

Abstract
Competitive athletes endure extreme bodily stress when participating in sports-related activities. An athlete’s skin is particularly susceptible to a wide array of repetitive physical and environmental stressors that challenge the skin’s protective function. Many unique dermatoses are well-known to the serious athlete due to countless hours of intense physical training, but are frequently unrecognized by many healthcare professionals. Sports dermatology is a distinctive, budding field of dermatology that focuses on dermatoses frequently encountered in athletes. Athletic skin problems are notoriously infectious in nature due to the inherent environment of close-contact physical activity. Nonetheless, other skin conditions can manifest or worsen with recurring mechanical or traumatic injury or exposure to environmental hazards. Additionally, sports-related activities may exacerbate other pre-existing dermatological conditions that may possibly be unknown to the athlete or clinician. The objective of this two-part review is to arm the astute physician with the fundamental knowledge of the range of dermatological conditions distinct to the competitive athlete. Knowledge of these cutaneous conditions in the context of specific sporting events will permit the clinician to manage these unique patients most effectively. Part one will focus on traumatic or mechanical injuries, inflammatory conditions, and exacerbations of pre-existing conditions frequently seen in athletes.
Total body skin examinations are typically performed by dermatologists to search for unusual or suspicious-looking lesions or skin conditions most commonly found in people at high risk for skin cancer such as melanoma.1-3 It is common that healthcare professionals be required to perform a history and physical examination on athletes for participation in sports. A complete skin examination is often forgone, as other parts of the physical examination, such as the cardiovascular, pulmonary, and neurological systems, are a priority. Although nothing can downplay the importance of examining the major regulatory systems in an athletic physical examination, there are many reasons for a proper complete skin examination in the competitive athlete who may be encountering a slue of sports-related physical and environmental stressors on their skin, hair, nails, and mucous membranes. A clinical evaluation of these locations is often sufficient enough to ensure adequate assessment for frequently encountered benign conditions, but often what is observed may be more complex and further evaluation may include other regulatory systems. Dermatologists may palpate for lymphadenopathy when examining patients suspected to have malignancy or infectious processes; examine the joints in patients who have connective tissue diseases; test for sensory deficits in patients being treated with neurotoxic medications or those with chronic neuropathies; or examine the oral mucosa for lesions suggestive of an underlying pathology, such as human immunodeficiency virus, autoimmune diseases, or nutritional deficiencies.
The ideal skin examination requires the patient to fully undress and be in an examination room with bright illumination. The patient should be examined systematically with consistency and adherence to a similar routine in order to minimize any omissions. Most dermatologists will begin at the head and work their way down the body, paying particular attention to areas often overlooked, such as behind and inside the ears, buttocks, genitals, bottom of feet, finger and toe web spaces, posterior scalp, nails, and mouth. Gloves should always be worn when examining a patient. Although most dermatologists like to touch skin lesions for texture and feel, which can help aid in diagnosis, this practice may increase the spread of communicable infections if the correct contact precautions are not maintained. It is important to look for any abnormality on the skin related to pattern, color, location/distribution, or general condition. Since there is considerable variation among individuals, an extensive language has been developed to standardize the description of skin lesions. It is prudent to have the knowledge of these characterizations to help in generating a substantial differential diagnosis (Table 1).
TABLE 1.
Standard description of skin lesions in dermatology
| NAME | DESCRIPTION | EXAMPLES |
|---|---|---|
| PRIMARY LESIONS (RESULTS FROM DISEASE PROCESS ITSELF) | ||
| Macule | Flat, non-palpable lesions <1cm in diameter | Freckles, flat moles, drug eruptions, mastocytosis, postinflammatory hyperpigmentation |
| Patch | Flat, non-palpable lesion >1cm in diameter | Tattoo, port-wine stain, rubella/measles, vitiligo |
| Papule | Solid, elevated, superficial, palpable lesion <1cm in diameter | Nevi, warts, acne, insect bites |
| Plaque | Solid, elevated, superficial, palpable lesions >1cm in diameter | Psoriasis, granuloma annulare |
| Nodule | Solid, elevated, deep, palpable lesion >1cm in diameter | Cysts, lipomas, fibromas, erythema nodosum |
| Tumor | Larger and often deeper seeded than a nodule | AV malformation, skin cancer, neuroma |
| Abscess | Nodule or tumor with free pus (purulent material) | Carbuncle, hidradenitis suppurtiva |
| Vesicle | Elevated, superficial, clear fluid-filled lesions <1cm in diameter | Herpes, contact dermatitis |
| Bullae | Elevated, superficial, clear fluid-filled lesions >1cm in diameter | Burns/bites, autoimmune blistering disorders, drug reactions, contact dermatitis |
| Pustule | Papule or vesicle with pus (purulent material) | Folliculitis, pustular psoriasis, drug eruptions, acne, rosacea |
| Wheal | Transient flat-topped cutaneous papule or plaque with erythematous boarder and pale center | Hypersensitivity to drugs, insect stings or bites, physical stimuli, autoimmunity, urticaria/anaphylaxis |
| Burrow | Formation of a tunnel in the skin | Scabies, cutaneous larva migrans |
| Telangiectasia | Dilatation of superficial blood vessels in the skin | Liver disease, scleroderma, chronic sun exposure, potent topical corticosteroids |
| SECONDARY LESIONS (CAUSED FROM OUTSIDE FACTORS, SUCH AS RUBBING, SCRATCHING, AND INFECTION) | ||
| Scale | Flakes or plates representing heaped-up accumulation of epithelium | Psoriasis, eczema, fungal infection, seborrheic dermatitis |
| Crust | Scab with dried serum, blood, or pus | Inflammatory or infectious skin diseases |
| Erosion | Superficial loss and depressed area of epidermis | Inflammatory or infectious skin diseases, trauma (friction or pressure), chemical burn |
| Ulcer | Deep loss and depressed area of epidermis and dermis | Venous stasis dermatitis, infections, vasculitis, decubitus (pressure) ulcer, peripheral arterial disease, burns, pyoderma gangrenosum |
| Excoriation | Traumatized, linear or wedge-shaped erosion as a result of scratching, rubbing, and picking | Swimmer’s itch, atopic dermatitis, neurotic excoriations |
| Fissure | Linear crack in skin, which extends into the dermis | Angular cheilitis, hyperkeratotic disorders, asteatotic eczema |
| Lichenification | Thickened area of epidermis with accentuated normal skin markings | Atopic dermatitis, scabies, lichen simplex chronicus |
| Atrophy | Thinning of the skin with resultant loss of hair and sweat glands | Chronic sun exposure, aging, cutaneous T-cell lymphoma, lupus erythematosus, a result of long-term potent topical corticosteroids |
| Others: scar, keloid, eschar, vegetating | ||
| COLOR | ||
| Erythema | Blanchable redness | |
| Petechiae/purpura/ecchymosis | Non-blanchable, deep red to purple color of varying sizes | |
| Hyperpigmentation | Darkening of skin color | |
| Hypopigmentation | Lightening of skin color | |
| Other: brown, black, grey, blue, yellow, fawn, orange | ||
| MORPHOLOGY (DESCRIPTIVE TERMS DESCRIBING PATTERNS AND/OR DISTRIBUTION OF SKIN LESIONS) | ||
| Reticular | Net-like arrangement | |
| Linear | In a line or band-like | |
| Herpetiform | Clustered or grouped | |
| Annular | Ring-shaped with central clearing | |
| Dermatomal | Following skin lines | |
| Serpiginous | Linear, branched, and curved elements like the track of a snake | |
| Nummular or discoid | Circular or coin-like | |
| Others: discrete, confluent, follicular, guttate, targetoid, scarlantiform, morbiliform, satellite lesions | ||
In recent years, many dermatologists have integrated dermoscopy, also known as epiluminescene microscopy, into the skin exam because dermatoscopes have become more accessible and mobile; there are even attachments available for smart phones. Through magnification and illumination, the dermatoscope enables the physician to see lesions more clearly and has been shown to improve the diagnostic accuracy of pigmented lesions such as melanoma in trained physicians.4,5 Physicians may also use in vivo reflectance confocal microscopy to visualize lesions at a cellular level to allow for more accurate identification of skin lesions, including lentigo maligna, pigmented macules, and melanoma.6
Another important aspect of the skin examination is body mapping, which enables physicians and patients to detect and follow skin lesions over time. Physicians can record skin lesions on paper printed with specifically designed human figures that allow for clear and methodical record keeping. The American Academy of Dermatology and the Skin Cancer Foundation provide detailed patient-focused literature that educates and enables patients to do similar skin lesion mapping at home.7 In addition to these bodymapping techniques, computerized body mapping technology using cameras and technical programs are becoming a more popular method to track moles over time. This process, which is cleverly termed “mole mapping,” enables a physician to document moles and skin lesions across the whole skin surface of a patient and track changes via digital photographs rather than relying on memory alone or paper markings. The potential benefits of this new technology is vast, but the required training, expense, and time limits wide adoption.8 Many clinics with well-trained subspecialized dermatologists whose practices are focused on this practice have emerged over recent years and are particulary helpful for patients at high-risk for melanoma.
