

Abstract
Background:
There is an increasing amount of stress in undergraduate dental students leading to anxiety, depression, and suicidal attempts/suicide.
Aims:
This study aims to evaluate anxiety, depression and suicidal intent in undergraduate dental students and to find out the various areas of stress.
Materials and Methods:
A cross-sectional study was conducted using a semi-structured questionnaire (to assess academic and nonacademic areas of stress) and three scales-Hamilton scale for anxiety (HAM-A); Hamilton depression rating scale (HDRS) and Beck's Suicide Intent Scale (BSI). Descriptive statistics; Pearson's Chi-square test; Multiple ANOVA; Kruskal–Wallis test and Mann–Whitney test were used to analyze the data at the significant level of P ≤ 0.05.
Results:
In a total of 258 dental undergraduate students, academic areas of stress that were found to be statistically significant were long teaching hours (P = 0.002); high workload (P ≤ 0.001); frequency of tests (P ≤ 0.001) and competition/fear of failure (P = 0.009). Lack of interest in the profession was a statistically significant nonacademic area for stress (P ≤ 0.001). The students of first and final year reported higher anxiety (HAM-A 13.93 ± 6.908 and 16.44 ± 7.637 respectively) and depression (HDRS 14.29 ± 6.302 and 14.22 ± 5.422); whereas suicidal intent was reported almost the same throughout the study sample (BSI 5.65 ± 5.465).
Conclusion:
An increasing level of anxiety, depression and suicidal intent due to various stressors in undergraduate dental students indicate a need to modify current education system and timely help to have psychological healthy dental professionals in future.
Keywords: Academic stress, anxiety, dental students, depression, nonacademic stress, suicidal intent
Introduction
A growing body of research has reported a considerable amount of stress in undergraduate dental students even recording a 100% prevalence rate in few studies.[1,2] The phenomenon occurs almost across all years of dental education training and is prevalent indifferent countries with a different education system.[1,2,3,4,5,6,7] Stress is a normal response of a body to any demands while stressors are the demands and pressure that lead to stress. Stress results due to the discrepancy between excessive pressure and different types of demand and individual capacities to fulfill these demands.[8,9] Perception of stress is under the control of one's personal system of belief and attitude.[2] Distorted perceptions overemphasize our limitations and make the situation more stressful. Even stressors can vary with individual attitude, belief, and cultural background.[10]
Dental education has long been recognized as a complex and highly demanding training and hence can be one of the reasons for stress that can also persist in professional life.[2,6] Dental students are expected to achieve a high degree of diverse competencies, including theoretical knowledge, clinical practice and interpersonal skills.[9] Currently in India, undergraduate dental curriculum is covered over a period of 5 years, including 1-year compulsory internship. First 2 years mainly focus on core curriculum, including didactic or basic sciences. During third and 4th-year students are exposed to various clinical departments along with regular classes. At the end of each academic year, clinical skills and theoretical knowledge of the student is judged based on oral, written and practical examination. During the internship, students are rotated through different dental specialties in order to get clinical exposure.[11]
Academic and nonacademic stressors commonly reported in Indian dental students are examination and grades, performance pressure, managing difficult patient, poor patient co-operation, demanding nature of training, full working day, dealing with faculty and administration and parental pressure.[3,10,12,13] Persistent stressors can lead to psychological disturbance in the form of depression, anxiety and emotional exhaustion, loss of self-confidence, hostility, unprofessional conduct and burnout.[4,7,14,15] Paudel et al., 2013 reported significant negative effect of perceived stress on health in the form of fatigue, tiredness, mood alteration, sleep disturbance, back pain, headache, abdominal disturbances, oral ulcers and flu or common cold.[2] Subsequently, such disturbances in physical and mental well-being can hamper learning ability and academic performance of students.[7,16,17] Poor psychological health can also initiate thought of suicide/self-harm. Lay public and professional media usually depicted dental health professionals as a group of health-care workers with the highest suicidal rate though the evidences are less supporting.[18]
Hence, we planned this study to find out anxiety, depression and suicidal intent across all the 4 years of undergraduate dental students and identify different areas of stress in relation to academics and nonacademic surrounding.
