

Abstract
Background:
Reaction time (RT) is a measure of the response to a stimulus. RT plays a very important role in our lives as its practical implications may be of great consequences. Factors that can affect the average human RT include age, sex, left or right hand, central versus peripheral vision, practice, fatigue, fasting, breathing cycle, personality types, exercise, and intelligence of the subject.
Aim:
The aim was to compare visual RTs (VRTs) and auditory RTs (ARTs) on the basis of gender and physical activity levels of medical 1st year students.
Materials and Methods:
The present cross-sectional study was conducted on 120 healthy medical students in age group of 18–20 years. RT for target stimulus that is, for the beep tone for measuring ART, and red circle for measuring VRT was determined using Inquisit 4.0 (Computer Software) in the laptop. The task was to press the spacebar as soon as the stimulus is presented. Five readings of each stimulus were taken, and their respective fastest RT's for each stimuli were recorded. Statistical analysis was done.
Results:
In both the sexes’ RT to the auditory stimulus was significantly less (P < 0.001) as compared to the visual stimulus. Significant difference was found between RT of male and female medical students (P < 0.001) as well as between sedentary and regularly exercising healthy medical 1st year students.
Conclusion:
The ART is faster than the VRT in medical students. Furthermore, male medical students have faster RTs as compared to female medical students for both auditory as well as visual stimuli. Regularly exercising medical students have faster RTs when compared with medical students with sedentary lifestyles.
Keywords: Auditory reaction time, exercise, females, males, medical students, visual reaction time
INTRODUCTION
Reaction time (RT) is a measure of the quickness with which an organism responds to some sort of stimulus. RT is defined as the interval of time between the presentation of the stimulus and appearance of appropriate voluntary response in the subject.[1] Luce[2] and Welford[3] described three types of RT. (1) Simple RT: Here there is one stimulus and one response. (2) Recognition RT: Here there is some stimulus that should be responded to and other that should not get a response. (3) Choice RT: Here there are multiple stimulus and multiple responses.
Abū Rayhān al-Bīrūnī was the first to describe the concept of RT.[4] Dutch physiologist Franciscus Cornelis Donders (1865) was among the first to systematically measure human RT using a telegraph like device invented in 1840 by Charles Wheatstone. Prior to his studies, there is no significant traceable thread in the literature about human RTs being measured.
Human RT works by having a nervous system recognize the stimulus. The neurons then relay the message to the brain. The message then travels from the brain to the spinal cord, which then reaches person's hands and fingers. The motor neurons then tell the hands and fingers how to react. The accepted figures for mean simple RTs for college-age individuals have been about 190 ms for light stimuli and about 160 ms for sound stimuli.[3] RT in response to a situation can significantly influence our lives due its practical implications. Fast RTs can produce rewards (e.g. in sports) whereas slow RT can produce grave consequences (e.g. driving and road safety matters). Factors that can affect the average human RT include age, sex, left or right hand, central versus peripheral vision, practice, fatigue, fasting, breathing cycle, personality types, exercise, and intelligence of the subject.[5]
In the literature very few studies[5,6] can be found determining RTs in medical students. Thus, this study was conducted to scientifically contribute to the field of RT. The present study seeks to determine (i) whether RT varies with the receptor system involved, (ii) the difference if any to RTs between the two sexes (iii) difference in RT in medical students with sedentary lifestyle and regularly exercising students.
MATERIALS AND METHODS
A total of 130 medical students were taken out of which 10 were excluded by various exclusion criteria comprising of any history of hearing or visual disorder, smoking, alcoholism, cardiovascular and respiratory disease, on any medication affecting cognitive performance. Thus, this cross-sectional study was conducted on a total of 120 (60 male and 60 female) healthy medical students who were physically normal in the age group 18–20 years. The subjects were randomly selected for the study. Ethical clearance for the study was obtained from Institutional Ethical Committee. Participation in the test was voluntary and informed written consent was taken from every participant.
The tests were done using Inquisit 4.0 computer software released in 2013 by Millisecond Software in Seattle, Washington. During the visual RT (VRT) task, in the center of the white screen background, the participant gets presented a black fixation cross that is followed after variable time intervals by a target stimulus that is, red circle. The students were asked to concentrate on the fixation cross and press the “space bar” key, as soon as possible once the red circle (target stimulus) appears on the screen. In a simple auditory RT (ART) task after variable time intervals, the sound is played for 30 s to the participant through the speakers. The task is to press the spacebar as soon as the sound is presented. All the subjects were thoroughly acquainted with the procedure and practice trial was given every student before taking the test. By default, the time intervals are randomly chosen from 2000 ms, 3000 ms, 4000 ms, 5000 ms, 6000 ms, 7000 ms, 8000 ms. Five readings of each stimuli were taken, and their respective fastest RT's for each stimuli were recorded. The readings were taken between 10 a.m. and 12 p.m. in a quiet secluded room.