In competitive athletes, skin disorders may manifest with a particular pattern or in a specific location, and early recognition is important for diagnosis and treatment. Regardless of the sport, these dermatological disease entities are often multifactorial and identification will require a perceptive physician. For certain diseases, the physician may play a role in deciding whether it is safe for the athlete to begin or return to play.
RETURN TO PLAY GUIDELINES
Dermatologists play a vital role in diagnosing and treating skin diseases in the general patient population, but play an even more critical role in the treatment of athletes because proper diagnosis, treatment, and management are crucial for prevention of spread to teammates.9 Refer to the National Federation of State High School Associations (NFHS) and National Collegiate Athletic Association (NCAA) return-to-play guidelines for detailed recommendations on the care and prevention of skin diseases in athletes.10,11 Generally, before an athlete should return to play, skin conditions should be properly covered to prevent spread, the athlete should have no systemic symptoms for more than 72 hours, there should be no active or oozing lesions present, and the athlete should follow the recommended medication regimen. These guidelines are minimum requirements and physicians should continue treatment even after the athlete has returned to play and until complete clearance. Most of the return-to-play guidelines refer to the treatment of infections diseases for which Part 2 of this review will cover in full detail.
TRAUMATIC OR MECHANICAL INJURIES
Friction blisters. Friction blisters commonly occur in competitive athletes as a result of multiple frictional forces acting on an involved skin area (Figure 1). With a greater frictional force, fewer cycles of rubbing against the skin are needed to produce skin disruption. Erythema followed by pallor develops with associated stinging, burning, and pain leading to vesicles or bullae. Factors that contribute to the formation of blisters include heat, moisture, poorly fitting shoes, and excessive or unusual exercises early in training.12,13 A hot, humid environment found in the inside of an athlete’s shoe or glove and increased skin hydration from excessive sweating or occlusion causes a change in the skin’s protective barrier function. These multiple factors can lead to skin softening and increased risk of blister development. Blisters were the most common complaint of marathon runners with an incidence of 0.2 to 39 percent in surveys taken from 1973 to 1994.14 The most commonly affected sites include the tips of the toes, balls of the feet, and the posterior heel.
Figure 1.

Friction blister. Discrete bullae formation at the site of irritation in an athlete with poorly fitted shoes
Measures used to prevent blister formation are wearing highly absorbent socks or layering socks of differing materials, using drying powders or other antiperspirant agents, applying petrolatum jelly, hardening the skin with 10% tannic acid soaks, and wearing properly fitted shoes or gloves.15 A double-blind study performed by Herring and Richie in 199016 investigated the blistering effect of 100% acrylic versus 100% cotton socks in long-distance runners and found that fewer and smaller blisters occurred with 100% acrylic socks. For patients with excessive hand or foot sweating, treatments can be utilized to decrease perspiration, including topical and oral anticholinergic agents, topical 20% aluminum chloride, iontophoresis, and botulinum toxin injections. In a double-blind trial in which military cadets applied either an antiperspirant containing 20% aluminum chloride or a placebo to their feet for at least three nights before a long hike, the rate of foot blisters in the group using the antiperspirant was only 21 percent compared with 48 percent in the placebo group. However, the cadets who used the antiperspirant were significantly more likely to experience foot irritation.17,18
Friction blisters create localized discomfort, but should be taken seriously as secondary impetigo can become a serious complication with potential cellulitis, osteomyelitis, and sepsis if left untreated. The correct management includes a sterile drainage of the site with an 11-blade while leaving the blister roof intact to serve as a natural dressing, thus relieving discomfort and protecting the site from superinfection.19 Treat the site as an open wound with appropriate antiseptic and surgical bandage application. The affected area will rarely need antibiotic ointment or specialized bandages, but may benefit from a petrolatum covering. The athlete may return to activity immediately once the pain has resolved, but should be monitored closely for possible infectious complications.
Calluses and corns. Calluses and corns (clavi) are thickened skin areas that represent a protective reaction pattern to chronic and repetitive friction commonly over bony prominences of the feet and toes.20 They are often seen in competitive athletes as well as those exposed to uneven friction from footwear, gait abnormalities, or high activity level.21 The most common sites are on the hands and feet (Figure 2). Corns are often misdiagnosed as calluses, which are also thickened skin lesions resulting from excess friction.22 Most corns are firm, dry, and tender with a shiny polished surface. If the upper layers are pared away, a small, 1 to 2mm translucent central core may be seen within the base of the lesion.23 Calluses lack this central core, which is characteristically revealed upon the removal of a corn.
Figure 2.

Callus. Hyperkeratotic or thickened, asymptomatic plaque of the big toe
Corns frequently restrict an athlete from competing at maximum intensity due to the associated tenderness and inflammation where calluses are often painless and considered desirable for some competitive activities, such as gymnastics, weightlifting, or racket sports.15 A full examination should include assessment of the types of gloves and footwear worn, activities performed, gait, and complete past medical history. Lesions should be palpated and pared to look for underlying blood vessels (black dots or pinpoint bleeding seen in warts) or skin markings (dermatoglyphics not seen in warts). Treatment generally consists of debridement of the lesions by either surgical (paring or laser) or medical methods (good foot hygiene, warm water soaks, keratolytics, topical retinoids, topical or intralesional corticosteroids, topical catharidin, and/or synthetic filler injections).24-26 Bevans et al27 examined 59 subjects in a randomized control trial comparing hard corn treatment by electrosurgery with standard sharp debridement and found that electrosurgery more effectively cured treatment-resistant hard corns. Treatment is initially aimed at reducing pain and inflammation, after which the underlying cause of callus or corn formation should be addressed.
Knuckle pads and athlete’s nodules (collagenomas). Knuckle pads are distinct callosities that can develop over the knuckles in particular professional occupations or hobby sports. Knuckle pads are benign, asymptomatic, well-circumscribed, smooth, firm, skin-colored papules, nodules, or plaques (Figure 3). They most commonly occur on the dorsal aspect of the proximal interphalangeal joint of the finger, but also may occur on the dorsal aspects of the foot over joints.28 Knuckle pads due to boxing are extremely common although seldom reported in the literature.29 One case highlighted a 21-year-old man who developed painful hyperkeratotic, fissured, callosities on his knuckles after having boxed for five evenings a week for six months.30 Knuckle pads have elsewhere been identified as a result of other occupation hazards (live-chicken hangers or manual tool operators) from various professions, trades, and hobbies.31 Dickens et al28 reported an unusual case of acquired pads of the feet caused by the use of sporting equipment for which they named sports-related pads.
Figure 3.

