

Abstract
Objective
Students with poor mental health are at increased risk for problematic alcohol use. These students also tend to underutilize alcohol-related protective behavioral strategies (PBS). Cross-sectional studies indicate that PBS use may be particularly useful for students with mental health challenges; however, it is unclear whether training these students to use PBS is an effective approach for reducing alcohol use and consequences. The current study evaluated the efficacy of a standalone PBS skills training and personalized feedback (PBS-STPF) intervention among students accessing mental health services.
Method
Participants (N = 251) were randomly assigned to either an individual facilitator-led PBS-STPF intervention or a health-related control condition. Participants completed online follow-up surveys 1- and 6-months post-intervention which included measures of alcohol use, negative consequences and a composite measure of PBS use.
Results
Relative to control participants, students in the PBS-STPF condition reported significantly greater PBS use, but no differences in alcohol use or consequences. Participants in both conditions reported decreases in drinking outcomes over time. Tests of mediation indicated that the intervention indirectly led to reduction in drinking outcomes at 6 months through increased PBS use.
Conclusions
Although the intervention resulted in changes in PBS use that were maintained for up to 6 months post-intervention, the effects of the intervention on drinking and consequences were limited. A brief standalone PBS training may need augmentation in order to promote effective use of PBS for substantial decreases in alcohol consequences.
Keywords: college drinking, protective behavioral strategies, brief intervention, mental health
Incidence of poor mental health and mental distress among U.S. college students has risen dramatically and is a significant concern on college campuses (American College Health Association, 2007; Center for the Study of Collegiate Mental Health, 2009; Erdur-Baker, Aberson, Barrow, & Draper, 2006; Gallagher, 2006). A recent national survey of 27,774 college students found that nearly one-third reported feeling so depressed that it caused functional impairment and one-half reported experiencing overwhelming anxiety in the past year (American College Health Association, 2011). Nationwide, college counseling center directors report increases in both the number of students seeking services for mental health issues as well as the severity and chronicity of the presenting problems (Erdur-Baker et al., 2006; Gallager, 2006). The academic and social stressors associated with college may be particularly challenging for students experiencing poor mental health and who are susceptible to co-occurring health risk behaviors, such as alcohol misuse.
Among colleges students, depression, anxiety, and general psychological distress are associated with increased alcohol-related problems (Camatta & Nagoshi, 1995; LaBrie, Kenney, & Lac, 2010; Litt, Lewis, Blayney, & Kaysen, 2013; Martens et al., 2008; Park & Grant, 2005; Weitzman, 2004) and alcohol use disorders (Dawson, Grant, Stinson, & Chou, 2005; Weitzman, 2004). Students with poorer mental health may be at heightened risk for negative consequences when they drink. This is likely the result of several factors including using alcohol to cope with negative affect, having lower drinking refusal self-efficacy, as well as enhanced salience of alcohol cues, and decreased awareness of alcohol-related risks (Ham & Hope, 2003; Kuntsche, Knibbe, Gmel, & Engels, 2005; Monti, Rohsenow, & Hutchison, 2000; Park, Armeli, & Tennen, 2004; Park & Grant, 2005; Simons, Gaher, Correia, Hansen, & Christopher, 2005). Rather than resolving problems, coping-motivated drinking is related to adverse alcohol-related outcomes, including the development of maladaptive drinking patterns (Britton, 2004; Cooper, Agocha, & Sheldon, 2000). Furthermore, students with poorer mental health may lack the volitional self-control and supportive social networks to mitigate potential consequences. Thus, there is a need to provide these students with skills and strategies to reduce risk when drinking. Despite the strong relationship between poor mental health and alcohol risk, surprisingly little research has examined strategies that may reduce alcohol misuse and harm among students experiencing mental health issues.
Recent cross-sectional studies have indicated that protective behavioral strategies (PBS; Martens et al., 2005; e.g., “avoid drinking games”, “stop drinking at a predetermined time”, “use a designated driver”) may be particularly effective at reducing alcohol-related harm for students with poorer mental health (LaBrie et al., 2010; LaBrie, Kenney, Lac, Garcia, & Ferraiolo, 2009). Among the general student population, PBS use is associated with less alcohol use and fewer negative alcohol-related consequences (American College Health Association, 2011; Araas & Adams, 2008; Martin et al., 2012; Patrick, Lee, & Larimer, 2011; Ray, Turrisi, Abar, & Peters, 2009). Although students with poorer mental health (e.g., depression, anxiety) are less likely to utilize PBS naturally (LaBrie et al., 2010; LaBrie et al., 2009), PBS use among these students is more strongly associated with fewer harmful consequences of drinking than for students without mental health challenges. Given that students with poorer mental health experience more alcohol-related consequences than their peers, even at comparable levels of alcohol consumption (LaBrie et al., 2010; LaBrie et al., 2009; Markman Geisner, Larimer, & Neighbors, 2004), and are less likely to naturally or spontaneously utilize PBS, training these students to use PBS may be particularly beneficial. To date, however, no studies have examined the efficacy of PBS interventions among heavy drinking college students who have poorer mental health.
Multi-component alcohol interventions that incorporate PBS skills training are effective at reducing alcohol related-harm among the general population of college students (Barnett, Murphy, Colby, & Monti, 2007; Larimer et al., 2007). Furthermore, changes in PBS use post-intervention appear to be an important mediator of intervention efficacy (Barnett et al., 2007; Larimer & Cronce, 2007; Murphy et al., 2012). Recently, Kenney et al. (in press) found that a brief group standalone PBS intervention was associated with increased PBS use and reductions in heavy drinking and alcohol consequences among first-year college women. Further, PBS emerged as a mediator of intervention efficacy on alcohol consequences post-intervention among participants exhibiting high levels of anxiety. Despite the overall promising effects of PBS skills training, other research indicates that standalone PBS interventions may not be sufficient to reduce alcohol use. For example, Sugarman and Carey (2009) found that instructing students to use more PBS increased strategy use, but did not reduce drinking. Further, a recent study by Martens et al. (2013) compared standalone PBS feedback (PBSF) to personalized normative feedback (PNF) and an alcohol education control condition among heavy drinking college students. Findings indicated that PBS use increased for up to 6 months post-intervention on one of two measures of PBS use. PBSF participants also reported within-persons decreases in drinks per week, peak BAC and consequences for up to 6-months post-intervention. However, the authors also note that shorter-term (e.g., 1-month) increases in PBS use were also found in the PNF condition, and reductions in alcohol use after PBS training were no different to those in the alcohol education control condition. Indeed, the PNF condition produced larger reductions in alcohol consumption than PBSF. The authors suggest that the limited effects of PBSF may reflect that the intervention did not specifically motivate changes in drinking and call for additional research examining the efficacy of single-component brief interventions. Finally, although this study sheds light on the use of a PBS-only intervention, the study specifically excluded students with elevated symptoms of depression and did not screen for other mental health issues.
