

Abstract
Background:
The main aim of this study is to evaluate the association between serum cholesterol level and abdominal obesity in adult men and women in the north of Iran.
Materials and Methods:
This cross-sectional and analytical study was conducted on the 1956 subjects (990 men and 966 women) between 25 and 65 years old chosen by cluster sampling. Plasma cholesterol was measured in the morning after a 12 h fast and determined by auto-analyzer. Hypercholesterolemia (HC) was defined by a total plasma cholesterol level over 200 mg/dl. Waist circumference ≥102 cm and ≥88 cm in men and women were defined as abdominal obesity. SPSS 16.0 software was used for statistical analysis and P < 0.05 considered as statistical significance.
Results:
Averagely, the mean of age was 44.2 years and mean ± standard deviation of plasma total cholesterol level was 203 ± 11.3 mg/dl. The HC was seen in 50.8% of subjects with a more common in women than in men. Compared with normal subjects, in abdominal obese people, the odds ratio (OR) of HC was (OR = 4.208 [95% confidence interval [CI]: 1.939–9.130]) and (OR = 3.956 [95% CI: 1.821–8.592]) in men aged 25–35 and 35–45 years, respectively. In women aged 25–35 years, it was (OR = 3.444 [95% CI: 1.959–6.056]) in abdominal obese compared with normal subjects.
Conclusion:
Hypercholesterolemia was revealed as a major health problem among adults, and it was associated with abdominal obesity especially in the early middle-age in the north of Iran. This association was not significant in men and women after the age of 45 and 35, respectively.
Keywords: Abdominal obesity, adult, gender, Iran, serum cholesterol level
INTRODUCTION
In middle-age, hypercholesterolemia (HC) is one of the major risk factors for heart disease patients[1] and 10% serum cholesterol reduction is associated with 30% mortality rate among them.[2]
The prevalence rate of HC was not equal in two genders as far as varied in populations from 3% to 53% in men and from 4% to 40% in women.[3]
Some plasma cholesterol correlated factors are included lifestyle, diet, smoking, central obesity, gender, physical activity and age.[4,5,6]
The association between waist circumference (WC) and cardiovascular disease (CVD) are established well in some studies[7,8,9,10] besides a negative correlation between serum cholesterol level and height was observed in men.[11,12] The alterations in lipid and lipoprotein concentration resulted in a changing of CVD risk factors.[13,14,15,16] The mortality and morbidity rates due to CVD have been estimated by plasma cholesterol levels in young and adult people in Framingham study.[17]
Direct correlation between serum cholesterol level and age has been seen in men and women.[18] Waist to hip ratio (WHR) was directly related to serum cholesterol.[7] In pubertal period, the correlation between total cholesterol and height was not steady.[19] The prevalence of HC increased with age and was significantly common in men more than in women at age range 24-29 years.[20] In Tibet adults,[21] total cholesterol level raised 0.24 mmol/L for 0.1 unit in WHR increasing.
Golestan province is in the north of Iran (south east of Caspian sea). Of 1.7 million people in this area, 66.39% were 15-64 years old, also 71% and 29% are living in urban and rural areas, respectively. Agriculture is the main job in a rural area and different ethnic groups such as fars (native), Turkman and Sisstani live in this region.[22]
The aim of this study is to evaluate the association between serum cholesterol level and abdominal obesity in men and women in 25-65-year-old people in Golestan province in the north of Iran.
MATERIALS AND METHODS
This is a cross-sectional study conducted on the 1956 subjects aged 25-65 years (990 men and 966 women). The required sample size based on the previous study,[3] with estimation of 25% HC rate; a confidence level of 95% and a maximum marginal error 0.02 was calculated 1800. The sample size increased to 2000 to compensate for an expected dropout rate of approximately 20%. Subjects were chosen randomly from 100 clusters and each cluster comprised 20 cases with equal proportions of genders and age groups in 11 districts. In the first stage, the clusters were chosen randomly using systematic sampling technique based on postal code in urban areas and family health number in Primary Health Centers in rural areas. In the second stage, we selected 20 subjects randomly in each cluster. This study included all family members in aged 25-65 years. A trained staff recorded the data during 3 mounts. The subjects who were pregnant, on lowering drugs and those who refused to participate in this study were excluded from the study. Finally, 2.2% (44) of subjects refused in this study.