Knuckle pads. Asymptomatic, well-circumscribed, smooth, firm, skin-colored papules and plaques over the dorsal aspects of the foot
Regardless of the nomenclature, these entities are all similar and treatment consists of removing the eliciting factors.
Athlete’s nodules are small, asymptomatic, flesh-colored nodules on the dorsum of the feet, knees, or knuckles as a result of recurrent pressure, trauma, and friction. The term “athlete’s nodule” is a general term referring to a hyperplastic and reactive dermatosis in various athletes. These are common in surfers, boxers, and football and hockey players and are accompanied by thickening of the overlying epidermis.32,33 Boxers typically develop athlete’s nodules on the knuckles although have the susceptibility for lesions to develop on the feet or toes. The majority of these nodules result from recurrent friction; others result from granulomatous reaction to material embedded within the skin. Cohen et al32 described athlete’s nodules on the dorsum of a middle-aged man’s feet as a result of tight-fitting athletic shoes he wore as a younger athlete. Microscopic examination revealed an increase in collagen bundles in the reticular dermis resembling connective tissue nevi of collagen type. They speculated these collagenomas, or athlete’s nodules, were the result of recurrent trauma to the dorsum of the foot from athletic shoes. The same process can occur in other athletes as a result of trauma; however, most authors resist separately naming all clinically similar nodules found in athletes as “athlete’s nodules.”
Neither medical nor surgical interventions for knuckle pads or athlete’s nodules are very effective.34 Eliminating the source of mechanical or repetitive trauma may improve the lesions and wearing protective gloves or changing occupation may be all that is required.35 Intralesional injections of corticosteroids may reduce the size of the lesions. A cast or splint placed temporarily on the involved areas of the hand may aid in reducing the lesion. Applications of keratolytics, such as salicylic acid or urea, can help to soften and reduce the lesion size. Surgical intervention or ablative laser therapy may be indicated if these entities cause a functional problem, although recurrence or scar formation following surgery is likely.
Piezogenic papules (cutaneous hernia). Piezogenic papules are multiple, small (1 to 5mm), skin- or yellow-colored, painless papules found in weight-bearing areas, such as on the lateral, posterior, or medical surface of the heel36 (Figure 4). They are a result of subdermal fat herniation and are most noticeable when pressure is applied to the affected area or after prolonged exercise or standing.37 Zaidi et al38 examined 100 people for piezogenic papules and identified both pedal and wrist papules with most being bilateral and multiple. Although most often found in long-distance runners, piezogenic papules may be found in other athletes participating in sports, such as boxing or gymnastics, where constant pressure around the hand may cause subdermal fat herniation on the wrist or palm.39,40 No specific treatment has shown to be of complete benefit for piezogenic papules. Multiple treatment modalities have been tried with varying degrees of success, such as injectable corticosteroids and anesthetic agents, compression, electro-acupuncture, and heel cup or pad inserts into the athlete’s shoe.41-43 Injectable fillers, such as calcium hydroxyl-apatite or silicone, can sometimes help curb the pressure put on the heel or wrist during intense exercise or to treat the associated pain.
Figure 4.

Piezogenic papules. Asymptomatic, compressible, skin-colored to yellow papules of the posterior heel as a result of increased heel pressure from sporting activities
Black heel (talon noir or calcaneal petechiae) and black palm (tache noir). Black heel is a self-limited, asymptomatic, trauma-induced lesional darkening of the posterolateral aspect of the heel24-44 (Figure 5). Black heel is seen almost exclusively in adolescents or young adults engaged in active sports, especially basket-ball, football, lacrosse, and tennis, as these are sports associated with frequent quick starts and stops.45 However, any sport that induces sheering or pinching stress from the abrupt contact of the foot with the floor or hard ground can induce these lesions with multiple variants. It is caused by hemorrhage in a location where blood vessels are minimally protected by fatty tissue, such as at the upper edge of the calcaneal fat-pad.46 Urbina et al47 described a series of six patients with superficial cutaneous hemorrhages that they considered atypical variants of black heel seen with burns from hot sand, friction against the rough edge of a swimming pool, wearing of new shoes, jogging, and picking of a blister with a needle.47 They suggested a new term labeled “post-traumatic cutaneous intracorneal blood” to describe black heel and its diverse clinical presentations on the heel. Often the lesion is asymptomatic, thus may be disregarded or only observed by chance (Figure 6). Clinically, it may be confused with malignant melanoma and should be investigated when discovered.48 Hemoccult card testing can confirm blood and give reassurance. A similar lesion termed black palm (tache noir) has been described on the thenar eminence in weightlifters, gymnasts, golfers, tennis players, mogul skiers, and mountain climbers, as these athletes apply pressure to their hands.49,50 Black heel and palm are harmless and heal with time. Involution of the lesion occurs in a few weeks from time of onset and should not restrict an athlete from participation in sports.
Figure 5.
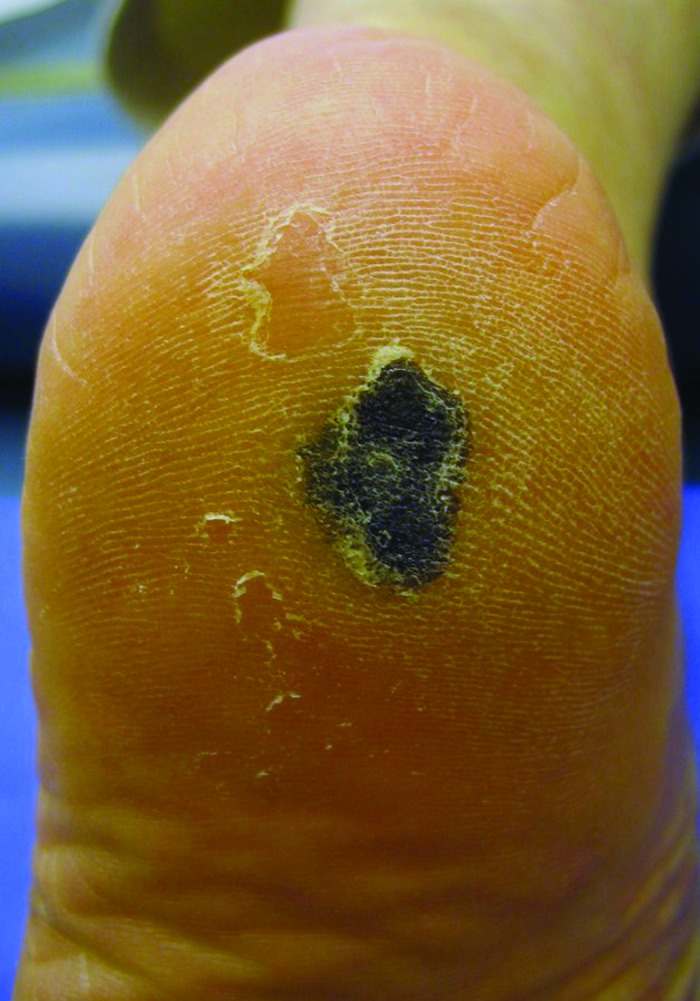
Talon noir. Asymptomatic, trauma-induced, dark plaque of the heel that occurs predominantly in young adult athletes and clinically resembles malignant melanoma
Figure 6.