Materials and Methods
A cross-sectional study was conducted at Maharishi Markandeshwar College of Dental Sciences and Research, Maharishi Markandeshwar University, Mullana (Ambala). Institutional Ethics Committee approval was obtained prior to the study. After obtaining informed consent, a total of 258 Bachelor of Dental Surgery (BDS) students across all 4 years of either sex were included in the study sample. Students with a history of substance dependence, psychotic disorders, and any co-morbid chronic medical illness were excluded from the study. Student's participation was completely voluntary without undue pressure. At the start of the study, principal investigator (MB) briefed all participants on aim and objectives of the study. The overall response rate from participants was good without any dropout.
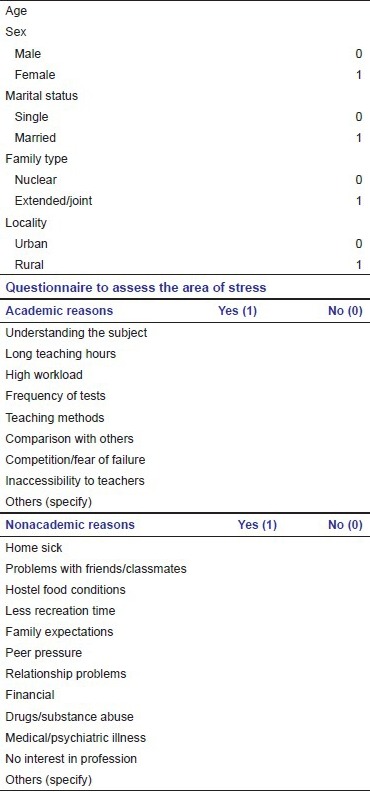
A semi-structured proforma was used to assess the different areas of stress. It included sociodemographic information of the students (age, sex, marital status, family type and locality), 9 academic and 12 nonacademic areas for stress. Response for each question related to academic and nonacademic areas for stress was reported in the form of ‘Yes’ (1) or ‘No’ (0) [Appendix]. The level of anxiety, depression, and suicidal intent was evaluated using Hamilton scale for anxiety (HAM-A) for assessment of anxiety;[19] Hamilton depression rating scale (HDRS) for assessment of depression[20] and Beck's Suicide Intent Scale (BSI) for assessment of suicidal intent[21] respectively. All students from 1st year BDS to final year BDS were given the questionnaire separately year wise by MB (PI) in lecture with the prior permission of the principal and the concerned teacher. Time allocated to complete the questionnaire was 30 min. Students absent for the respective study class were not included in the study sample. The semi-structured proforma and three scales were administered at the same time.
Statistical analysis
The sociodemographic variables were computed/analyzed by calculating the mean and standard deviation for age and frequency for sex, marital status, family type and locality.
The presence or absence of academic and nonacademic areas of stress was calculated by frequency.
Means and standard deviation were determined for the score of HAM-A; HDRS; BSI scales and the total score of HAM-D, HAM-A and BSI were compared across each 4 years. For the purpose of identifying levels of anxiety and depression across different training years, HAM-A and HDRS were graded as normal, mild, moderate and severe. Pearson's Chi-square test; multiple ANOVA; Kruskal–Wallis test and Mann–Whitney test were used to analyze the data at the significant level of P ≤ 0.05.
Results
A total of 258 undergraduate dental students were participated in the study. The students were between the ages of 18 and 22 years (overall mean age - 20.11 ± 1.426; BDS 1-18.47 ±0.775; BDS 2-19.85 ±0.718; BDS 3-20.69 ±.769; BDS 4-21.82 ±.796).
The study sample comprised of about 78% females (n = 201) (BDS 1 - male: 12; female 58;BDS 2 - male: 20, female 48; BDS 3 - male: 15, female 50; BDS 4 - male: 10, female 45). It was interesting to note that there was more number of female students across all the 4 years.
All students were single. Most of the students (74%) were from nuclear families (BDS 1-51; BDS 2-56; BDS 3-49; BDS 4-35). Over 85% students were from urban areas (BDS 1-61; BDS 2-58; BDS 3-59; BDS 4-42).