The Current Study
The limited data examining the utility of PBS training in multi- and single-component interventions have produced mixed results. The current study sought to extend past research by evaluating the efficacy of a PBS Skills Training and Personalized Feedback (PBS-STPF) intervention among heavy drinking students accessing mental health services. Since previous research has shown that PBS use is negatively associated with alcohol consumption and risk (American College Health Association, 2011; Martin et al., 2012; Patrick et al., 2011) and that these strategies may be especially useful for those students with poorer mental health (LaBrie et al., 2010; LaBrie et al., 2009), we hypothesize that post-intervention participants in a PBS-STPF condition will report greater PBS use, less alcohol consumption and fewer alcohol related negative consequences relative to a generic health information control condition.
Method
Participants
Participants were heavy-drinking students recruited from the psychological counseling center at a west coast, mid-sized private university. Of 560 students who contacted the research office and completed an initial screening interview, 279 (49.82%) met the eligibility criteria and were invited to participate in the study. The final sample (N = 251) was 70% female and had a mean age of 19.98 years old (SD = 1.22). The sample was 67.7% Caucasian, 13.5% Multiracial, 6.4% Other, 5.6% Asian, 3.2% African American, 1.2% Native Hawaiian/Pacific Islander, and 0.8% American Indian/Alaskan Native. Additionally, 20.7% of participants identified as Hispanic.
Procedure
Participants were recruited through an on-campus counseling center. Flyers were posted in the lobby of the center and advertisements were placed in the student newspaper describing a health study recruiting students who drank alcohol and were accessing college mental health services. In addition, students voluntarily accessing counseling services were referred to the study by the center staff during intake. All interested students were screened for eligibility over the phone. To participate, students had to report receiving services from a mental health provider within the past two years. Further, given that heavy drinkers are at greater risk of experiencing negative consequences from alcohol use compared to light drinkers (Nelson, Xuan, Lee, Weitzman, & Wechsler, 2009; Wechsler & Nelson, 2006), only students who reported heavy episodic drinking (four or more drinks for a female, five or more drinks for a male on one drinking occasion) in the past two weeks were eligible to participate. Eligible participants were provided with information about the study and invited to attend an in-person one-hour meeting. Participants met individually with a researcher who further explained the purpose of the study. After providing informed consent, participants completed a 20-minute computerized survey in the research lab. Following the survey, participants were given a short break before beginning either the PBS skills training and personalized feedback (PBS-STPF) intervention or control task. Both the PBS-STPF and control session took approximately 30 minutes. Participants in both conditions completed online follow-up surveys 1-and 6-months post intervention. Participants received a nominal stipend for completing each phase of the study (baseline and 2 follow-ups), as well as a bonus stipend for having completed all phases of the study.
Measures
Participants were asked to provide demographic information as part of the initial baseline assessment survey including: age, sex, Greek status, ethnicity and race. The follow-up surveys contained the same measures of alcohol consumption, alcohol consequences and PBS use as the baseline assessment.
Alcohol consumption
The Daily Drinking Questionnaire (DDQ; Collins, Parks, & Marlatt, 1985) was used to obtain information regarding participants’ drinking patterns during a typical week in the past 30 days. Participants were asked to provide the number of standard drinks consumed each day as well as the number of hours spent drinking. A standard drink was defined as a “12 oz. beer or wine cooler, 8 oz. of malt liquor, 4 oz. of table wine, or 1.25 oz. of spirits”. The DDQ is commonly used to assess typical drinking and has demonstrated good test-retest reliability (Neighbors, Dillard, Lewis, Bergstrom, & Neil, 2006) as well as validity (Collins et al., 1985). The Quantity, Frequency, Maximum Index (QFM; Baer, 1993; Marlatt, Baer, & Larimer, 1995) assessed the maximum number of standard drinks consumed on any one occasion within the past 30 days.
Alcohol-related consequences
The Brief Young Adult Alcohol Consequences Questionnaire (BYAACQ; Kahler, Strong, & Read, 2005) also assessed the negative consequences resulting from alcohol use in the past month. Participants indicate (“Yes” or “No”) which of the 24 items they have experienced in the past month. A composite score indicating how many consequences were experienced by each participant was created by summing the number of problems endorsed (α = .85). Items include consequences such as “I have taken foolish risks when I have been drinking” and “My drinking has gotten me into sexual situations I later regretted”. The BYAACQ has demonstrated good reliability as well as validity (Kahler, Hustad, Barnett, Strong, & Borsari, 2008).
Protective behavioral strategies
Participants completed 14-items from the Protective Behavioral Strategies Survey (Martens et al., 2005) and an additional 18 items from the Strategy Questionnaire (SQ; Sugarman & Carey, 2007). These 32 item reflect the content of the PBS feedback used in the intervention condition. The combination of non-overlapping items from the SQ and PBSS allowed for the assessment of a wider, more complete range of alcohol-related protective behavioral strategies. Examples of the items present included “Avoid drinking games”, “Put extra ice in your drink”, “Limit drinking to certain days of the week”, and “Avoid situations where heavy drinking is likely”. Participants were asked to rate how frequently they used each behavioral strategy during the past month using a Likert scale ranging from 1 (Never) to 6 (Always). The 32 items were summed to form a composite score (α = .90).
Mental health
The 21-item Depression Anxiety Stress Scale (DASS-21; Lovibond, P. F. & Lovibond, S. H., 1995) was used to assess students’ psychological distress. The DASS-21 has three subscales named depression (α = .86), anxiety (α = .72) and stress (α = .83). Response options range from 0 (Did not apply to me at all) to 3 (Applied to me very much, or most of the time). As described in the mental health literature (Crawford & Henry, 2003; Henry & Crawford, 2005; Lovibond, P. F. & Lovibond, S. H., 1995), pre-established cut-points were used to classify DASS subscales scores as indicators of normal, mild, moderate, severe, or extremely severe distress.
Intervention and Control Sessions
Prior to the session, participants were randomly assigned into either the PBS skills training intervention with personalized feedback intervention condition (PBS-STPF) or a control condition.