A comparison was made between a. VRT and ART; b. VRT and ART between males and females; and c. VRT and ART between sedentary and regularly exercising healthy students. Both male and female medical students who participated in at least 30 min of moderate physical activity which made them sweat or breathe hard, such as fast walking, slow bicycling, skating, pushing a lawn mower, etc., on 5 or more days/week or in at least 20 min of vigorous physical activity that made them sweat or breathe hard, such as basketball, soccer, running, swimming, fast bicycling, fast dancing etc., on 3 days or more/week for a minimum duration of 6 weeks were considered to be regularly exercising healthy adult students, whereas those students who did not participate in these activities were considered to have a sedentary lifestyle.[7]
The statistical analysis was carried out with Statistical Package for Social Sciences version 17.0 manufactured by SPSS Inc. (Chicago). P < 0.05 was considered to be statistically significant.
RESULTS
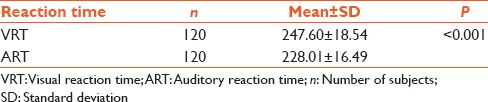
Table 1 shows comparison between VRT and ART using Paired t-test. The present study was undertaken on 120 students (n = 120). The statistical analysis of the results show that there is highly significant difference between the two and the ART is faster than the VRT in medical students.
Table 1.
Comparison between VRT and ART of medical students
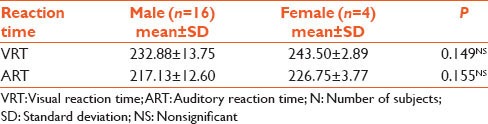
Unpaired t-test was used for overall comparison between male (n = 60) against female medical students (n = 60) for ART and VRT separately as shown in Table 2a. P < 0.001 was obtained, which is highly significant indicating that males have faster RTs when compared to females for both auditory, as well as visual stimuli. Table 2b shows comparison between sedentary male medical (n = 44) and female medical students (n = 56). P < 0.001 was obtained indicating sedentary male students have faster RTs (VRT and ART) as compared to sedentary female students. However when regularly exercising male (n = 16) and female students (n = 4) were compared as shown in Table 2c, nonsignificant differences were obtained.
Table 2a.
Overall comparison between male and female medical students
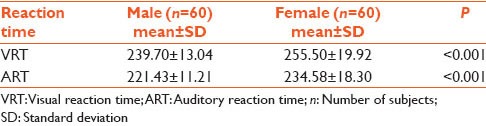
Table 2b.
Comparison between sedentary male and female medical students
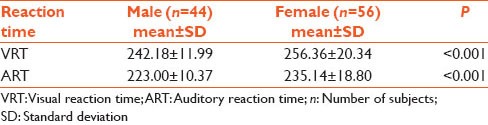
Table 2c.
Comparison between regularly exercising male and female medical students
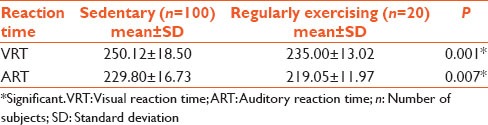
According to our statistical analysis of the overall comparison between sedentary and regularly exercising healthy medical students in Table 3, a significant difference was found indicating that sedentary medical students have slower RTs.
Table 3.
Overall comparison between sedentary and regularly exercising healthy medical students
DISCUSSION
The study was conducted on 120 healthy medical students to study the VRTs and ARTs and how do they vary on the basis of gender, and sedentary and regularly exercising healthy students.
Auditory reaction time versus visual reaction time
Our study shows that the ART is faster than the VRT [Table 1]. The results obtained are in parallel with the studies existing in the literature. Research done by Pain and Hibbs,[8] shows that simple ART has the fastest RT for any given stimulus. A study was carried out by Thompson et al.[9] has documented that the mean RT to detect visual stimuli is approximately 180–200 ms, whereas for sound it is around 140–160 ms. Researches by Kemp[10] show that an auditory stimulus takes only 8–10 ms to reach the brain, but on the other hand, a visual stimulus takes 20-40 ms. Therefore, since the auditory stimulus reaches the cortex faster than the visual stimulus, the ART is faster than the VRT. Shelton and Kumar[11] also concluded that simple RT is faster for auditory stimuli compared with visual stimuli and auditory stimuli has the fastest conduction time to the motor cortex along with fast processing time in the auditory cortex. On the other hand, there is a research done by Yagi et al.,[12] which shows that RT to visual stimuli is faster than to auditory stimuli. Hence, our study further supports the evidence that ART is faster than the VRT even in medical college students when confounding factors are removed.