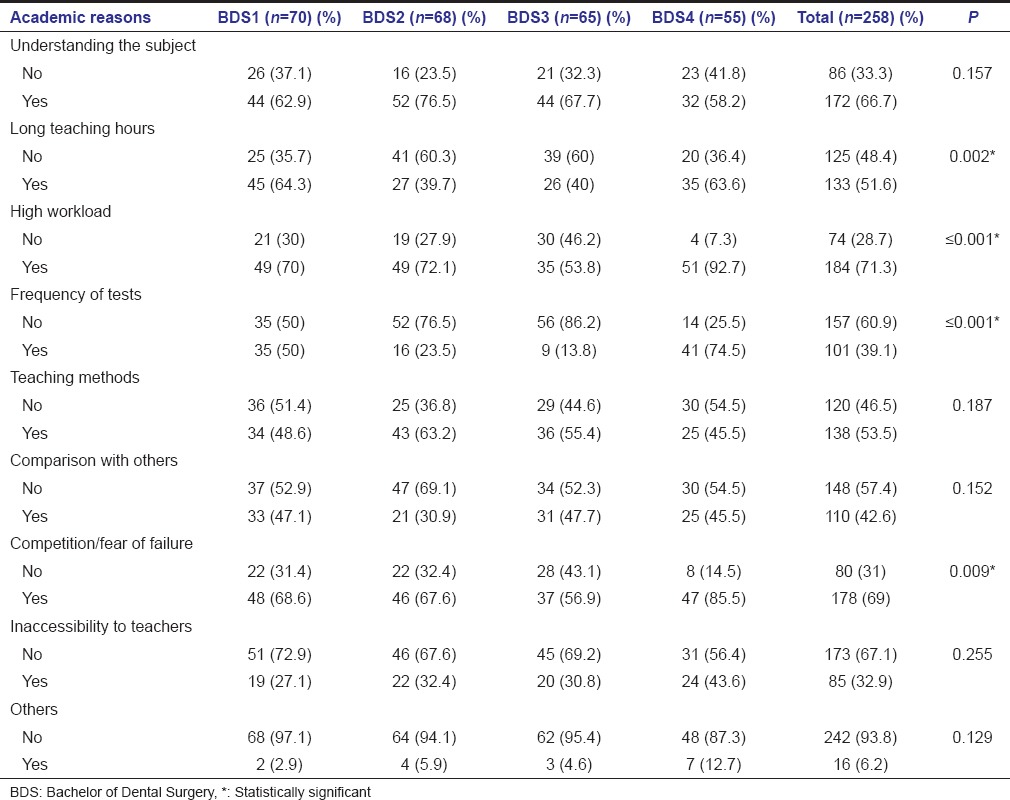
Table 1 shows areas of stress in relation to academic reasons. The common reasons for stress across all 4 years were long teaching hours (P = 0.002); high workload (P ≤ 0.001), frequency of tests (P ≤ 0.001) and competition/fear of failure (P = 0.009). Most of these academic stressors were higher for final year students.
Table 1.
