Z values as interval values for the second sampling to obtain an exponential smooth curve to analyze the mean, standard deviation, and sites of attachment.
Results
Ten articles were included in the pooled analysis, and these articles included participants from different areas of China. The point of intersection with the WHO curve was 3.5 years with higher values at earlier ages and lower values at older ages. Boys curve was steeper after puberty. The curves in the studies had a merged line compatible. The Z values of exponential smoothing showed the curves were similar for body weight and had a right normal distribution.
Conclusions
The integrated index of UAC in Chinese children and adolescents indicated slightly variations with regions. Exponential curve smoothing was suitable for assessment at different developmental stages.
Keywords: Upper arm circumference, Chinese children and adolescents, Pooled analysis
Introduction
Upper arm circumference (UAC) assessment reflects comprehensive growth in children, such as growth of skeleton, muscles, and subcutaneous fat, which has been used as an alternative indicator of nutritional status if collection of height and weight measurements was difficult. Previous Chinese reports have concentrated on assessment during the 2000s, and these reports mainly focused on malnutrition in children [1].
There are some differences in UAC among different racial or ethnic groups: the general population and athletes or people who do physical labor for a living. Adult muscle strength in the African, European, and Asian populations are different, with Asians being slightly inferior in terms of UAC. There are also some differences among ethnic groups. According to the anthropological human body physique study performed by the Chinese National Natural Foundation [2–5], clustering analysis showed that the male Han Chinese urban and rural area populations in Jiangsu, Uzbeks, Russians, Kazaks, and 10 other northern ethnic groups had a UAC that was about 28 cm, which would be considered as medium dimensions. The average mean of other groups were 30 to 24 cm for the highest to lowest UAC. Women had a lower average about 2 cm both medial and other groups.
Although there are these differences in adults, as well as the uncertainty of muscle development rates in youngsters [6], WHO study was revised UAC by age and gender from 0 to 60 months (http://www.who.int/childgrowth). A pooled analysis of populations in Norway, Brazil, Hong Kong, and a total of seven other nationalities was carried out based on growth. Little obvious differences during the period that was studied were found, and this study is considered the representative reference.
National data on children’s growth and development was also published by the Chinese Public Health Ministry, and the data were mainly about height, weight, and head circumference by age and gender, but the study did not clarify UAC. Searching the published data to date, articles have mainly described results of region’s survey. It is therefore necessary to carry out a pooled analysis to determine the UAC growth conditions of children and adolescents in Chinese population, which is one fourth of the world’s population.
Methods
Data sources
A search was carried out for articles published in journals such as the Wanfangdata and Tsinghua-Tongfang using the keywords “upper arm circumference” to identify published or dissertations on UAC measurements. Hundreds of articles were considered, and ten of them included measurement values for UAC. The articles included participants in various regions of China, which involved Capital Beijing and central, northeast, southeast, northwest, and southwest provinces and cities in China. The UAC measurements in these articles were all the same to the pediatric measuring method generally used as the attachment of halfway point of the acromion to olecranon as a measurement point. Age groups in the studies varied (Table 1). Data were extracted and entered into an Excel database and were then analyzed with SPSS16.
Table 1.