Gender
A review of the literature on the influence of gender on RT shows that in almost every age group, males have faster RTs as compared to females, and female disadvantage is not reduced by practice.[13,14,15] Researches done by Misra et al.[16] also showed that males responded faster than females. Study done by Shelton and Kumar,[11] Nikam and Gadkari[17] also reported similar findings to support females have longer RTs than males. The results of our study [Table 2a] agree with these studies and indicate that male medical students have faster RTs when compared to female medical students for both auditory, as well as visual stimuli. In our study when sedentary male and female medical students [Table 2b] were compared removing any confounding factors, RTs of male students were faster; thereby further supporting the evidence that males have faster RTs than females.
The male-female difference is due to the lag between the presentation of the stimulus and the beginning of muscle contraction. It is documented in the literature that the muscle contraction time is the same for males and females[18] and motor responses in males are comparatively stronger than females,[19] this explains why males have faster simple RTs for both auditory as well as visual stimuli. Nowadays the male advantage is getting smaller, possibly because more women are participating in driving and fast-action sports.[19] This is evident from Table 2c in which nonsignificant differences were obtained when regularly exercising male and female medical students were compared.
Sedentary and regularly exercising healthy students
The findings of our study [Table 3] indicate that regularly exercising healthy medical students have faster RT than medical students with sedentary lifestyles and the difference between the two groups was statistically significant. These findings confirm the effect of physical activity and doing sports on improving RT which is supported by literature review done in this regard. Welford[3] found that physically fit subjects had faster RTs. Nougier et al.[20] suggest that athletes have better RT as compared to control subjects. Kaur et al.[21] found that athletes performed better than controls for auditory as well as VRT tasks. Nakamoto and Mori[22] found that college students who played basketball and baseball had faster RTs than sedentary students. Ghuntla et al.[23] showed that basketball players show faster RT than healthy controls. There are several possible explanations for this. Spirduso[24] proposed that less RT of athletes as compared to nonathletes was attributed to faster central nervous system processing times producing faster muscular movements in athletes. According to Gavkare et al.[25] shorter RT in athletes could be due to improved concentration and alertness, better muscular coordination, improved performance in the speed and accuracy task. Also, motor response execution is a physical task, so it is logical that people trained in physically reactive sports may have superior motor response ability.[26] It is also thought that individuals who exercise at moderate to intense levels have higher rates of cerebral blood flow. This increased amount of blood flow in the brain results in improvements in cognitive functioning due to increased supply of necessary nutrients, such as oxygen and glucose.[27,28]
CONCLUSION
Our study concluded that the ART is faster than the VRT in medical students. Male medical students have faster RTs as compared to female medical students for both auditory, as well as visual stimuli. Regularly exercising medical students have faster RTs as compared to medical students with sedentary life styles. Thus, it is strongly suggested that regular exercising must be encouraged in both male and female medical students to improve their efficiency levels.
Limitation of our study
We have conducted our study using simple RT. Choice RTs could be used as an expansion of the study in the future.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Duke-Elder S. Franciscus Cornelis Donders. Br J Ophthalmol. 1959;43:65–8. doi: 10.1136/bjo.43.2.65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Luce RD. London: Academic Press; 1968. [Last accessed on 2011 Aug 08]. Information Theory of Choice. Reaction Times. Available from: http://www.biology.clemson.edu/bpc/bp/Lab/110/reaction.htm . [Google Scholar]
- 3.Welford AT. Choice reaction time: Basic concepts. In: Welford AT, editor. Reaction Times. New York: Academic Press; 1980. pp. 73–128. [Google Scholar]
- 4.Muhammad I. The spirit of Muslim culture, the reconstruction of religious thought in Islam. [Last retrieved on 2008 Jan 25]. Available from: http://www.allamaiqbal.com/works/prose/english/reconstruction .