PBS-STPF Intervention
The PBS intervention involved a facilitator-led one-on-one PBS cognitive behavioral skills training with personalized feedback. Facilitators received training in the intervention protocol and motivational interviewing techniques. For example, facilitators were trained to interact with participants in a supportive, non-confrontational, empathetic manner consistent with the spirit of the motivational interviewing approach. A licensed clinical psychologist oversaw both the facilitators’ interactions with participants and adherence to the intervention protocol. During the session, the facilitator and participant first discussed both the positive (e.g., enhancement of social situations) and negative aspects (e.g., reduced academic performance, health, and wellbeing) of drinking. Next the participant's current use of PBS was examined. Immediately prior to the intervention, the facilitator printed a personalized feedback sheet using the participant's self-reports of PBS use from the baseline survey. This list consisted of 32 PBS and each item was marked as being used either “never”, “rarely”, “occasionally/sometimes”, or “usually/always” by the participant. Using the personalized feedback sheet, the participant and the facilitator discussed PBS already in use and their benefits. The facilitator also probed about PBS that were not currently being used, but that participants found appealing. After exploring the potential use of new PBS, the facilitator asked the participant to identify specific situations in which he or she typically drank. For each situation, the participant generated a list of PBS that could be used to reduce alcohol-related harm. Additionally, the participant was asked to identify potential barriers to PBS utilization in each situation and develop strategies for overcoming these obstacles. The participant was then asked to set personal behavioral goals regarding his or her use of PBS, a weekly drinking limit goal, and a drinking behavioral goal. Examples of behavioral goals include “I will only spend $20 per week on alcohol” or “I will not drink more than 3 drinks in one night”. Participants were not asked to make commitments toward these goals, but were asked to generate goals that they believed would be realistic for them to implement in the next 30 days.
Control session
In the control condition, facilitators provided participants with educational information regarding diet and exercise. Pamphlets containing information about the US dietary guidelines along with suggested healthy snacks were given to participants. The facilitator and participant discussed whether the participant's current diet matched existing recommendations and how the participant might be able to improve their adherence to dietary guidelines. Healthy snacks choices were discussed, along with possible ways to integrate a healthy diet into the college lifestyle such as bringing fruit to class and not skipping meals or eating junk food. Recommended guidelines for exercise behaviors were also included in the pamphlets. Participants discussed their current exercise activities, considered how well current behaviors aligned with recommended guidelines, and identified barriers to engaging in exercise. Finally, participants reflected on their reaction to the health information and were encouraged to make healthier dietary and exercise choices.
Analytic Plan
To ensure that the distribution of variables satisfied statistical assumptions, scores exceeding three standard deviations away from the mean were replaced with values at three standard deviations (Tabachnick & Fidell, 2007). After this procedure, the skewness of variables was no higher than an absolute value of 1.50. As the main analyses involved repeated measures ANOVA, no sphericity issues were encountered, with high epsiolon values evidenced.
To evaluate the efficacy the PBS-STPF intervention, a set of four repeated-measures ANCOVAs were undertaken. The intervention condition (PBS-STPF vs. Control) was specified as the between-subjects factor. Time (baseline, 1 month follow-up, and 6-month follow-up) served as the within-subjects factor. Composites representing PBS, drinks per week, maximum drinks, and negative consequences were specified as the repeated measures in separate models. If the interaction of condition and time was found to be significant, follow-up LSD contrasts were used to evaluate pair-wise mean differences. As previous research has documented variations in levels of drinking attributed to sex (male vs. female) and Greek affiliation (member of a fraternity/sorority or not) (Barry, 2007; Scott-Sheldon, Carey, & Carey, 2008), both of these variables were included as covariates in all the repeated measures analyses.
To examine whether post-intervention PBS use mediated intervention effects, tests of mediation were performed using the Preacher-Hayes INDIRECT bootstrap test (5,000 resamples) in SPSS (Preacher & Hayes, 2008). Intervention condition was specified as the independent variable, one-month PBS use as the mediator, and drinking and consequences at 6 months as the dependent variables. All mediation analyses controlled for sex and Greek status.
Results
Descriptive Data
Using established severity cut-points for scores on the Depression, Anxiety, and Stress, Scale (DASS) scores in student samples (Crawford & Henry, 2003; Henry & Crawford, 2005; S.H. Lovibond, & P.F. Lovibond, 1995), 55% of participants were classified with mild-to-extremely severe distress associated with depressive symptoms, 46.2% for mild-to-extremely severe distress associated with anxiety symptoms, and 62.2% for mild-to-extremely severe distress associated with stress; while 12.7% reported symptoms corresponding to severe or extremely severe distress associated with depression, 27.1% reported severe or extremely severe distress associated with anxiety, and 39% reported severe or extremely severe distress associated with stress. Participants reported various reasons for seeking counseling services including anxiety (57.0%), stress (55.0%), depression (41.0%), and panic attacks (14.7%). Only 11.6% reported seeking counseling services for alcohol use concerns.
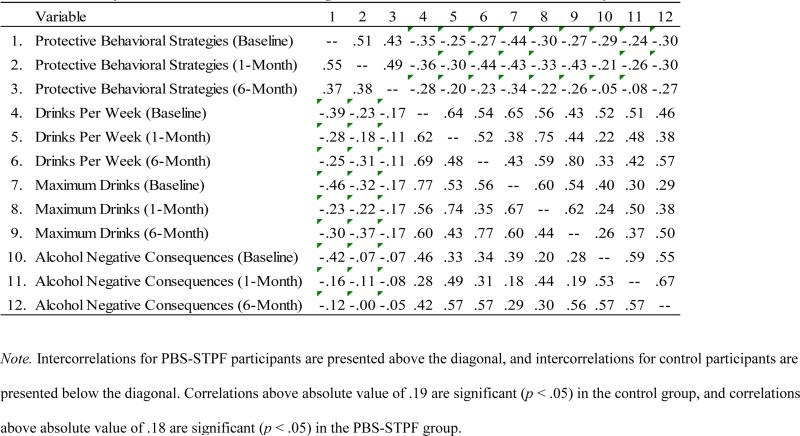
A correlation matrix of PBS use and alcohol outcomes is presented in Table 1. Within the PBS-STPF group, PBS use was significantly and inversely correlated with drinking and consequences at each time point. In contrast, within the control condition PBS use was negatively correlated with both drinks per week and consequences at baseline, but these relationships were no longer significant at 1 and 6 months.