Digital hemorrhage. Black discoloration secondary to trauma representative of hemorrhage on the index finger of a patient that clinically resembles malignant melanoma
Erythema ab igne. Erythema ab igne (EAI) is a skin condition that results from chronic exposure to a heat source (Figure 7). EAI results in persistent, reticulate or lacy-like, erythematous patches often with telangiectasias and hypo- or hyperpigmentation in areas exposed to excess external heat sources.51,52 In athletes, these sources may commonly be heating pads, hot water bottles, hot showers, hot baths or whirlpools, hot stone massages, sauna and steam rooms, and heated recliners, especially in those treated for muscle or joint aches or pains. The diagnosis is clinical and straightforward for those who recognize this entity, but a referral to a dermatologist may be necessary in cases where the diagnosis is uncertain. In chronic cases, topical lightening agents and/or laser therapy may help the pigmentary changes. Malignant transformation is a possible sequelae of EAI; squamous cell carcinoma (SCC), merkel cell carcinoma, and cutaneous marginal zone lymphoma have been reported to arise from EAI. Sigmon et al53 reported a case of poorly differentiated carcinoma arising in an EAI lesion on a 92-year-old female with a history of sitting in front of wood-burning stoves as a child. Due to this malignant potential, it is important to readily diagnose lesions, discontinue offending heat exposure, follow the lesion over time, and biopsy suspicious lesions.
Figure 7.

Erythema ab igne. Reticulated, hyperpigmented patches over the trunk secondary to exposure of an external heating source (a heating pad)
INFLAMMATORY CONDITIONS
Contact dermatitis. Contact dermatitis is any inflammatory reaction of the skin that results from direct contact with an offending agent. Athletes represent a unique population of patients who are frequently exposed to various allergens and chemicals on top of repeated exposure to trauma, heat, and moisture that can precipitate the dermatitis. Recognizing the unique environmental irritants and allergens encountered by athletes is paramount to facilitate appropriate therapy and prevention. Allergic contact dermatitis (ACD) typically affects individuals previously sensitized to the substance and represents a delayed-type hypersensitivity reaction, which demonstrates a lag-interval of several hours to days from the initiation of the immunological cascade and the manifestation of symptoms. On the other hand, irritant contact dermatitis (ICD) results from direct injury to the skin seconds to minutes after exposure and does not involve the immune system cascades, thus it affects any athlete directly exposed to specific irritants and often produces symptoms.
The hazards of equipment, topical medications, and flora in the playing field put the athlete at a unique risk for developing contact dermatitis.54 ACD has been demonstrated in athletes from equipment, such as athletic shoes or gloves, wet-suits, goggles and underwater masks, swim caps, adhesives for athletic tape, swimming pool water, knee and shin pads, metal weights and bars, topical antibiotics and anti-inflammatory creams (Figure 8). ICD has been demonstrated from clothing, basketballs, hockey sticks, rafts and boards, pool water, chalk, seaweed and coral, and hair.25 ICD is often initiated by friction and sweat, surface of various equipment, repeated wetting and drying, and chemicals used to disinfect water or equipment or line field markings.55 ICD has various vernacular terms, such as baseball pitcher’s friction dermatitis, jogger’s nipples, pool water and seaweed dermatitis, surf rider’s dermatitis, basketball pebble fingers, cement hand dermatitis, and canyoning hand. Kockentiet and Adams56 comprehensively reviewed the literature on contact dermatitis in athletes and included all forms of contact dermatitis classified under sport-specific subheadings defined in the literature. They demonstrated that both land and water sports have been extensively shown to cause contact dermatitis with the common offenses coming from materials found in protective athletic gear. Many culprits exist and are sports-specific to the protective equipment used and environment to which the athlete is exposed.
Figure 8.

Contact dermatitis. Localized, well-demarcated, erythematous, lichenified plaques over the dorsal aspect of the bilateral feet in a patient with contact allergy to shoe antigen components
The diagnosis of contact dermatitis is often evident from the patient’s history and characteristic clinical findings, such as erythematous and pruritic plaques often associated with fluid-filled vesicles and/or bullae and edema. The skin lesions are often sharply demarcated and located in the distribution of the area of contact or exposure. Subacute or chronic lesions may demonstrate papules instead of vesicles or bullae and scaling, fissuring, lichenification, or excoriations with crusting.57 Patch testing can help identify the allergen and confirm the diagnosis. Topical or systemic corticosteroids and antihistamines are the mainstay of treatment. Topical or oral antibiotics may be required in cases of secondary infection. Topical soaks with cool tap water, Burrow’s solution, or silver nitrate solution are soothing and have an antipruritic and antiseptic affect. In severe or chronic cases, topical emollients and barrier creams as well as oral immunosuppressives such as cyclosporine or methotrexate can help. Topical calcineurin inhibitors may be beneficial in patients who cannot tolerate topical corticosteroids or the disease location is in a sensitive skin area such as the skin folds or face/neck. It is important to advise patients to avoid direct skin contact with the allergenic material and to investigate companies that make athletic equipment with alternative agents for those who are allergic. As long as the affected eczematous areas are not secondarily infected, the athletes should not be restricted from play.
Sunburn and sun-related conditions. Patient education about the risks and consequences of excessive sun exposure is key in the prevention of acute sunburn, premalignant skin changes including actinic keratosis, cancer including melanoma, SCC, and basal cell carcinoma (BCC), and cosmetic skin changes including wrinkles and solar lentigines. Although pain and irritation due to severe sunburn itself can prevent an athlete from participating in a sport, sun exposure prevention is most valuable for its prevention of cancer. Physicians have the most impact through education and promotion of sun-protective habits that can prevent the sun exposure in the first place. This education and awareness is critical when treating and advising athletes in sports that involve sun exposure. The environment an athlete performs in can also increase the amount of ultraviolet (UV) radiation exposure due to how the light reflects and bends when it hits sweat, water, or snow. Skin hydration, especially in the stratum corneum, increases the photosensitivity to UV rays and shifts the wavelength that is best absorbed to the more dangerous shorter wavelength light rays.58
A review article about skin conditions in baseball, cricket, and softball players recommends that athletes wear sun-protective clothing and waterproof sunscreen with broad spectrum protection against UVA (longer wavelength) and UVB (shorter wavelength) rays of at least 30 sun protective factors (SPF) applied every two hours per the American Academy of Dermatology recommendations.59 A review article about skin conditions in long distance runners recommends that sunscreen should be applied 30 minutes before activity to allow for absorption into the stratum corneum to decrease the amount washed away by sweat or water.6C Regular full body skin examinations, as mentioned earlier, are especially important for outdoor athletes in the detection of lentigines, freckles, moles, and malignancies.
In addition to protective clothing and sunscreen, which can be a hassle and is underused by many athletes, there are new tools being developed for sun protection. Polypodium leucotomos (PL), a fern extract, has been reported as a treatment of numerous skin conditions, such as vitiligo, melasma, psoriasis, and atopic dermatitis, because of its protective UV radiation properties. Choudhry et al published a review article summarizing the various uses of PL, including the photoprotective activity, which, if taken orally as a 240mg capsule every morning and 2 to 3 hours prior to extended sun exposure, provides full-body sun protection and anti-aging benefits.61 Extracts of PL are marketed commercially as Heliocare (Ferndale Healthcare, Ferndale, Michigan) and Fernblock (Life Extention, Fort Lauderdale, Florida). When used orally, these products allow PL to function as an antioxidant to prevent deoxyribonucleic acid (DNA) damage and mutagenesis and it also has anti-inflammatory, anti-tumor, and anti-aging functionality.62 Rodriguez-Yanes et aP found that PL when given to hairless mice before UVB/UVA lamp irradiation delayed cutaneous tumorigenesis, diminished actinic keratosis formation in non-tumoral skin, and increased the numbers of cells expressing the tumor suppressor p53. It is still recommended to use topical sunscreen along side any topical or oral PL extract.
EXACERBATION OF PRE-EXISTING DERMATOSES
Acne mechanica (sports-induced acne). Acne mechanica (AM) is a papulopustular eruption that simulates acne vulgaris, but is caused primarily by a combination of pressure, occlusion, friction, and/or heat.24,64 Stress on the skin appears to be the key element in AM rather than the inflammation and hyperkeratinization of the pilosebaceous unit seen in acne vulgaris. It is most often seen on the chin, jawline, forehead, neck, or shoulders, and is characteristic for occurring predominantly beneath heavy protective equipment.54 The most common sports associated with this condition are those that use body or head gear, such as football, hockey, and lacrosse.65 AM may occur in other instances, such as beneath protective padding in boxers or equestrian riders (chin or forehead), wrestlers (knee), or in orthopedic patients using crutches (axillae).66 For acne presenting in an abnormal distribution and that does not resolve with standard therapeutic interventions, other investigations may be needed to rule out a hormonal or fungal cause.