Academic reasons for stress in study subjects across each year
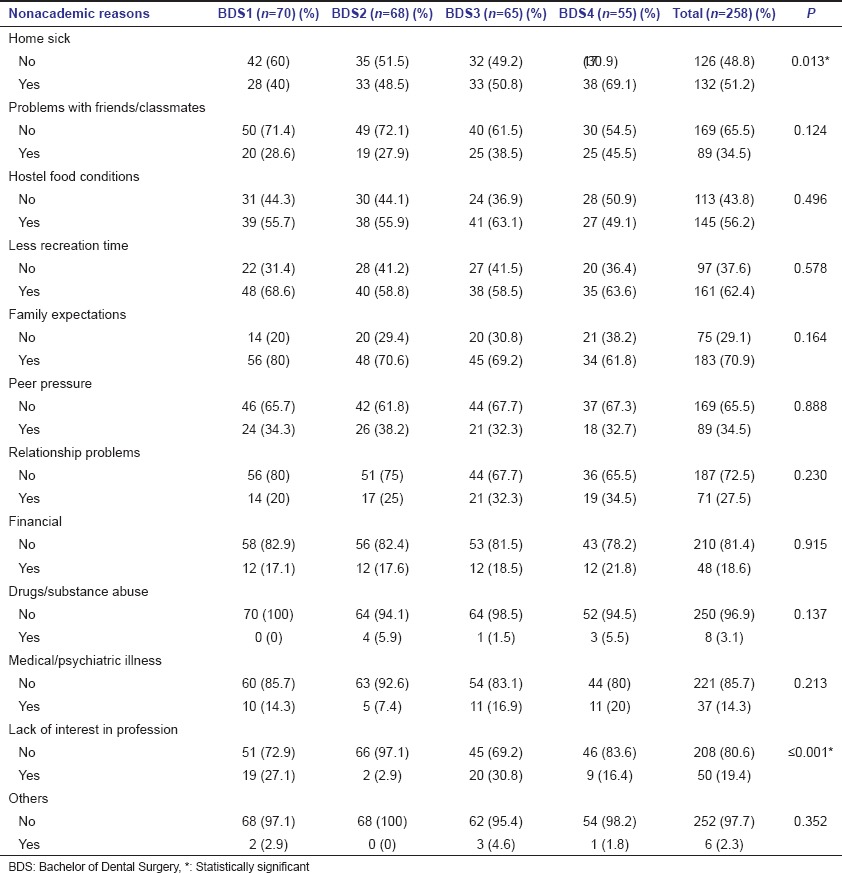
Lack of interest in the profession (P ≤ 0.001) and homesickness (P = 0.13) were the commonest nonacademic reason for stress in study subjects [Table 2].
Table 2.
Nonacademic reasons for stress in study subjects across each year
First and the final year students reported higher level of anxiety (HAM-A 13.93 ± 6.908 and 16.44 ± 7.637 respectively) and depression (HDRS 14.29 ± 6.302 and 14.22 ± 5.422); whereas the suicidal intent was almost the same throughout the sample (BSI 5.65 ± 5.465). The mean score for HAM-A; HDRS and BSI were 13.38 ± 8.489; 12.94 ± 6.635 and 5.65 ± 5.465respectively [Table 3].
Table 3.
HAM=A; HDRS; BSI (mean±SD) in study subjects

Tables 4 and 5 show the year-wise grading of HAM-A and HDRS as normal (0–6), mild (7–17), moderate (18–24) and severe (≥24). The majority of the students have graded themselves to be mildly anxious and depressed across all years.
Table 4.
Grading of HAM-A in study subjects

Table 5.
Grading of HDRS in study subjects

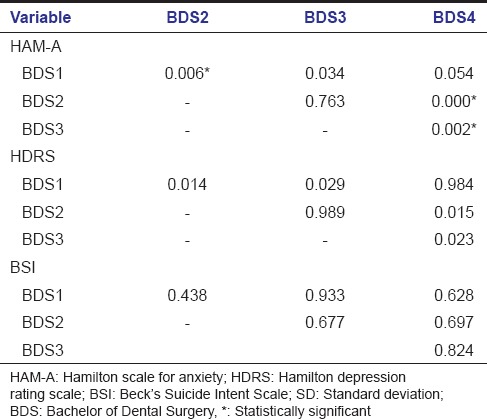
On comparing P value of HAM-A among different years of BDS, it was statistically significant for BDS 1 and BDS 2 (P = 0.006), BDS 2 and BDS 4 (P ≤ 0.001) and BDS 3 and BDS 4 (P = 0.002) respectively. On comparing P value of HDRS among different years of BDS, it was statistically significant for BDS 1 and BDS 2 (P = 0.014), BDS 1 and BDS 3 (P = 0.029) and BDS 2 and BDS 4 (P = 0.015) and BDS 3 and BDS 4 (P = 0.023) respectively. No statistical significance was found for BSI scores [Table 6].
Table 6.
Comparison of P of HAM-A, HDRS and BSI among different year of BDS
Tables 7 and 8 show the relationship between HAM-A and HAM-D with the academic and nonacademic reasons respectively, for the students reporting as “Yes” on the semi-structured proforma to assess the areas of stress.
Table 7.