Table 1.
Intercorrelations for Protective Behavioral Strategies and Alcohol Outcomes as a Function of Condition
|
Protective Behavioral Strategies
A repeated-measures ANCOVA was performed with PBS as the dependent variable (Table 2). The main effects of intervention, F(1, 207) = 1.86, p = .17, and time, F(2, 414) = .57, p = .57, were not significant. However, a significant condition × time effect emerged, F(2, 414) = 3.08, p < .05 (Figure 1). Pair-wise comparisons of mean scores indicated that the PBS-STPF group and control group were not systematically different at baseline. At the 1-month follow-up, PBS-STPF participants were significantly more likely than the control participants to use protective strategies, p < .05. At the 6-month follow-up, the adoption of behavioral strategies by the treatment participants persisted and remained significantly higher than that of the control participants, p < .05. For the PBS-STPF group, the use of protective strategies significantly increased from baseline to 1 month (p < .05), from baseline to 6-month (p < .05), and from 1-month to 6-month (p < .05). Within the control group, no significant mean difference in protective strategies was evident from baseline to 1-month, but, the use of these strategies at 6-month was higher than the previous time points (both ps < .05).
Table 2.
Repeated Measures ANCOVAs Examining PBS Use, Past Month Alcohol Consumption and Consequences by Condition at Baseline, 1-month, and 6-month Follow-ups.
| Measure | PBS-STPF M (SD) |
Control M (SD) |
Condition (C) F test |
Time (T) F test |
T × C F test |
|---|---|---|---|---|---|
| PBS | 1.86 | .57 | 3.08* | ||
| Baseline | 98.09 (21.94) | 99.40 (22.45) | |||
| 1-month | 106.34 (29.00) | 99.07 (25.49) | |||
| 6-month | 110.59 (29.49) | 105.46 (30.50) | |||
| Weekly drinking | 0.10 | 3.68* | 0.27 | ||
| Baseline | 15.99 (9.24) | 15.57 (10.20) | |||
| 1-month | 11.13 (8.99) | 11.28 (9.07) | |||
| 6-month | 12.59 (10.96) | 11.80 (11.82) | |||
| Max drinks | 0.62 | 8.82** | 0.36 | ||
| Baseline | 9.47 (4.31) | 9.69 (4.09) | |||
| 1-month | 7.25 (3.93) | 7.91 (4.09) | |||
| 6-month | 7.22 (4.39) | 7.45 (4.97) | |||
| Alcohol consequences | 0.14 | 1.50 | 0.40 | ||
| Baseline | 7.89 (5.05) | 8.04 (4.71) | |||
| 1-month | 6.11 (5.59) | 6.68 (5.45) | |||
| 6-month | 6.14 (5.97) | 6.12 (5.26) |
Note. All analyses statistically control for participant sex and greek status
p < .05.
p < .001.
Figure 1.

Protective behavioral strategies across time as a function of intervention condition, controlling for participant sex and Greek status.
Drinks Consumed and Alcohol Consequences
Next, repeated-measures ANCOVAs were conducted featuring drinks per week, maximum drinks, and negative alcohol consequences as respective outcome variables (Table 2). Greek status and sex of the participant were controlled for across analyses. For the model predicting drinks per week, the time effect was significant, F(2, 414) = 3.68, p < .05, but the condition effect, F(1, 207) = 0.10, p = .76, and the interaction between these two factors , F(2, 414) = 0.27, p = .77, did not attain significance. Closer inspection of the main effect for time indicated that across both the PBS-STPF and control groups the number of drinks per week significantly decreased from baseline to 1 month (p < .001), and baseline to 6 month (p < .001).
Similarly, the maximum drinks model indicated that time was significant, F(2, 414) = 8.82, p < .001, but the condition, F(1, 207) = 0.62, p = .43, and the interaction, F(2, 414) = .36, p = .70, did not emerge as significant. Closer examination of the main effect for time revealed that participants decreased in the maximum number of drinks consumed per occasion from baseline to 1 month (p < .001) and baseline to 6 months (p < .001). The pattern for maximum drinks paralleled that of the results obtained for drinks per week (Figure 2).
Figure 2.

Alcohol use and consequences across time as a function of intervention condition, controlling for participant gender and Greek status.
For the model predicting negative consequences, the effects were non-significant for condition, F(1, 207) = 0.14 , p = .71, time, F(2, 414) = 1.50, p = .22, and interaction, F(2, 414) = .40, p = .67 (Figure 2).
Tests of Mediation
Three sets of mediational analyses were conducted with intervention participants only, using recommended guidelines based on 5,000 bootstrap samples and bias corrected confidence intervals (Hayes, 2009; Preacher & Hayes, 2004; Zhao, Lynch, & Chen, 2010). All analyses control for participant sex and Greek status. Meditational analyses were conducted to determine whether the intervention may indirectly, through the mediating process of PBS use, result in subsequent reductions in the drinking outcomes.
The first mediational model revealed that the intervention significantly predicted PBS use (p < .05), and that this mediator subsequently predicted drinks per week (p < .001). Further scrutinization of this model revealed a significant indirect effect from the intervention to PBS to drinks per week, B = -1.14, 95% confidence interval (CI) [-2.63, -0.08], but the direct effect from the intervention to weekly drinking was not significant. A similar finding was obtained with maximum drinks as the outcome variable. The intervention significantly explained variance in PBS (p < .05), which in turn significantly accounted for variance in maximum drinks (p < .001). In this mediational model, results show a significant indirect effect, B = -0.43, 95% CI [-0.98, -0.02], but no significant direct effect. Finally, with consequences as the outcome variable, the mediational model showed that the intervention predicted PBS (p < .05), a factor that subsequently predicted negative consequences (p < .05). The direct effect did not attain significance; however, there was significant indirect effect of the intervention to the final outcome of alcohol-related consequences, B = -0.25, 95% CI [-0.75, -0.01].These results underscore that the intervention indirectly fostered reductions in drinking and consequences through correspondingly greater post-intervention usage of PBS. Phrased differently, without participants’ increased use of PBS, no longitudinal predictive connection would have been observed from the intervention to levels of alcohol consumption and consequences. The traversal of these particular pathways is consistent with the fact that the information offered by the intervention design was specifically tailored to engaging participants about how they may effectively take advantage of PBS.