The 10 articles included in the pooled analysis
| Order | Sitting | Areas of China | Data collection | Age(interval) | N (total) | N (boys) | N (girls) | Presentation | Method of measurements | Relative measuring |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | BJ | Capital Beijing | Cluster sampling in schools and kindergartens in urban and suburban | 3–18 years (1 year) | 19,705 | 10,151 | 9554 | Dissertation 2009 | Mid-upper arm circumference | Height, weight |
| 2 | SX(U,R) | Yangquan city of Shanxi province of central north | Hierarchy cluster sampling in 101 survey sets | 0–5 years (0–6 months (1 months), 6–12 months (2 months), 1–2 years (3 months), 3–5 years (6 months)) | 6334 | 3262 | 3072 | Pan 2011 | Mid-upper arm circumference | Height, weight, circumference of chest and head |
| 3 | AH | Anhui province of central south | Random cluster sampling in 3 elementary schools and 2 junior high schools | 6–17 years (2 years) | 4476 | 2275 | 2201 | Jiang 2002 | Mid-upper arm circumference | Height, weight, circumference of chest, triceps skin-fold thickness |
| 4 | SZ | Suzhou city in Jiangsu province in Yangtze north | Cluster sampling in kindergartens | 3–6 years (1 years) | 1061 | 577 | 484 | Liu 1988 | Mid-upper arm circumference | Height, weight |
| 5 | ZJ | Zhejiang province in Yangtze south | Random sampling 1–3grade in 16 elementary schools | 6–10 years (1 years) | 1515 | 843 | 672 | Tan 2004 | Mid-upper arm circumference | Height, weight |
| 6 | IM | Hohhot city of Inner Mongolia of Northwest | Random sampling in 10 kindergartens | 3–7 years (6 months) | 3662 | 1936 | 1726 | Wuyunrle 2000 | Mid-upper arm circumference | Nine circumferences of chest, head, waist, and so on |
| 7 | LN | Dalian city of Liaoning province of Northeast | Random sampling | 7–17 years (1 years) | 1203 | 594 | 609 | Xu 2000 | Mid-upper arm circumference in Shao’s version | Four circumferences of chest, hip, minimum-waist, maximum-leg |
| 8 | GX(Miao) | Miao nationality in Guangxi municipality in Southwest | Miao nationality sampling | 8–16 years (1 years) | 814 | 454 | 360 | Huang 2005 | Mid-upper arm circumference in Wu Rukang’s version | Height, weight, skin-fold thickness, body fat |
| 9 | GX(Zhuang) | Zhuang nationality municipality of Guangxi of Southwest | Random sampling in 21 schools in 4 counties in 2 cities | 7–18 years (1 years) | 12,339 | 6825 | 5514 | Tan 1994 | Mid-upper arm circumference | Height, weight |
| 10 | GD | Guangzhou city of Guangdong province of Southeast | 2 hierarchy cluster sampling in 10 kindergartens | 4–8 years (1 years) | 9108 | 4780 | 4328 | Su 2003 | Mid-upper arm circumference | Height, weight, skin-fold thickness |
Data processing
UAC data were summarized and weighted by age and gender. Z values were calculated and the mean and standard deviations were determined. Weighted smoothing of the curves was carried out after the means were connected. According to age and gender, the median average was Z = 0 ( Z > = −1 and Z < =1); Z = −1 (Z < −1 and Z > = − 2); Z = −2 (Z > −2 and Z < = −3); Z = −3 (Z > −3 and Z > = − 4); Z = 1 (Z > 1 and Z < = 2); Z = 2 (Z > 2 and Z < =3); and Z = 3 (Z > 3 and Z < =4). To calculate the mean and standard deviation with the Z value intervals, we obtained a smooth curve with exponential smoothing.
Data analysis
The Chinese weighted values and the WHO data released online in 2006 (0- to 60-month-old children) were analyzed. Data, those compared and merged with growth curves by gender, were included. The Z values and exponential smoothing curve points were determined.
Results
Multicenter data distribution
Ten articles were included in the pooled analysis and participants from the northeast (DL), northwest (IM), southeast (GD), southwest (GX), the central plains (SX), central south (AH), and southwest (GD), and Yangtze areas (SZ and ZJ) of China, as well as Capital Beijing. The data on central Yangquan, Shanxi province, covered ages from 0 months to 4.5 years old and included both urban and rural children. Other multicenter reports based on a wide geographic distribution were representative of the general population and covered children who were 0~18 years old (Table 1) [7–15].
Weighted comparison with the WHO study by gender
By gender, the weighted mean compared with the WHO study had a similar cross point at 3.5 years old. Differences with the WHO study were not obvious for boys and girls (Figs. 1 and 2).
Fig. 1.
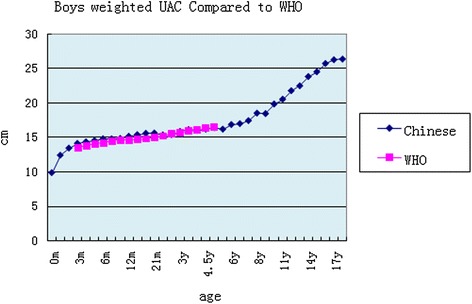
Boys weighted UAC compared to the WHO study
Fig. 2.