Relationship of HAM-A and HAM-D score with the academic reasons
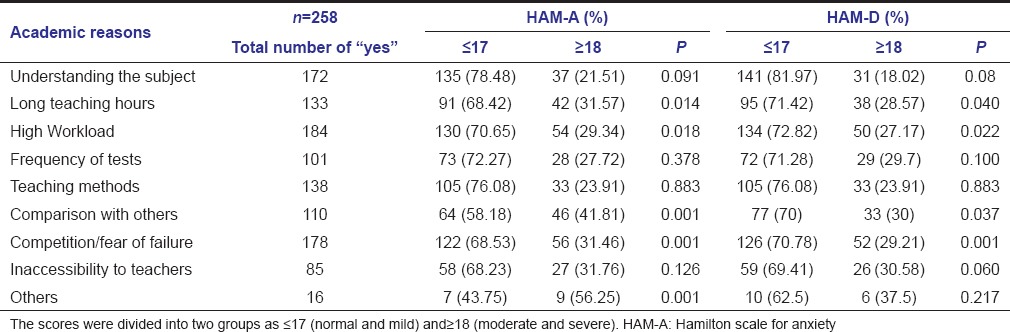
Table 8.
Relationship of HAM-A and HAM-D score with the nonacademic reasons
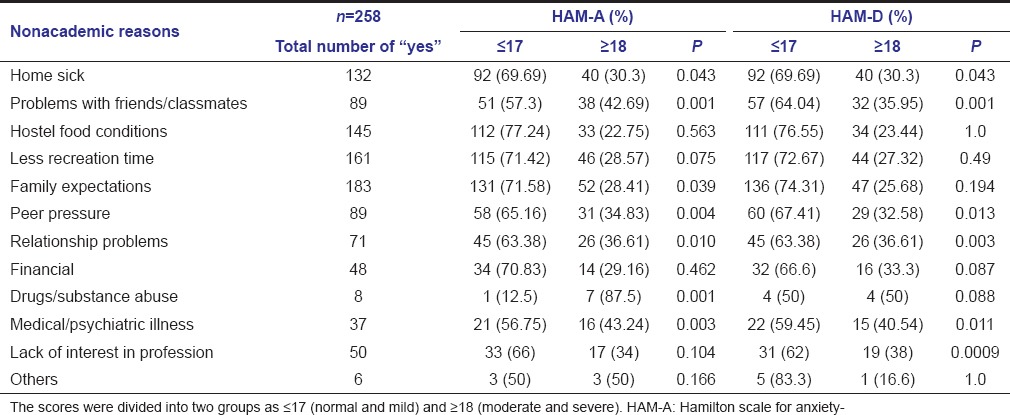
Table 7 – Students scoring “Yes” on academic reasons – long teaching hours (P = 0.014 [HAM-A] and 0.40 [HAM-D]), high workload (P = 0.018 [HAM-A] and P = 0.022 [HAM-D]), comparison with others (P = 0.001 [HAM-A] and P = 0.037 [HAM-D]) and competition/fear of failure (P = 0.001 [HAM-A] and P = 0.001 [HAM-D]) shows statistically significant level of both anxiety and depression.
Table 8 – Students scoring “Yes” on nonacademic reasons – home sick (P = 0.43), problems with friends/class mates (P = 0.001), family expectations (P = 0.39), peer pressure (P = 0.004), relationship problems (P = 0.01) and medical/psychiatric illness (P = 0.003) shows statistically significant level of both HAM-A and HDRS score. Whereas the students scoring “Yes” on drugs/substance abuse (P = 0.001) and family expectations (P = 0.039) were statistically significant for HAM-A score and parameters such as lack of interest in profession (P = 0.009) was statistically significant in relation to HDRS score.