Treatment is more difficult than typical acne vulgaris.67 The most important management strategy is prevention, such as wearing moisture-wicking clothing or clean absorbent cotton shirts underneath any sport equipment and frequent diligent cleansing of the skin following any intense physical activity. Medical treatment is similar to other forms of acne using topical or systemic antibiotics, topical benzoyl peroxide, topical and systemic retinoids, and injectable corticosteroids. Other agents may also be of benefit, such as keratolytics (salicylic acid), chemical peels (glycolic, trichloroacetic acid, or resorcinol combination), topical azelaic acid, or topical sulfur preparations.68 Newer treatment modalities used to treat refractory acne vulgaris, such as photodynamic therapy, intense pulsed light therapy, fractionated nonablative lasers, or topical dapsone may be of benefit in recalcitrant cases. A unique variant of AM termed acne keloidalis nuchae has been described in football players with severe cases the occiput.69 In 2011, Beckett et al70 published a case report of acne keloidalis nuchae successfully treated by electrosurgical excision with second intention healing. The use of laser hair removal, microneedling, and nonablative lasers, alone or in combination, have been effective for the author’s (JE) patients. No sports restrictions exist regarding AM.
Cholinergic urticaria and exercise-induced anaphylaxis. Changes in body temperature and sweating are common in the participation of sports and these two distinct dermatological entities are related to the body’s ability to initiate a sympathetic response during a workout. Cholinergic urticaria (hives) is one of the physical urticarias brought on by the stimulus of sweating, although some consider it to be secondary to the elevated body temperature (heat) of the athlete. Urticaria (hives) is clinically characterized by well-defined, edematous, and erythematous plaques of varying sizes, which typically resolve within hours (Figure 9). Urticaria is classified into various varieties depending on the stimulus (cholinergic, cold, solar, pressure, and aquagenic) and many patients may have a combination.71 These patients present with itching, burning, tingling, warmth, or irritation that precedes the onset of numerous small (l-4mm in diameter) pruritic wheals with large surrounding flares. Wheals can occur anywhere in the body except for the palms and soles, and rarely the axillae. Skin lesions frequently resolve after removal of the eliciting factor. Treatment includes rapid cooling, systemic antihistamines or leukotriene antagonists or corticosteroids, immunotherapy with anti-immuno-globulin E (omalizumab), danazol, or in severe cases the use of cyclosporine, mycophenolate mofetil, or methotrexate.72-75 Patients with cholinergic urticaria should avoid the precipitating factors including exercise and any activity that causes sweating, such as elevated environmental temperature, hot food, sauna baths, immersion in hot water, emotional stress, and hemodialysis, because these can precipitate a cholinergic urticaria attack in some patients. Beyond avoidance of the precipitating factor, in 2011, Kozaru et al reported original research finding successful rapid desensitization to sweat after autologous sweat treatment.76
Figure 9.

Cholinergic urticaria. Itching and burning preceding the onset of numerous small wheals with large surrounding flares on the torso of a patient
A severe form of urticaria exacerbated by athletic activity is exercise-induced anaphylaxis (EIA), which commonly occurs in atopic or food allergy patients who are also well-conditioned athletes. It develops shortly after exercise with cutaneous pruritus, erythema, urticaria and then progresses to include angioedema, respiratory distress, gastrointestinal symptoms (nausea, diarrhea, vomiting) and possible vascular collapse.77 Multiple mechanisms have been suggested, including histamine and complement mediated pathways.78 In a large retrospective study of cases of EIA, 78 percent of participants noted that running induced their lesions. Subjects reduced their attacks by avoiding exercise during extremely hot or cold weather (44%), avoiding ingestion of certain foods before exercise (37%), and restricting exercise during their allergy season (36%) or humid weather (33%).79 Treatment of an acute episode of EIA includes the same used for any anaphylactic episode (fluids, epinephrine, beta-agonists, antihistamines, and corticosteroids), but prevention is the most important measure.80,81 Athletes can reduce their chance of EIA by avoiding exercise in extremely hot, humid, or cold weather as well as learning to avoid the use of certain medications (aspirin and nonsteroidal anti-inflammatory drugs) and foods (wheat, vegetables, and crustaceans) that could potentiate an attack.82
Physical intertrigo. Intertrigo is an inflammatory condition of skin folds that is induced by mechanical factors, such as friction from skin-to-skin rubbing and aggravated by heat, moisture, and infection. Opposing skin surfaces that consistently rub can cause inflammation with resulting maceration and erosion.83 The condition frequently is worsened by secondary infection of colonized bacterial, fungal, or viral agents. Intertrigo typically affects the intertriginous areas, such as the groin, axillae, inframammary and abdominal folds, and the web spaces of fingers and toes. Intertrigo characteristically presents chronically with an insidious onset of symptoms, such as itching, burning, and stinging that, with repetitive rubbing, leads to erythema and inflammation. This inflammation may progress to maceration, erosion, and fissuring with resulting weeping and crusting of the skin folds that is extremely painful and may herald infection84 (Figure 10). Intertrigo is often confused with other skin disorders that are caused by a wide variety of inflammatory, infectious, metabolic, and malignant causes. The diagnosis is obtained clinically; however, potassium hydroxide (KOH) preparation can help to rule out fungal causes, a wood’s lamp examination and culture of skin scrapings can help to diagnose bacterial etiologies, and skin biopsy can be used to rule out malignant suspicions or to diagnose pemphigus or psoriatic disease.85,86
Figure 10.

Intertrigo. Erythema and weeping that progressed to maceration and crusting with secondary infection in an abdominal fold
The primary treatment for intertrigo is preventative to eliminate friction, heat, and maceration by taking precautions to keep the skin folds cool and dry.87,88 Patients should wear light, nonocclusive, highly absorbent clothing, such as cotton or linen, and avoid wool and synthetic fibers that could induce chafing. Topical antifungal medications are helpful, especially if used with a low-dosage topical corticosteroid or topical calcineurin inhibitor for a short duration as these medications help to decrease inflammation and associated pruritus.89 The use of more potent topical corticosteroids should be avoided because the occlusive effect of skin folds can accelerate the development of skin atrophy, striae, and telangiectasias, which are frequent side effects of potent topical steroids used in thin skin locations.90 After completion of an appropriate course of topical therapy, patients should use a drying agent, such as an antifungal or talc powder, to help maintain a dry environment and minimize the risk of maceration and reinfection. Patients at high risk of recurrence should use a drying agent on an ongoing basis. Castellani paint (carbol-fuchsin paint), a first aid antiseptic and antifungal drying agent, can also be helpful. Formulations combining protective/barrier agents, antimicrobials, and topical steroids, such as Triple Paste (petrolatum, zinc oxide, lanolin, and beeswax), Greer’s Goo (nystatin, hydrocortisone, and zinc oxide), and Desitin (zinc oxide, aloe, and vitamin E) are of benefit. Botulinum toxin has been used to treat intertrigo in a patient with Darter’s disease and inguinal hyperhidrosis.91 Newer medicated devices and/or barrier creams such as Eletone, Atopiclair, MimyX, and Tetrix have been shown to benefit various forms of inflammation such as eczema and may also help for intertrigo, but are currently only available by prescription and are more expensive than over-the-counter creams.