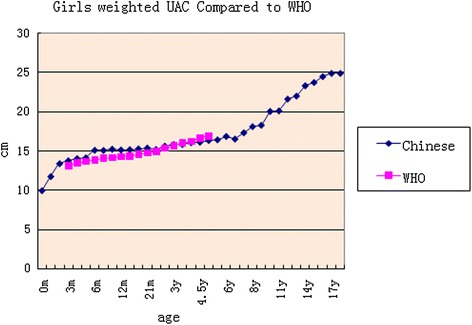
Girls weighted UAC compared to the WHO study
UAC weighted curves comparisons by gender
There were subtle differences in gender before puberty and more differences after puberty. The curve for boys was steeper (Fig. 3). Within each UAC curve chart, age groups cross-covered each other. The weighted curve integrated the studies smoothly, which had the possibility to add the Z score loci on it excluding 0–2 years (Figs. 4 and 5).
Fig. 3.
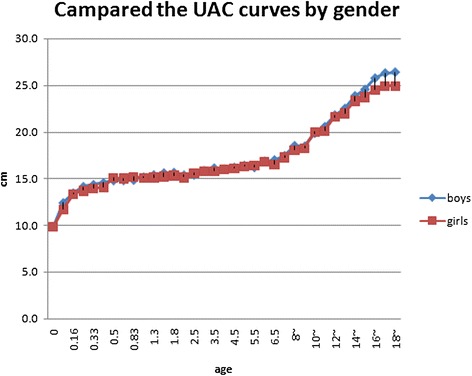
Compared UAC merged curves by Gender
Fig. 4.
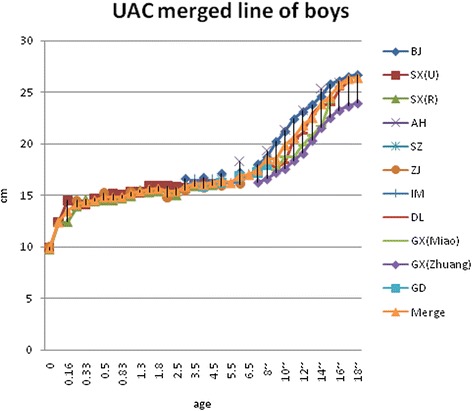
UAC curves comparing with boys
Fig. 5.
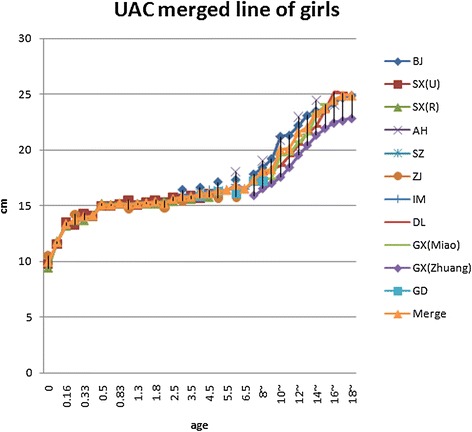
UAC curves comparing with girls
Curve smoothing
The pooled analysis of the studies from the literature showed some regularities in Z scores for each locus, with boys and girls showing similar variation. After puberty, the values for boys were higher than for girls in the exponential smoothed curve (Table 2 and Figs. 6 and 7).
Table 2.
The equations for Z score loci by gender
| Girls | Boys |
|---|---|
| Y 0 = 15.508e0.0321X R 2 = 0.9703 | Y 0 = 15.428e0.0361X R 2 = 0.9637 |
| Y + 3 = 22.786e0.0349X R 2 = 0.8277 | Y + 3 = 23.293e0.0402X R 2 = 0.8389 |
| Y + 2 = 20.447e0.0341X R 2 = 0.8883 | Y + 2 = 21.089e0.0384X R 2 = 0.8704 |
| Y + 1 = 18.491e0.0332X R 2 = 0.9263 | Y + 1 = 18.777e0.0383X R 2 = 0.8965 |
| Y − 1 = 13.458e0.0294X R 2 = 0.9563 | Y − 1 = 13.235e0.0337X R 2 = 0.8437 |
| Y − 2 = 12.724e0.0235X R 2 = 0.9178 | Y − 2 = 11.136e0.0337X R 2 = 0.8546 |
Fig. 6.