Waist circumference was measured to the nearest 0.5 cm at the superior border of the iliac crest. Abdominal obesity was defined based on WHO the classification[23] with a WC ≥102 cm and ≥88 cm in men and women, respectively.
The blood was drowned from each subject after 12 h fast in the morning in order to measure the serum cholesterol level. It was measured on commercial kits (Pars Azmoon, Karaj, Iran) by auto-analyzer. Plasma cholesterol more than 200 mg/dl included as HC.[18]
SPSS 16.0 software (Chicago II, USA) was used for the statistical analysis using Chi-square test and t-test for comparing frequencies and the means, respectively. Logistic regression analysis was applied in order to estimate the odds ratio (OR) of HC considering the WC ranges at 95% significant level. P < 0.05 considered statistically significant. This study was approved by Ethical Research Committee and consent was received from all participants.
RESULTS
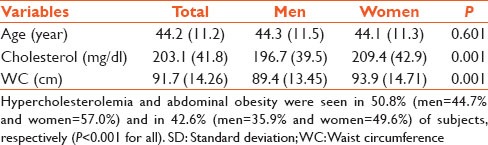
Mean and standard deviation of age and serum cholesterol level were 44.2 ± 11.3 years and 203 ± 11.3 mg/dl, respectively. The prevalence of abdominal obesity was seen in 42.6% (35.9% in men and 49.6% in women). HC was common in 50.8% with more prevalence in women (57.0%) than men (44.7%) [Table 1].
Table 1.
Characteristics of subjects, mean (SD), (total=1956, men=990, women=966)
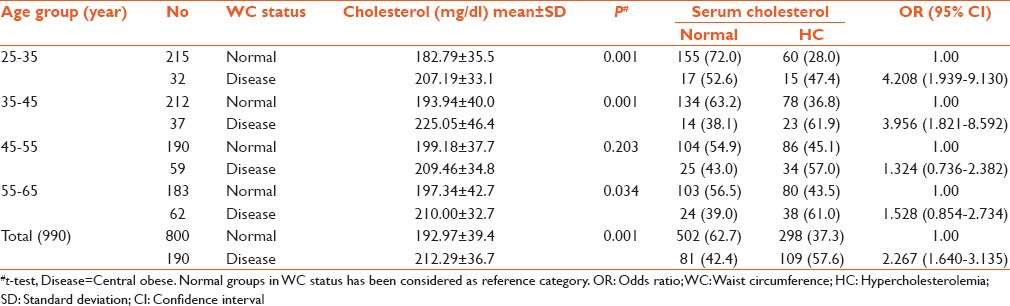
Distribution of serum cholesterol levels and WC based on age in men were presented in Table 2. As whole the mean of cholesterol was 20 mg/dl in abdominal obese more than in normal people and statistical differences was significant among all age groups (P < 0.001). Results of logistic regression analysis showed that the OR of HC is (OR = 4.208 [95% confidence interval [CI]: 1.939–9.130]) in abdominal obese compared to normal subjects and (OR = 3.956 [1.821–8.592]) in men aged 25–35 and 35–45 years, respectively. OR was not significant after age 45.
Table 2.