Discussion
To date, only two studies have tested the efficacy of a standalone PBS training intervention (Kenney et al., in press; Martens et al., 2013), and neither study targeted students with poor mental health. Students with poorer mental health often underutilize PBS, but when they do employ these strategies, they can garner significant benefits (LaBrie et al., 2010; LaBrie et al., 2009). The present study is the first to evaluate the efficacy of a standalone PBS cognitive behavioral skills training and personalized feedback intervention (PBS-STPF) for heavy drinking students with poorer mental health. Results indicated that at one- and six-month follow-up, PBS use was correlated with less drinking and fewer consequences for intervention participants, but not control participants. Relative to a control condition, participants in the PBS-STPF condition reported significantly higher PBS use at one-month post-intervention. Furthermore, this difference in usage of PBS was maintained for up to six months after the intervention. Yet, despite the promising findings regarding PBS use, there was no Time × Condition interaction effect for either alcohol use or consequences.
Compared to baseline, participants collapsed across both conditions reported significantly less weekly drinking, reductions in the maximum number of drinks consumed on one occasion, and trends toward fewer consequences at one- and six-months. There are several possible explanations for why the interventions did not result in significantly greater reductions in alcohol use and harm relative to the control condition. First, intervention participants may not have employed PBS effectively. For example, participants may have increased their use of PBS in low-risk contexts where they found them easy to use and faced limited peer pressure to drink or engage in high-risk activities (e.g., drinking shots, playing drinking games). Students with poorer mental health may lack the resiliency or social skills necessary to employ PBS in higher-risk contexts where PBS may have been most beneficial for reducing alcohol-related consequences. Interventions incorporating multiple sessions could shed light on how students with poorer mental health employ new PBS, and help students overcome potential barriers to increasing use.
While participants in the intervention condition may not have optimally used PBS, it is also possible that the strategies themselves were ineffective. A growing body of literature suggests that different types of PBS may not be equally useful for reducing alcohol risk (Napper, Kenney, Lac, Lewis, & LaBrie, 2014). For example, strategies aimed at avoiding consequences or changing the way a student drinks are more closely related to less drinking and consequences than strategies that involve stopping or limiting drinking (Frank, Thake, & Davis, 2012; Napper et al., 2014; Pearson, Kite, & Henson, 2012, 2012). In the current study, intervention students reported the greatest increases in stopping or limiting drinking PBS, rather than strategies more closely related to reductions in alcohol risk. Stopping and limiting drinking strategies include deciding not to exceed a set number of drinks and stopping drinking at a predetermined time. Examination of the behavioral and PBS goals set by the students in the intervention condition indicated that some students set goals that were unlikely to lead to reductions in drinking or consequences (e.g., “I plan not to exceed 12 drinks” or “don't stay out past 2am”). Future intervention studies might consider focusing on training PBS skills that appear most beneficial for reducing alcohol use and risks, and working with students to ensure they set realistic and harm-reducing goals for stopping and limiting drinking.
Further, teaching PBS skills alone may not be sufficient to reduce the negative consequences of alcohol use in heavy drinking students with poorer mental health. Indeed the current findings are consistent with previous studies demonstrating that standalone PBS instruction and feedback, at best, produces limited reductions in alcohol consumption among students without mental health challenges (Martens et al., 2013; Sugarman & Carey, 2009). Martens and colleagues suggest that PBS training may not be adequate to motivate reductions in drinking. For some students PBS may even allow students to continue drinking at the same or even greater levels. This may be particularly true when PBS training is not paired with additional intervention components specifically aimed at increasing motivation to reduce drinking. However, the Martens et al. and Sugarman & Carey studies were very brief, as was the current study and more substantial PBS interventions, particularly with students with poorer mental health, may be more effective. Further, Kenney et al. (in press) found effects for a group PBS intervention that was about twice as long as the current intervention.
Although the intervention did not directly affect drinking outcomes, tests of mediation indicated that the intervention indirectly led to reductions in weekly drinking, peak drinking and alcohol-related consequences. Participants in the intervention used more PBS at one month, which predicted less drinking and fewer consequences at six months. This suggests that reductions in drinking within the control condition were not a result of changes in PBS use, but some other mechanism. It is possible that either the control condition content or the assessment of drinking affected student drinking. While the control condition did not address alcohol consumption, encouraging students to make healthy diet and exercise choices combined with assessments that focused on alcohol use and consequences may have indirectly motivated students to reduce their alcohol consumption. Indeed, encouraging students to think more intentionally about their calorie consumption and overall health may have resulted in decreased alcohol use. Further, assessments which focused on PBS, alcohol consumption, and alcohol consequences may have influenced post-assessment behavioral reporting. Future research including a non-health related control and involving minimal or multi-faceted assessments would help further clarify the effects of PBS interventions and health-related controls.
Interestingly, participants in the control condition reported a slight increase in PBS use at 6 months. Although students in the control group did not receive PBS training, they were presented with a list of PBS during surveys at each time point. This exposure, even without feedback or training, may have led to the slight increase in PBS seen at the final assessment.
Limitations and Future Directions
Although steps were taken to decrease biases in responding, such as reminding participants of confidentiality, limitations of this study include the use of self-report measures. Secondly, the measure of PBS used in the current study may not have adequately assessed all the types of strategies students employed. During the intervention, students were encouraged to generate their own personally-relevant PBS (e.g., avoiding drinking with a specific person or at a specific venue) that were not captured by the PBS measure. Additionally, the measures of PBS, alcohol use and consequences included in follow-up surveys were not event-level. Therefore, it is not possible to specifically examine how participants employed PBS, or whether PBS use on a specific occasion was associated with less alcohol use and fewer consequences. Finally, the current study focused on students accessing mental health services. Consequently, the findings may not generalize to other college student groups, including those not accessing psychological services and those with more severe mental health challenges. Furthermore, while focusing on a group of students who are most likely to benefit from increased use of PBS (LaBrie et al., 2010; LaBrie et al., 2009), the intervention did not specifically address how mental health issues may affect alcohol use or the connection between PBS and mental health. Only a couple of the PBS included in the intervention feedback touched on coping and mental health (e.g., “Finding other ways besides drinking to reduce stress”, “Practicing ways to be more comfortable in social settings without using alcohol”). Interventions that provide a more detailed exploration for how students can successfully implement PBS that address coping and anxiety would be beneficial.