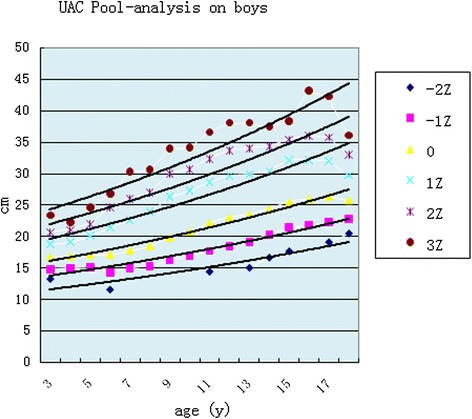
Pooled analysis for boys
Fig. 7.
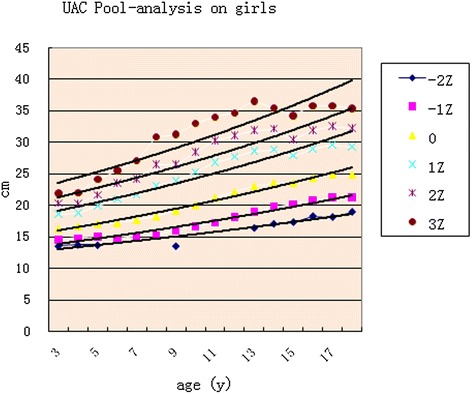
Pooled analysis for girls
Discussion
Comparison with the WHO study
The age phases of the pooled analysis were broad; 0 to 60 months range was compared in the WHO study [6]. In our study, the weighted age boundary segmentation was the following: cutoff 1 month before a half year of age, 2 months after a half year old, 3 months at 2 years old, 6 months within 2–6 years of age, and 1 year during the range 7 to 18 years old. The comparison of results showed that there was some crossover with the curve of the WHO study but with the first segment showing values that a few above and then below the WHO study curve with a node located at 3.5 years. The reason may be that the curve of WHO study was obtained with exponential smoothing (http://www.who.int/nutrition/media_page). Many studies in the developing countries compared children’s UAC to WHO references as well. Reports have shown that a ROC curve can be used for evaluation of malnutrition in children under the age of five and UAC by age has better sensitivity than height in Kenya, Africa [16]. There were 26.8 % of children below 2 standard deviations from the mean in a study on children in Malaysia, Asia [17]. Nevertheless, some results implied that the use of the international reference may lead to lower specificity and predictive value in the screening of malnourished children in developing countries such as Uganda [18]. The average of children under 5 years old was at −2 standard deviations from the mean in a study carried out in Kenya [19]. Therefore, that seems to need a local UAC curve for references.
Chinese children UAC curves integration
There were significant differences in adult UAC in China, because China is a large region and includes many nationalities. The Male Xinjiang Khalkhas, Tatar, and Xibo populations had a UAC of about 30 cm, which would be considered as brawnier. Ten southern ethnic groups, i.e., Hainan Han, Hui, Miao, DuLongZu, MuLaoZu, Buyi, Uighur, Tu, Mongolian, and Li had a UAC of about 24~25 cm, which would be considered as smaller. Women were divided into four types, and the strongest groups, in addition to the three of the male groups and ethnic Russians, had a UAC of about 28 cm. The Han, Uzbek, and Kazak urban and rural area populations in Jiangsu had a UAC of about 26 cm. Uely had a below average UAC of about 23~24 cm. The Hui, Soil, and Mongolian populations had a UAC of about 22~23 cm, which would be considered as thin [2–5, 20]. Asian children had less UAC than Caucasians [21]. In the present study, Children UAC development showed some differences in different regions, but the mean gaps between the values of highest and lowest curve of each age groups were all less than the standard deviation of their own study, although those were narrow before puberty and wider in adolescence (Figs. 4 and 5). The charts of the curves showed the merged curve was feasible made by combined studies, and the ligature of weighted mean UAC of age phases is also thought as the mean value of the reference curve. The Z score values could be added as well.