- 5.Karia RM, Ghuntla TP, Mehta HB, Gokhale PA, Shah CJ. Effect of gender difference on visual reaction time: A study on medical students of Bhavnagar region. IOSR-PHR. 2012;2:452–4. [Google Scholar]
- 6.Badwe N, Patil KB, Yelam SB, Vikhe BB, Vatve MS. A comparative study of hand reaction time to visual stimuli in students of 1 st MBBS of a rural medical college. Pravara Med Rev. 2012;4:4–6. [Google Scholar]
- 7.Anand M, Jain A. Comparative study of blood pressure and heart rate recovery after submaximal exercise in sedentary and regularly exercising healthy adult students. J Clin Diagn Res. 2012;6(Suppl 2):574–6. [Google Scholar]
- 8.Pain MT, Hibbs A. Sprint starts and the minimum auditory reaction time. J Sports Sci. 2007;25:79–86. doi: 10.1080/02640410600718004. [DOI] [PubMed] [Google Scholar]
- 9.Thompson PD, Colebatch JG, Brown P, Rothwell JC, Day BL, Obeso JA, et al. Voluntary stimulus-sensitive jerks and jumps mimicking myoclonus or pathological startle syndromes. Mov Disord. 1992;7:257–62. doi: 10.1002/mds.870070312. [DOI] [PubMed] [Google Scholar]
- 10.Kemp BJ. Reaction time of young and elderly subjects in relation to perceptual deprivation and signal-on versus signal-off condition. Dev Psychol. 1973;8:268–72. [Google Scholar]
- 11.Shelton J, Kumar GP. Comparison between auditory and visual simple reaction times. Neurosci Med. 2010;1:30–2. [Google Scholar]
- 12.Yagi Y, Coburn KL, Estes KM, Arruda JE. Effects of aerobic exercise and gender on visual and auditory P300, reaction time, and accuracy. Eur J Appl Physiol Occup Physiol. 1999;80:402–8. doi: 10.1007/s004210050611. [DOI] [PubMed] [Google Scholar]
- 13.Noble C, Baker BL, Jones TA. Age and sex parameters in psychomotor learning. Percept Mot Skills. 1964;19:935–45. doi: 10.2466/pms.1964.19.3.935. [DOI] [PubMed] [Google Scholar]
- 14.Adam JJ, Paas FG, Buekers MJ, Wuyts IJ, Spijkers WA, Wallmeyer P. Gender differences in choice reaction time: Evidence for differential strategies. Ergonomics. 1999;42:327–35. doi: 10.1080/001401399185685. [DOI] [PubMed] [Google Scholar]
- 15.Der G, Deary IJ. Age and sex differences in reaction time in adulthood: Results from the United Kingdom Health and Lifestyle Survey. Psychol Aging. 2006;21:62–73. doi: 10.1037/0882-7974.21.1.62. [DOI] [PubMed] [Google Scholar]
- 16.Misra N, Mahajan KK, Maini BK. Comparative study of visual and auditory reaction time of hands and feet in males and females. Indian J Physiol Pharmacol. 1985;29:213–8. [PubMed] [Google Scholar]
- 17.Nikam LH, Gadkari JV. Effect of age, gender and body mass index on visual and auditory reaction times in Indian population. Indian J Physiol Pharmacol. 2012;56:94–9. [PubMed] [Google Scholar]
- 18.Botwinick J, Thompson LW. Components of reaction time in relation to age and sex. J Genet Psychol. 1966;108:175–83. doi: 10.1080/00221325.1966.10532776. [DOI] [PubMed] [Google Scholar]
- 19.Silverman IW. Sex differences in simple visual re-action time: A historical meta-analysis (Sports Events) Sex Roles. 2006;54:57–69. [Google Scholar]
- 20.Nougier V, Ripoll H, Stein JF. Orienting of attention with highly skilled athletes. Int J Sport Psychol. 1989;20:205–23. [Google Scholar]
- 21.Kaur P, Paul M, Sandhu JS. Auditory and visual reaction time in athletes, healthy controls, and patients of type I diabetes mellitus: A comparative study. Int J Diabetes Dev Ctries. 2006;26:112–5. [Google Scholar]
- 22.Nakamoto H, Mori S. Sport-specific decision-making in a Go/NoGo reaction task: Difference among nonathletes and baseball and basketball players. Percept Mot Skills. 2008;106:163–70. doi: 10.2466/pms.106.1.163-170. [DOI] [PubMed] [Google Scholar]
- 23.Ghuntla TP, Mehta HB, Gokhale PA, Shah CJ. A comparative study of visual reaction time in basketball players and healthy controls. Natl J Integr Res Med. 2012;3:49. [Google Scholar]
- 24.Spirduso WW. Reaction and movement time as a function of age and physical activity level. J Gerontol. 1975;30:435–40. doi: 10.1093/geronj/30.4.435. [DOI] [PubMed] [Google Scholar]
- 25.Gavkare AM, Nanaware NL, Surdi AD. Auditory reaction time, visual reaction time and whole body reaction time in athletes. Ind Med Gaz. 2013;6:214–9. [Google Scholar]
- 26.Welford AT. London: Menthuen; 1968. [Last accessed on 2011 Aug 08]. Fundamentals of Skill. Available from: http://www.biology.clemson.edu/bpc/bp/Lab/110/reaction.htm . [Google Scholar]
- 27.Etnier JL, Walter S, Landers DM, Petruzzelo SJ, Han M, Nowell P. The influence of physical fitness and exercise upon cognitive functioning: A meta-analysis. J Sport Exerc Psychol. 1997;19:249–77. [Google Scholar]
- 28.Tomporowski PD, Ellis NR. Effects of exercise on cognitive processes: A review. Psychol Bull. 1986;99:338–46. [Google Scholar]