Discussion
Stress is a normal biological response to adverse external or internal stimulus. In some cases, stress may motivate a person to achieve exceptionally high performance both personally and professionally. However, if the compensating response is inappropriate or inadequate, the same stress can result in clinical disorders such as anxiety and depression.[14]
Findings of the current study suggest that a significant percentage of undergraduate dental students experience stress across all years of training placing them at a risk of psychological disturbances. The results of our study also support the evidence from literature demonstrating a substantial level of stress among undergraduate dental students related to various academic or nonacademic reasons.[1,2,9]
We identified high workload as a noteworthy academic source of stress among undergraduate dental students. This is in agreement with the findings of other studies.[2,5,9] High workload in dental students during undergraduate years is usually associated with lots of tests, too many assignments, preparation for examination, scarcity of time and expectations in both theoretical and clinical knowledge. This is followed by competition or fear of failure as a second major stress evoking factor during academic years. Al-Samadani and Al-Dharrab reported fear of failure (51.3%) as a major cause of stress in undergraduate dental student, a finding very similar to our result.[9] We also found long teaching hours and frequency of tests as other common but significant academic stressors in dental program. Most of these academic stressors were reported high for final year students. During final years, students have to spend more time on patient care to excel clinical requirements. This left very little time for them to complete an assignment or prepare for examination. Overall stress level increases as the student progress in the academic program, mainly due to transition from nonclinical to clinical setting and expectation of excellence in both academic and clinical skills.[6,7,9]
Lack of interest in the profession was reported as a commonest nonacademic reason for stress in our study. This is frequently perceived in two circumstances when students are forced to join a dental school which is not of their choice. First when meritorious students failed to enroll in medical school either due to poor ranking in the entrance examination or due to financial constraints to pay high tuition fees of private medical college.[11] Secondly, this situation occurs when parents expected their children to take admission in a highly respectable profession like dentistry. This is commonly seen in India with strong family values where children can’t refuse their parents wish.[6] A study conducted in private dental college in India recorded greater stress among students who joined dentistry either due to parental pressure or whose career field of choice was different.[10]
Mild to moderate level of anxiety and depression was reported across all years of a dental education program. The trend of the mean score shows that that was a fall in mean score of both HAM-A and HDRS in second and third year followed by a rise again in the mean score in final year students.
Factors leading to anxiety can vary with academic years.[6] During 1st year, students are exposed to new educational environment. They may face difficulties with learning new syllabus; adjustment with new friends; adjustment with faculty and staff and new living accommodation if they are from other cities. As mentioned above, academic stressors are high in final year students. At this training level, final year students are expected to excel their clinical skills along with theoretical knowledge. These students may find difficulty in managing patient, feeling of inadequacy to complete clinical task, lack of time to complete assignment and preparation for examination, and fear of future dental career. A recent survey in Colombian dental students recorded marked increased in psychological distress level during transition from preclinical to clinical phases of training. Though our findings for 1st year students did not match with a survey, but they are in agreement for final year students.[7] When depression is evaluated at mild, moderate and severe levels, our findings are consistent with study by Reddy et al. for first 3 academic years. A constant stress if not recognized or left untreated can lead to depression and hence stress should not be ignored. Even early identification and management is necessary to prevent future health-related consequences.[17] Persistence of some degree of anxiety and depression can be manifestations of severe stress associated with high workload, rising competition and feeling of failure across all academic years.
Suicidal intent was found to be almost the same throughout the study sample. Not all the previously published studies dealing with suicide rates among dentists found increased suicide risk.[22] There are no valid data suggesting dentists are more prone to suicide as usually depicted in media.[18] However, a recently conducted study by Galán et al. for the 1st time reported prevalence of suicidal ideation among dental students for both preclinical and clinical years.[15] This area needs to be addressed regarding an association of stress and suicidal ideation among dentists.
There is no such study which has evaluated the relationship of the areas of stress to the level of anxiety, depression and suicidal intent. In our study though the relationship appears that the students having less score on the scales of HAM-A and HAM-D show more amount of stress appears to be paradoxical to the current literature. This could be explained by the fact that the stigma associated with the psychiatric disorders have actually inhibited the students to score themselves on the rating scales but whereas they have actually shown to be in stress in different areas of academic and nonacademic reasons.