Growth curve for each Z score
Many studies have supported the superiority of Z scores for UAC by age. Use of UAC with age- and sex- adjusted Z scores gave a better sensitivity than absolute cut of values in the identification of children wasting (acute undernutrition) [22–24]. Furthermore, regarding preschool obesity screening, the Z score of UAC by age seemed to be an appropriate alternative, which was better than UAC by height [25]. In addition, Z scores for other anthropometric indicators such as weight have showed symmetry if cut small in the right tail with Z score analysis [26]. UAC Z scores in this pooled analysis showed a normal distribution, similar to the curve for weight, which was a −2~+ 3 right normal curve. The index-smoothing trend showed some regularities with directions going up and down through various points in each Z trend. The development chart can be a representative reference for Chinese children and adolescents.
Conclusion
The pooled analysis on UAC data for Chinese children and adolescents had a broad weighted value. The age group 0~60 months compared with the WHO curve showed there was some crossover with a little higher values for children younger than 3.5 years old and lower values for children older than 3.5 years old. Z scores ranged from −2 to ~3 and formed a normal distribution. Exponential smoothing was suitable for assessment.
The research has been approved by Ethics Committee of the Capital Institute of Pediatrics, within which the work was undertaken and that it conforms to the provisions of the Declaration of Helsinki.
Acknowledgements
We thank Professor Lianbin Zheng, from Tianjin Normal University, who gave the good suggestions. We also thank Professor Ting Zhang, and Long Li from the Capital Institute of Beijing, China, who partly supported this article publication. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Abbreviations
- UAC
mid-upper arm circumference
- ROC
receiver operating characteristic curve
- WHO
Would Health Organization
- CDC
Center for Disease Control and Prevention
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
This paper was conceived, designed, and written by FT. FT and TF analyzed the data. TF contributed analysis tools. Both authors read and approved the final manuscript.
Contributor Information
Fang Tong, Email: tongfang371@163.com.
Tong Fu, Email: eros0602@vip.qq.com.
References
- 1.Duggan MB. Anthropometry as a tool for measuring malnutrition: impact of the new WHO growth standards and reference. Ann Trop Paediatr. 2010;30(1):1–17. doi: 10.1179/146532810X12637745451834. [DOI] [PubMed] [Google Scholar]
- 2.Zhang XR, Zheng LB, Yu KL, Xue H, Wang Y, Rong WG, et al. Circumference and its variation with age of Jiangsu Han nationality adults. J Tianjin Normal Univ (Nature Science Edition). 2011;31(4):74–81. [Google Scholar]
- 3.Xu BS, Zheng LB, Lu SH, Luo DM. The circumfenrence and its variation with Age changes of the adults of dulong nationality. J Tianjin Normal Univ (Nature Science Edition). 2008;28(1):19–25. [Google Scholar]
- 4.Xie B, Lu SH, Zheng LB, Suo LY. Analysis of bodily circumference characteristics of Russ adults in inner Mongolia. Chin J Anatomy. 2007;30(4):483–7. [Google Scholar]
- 5.Li SY, Zheng LB. The variation of circumference values of Uzbek adults. J Tianjin Normal Univ. 2006;26(3):15–20. [Google Scholar]
- 6.Onis MD, Yip R, Mei Z. The development of MUAC-for-age reference data recommended by a WHO Expert Committee. Bull World Health Organ. 1997;75(1):11–8. [PMC free article] [PubMed] [Google Scholar]
- 7.Xu F, Zhao W, Ma XK. Study on development of body growth of Dalian Han nationality students. Chin J Anatomy. 2000;23(5):479–82. [Google Scholar]
- 8.Huang XF, Li LZ, Wu YY, Wei QJ, Li ZHH. Study on skinfold of Guangxi Miao nationality students. Anat Res. 2005;27(2):141–3. [Google Scholar]
- 9.SuYX XXC. Evaluation of growth and development status of children aged 4–8 years in Guangzhou city. Chin J School Health Dec. 2003;24(6):598–9. [Google Scholar]