Conclusions
The current study highlights the concerning levels of high-risk drinking among college students with poorer mental health. At baseline, female participants consumed on average 8.3 drinks on their maximum drinking occasion and males 12.3 drinks. This finding is consistent with data from first-time counseling center clients who report higher rates of heavy episodic drinking (57%; LaBrie, 2009) than among the general college population (40 to 50%; O'Malley & Johnston, 2002; Wechsler & Nelson, 2008). These numbers underscore the need for alcohol prevention efforts targeting students accessing mental health services. In light of the small proportion of participants who reported seeking help for alcohol concerns (12%), incorporating alcohol screening into campus mental health programs would also be beneficial.
PBS-STPF appears to be a useful tool for increasing PBS use for students who may lack the resources to employ these skills naturally or spontaneously. Despite the encouraging increases in PBS post-intervention, the current study's findings suggest that a standalone brief PBS skills training may not be sufficient to produce substantial decreases in drinking and consequences relative to a health-related control condition. Still, the demonstrated effectiveness of PBS training when incorporated in multi-component interventions (Barnett et al., 2007; Larimer et al., 2007) and relative to a less robust control condition (i.e., study skills focused) in a longer standalone PBS group intervention (Kenney et al., in press) point to the potential of PBS skills training. Additional research is needed to identify intervention components that may be important for motivating changes in drinking behavior. Future studies should consider examining the efficacy of teaching specific types of PBS that are more closely related to reductions in drinking and consequences, examining post-intervention use of PBS during specific drinking events, and providing multiple sessions to explore challenges employing PBS in high-risk contexts.
Acknowlegements
This research was supported by Grant R21AA020104 from the National Institute of Alcohol Abuse and Alcoholism (NIAAA). Support for Drs. Napper and Kenney was provided by ABMRF/The Foundation for Alcohol Research. Dr. Kenney is also supported by Grant T32AA007459 (NIAAA). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIAAA or the National Institutes of Health.
Footnotes
The authors declare that they have no conflict of interest.
References
- American College Health Association American College Health Association National College Health Assessment Spring 2006 Reference Group data report (abridged). Journal of American College Health. 2007;55(4):195–206. doi: 10.3200/JACH.55.4.195-206. doi: 10.3200/JACH.55.4.195-206. [DOI] [PubMed] [Google Scholar]
- American College Health Association . American College Health Association-National College Health Assessment II: Reference Group Executive Summary Spring 2011. Author; Hanover, MD: 2011. [Google Scholar]
- Araas T, Adams T. Protective behavioral strategies and negative alcohol-related consequences in college students. Journal of Drug Education. 2008;38(3):211–224. doi: 10.2190/DE.38.3.b. doi: 10.2190/DE.38.3.b. [DOI] [PubMed] [Google Scholar]
- Baer JS. Etiology and secondary prevention of alcohol problems with young adults. In: Baer JS, Marlatt GA, McMahon RJ, editors. Addictive behaviors across the lifespan. Sage; Newbury Park: 1993. pp. 111–137. [Google Scholar]
- Barnett NP, Murphy JG, Colby SM, Monti PM. Efficacy of counselor vs. computer-delivered intervention with mandated college students. Addictive Behaviors. 2007;32(11):2529–2548. doi: 10.1016/j.addbeh.2007.06.017. doi: 10.1016/j.addbeh.2007.06.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barry AE. Using theory-based constructs to explore the impact of Greek membership on alcohol-related beliefs and behaviors: A systematic literature review. Journal of American College Health. 2007;56(3):307–315. doi: 10.3200/JACH.56.3.307-316. doi: 10.3200/Jach.56.3.307-316. [DOI] [PubMed] [Google Scholar]
- Britton P. The relation of coping strategies to alcohol consumption and alcohol-related consequences in a college sample. Addiction Research and Theory. 2004;12(2):103–114. doi: 10.1080/16066350310001613062. [Google Scholar]
- Camatta CD, Nagoshi CT. Stress, depression, irrational beliefs, and alcohol use and problems in a college student sample. Alcoholism: Clinical and Experimental Research. 1995;19(1):142–146. doi: 10.1111/j.1530-0277.1995.tb01482.x. doi: 10.1111/j.1530-0277.1995.tb01482.x. [DOI] [PubMed] [Google Scholar]
- Center for the Study of Collegiate Mental Health 2009 Pilot Study: Executive Summary. 2009 Retrieved from http://www.sa.psu.edu/caps/pdf/2009-CSCMH-Pilot-Report.pdf.
- Collins RL, Parks GA, Marlatt GA. Social determinants of alcohol consumption: The effects of social interaction and model status on the self-administration of alcohol. Journal of Consulting and Clinical Psychology. 1985;53(2):189–200. doi: 10.1037//0022-006x.53.2.189. doi: 10.1037/0022-006X.53.2.189. [DOI] [PubMed] [Google Scholar]
- Cooper ML, Agocha VB, Sheldon MS. A motivational perspective on risky behaviors: The role of personality and affect regulatory processes. Journal of Personality. 2000;68(6):1059–1088. doi: 10.1111/1467-6494.00126. [DOI] [PubMed] [Google Scholar]
- Crawford JR, Henry JD. The Depression Anxiety Stress Scales (DASS): Normative data and latent structure in a large non-clinical sample. British Journal of Clinical Psychology. 2003;42(2):111–131. doi: 10.1348/014466503321903544. [DOI] [PubMed] [Google Scholar]
- Dawson DA, Grant BF, Stinson FS, Chou PS. Psychopathology associated with drinking and alcohol use disorders in the college and general adult populations. Drug and Alcohol Dependence. 2005;77(2):139–150. doi: 10.1016/j.drugalcdep.2004.07.012. doi: 10.1016/j.drugalcdep.2004.07.012. [DOI] [PubMed] [Google Scholar]
- Erdur-Baker O, Aberson CL, Barrow JC, Draper MR. Nature and severity of college students' psychological concerns: A comparison of clinical and nonclinical national samples. Professional Psychology: Research and Practice. 2006;37(3):317–323. doi: 10.1037/0735-7028.37.3.317. [Google Scholar]