It is impractical to remove all stress provoking factors from the current dental education system. However, identifying different areas of stress help to reduce a stress level by making changes in curriculum; revising education process in consideration with both student and staff and use of resources such as counseling service.[6] Paudel et al. recommended that dental colleges must take help of educational expert in designing and developing student-oriented curriculum in order to reduce stress and improve psychological well-being of the student. This will help to develop professionally sound graduates with better academic and clinical performance.[2] It is equally important that parents should be advised not to force their children to join educational program that they don’t like.[10]
Major drawback of a current dental education system is that there is no stress management class in regular training. Apart from standardizing current dental education, there is a need to create stress-free learning environment. Divaris et al. gives a concept of the ideal academic environment as one that prepares the students for their future professional life and contributes toward their personal development, psychosomatic and personal well-being.[23] Dahan and Bedos suggested implementation of two strategies to help stressed students that is, decreasing number of stressor and increasing ability to cope with stress. First strategy involved measures to minimize a number of stressors such as reducing fear of failure and workload related to examination and requirement. Increasing length of the curriculum can be one of the ways to reduce a workload on students and also help to reduce fear of failure. In implementation of this strategy, faculty members can play a crucial role by reconsidering prerequisites to pass examinations, scheduling information session between students and their seniors to share information, nurturing interpersonal relationship between students and educators and giving constructive feedback to struggling students.[8] In addition to student-oriented programs, there is a need of student advisor and counselors with faculty advising system to minimize the stress level.[2,3] Second strategy focuses on use of different coping techniques to overcome stress. In this scenario, organizing stress management and time management programs for students; discussing the importance of wellness and use of stress relievers like yoga and meditation are helpful options to reduce the stress level.[8]
Limitations of the study
However, results of our study can’t be generalized as it was conducted on small sample size and at a single center. There are chances of respondent's bias as the study was based on answering questionnaire by students who could manipulate information. In addition, the current study did not record demographic and socioeconomic factors influencing stress level and psychological disturbances. Literature about suicidal ideation among dental student is somewhat controversial.
So in future, larger studies involving large sample size, conducted at various geographical centers, carried out inconsideration with other factors for psychological disturbances and suicidal ideation will be required for more substantial results. In addition, the rating scales should be used in concordance with the clinical interview at least in those students scoring high on rating scales.
Strengths of the study
This is the only study which has evaluated the relationship of the areas of stress to the level of anxiety, depression and suicidal intent.
Conclusion
Persistence of anxiety, depression and suicidal intent in undergraduate dental students due to diverse academic and nonacademic reasons suggest a need for modifying current dental education system and creating stress-free learning environment. Based on these findings, it is imperative to revise current teaching methodology, boosts interpersonal relationships, and the introduction of stress management interventions and various coping strategies to overcome stress during an undergraduate program. Further, we suggest a creation of positive academic environment as a team work of faculty, administration, educational experts and students to develop psychological healthy dental professionals who can perform better in a coming future.
Appendix: Semi-Structured Proforma used for the study
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Ahmad MS, Md Yusoff MM, Abdul Razak I. Stress and its relief among undergraduate dental students in Malaysia. Southeast Asian J Trop Med Public Health. 2011;42:996–1004. [PubMed] [Google Scholar]