- 10.Jiang JH, Zhang JX, Gao YQ, Liu JP, Gao M. Growth indexes building of 6–17 children reference in Hefei city. Acta Univ Med. 2002;37(1):65–6. [Google Scholar]
- 11.Wuyungerle D, Temuqiletu G, Jin YC. Studies on present growth of 10 body parts circumference of children aged from 3 to 7 in huhhot. J Inner-Mongolia Normal Univ (Nature Science Edition). 2000;29(3):229–33. [Google Scholar]
- 12.Pan YQ, Li HY, Song ZHH, Li ZHY, Duan SHH, Ge JJ, et al. Study of growth and nutritional status of children aged 0–5 year in Yangquan city. Chin J Woman Child Health Res. 2011;22(6):723–7. [Google Scholar]
- 13.TanY ZJK, Ding BG, Liu HJ, Chang J, Fan DM. Assessment of children nutritional status with upper-arm circumference for height. Chin J Public Health Dec. 2004;20(12):1456–7. [Google Scholar]
- 14.Tan ChM LBH, Huang JP, Lu MY, Chen HH. To probe assessing the nutrition statues of the children and adolescent with upper-arm circumference. Chin J School Health. 1994;15(5):331–2. [Google Scholar]
- 15.Liu LM, Gu YM, Gu JZH, Bai HY, Zhang HS. To probe the nutrition statues of the preschool children with upper-arm circumference. Chinese academic J. Suzhou Med Univ. 1988;8(2):118–20. [Google Scholar]
- 16.Mei Z, Grummer-Strawn LM, de Onis M, Yip R. The development of a MUAC-for-height reference, including a comparison to other nutritional status screening indicators. Bull World Health Organ. 1997;75(04):333–41. [PMC free article] [PubMed] [Google Scholar]
- 17.Cheah WL, Wan Muda WA, Mohd Hussin ZA, Thon CC. Factors associated with undernutrition among children in a rural district of Kelantan, Malaysia. Asia-Pacific J Public Health Asia-Pacific Acad Consortium Public Health. 2010;XX(X):1–13. doi: 10.1177/1010539510380737. [DOI] [PubMed] [Google Scholar]
- 18.Cortinovis I, Vella V, Ndiku N, Milani S. Weight, height and arm circumference of children under 5 in the district of Mbarara, south-west Uganda. Ann Hum Biol. 1997;24(6):557–68. doi: 10.1080/03014469700005322. [DOI] [PubMed] [Google Scholar]
- 19.Vonk R. Growth of under five-year-old children in Kyeni, Kenya. Trop Geogr Med. 1993;45(4):175–8. [PubMed] [Google Scholar]
- 20.Xuehereti L, Polat Y. An investigation of the subcutaneous fat thickness of Uygur, Kazak, Han and Hui children in Urumqi city. J Xinjiang Med Univ. 2003;26(3):265–9. [Google Scholar]
- 21.Yu S, Huang ZJ, Singh CK. Health status and health services utilization among US Chinese, Asian Indian, Filipino, and other Asian/Pacific Islander children. Pediatrics. 2004;113(1):101–7. doi: 10.1542/peds.113.1.101. [DOI] [PubMed] [Google Scholar]
- 22.Gernaat HB, Dechering WH, Voorhoeve HW. Absolute values or Z scores of mid-upper arm circumference to identify wasting? Evaluation in a community as well as a clinical sample of under fives from Nchelenge, Zambia. J Trop Pediatr. 1996;42(1):27–33. doi: 10.1093/tropej/42.1.27. [DOI] [PubMed] [Google Scholar]
- 23.Gewa CA, Oguttu M, Yandell NS. Maternal nutrition in rural Kenya: health and socio-demographic determinants and its association with child nutrition. Maternal Child Nutr. 2011;5:1–12. doi: 10.1111/j.1740-8709.2011.00322.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ghosh A, Dutta R, Sarkar A. Heritability estimation of conventional cardiovascular disease risk factors in Asian Indian families: The Calcutta family study. Indian J Hum Gene. 2010;16(01):28–32. doi: 10.4103/0971-6866.64944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.de Almeida CA, Del Ciampo LA, Ricco RG, Silva SM, Naves RB, Pina JF. Assessment of mid-upper arm circumference as a method for obesity screening in preschool children. J Pediatr. 2003;79(5):455–60. doi: 10.2223/jped.1081. [DOI] [PubMed] [Google Scholar]
- 26.Tong F, Mi J, Yan SJ, Cheng H, Hou DQ, Zhao XY. Children growth assessment with Z-score in Beijing. Chin J Children Health Care. 2007;15(4):350–3. [Google Scholar]