The association between serum cholesterol level and WC based on age in men
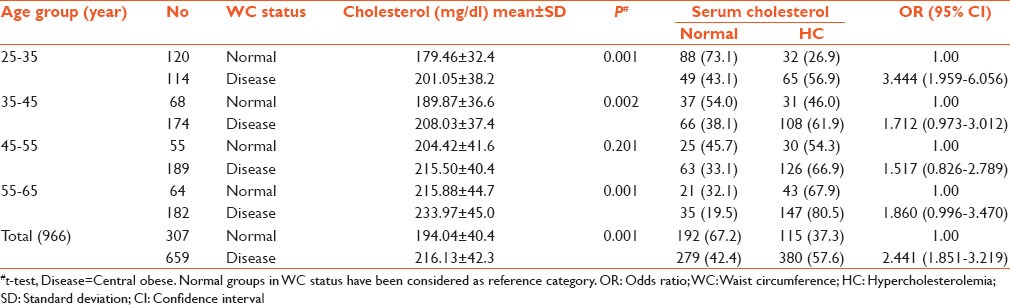
Distribution of serum cholesterol levels and abdominal obesity based on age in women are presented in Table 3. The mean of serum cholesterol levels differences was significant among normal and abdominal obese in all age groups (P < 0.001). The risk of HC is (OR = 3.444 [95% CI: 1.959–6.056]) in abdominal obese compared to normal subjects in women aged 25–35 years. OR was not significant in other age groups.
Table 3.
The association between serum cholesterol level and WC based on age in women
Contrary to normal subjects, abdominal obese people's mean serum cholesterol level remained significantly high in all of the age groups except for men aged 45–55 years.
DISCUSSION
The association between HC and abdominal obesity in men and women was not similar. In men aged under 45 years and in women aged under 35 years, the OR for HC was seen in abdominal obese subjects more than in normal ones.
The same as our study, the association between serum cholesterol level and abdominal based on age and sex has been reported in other studies. In a systematic review study, the direct association between serum cholesterol level and age was reported in two genders.[18] Among 25-64 years old, HC increased with age and it was more in men more than in women in 24-49 years age group.[20] Total serum cholesterol and nonhigh-density lipoprotein cholesterol have been correlated with WHR.[7] The association between age and serum cholesterol was not similar in all studies. Besides, inverse relationship between dyslipidemia and both WC and age among Turkish adult men,[24] the decline trend has been shown between HC and body mass index when adjusted with age in WHO MONICA project.[20]
Like above studies, we found the association between abdominal obesity and serum cholesterol level while it was weaker in upper age and less in women. With regard to different ethnic groups in the north of Iran, genetic factors probably influence on changing of serum cholesterol level and it should be considered in future studies. Lifestyle had a meaningful role in changing of serum cholesterol level in adults.[25,26] Look upon changing of lifestyle in Iran as a developing country,[27] we recommended to establish an educational planning for controlling the abdominal obesity and HC especially in early middle age.
Diet, physical activity, ethnicity, job and background disease were not assessed in our study. In addition, we did not provide a proper statistical test to evaluate the design effect resulted by cluster sampling. If we used a proper statistical test, it would change the narrow CI and low P value. They are limited factors for our study.
CONCLUSION
Hypercholesterolemia is a major health problem in the north of Iran and abdominal obesity is associated with it. In the early middle age, the association between WC and serum cholesterol level in abdominal obese subjects was more than in normal subjects, while this association has not been revealed in men and women upper age 45 and 35 years, respectively.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Kones R. Primary prevention of coronary heart disease: Integration of new data, evolving views, revised goals, and role of rosuvastatin in management. A comprehensive survey. Drug Des Devel Ther. 2011;5:325–80. doi: 10.2147/DDDT.S14934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jousilahti P, Vartiainen E, Pekkanen J, Tuomilehto J, Sundvall J, Puska P. Serum cholesterol distribution and coronary heart disease risk: Observations and predictions among middle-aged population in eastern Finland. Circulation. 1998;97:1087–94. doi: 10.1161/01.cir.97.11.1087. [DOI] [PubMed] [Google Scholar]