CONCLUSION
Sports dermatology is a growing field that continues to identify common as well as unique and interesting sports-related skin conditions. Athletes are a distinct group of patients whose activities place them at high risk for dermatological disease. Repetitive physical activity along with environmental stressors places the athlete at high risk for acquisition or exacerbation of various sports-related dermatologic conditions. Part 1 of this two-part series focused on traumatic injuries, inflammatory conditions, and exacerbation of pre-existing dermatoses. Part 2 will focus on infections and infestations as well as the dermatological effects of anabolic steroids (Table 2). The authors’ goal with this review is to arm physicians with the fundamental knowledge of skin diseases in athletes. Failure to acknowledge the role of sports participation in the pathogenesis of skin disease can lead to delayed diagnosis and incorrect treatment and cause unnecessary participation restriction.
TABLE 2.
Dermatoses associated with close contact sports
| PART 1: TRAUMATIC OR MECHANICAL |
| Friction blisters Calluses and corns Knuckle pads and athlete’s nodules Piezogenic pedal papules (cutaneous hernia) Black heel (talon noir or calcaneal petechiae) and black palm (tache noir) Erythema ab igne |
| Inflammatory |
| Contact dermatitis Sunburn and sun-related conditions |
| Exacerbation of pre-existing dermatoses |
| Acne mechanica (sports-induced acne) and acne keloidalis nuchae Cholinergic urticaria and exercise-induced anaphylaxis Physical Intertrigo |
| PART 2: INFECTIONS, INFESTATIONS, AND ANABOLIC STEROIDS |
| Infections and infestations |
| Bacterial |
| Impetigo |
| Folliculitis, furuncles, and carbuncles |
| Pitted keratolysis |
| Erythrasma |
| Viral |
| Molluscum contagiosum |
| Verruca (warts) |
| Herpes (simplex, gladiatorum, rugbeiorum) |
| Fungal |
| Tinea pedis, cruris, capitits/kerion |
| Tinea corporis gladiatorum |
| Infestations |
| Scabies |
| Pediculosis (lice) |
Footnotes
DISCLOSURE:The authors report no relevant conflicts of interest.
REFERENCES
- 1.Schwarzenberger K. The essentials of the complete skin examination. Med Clin North Am. 1998;82:981–999. doi: 10.1016/s0025-7125(05)70401-6. [DOI] [PubMed] [Google Scholar]
- 2.Fenske NA, Cohen LE. The dermatologic exam. Emerg Med Clin North Am. 1985;3:643–658. [PubMed] [Google Scholar]
- 3.Joy EA, Paisley TS, Price R, Jr, et al. Optimizing the collegiate preparticipation physical evaluation. Clin J Sport Med. 2004;14:183–187. doi: 10.1097/00042752-200405000-00012. [DOI] [PubMed] [Google Scholar]
- 4.Argenziano G, Soyer HP, Chimenti S, et al. Dermoscopy of pigmented skin lesions: results of a consensus meeting via the Internet. J Am Acad Dermatol. 2003;48:679–693. doi: 10.1067/mjd.2003.281. [DOI] [PubMed] [Google Scholar]
- 5.Binder M, Schwarz M, Winkler A, et al. Epiluminescence microscopy: a useful tool for the diagnosis of pigmented lesions for formally trained dermatologists. Arch Dermatol. 1995;131:286–291. doi: 10.1001/archderm.131.3.286. [DOI] [PubMed] [Google Scholar]
- 6.Pellacani G, Guitera P, Longo C, et al. The impact of in vivo reflectance confocal microscopy for the diagnostic accuracy of melanoma and equivocal melanoytic lesions. J Invest Dermatol. 2007;127:2759–2765. doi: 10.1038/sj.jid.5700993. [DOI] [PubMed] [Google Scholar]
- 7.http://www.aad.org/File%20Library/Global%20navigation/For%20the%20public/aad-body-mole-map.pdf Detect Skin Cancer: Body Mole Mapping [Internet download]. American Academy of Dermatology’s SPOT Skin Cancer™ Campaign; 2013 [cited 2014 Jul 30].
- 8.Higgins HW, Lee KC, Jeffell DJ. Point of care cutaneous imaging technology in melanoma screening and mole mapping. FlOOOPrime Rep. 2014;6:34. doi: 10.12703/P6-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Likness LP. Common dermatologic infections in athletes and return-to-play guidelines. J Am Osteopath Assoc. 2011;111:373–379. doi: 10.7556/jaoa.2011.111.6.373. [DOI] [PubMed] [Google Scholar]
- 10.https://www.doe.kl2.de.us/infosuites/students_family/diaa/files/110410SportsRel_SkinInfect_PSGuide.pdf Sports Related Skin Infections Position Statement and Guidelines. [Internet download]. National Federation of State High School Associations, Sports Medicine Advisory Committee. Indianapolis, IN: National Federation of State High School Associations; [updated 2010 April; cited 2014 Sep 2].
- 11.National Collegiate Athletic Association Sports Medicine Handbook. 22nd ed. Indianapolis, IN: National Collegiate Athletic Association; 2011. pp. 59–65. National Collegiate Athletic Association Guideline 2j: Skin infections in athletics. [Google Scholar]
- 12.Helm TN, Bergfeld WF. Sports dermatology. Clin Dermatol. 1998;16:159–165. doi: 10.1016/s0738-081x(97)00178-8. [DOI] [PubMed] [Google Scholar]
- 13.Freiman A, Barankin B, Elpern DJ. Sports dermatology part 1: common dermatoses. CMAJ. 2004;171:851–853. doi: 10.1503/cmaj.1041143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mailler EA, Adams BB. The wear and tear of 26.2: dermatological injuries reported on marathon day. Br J Sports Med. 2004;38:498–501. doi: 10.1136/bjsm.2004.011874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Adams BB. Sports dermatology. Adolesc Med. 2001;12:vii, 305–322. [PubMed] [Google Scholar]
- 16.Herring KM, Richie DH., Jr. Friction blisters and sock fiber composition. A double-blind study. J Am Podiatr Med Assoc. 1990;80:63–71. doi: 10.7547/87507315-80-2-63. [DOI] [PubMed] [Google Scholar]
- 17.Knapik JJ, Reynolds K, Barson J. Influence of an antiperspirant on foot blister incidence during cross-country hiking. J Am Acad Dermatol. 1998;39(2 Pt l):202–206. doi: 10.1016/s0190-9622(98)70075-1. [DOI] [PubMed] [Google Scholar]
- 18.Reynolds K, Darrigrand A, Roberts D, et al. Effects of an antiperspirant with emollients on foot-sweat accumulation and blister formation while walking in the heat. J Am Acad Dermatol. 1995;33:626–630. doi: 10.1016/0190-9622(95)91283-5. [DOI] [PubMed] [Google Scholar]
- 19.Brennan FH., Jr. Managing blisters in competitive athletes. Curr Sports Med Rep. 2002;1:319–322. doi: 10.1249/00149619-200212000-00003. [DOI] [PubMed] [Google Scholar]
- 20.Singh D, Bentley G, Trevino SG. Callosities, corns, and calluses. BMJ. 1996;312:1403–1406. doi: 10.1136/bmj.312.7043.1403a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bergfeld WF. Dermatologic problems in athletes. Clin Sports Med. 1982;1:419–430. [PubMed] [Google Scholar]