- 2.Paudel S, Subedi N, Shrestha A. Stress and its relief among undergraduate dental students in a tertiary health care centre in Eastern Nepal. Dentistry. 2013;3:157. [Google Scholar]
- 3.Kumar S, Dagli RJ, Mathur A, Jain M, Prabu D, Kulkarni S. Perceived sources of stress amongst Indian dental students. Eur J Dent Educ. 2009;13:39–45. doi: 10.1111/j.1600-0579.2008.00535.x. [DOI] [PubMed] [Google Scholar]
- 4.Stewart DW, de Vries J, Singer DL, Degen GG, Wener P. Canadian dental students’ perceptions of their learning environment and psychological functioning over time. J Dent Educ. 2006;70:972–81. [PubMed] [Google Scholar]
- 5.Polychronopoulou A, Divaris K. Perceived sources of stress among Greek dental students. J Dent Educ. 2005;69:687–92. [PubMed] [Google Scholar]
- 6.Tangade PS, Mathur A, Gupta R, Chaudhary S. Assessment of stress level among dental school students: An Indian Outlook. Dent Res J. 2011;8:95–101. [PMC free article] [PubMed] [Google Scholar]
- 7.Divaris K, Mafla AC, Villa-Torres L, Sánchez-Molina M, Gallego-Gómez CL, Vélez-Jaramillo LF, et al. Psychological distress and its correlates among dental students: A survey of 17 Colombian dental schools. BMC Med Educ. 2013;13:91. doi: 10.1186/1472-6920-13-91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dahan H, Bedos C. A typology of dental students according to their experience of stress: A qualitative study. J Dent Educ. 2010;74:95–103. [PubMed] [Google Scholar]
- 9.Al-Samadani KH, Al-Dharrab A. The perception of stress among clinical dental students. Word J Dent. 2013;4:24–8. [Google Scholar]
- 10.Acharya S. Factors affecting stress among Indian dental students. J Dent Educ. 2003;67:1140–8. [PubMed] [Google Scholar]
- 11.Elangovan S, Allareddy V, Singh F, Taneja P, Karimbux N. Indian dental education in the new millennium: Challenges and opportunities. J Dent Educ. 2010;74:1011–6. [PubMed] [Google Scholar]
- 12.Harikiran AG, Srinagesh J, Nagesh KS, Sajudeen N. Perceived sources of stress amongst final year dental under graduate students in a Dental Teaching Institution at Bangalore, India: A cross sectional study. Indian J Dent Res. 2012;23:331–6. doi: 10.4103/0970-9290.102218. [DOI] [PubMed] [Google Scholar]
- 13.Newton JT, Baghaienaini F, Goodwin SR, Invest J, Lubbock M, Marouf Saghakhaneh N. Stress in dental school: A survey of students. Dent Update. 1994;21:162–4. [PubMed] [Google Scholar]
- 14.Rada RE, Johnson-Leong C. Stress, burnout, anxiety and depression among dentists. J Am Dent Assoc. 2004;135:788–94. doi: 10.14219/jada.archive.2004.0279. [DOI] [PubMed] [Google Scholar]
- 15.Galán F, Ríos-Santos JV, Polo J, Rios-Carrasco B, Bullón P. Burnout, depression and suicidal ideation in dental students. Med Oral Patol Oral Cir Bucal. 2014;19:e206–11. doi: 10.4317/medoral.19281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Heath JR, Macfarlane TV, Umar MS. Perceived sources of stress in dental students. Dent Update. 1999;26:94–8. doi: 10.12968/denu.1999.26.3.94. 100. [DOI] [PubMed] [Google Scholar]
- 17.Reddy V, Naveenm N, Prabhu, Manipal S, Preethi A, Ahmed A. The evaluation of perceived stress and depression in dental undergraduates. Int Dent J Stud Res. 2013;1:36–41. [Google Scholar]
- 18.Alexander RE. Stress-related suicide by dentists and other health care workers. Fact or folklore? J Am Dent Assoc. 2001;132:786–94. doi: 10.14219/jada.archive.2001.0278. [DOI] [PubMed] [Google Scholar]
- 19.Hamilton A. The assessment of anxiety states by rating. Br J Med Psychol. 1959;32:50–5. doi: 10.1111/j.2044-8341.1959.tb00467.x. [DOI] [PubMed] [Google Scholar]
- 20.Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56–62. doi: 10.1136/jnnp.23.1.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Beck AT, Kovacs M, Weissman A. Assessment of suicidal intention: The Scale for Suicide Ideation. J Consult Clin Psychol. 1979;47:343–52. doi: 10.1037//0022-006x.47.2.343. [DOI] [PubMed] [Google Scholar]
- 22.Arnetz BB, Hörte LG, Hedberg A, Malker H. Suicide among Swedish dentists. A ten-year follow-up study. Scand J Soc Med. 1987;15:243–6. doi: 10.1177/140349488701500407. [DOI] [PubMed] [Google Scholar]
- 23.Divaris K, Barlow PJ, Chendea SA, Cheong WS, Dounis A, Dragan IF, et al. The academic environment: The students’ perspective. Eur J Dent Educ. 2008;12(Suppl 1):120–30. doi: 10.1111/j.1600-0579.2007.00494.x. [DOI] [PubMed] [Google Scholar]