- Frank C, Thake J, Davis CG. Assessing the protective value of protective behavioral strategies. Journal of Studies on Alcohol and Drugs. 2012;73(5):839–843. doi: 10.15288/jsad.2012.73.839. [DOI] [PubMed] [Google Scholar]
- Gallager R. National Survey of Counseling Center Directors. International Association of Counseling Services; Washington D.C.: 2006. [Google Scholar]
- Gallagher RP. National survey of counseling center directors. International Association of Counseling Services; Arlington, VA: 2006. Retrieved from http://www.collegecounseling.org/pdf/2006_survey.pdf. [Google Scholar]
- Ham LS, Hope DA. College students and problematic drinking: A review of the literature. Clinical Psychology. 2003;23:719–759. doi: 10.1016/s0272-7358(03)00071-0. doi: 10.1016/S0272-7358(03)00071-0. [DOI] [PubMed] [Google Scholar]
- Hayes AF. Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Communication Monographs. 2009;76(4):408–420. doi: 10.1080/03637750903310360. [Google Scholar]
- Henry JD, Crawford JR. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. British Journal of Clinical Psychology. 2005;44:227–239. doi: 10.1348/014466505X29657. doi: 10.1348/014466505X29657. [DOI] [PubMed] [Google Scholar]
- Kahler CW, Hustad J, Barnett NP, Strong DR, Borsari B. Validation of the 30-day version of the Brief Young Adult Alcohol Consequences Questionnaire for use in longitudinal studies. Journal of Studies on Alcohol and Drugs. 2008;69(4):611–615. doi: 10.15288/jsad.2008.69.611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kahler CW, Strong DR, Read JP. Toward efficient and comprehensive measurement of the alcohol problems continuum in college students: The Brief Young Adult Alcohol Consequences Questionnaire. Alcoholism, Clinical and Experimental Research. 2005;29(7):1180–1189. doi: 10.1097/01.alc.0000171940.95813.a5. doi: 10.1097/01.ALC.0000171940.95813.A5. [DOI] [PubMed] [Google Scholar]
- Kenney SR, Napper LE, Martens MP, LaBrie JW. Examining the efficacy of a brief group protective behavioral strategies skills training intervention with first-year college women. Psychology of Addictive Behaviors. doi: 10.1037/a0038173. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuntsche E, Knibbe R, Gmel G, Engels R. Why do young people drink? A review of drinking motives. Clinical Psychology. 2005;25:841–861. doi: 10.1016/j.cpr.2005.06.002. doi: 10.1016/j.cpr.2005.06.002. [DOI] [PubMed] [Google Scholar]
- LaBrie JW. [Alcohol use among first time clients at a college counselling center] 2009. Unpublished raw data.
- LaBrie JW, Kenney SR, Lac A. The use of protective behavioral strategies is related to reduced risk in heavy drinking college students with poorer mental and physical health. Journal of Drug Education. 2010;40(4):361–378. doi: 10.2190/DE.40.4.c. doi: 10.2190/DE.40.4.c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- LaBrie JW, Kenney SR, Lac A, Garcia JA, Ferraiolo P. Mental and social health impacts the use of protective behavioral strategies in reducing risky drinking and alcohol consequences. Journal of College Student Development. 2009;50(1):35–49. doi: 10.1353/csd.0.0050. doi: 10.1353/csd.0.0050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Larimer ME, Cronce JM. Identification, prevention, and treatment revisited: Individual-focused college drinking prevention strategies 1999-2006. Addictive Behaviors. 2007;32:2439–2468. doi: 10.1016/j.addbeh.2007.05.006. doi: 10.1016/j.addbeh.2007.05.006. [DOI] [PubMed] [Google Scholar]
- Larimer ME, Lee CM, Kilmer JR, Fabiano PM, Stark CB, Geisner IM, Neighbors C. Personalized mailed feedback for college drinking prevention: A randomized clinical trial. Journal of Consulting and Clinical Psychology. 2007;75(2):285–293. doi: 10.1037/0022-006X.75.2.285. doi: 10.1037/0022-006X.75.2.285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Litt DM, Lewis MA, Blayney J, Kaysen D. Anxiety as a mediator of the protective behavioral strategy and alcohol use relationship. Journal of Studies on Alcohol and Drugs. 2013;74:168–174. doi: 10.15288/jsad.2013.74.168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lovibond PF, Lovibond SH. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy. 1995;33(3):335–343. doi: 10.1016/0005-7967(94)00075-u. doi: 10.1016/0005-7967(94)00075-U. [DOI] [PubMed] [Google Scholar]
- Lovibond SH, Lovibond PF. Manual for the Depression, Anxiety and Stress Scales. 2nd ed. Psychology Foundation; Sydney, Australia: 1995. [Google Scholar]
- Markman Geisner I, Larimer ME, Neighbors C. The relationship among alcohol use, related problems, and symptoms of psychological distress: Gender as a moderator in a college sample. Addictive Behavior. 2004;29:843–848. doi: 10.1016/j.addbeh.2004.02.024. doi: 10.1016/j.addbeh.2004.02.024. [DOI] [PubMed] [Google Scholar]
- Marlatt GA, Baer JS, Larimer ME. Preventing alcohol abuse in college students: A harm-reduction approach. In: Boyd GM, Howard J, Zucker RA, editors. Alcohol problems among adolescents: Current directions in prevention research. Lawrence Erlbaum Associates, Inc.; Hillsdale, NJ: 1995. pp. 147–172. [Google Scholar]
- Martens MP, Ferrier AG, Sheehy MJ, Korbett K, Anderson DA, Simmons A. Development of the Protective Behavioral Strategies Survey. Journal of Studies on Alcohol. 2005;66(5):698–705. doi: 10.15288/jsa.2005.66.698. [DOI] [PubMed] [Google Scholar]
- Martens MP, Martin JL, Hatchett ES, Fowler RM, Fleming KM, Karakashian MA, Cimini MD. Protective behavioral strategies and the relationship between depressive symptoms and alcohol-related negative consequences among college students. Journal of Counseling Psychology. 2008;55(4):535–541. doi: 10.1037/a0013588. doi: 10.1037/a0013588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martens MP, Smith AE, Murphy JG. The efficacy of single-component brief motivational interventions among at-risk college drinkers. Journal of Consulting & Clinical Psychology. 2013 doi: 10.1037/a0032235. doi: 10.1037/a0032235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin RJ, Cremeens JL, Umstattd MR, Usdan SL, Talbott-Forbes L, Garner MM. Drinking behaviour, protective behavioural strategies and school performance of college students. Drugs: Education, Prevention & Policy. 2012;19(1):64–71. doi: 10.3109/09687637.2011.560910. [Google Scholar]