- 22.Houston SD, Knox JM. Skin problems related to sports and recreational activities. Cutis. 1977;19:487–491. [PubMed] [Google Scholar]
- 23.Richards RN. Calluses, corns, and shoes. Semin Dermatol. 1991;10:112–114. [PubMed] [Google Scholar]
- 24.Pharis DB, Teller C, Wolf JE., Jr. Cutaneous manifestations of sports participation. J Am Acad Dermatol. 1997;36(3 Pt l):448–459. doi: 10.1016/s0190-9622(97)80225-3. [DOI] [PubMed] [Google Scholar]
- 25.Cordoro KM, Ganz JE. Training room management of medical conditions: sports dermatology. Clin Sports Med. 2005;24 doi: 10.1016/j.csm.2005.03.008. 565-598, viii-ix. [DOI] [PubMed] [Google Scholar]
- 26.Balkin SW. Injectable silicone and the foot: a 41-year clinical and histologic history. Dermatol Surg. 2005;31(11 Pt 2):1555–1559. doi: 10.2310/6350.2005.31241. discussion 1560. [DOI] [PubMed] [Google Scholar]
- 27.Bevans JS, Bosson G. A comparison of electrosurgery and sharp debridement in the treatment of chronic neurovascular, neurofibrous and hard corns. A pragmatic randomized controlled trial. Foot (Edinb). 2010;20:12–17. doi: 10.1016/j.foot.2010.03.003. [DOI] [PubMed] [Google Scholar]
- 28.Dickens R, Adams BB, Mutasim DF. Sports-related pads. Int J Dermatol. 2002;41:291–293. doi: 10.1046/j.1365-4362.2002.01356_3.x. [DOI] [PubMed] [Google Scholar]
- 29.Hame SL, Melone CP., Jr. Boxer’s knuckle. Traumatic disruption of the extensor hood. Hand Clin. 2000;16 375-380, viii. [PubMed] [Google Scholar]
- 30.Kanerva L. Knuckle pads from boxing. Eur J Dermatol. 1998;8:359–361. [PubMed] [Google Scholar]
- 31.Guberman D, Lichtenstein DA, Vardy DA. Knuckle pads—a forgotten skin condition: report of a case and review of the literature. Cutis. 1996;57:241–242. [PubMed] [Google Scholar]
- 32.Cohen PR, Eliezri YD, Silvers DN. Athlete’s nodules: sports-related connective tissue nevi of the collagen type (collagenomas) Cutis. 1992;50:131–135. [PubMed] [Google Scholar]
- 33.Cohen PR, Eliezri YD, Silvers DN. Athlete’s nodules. J Am Acad Dermatol. 1991;24(2 Pt 1):317–318. doi: 10.1016/s0190-9622(08)80631-7. [DOI] [PubMed] [Google Scholar]
- 34.Richards TB, Gamble JF, Castellan RM, Mathias CG. Knuckle pads in live-chicken hangers. Contact Dermatitis. 1987;17:13–16. doi: 10.1111/j.1600-0536.1987.tb02636.x. [DOI] [PubMed] [Google Scholar]
- 35.Muller SA. Dermatologic disorders in athletes. J Ky Med Assoc. 1976;74:225–228. [PubMed] [Google Scholar]
- 36.Redbord KP, Adams BB. Piezogenic pedal papules in a marathon runner. Clin J Sport Med. 2006;16:81–83. doi: 10.1097/01.jsm.0000180871.22426.60. [DOI] [PubMed] [Google Scholar]
- 37.Payton L. Multiple bumps seen on the heels. Piezogenic pedal papules. JAAPA. 2007;20:15. doi: 10.1097/01720610-200707000-00003. [DOI] [PubMed] [Google Scholar]
- 38.Zaidi Z, Jafri N, Noori B, Thawerani H. Piezogenic papules—a study of 100 cases. J Pak Med Assoc. 1995;45:93–94. [PubMed] [Google Scholar]
- 39.Cox NH, Broome G. Piezogenic palmar papules: a novel physical sign of palmar lipoma. Br J Dermatol. 2008;159:757–758. doi: 10.1111/j.1365-2133.2008.08724.x. [DOI] [PubMed] [Google Scholar]
- 40.Laing VB, Fleischer AB., Jr. Piezogenic wrist papules: a common and asymptomatic finding. J Am Acad Dermatol. 1991;24:415–417. doi: 10.1016/0190-9622(91)70062-7. [DOI] [PubMed] [Google Scholar]
- 41.Doukas DJ, Holmes J, Leonard JA. A nonsurgical approach to painful piezogenic pedal papules. Cutis. 2004;73:339–340. [PubMed] [Google Scholar]
- 42.Woodrow SL, Brereton-Smith G, Handfield-Jones S. Painful piezogenic pedal papules: response to local electro-acupuncture. Br J Dermatol. 1997;136:628–630. [PubMed] [Google Scholar]
- 43.Böni R, Dummer R. Compression therapy in painful piezogenic pedal papules. Arch Dermatol. 1996;132:127–128. doi: 10.1001/archderm.1996.03890260027003. [DOI] [PubMed] [Google Scholar]
- 44.Metelitsa A, Barankin B, Lin AN. Diagnosis of sports-related dermatoses. Int J Dermatol. 2004;43:113–119. doi: 10.1111/j.1365-4632.2004.02101.x. [DOI] [PubMed] [Google Scholar]
- 45.Wilkinson DS. Black heel a minor hazard of sport. Cutis. 1977;20:393–396. [PubMed] [Google Scholar]
- 46.Ayres S, Jr, Mihan R. Calcaneal petechiae. Arch Dermatol. 1972;106:262. [PubMed] [Google Scholar]
- 47.Urbina F, Leon L, Sudy E. Black heel, talon noir or calcaneal petechiae? Australas J Dermatol. 2008;49:148–151. doi: 10.1111/j.1440-0960.2008.00454.x. [DOI] [PubMed] [Google Scholar]
- 48.Verbov J. Calcaneal petechiae. Arch Dermatol. 1973;107:918. [PubMed] [Google Scholar]
- 49.YaffeeH. Talon noir. Arch Dermatol. 1971:104–452. doi: 10.1001/archderm.104.4.452b. [DOI] [PubMed] [Google Scholar]
- 50.Rashkovsky I, Safadi R, Zlotogorski A. Black palmar macules. Palmar petechiae (“black palm”) Arch Dermatol. 1998;134 doi: 10.1001/archderm.134.8.1019-b. 1020, 1023-1024. [DOI] [PubMed] [Google Scholar]
- 51.Dissemond J, Grabbe S. Erythema ab igne. Intern Med J. 2008;38:675. doi: 10.1111/j.1445-5994.2008.01751.x. [DOI] [PubMed] [Google Scholar]
- 52.Chan CC, Chiu HC. Images in clinical medicine. Erythema ab igne. N Engl J Med. 2007;356:e8. doi: 10.1056/NEJMicm055084. [DOI] [PubMed] [Google Scholar]
- 53.Sigmon JR, Cantrell J, Teague D, et al. Poorly differentiated carcinoma arising in the setting of erythema ab igne. Am J Dermatopathol. 2013;35:676–678. doi: 10.1097/DAD.0b013e3182871648. [DOI] [PubMed] [Google Scholar]
- 54.Adams BB. Dermatologic disorders of the athlete. Sports Med. 2002;32:309–321. doi: 10.2165/00007256-200232050-00003. [DOI] [PubMed] [Google Scholar]
- 55.Morris-Jones R, Robertson SJ, Ross JS, et al. Dermatitis caused by physical irritants. Br J Dermatol. 2002;147:270–275. doi: 10.1046/j.1365-2133.2002.04852.x. [DOI] [PubMed] [Google Scholar]
- 56.Kockentiet B, Adams BB. Contact dermatitis in athletes. J Am Acad Dermatol. 2007;56:1048–1055. doi: 10.1016/j.jaad.2006.12.025. [DOI] [PubMed] [Google Scholar]
- 57.Brooks C, Kujawska A, Patel D. Cutaneous allergic reactions induced by sporting activities. Sports Med. 2003;33:699–708. doi: 10.2165/00007256-200333090-00005. [DOI] [PubMed] [Google Scholar]
- 58.De Luca JF, Adams BB, Yosipovitch G. Skin manifestations of athletes competing in the summer Olympics: what a sports medicine physician should know. Sports Med. 2012;42:399–413. doi: 10.2165/11599050-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 59.Farhadian JA, Tlougan BE, Adams BB, et al. Skin conditions of baseball, cricket, and Softball players. Sports Med. 2013;43:575–589. doi: 10.1007/s40279-013-0022-4. [DOI] [PubMed] [Google Scholar]