- Monti PM, Rohsenow DJ, Hutchison KE. Toward bridging the gap between biological, psychobiological and psychosocial models of alcohol craving. Addiction. 2000;95(2):229–236. doi: 10.1080/09652140050111799. [DOI] [PubMed] [Google Scholar]
- Murphy JG, Skidmore JR, Dennhardt AA, Martens MP, Borsari B, Barnett NP, Colby SM. A behavioral economic supplement to brief motivational interventions for college drinking. Addiction Research & Theory. 2012;20(6):456–465. doi: 10.3109/16066359.2012.665965. doi: 10.3109/16066359.2012.665965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Napper LE, Kenney SR, Lac A, Lewis LJ, LaBrie JW. A cross-lagged panel model examining protective behavioral strategies: Are types of strategies differentially related to alcohol use and consequences? Psychology of Addictive Behaviors. 2014;39(2):480–486. doi: 10.1016/j.addbeh.2013.10.020. doi: 10.1016/j.addbeh.2013.10.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neighbors C, Dillard AJ, Lewis MA, Bergstrom RL, Neil TA. Normative misperceptions and temporal precedence of perceived norms and drinking. Journal of Studies on Alcohol. 2006;67(2):290–299. doi: 10.15288/jsa.2006.67.290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nelson TF, Xuan Z, Lee H, Weitzman ER, Wechsler H. Persistence of heavy drinking and ensuing consequences at heavy drinking colleges. Journal of Studies on Alcohol and Drugs. 2009;70:726–734. doi: 10.15288/jsad.2009.70.726. [DOI] [PubMed] [Google Scholar]
- O'Malley PM, Johnston LD. Epidemiology of alcohol and other drug use among American college students. Journal of Studies on Alcohol. 2002:23–39. doi: 10.15288/jsas.2002.s14.23. [DOI] [PubMed] [Google Scholar]
- Park CL, Armeli S, Tennen H. The daily stress and coping process and alcohol use among college students. Journal of Studies on Alcohol. 2004;65(1):126–135. doi: 10.15288/jsa.2004.65.126. [DOI] [PubMed] [Google Scholar]
- Park CL, Grant C. Determinants of positive and negative consequences of alcohol consumption in college students: Alcohol use, gender, and psychological characteristics. Addictive Behaviors. 2005;30(4):755–765. doi: 10.1016/j.addbeh.2004.08.021. doi: 10.1016/j.addbeh.2004.08.021. [DOI] [PubMed] [Google Scholar]
- Patrick ME, Lee CM, Larimer ME. Drinking motives, protective behavioral strategies, and experienced consequences: Identifying students at risk. Addictive Behaviors. 2011;36(3):270–273. doi: 10.1016/j.addbeh.2010.11.007. doi: 10.1016/j.addbeh.2010.11.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pearson MR, Kite BA, Henson JM. The assessment of protective behavioral strategies: Comparing prediction and factor structures across measures. Psychology of Addictive Behaviors. 2012;26(3):573–584. doi: 10.1037/a0028187. doi: 10.1037/A0028187. [DOI] [PubMed] [Google Scholar]
- Pearson MR, Kite BA, Henson JM. Predictive effects of good self-control and poor regulation on alcohol-related outcomes: Do protective behavioral strategies mediate? Psychology of Addictive Behaviors. 2012 doi: 10.1037/a0028818. Advance online publication. doi: 10.1037/a0028818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behavior research methods, instruments, & computers : a journal of the Psychonomic Society, Inc. 2004;36(4):717–731. doi: 10.3758/bf03206553. [DOI] [PubMed] [Google Scholar]
- Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods. 2008;40:879–891. doi: 10.3758/brm.40.3.879. doi: 10.3758/BRM.40.3.879. [DOI] [PubMed] [Google Scholar]
- Ray AE, Turrisi R, Abar B, Peters KE. Social-cognitive correlates of protective drinking behaviors and alcohol-related consequences in college students. Addictive Behaviors. 2009;34(11):911–917. doi: 10.1016/j.addbeh.2009.05.016. doi: 10.1016/j.addbeh.2009.05.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scott-Sheldon LA, Carey KB, Carey MP. Health behavior and college students: Does Greek affiliation matter? Journal of Behavioral Medicine. 2008;31(1):61–70. doi: 10.1007/s10865-007-9136-1. doi: 10.1007/s10865-007-9136-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simons JS, Gaher RM, Correia CJ, Hansen CL, Christopher MS. An affective-motivational model of marijuana and alcohol problems among college students. Psychology of Addictive Behaviors. 2005;19(3):326. doi: 10.1037/0893-164X.19.3.326. doi: 10.1037/0893-164X.19.3.326. [DOI] [PubMed] [Google Scholar]
- Sugarman DE, Carey KB. The relationship between drinking control strategies and college student alcohol use. Psychology of Addictive Behaviors. 2007;21(3):338–345. doi: 10.1037/0893-164X.21.3.338. doi: 10.1037/0893-164X.21.3.338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sugarman DE, Carey KB. Drink less or drink slower: The effects of instruction on alcohol consumption and drinking control strategy use. Psychology of Addictive Behaviors. 2009;23(4):577–585. doi: 10.1037/a0016580. doi: 10.1037/a0016580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tabachnick BG, Fidell LS. Using multivariate statistics. 5th ed. Allyn & Bacon; Boston: 2007. [Google Scholar]
- Wechsler H, Nelson TF. Relationship between level of consumption and harms in assessing drink cut-points for alcohol research: Commentary on “Many college freshmen drink at levels far beyond the binge threshold” by White et al. Alcoholism: Clinical & Experimental Research. 2006;30:922–927. doi: 10.1111/j.1530-0277.2006.00124.x. doi: 10.1111/j.1530-0277.2006.00124.x. [DOI] [PubMed] [Google Scholar]
- Wechsler H, Nelson TF. What we have learned from the Harvard School of Public Health College Alcohol Study: Focusing attention on college student alcohol consumption and the environmental conditions that promote it. Journal of Studies on Alcohol and Drugs. 2008;69(4):481–490. doi: 10.15288/jsad.2008.69.481. [DOI] [PubMed] [Google Scholar]
- Weitzman ER. Poor mental health, depression, and associations with alcohol consumption, harm, and abuse in a national sample of young adults in college. Journal of Nervous and Mental Disease. 2004;192(4):269–277. doi: 10.1097/01.nmd.0000120885.17362.94. doi: 10.1097/01.nmd.0000120885.17362.94. [DOI] [PubMed] [Google Scholar]
- Zhao XS, Lynch JG, Chen QM. Reconsidering Baron and Kenny: Myths and truths about mediation analysis. Journal of Consumer Research. 2010;37(2):197–206. doi: 10.1086/651257. [Google Scholar]