- 60.Helm MF, Helm TN, Bergfeld WF. Skin problems in the longdistance runner 2500 years after the Battle of Marathon. Int J Dermatol. 2012;51:263–270. doi: 10.1111/j.1365-4632.2011.05183.x. [DOI] [PubMed] [Google Scholar]
- 61.Choudhry SZ, Bhatia N, Ceilley R, et al. Role of oral Polypodium leucotomos extract in dermatologic diseases: a review of the literature. J Drugs Dermatol. 2014;13:148–153. [PubMed] [Google Scholar]
- 62.González S, Gilaberte Y, Philips N, Juarranz A. Fernblock, a nutriceutical with photoprotective properties and potential preventive agent for skin photoaging and photoinduced skin cancers. Int J Mol Sci. 2011;12:8466–8475. doi: 10.3390/ijms12128466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Rodríguez-Yanes E, Cuevas J, González S, Mallol J. Oral administration of Polypodium leucotomos delays skin tumor development and increases epidermal p53 expression and the anti-oxidant status of UV-irradiated hairless mice. Exp Dermatol. 2014;23:526–528. doi: 10.1111/exd.12454. [DOI] [PubMed] [Google Scholar]
- 64.Basler RS. Acne mechanica in athletes. Cutis. 1992;50:125–128. [PubMed] [Google Scholar]
- 65.Farber GA, Burks JW, Hegre AM, Brown GR. Football acne- an acneiform eruption. Cutis. 1977;20:356–360. [PubMed] [Google Scholar]
- 66.Kang YC, Choi EH, Hwang SM, et al. Acne mechanica due to an orthopedic crutch. Cutis. 1999;64:97–98. [PubMed] [Google Scholar]
- 67.Pecci M, Comeau D, Chawla V. Skin conditions in the athlete. Am J Sports Med. 2009;37:406–418. doi: 10.1177/0363546508325663. [DOI] [PubMed] [Google Scholar]
- 68.Marks R. Acne and its management beyond the age of 35 years. Am J Clin Dermatol. 2004;5:459–462. doi: 10.2165/00128071-200405060-00011. [DOI] [PubMed] [Google Scholar]
- 69.Knable AL, Jr, Hanke CW, Gonin R. Prevalence of acne keloidalis nuchae in football players. J Am Acad Dermatol. 1997;37:570–574. doi: 10.1016/s0190-9622(97)70173-7. [DOI] [PubMed] [Google Scholar]
- 70.Beckett N, Lawson C, Cohen G. Electrosurgical excision of acne keloidalis nuchae with secondary intention healing. J Clin Aesthet Dermatol. 2011;4:36–39. [PMC free article] [PubMed] [Google Scholar]
- 71.Mahmood T. Urticaria. Am Fam Physician. 1995;51:811–816. [PubMed] [Google Scholar]
- 72.Metz M, Bergmann P, Zuberbier T, Maurer M. Successful treatment of cholinergic urticaria with anti-immunoglobulin E therapy. Allergy. 2008;63:247–249. doi: 10.1111/j.1398-9995.2007.01591.x. [DOI] [PubMed] [Google Scholar]
- 73.Feinberg JH, Toner CB. Successful treatment of disabling cholinergic urticaria. Mil Med. 2008;173:217–220. doi: 10.7205/milmed.173.2.217. [DOI] [PubMed] [Google Scholar]
- 74.Lee EE, Maibach HI. Treatment of urticaria. An evidence-based evaluation of antihistamines. Am J Clin Dermatol. 2001;2:27–32. doi: 10.2165/00128071-200102010-00005. [DOI] [PubMed] [Google Scholar]
- 75.La Shell MS, England RW. Severe refractory cholinergic urticaria treated with danazol. J Drugs Dermatol. 2006;5:664–667. [PubMed] [Google Scholar]
- 76.Kozaru T, Fukunaga A, Taguchi K, et al. Rapid desensitization with autologous sweat in cholinergic urticaria. Allergol Int. 2011;60:277–281. doi: 10.2332/allergolint.10-OA-0269. [DOI] [PubMed] [Google Scholar]
- 77.Hough DO, Dec KL. Exercise-induced asthma and anaphylaxis. Sports Med. 1994;18:162–172. doi: 10.2165/00007256-199418030-00003. [DOI] [PubMed] [Google Scholar]
- 78.Fisher AA. Sports-related allergic dermatitis. Cutis. 1992;50:95–97. [PubMed] [Google Scholar]
- 79.Shadick NA, Liang MH, Partridge AJ, et al. The natural history of exercise-induced anaphylaxis: survey results from a 10-year follow-up study. J Allergy Clin Immunol. 1999;104:123–127. doi: 10.1016/s0091-6749(99)70123-5. [DOI] [PubMed] [Google Scholar]
- 80.Carlsen KH, Anderson SD, Bjermer L, et al. Treatment of exercise-induced asthma, respiratory and allergic disorders in sports and the relationship to doping: Part II of the report from the Joint Task Force of European Respiratory Society (ERS) and European Academy of Allergy and Clinical Immunology (EAACI) in cooperation with GA(2)LEN. Allergy. 2008;63:492–505. doi: 10.1111/j.1398-9995.2008.01663.x. [DOI] [PubMed] [Google Scholar]
- 81.Carlsen KH, Anderson SD, Bjermer L, et al. Exercise-induced asthma, respiratory and allergic disorders in elite athletes: epidemiology, mechanisms and diagnosis: part I of the report from the Joint Task Force of the European Respiratory Society (ERS) and the European Academy of Allergy and Clinical Immunology (EAACI) in cooperation with GA2LEN. Allergy. 2008;63:387–403. doi: 10.1111/j.1398-9995.2008.01662.x. [DOI] [PubMed] [Google Scholar]
- 82.Nolte K, Janse Van Rensburg C. Exercise-induced anaphylaxis. J Allergy Clin Immunol. 2010;23:78–80. [Google Scholar]
- 83.Conklin RJ. Common cutaneous disorders in athletes. Sports Med. 1990;9:100–119. doi: 10.2165/00007256-199009020-00004. [DOI] [PubMed] [Google Scholar]
- 84.Brenner IK, Shek PN, Shephard RJ. Infection in athletes. Sports Med. 1994;17:86–107. doi: 10.2165/00007256-199417020-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Robins DN. Cutaneous groin lesions. Prim Care. 1978;5:215–232. [PubMed] [Google Scholar]
- 86.Fragola LA, Jr, Watson PE. Common groin eruptions: diagnosis and treatment. Postgrad Med. 1981;69 doi: 10.1080/00325481.1981.11715764. 159-163,166-169,172. [DOI] [PubMed] [Google Scholar]
- 87.Janniger CK, Schwartz RA, Szepietowski JC, Reich A. Intertrigo and common secondary skin infections. Am Fam Physician. 2005;72:833–838. [PubMed] [Google Scholar]
- 88.Mistiaen P, Poot E, Hickox S, et al. Preventing and treating intertrigo in the large skin folds of adults: a literature overview. Dermatol Nurs. 2004;16 43-46, 49-57. [PubMed] [Google Scholar]
- 89.Lebwohl M, Freeman AK, Chapman MS, et al. Tacrolimus ointment is effective for facial and intertriginous psoriasis. J Am Acad Dermatol. 2004;51:723–730. doi: 10.1016/j.jaad.2004.07.011. [DOI] [PubMed] [Google Scholar]
- 90.Guitart J, Woodley DT. Intertrigo: a practical approach. Compr Ther. 1994;20:402–409. [PubMed] [Google Scholar]
- 91.Santiago-et-Sánchez-Mateos JL, Beà S, Fernández M, et al. Botulinum toxin type A for the preventive treatment of intertrigo in a patient with Darier’s disease and inguinal hyperhidrosis. Dermatol Surg. 2008;34:1733–1737. doi: 10.1111/j.1524-4725.2008.34361.x. [DOI] [PubMed] [Google Scholar]