- 3.Tolonen H, Keil U, Ferrario M, Evans A. WHO MONICA Project. Prevalence, awareness and treatment of hypercholesterolaemia in 32 populations: Results from the WHO MONICA Project. Int J Epidemiol. 2005;34:181–92. doi: 10.1093/ije/dyi056. [DOI] [PubMed] [Google Scholar]
- 4.Morikawa Y, Nakagawa H, Miura K, Soyama Y, Ishizaki M, Kido T, et al. Effect of shift work on body mass index and metabolic parameters. Scand J Work Environ Health. 2007;33:45–50. doi: 10.5271/sjweh.1063. [DOI] [PubMed] [Google Scholar]
- 5.Oancã ME, Azoicãi D, Manole A, Ivan A. Contributions at clinical epidemiological peculiarities of essential arterial hypertension knowledge in a geographical area from Moldavia, Romania. Rev Med Chir Soc Med Nat Iasi. 2007;111:1012–6. [PubMed] [Google Scholar]
- 6.Kolovou GD, Anagnostopoulou KK, Damaskos DS, Mihas C, Mavrogeni S, Hatzigeorgiou G, et al. Gender influence on postprandial lipemia in heterozygotes for familial hypercholesterolemia. Ann Clin Lab Sci. 2007;37:335–42. [PubMed] [Google Scholar]
- 7.Henriksson KM, Lindblad U, Agren B, Nilsson-Ehle P, Råstam L. Associations between body height, body composition and cholesterol levels in middle-aged men. The coronary risk factor study in southern Sweden (CRISS) Eur J Epidemiol. 2001;17:521–6. doi: 10.1023/a:1014508422504. [DOI] [PubMed] [Google Scholar]
- 8.Jabbar A, Irfanullah A, Akhter J, Mirza YK. Dyslipidemia and its relation with body mass index versus waist hip ratio. J Pak Med Assoc. 1997;47:308–10. [PubMed] [Google Scholar]
- 9.Hashemipour M, Soghrati M, Malek Ahmadi M, Soghrati M. Anthropometric indices associated with dyslipidemia in obese children and adolescents: A retrospective study in isfahan. ARYA Atheroscler. 2011;7:31–9. [PMC free article] [PubMed] [Google Scholar]
- 10.Rhéaume C, Leblanc MÈ, Poirier P. Adiposity assessment: Explaining the association between obesity, hypertension and stroke. Expert Rev Cardiovasc Ther. 2011;9:1557–64. doi: 10.1586/erc.11.167. [DOI] [PubMed] [Google Scholar]
- 11.Hebert PR, Rich-Edwards JW, Manson JE, Ridker PM, Cook NR, O’Connor GT, et al. Height and incidence of cardiovascular disease in male physicians. Circulation. 1993;88:1437–43. doi: 10.1161/01.cir.88.4.1437. [DOI] [PubMed] [Google Scholar]
- 12.Kannam JP, Levy D, Larson M, Wilson PW. Short stature and risk for mortality and cardiovascular disease events. The Framingham Heart Study. Circulation. 1994;90:2241–7. doi: 10.1161/01.cir.90.5.2241. [DOI] [PubMed] [Google Scholar]
- 13.National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143–421. [PubMed] [Google Scholar]
- 14.Sarwar N, Danesh J, Eiriksdottir G, Sigurdsson G, Wareham N, Bingham S, et al. Triglycerides and the risk of coronary heart disease: 10,158 incident cases among 262,525 participants in 29 Western prospective studies. Circulation. 2007;115:450–8. doi: 10.1161/CIRCULATIONAHA.106.637793. [DOI] [PubMed] [Google Scholar]
- 15.Freiberg JJ, Tybjaerg-Hansen A, Jensen JS, Nordestgaard BG. Nonfasting triglycerides and risk of ischemic stroke in the general population. JAMA. 2008;300:2142–52. doi: 10.1001/jama.2008.621. [DOI] [PubMed] [Google Scholar]
- 16.Labreuche J, Touboul PJ, Amarenco P. Plasma triglyceride levels and risk of stroke and carotid atherosclerosis: A systematic review of the epidemiological studies. Atherosclerosis. 2009;203:331–45. doi: 10.1016/j.atherosclerosis.2008.08.040. [DOI] [PubMed] [Google Scholar]
- 17.D’Agostino RB, Sr, Grundy S, Sullivan LM, Wilson P. CHD Risk Prediction Group. Validation of the Framingham coronary heart disease prediction scores: Results of a multiple ethnic groups investigation. JAMA. 2001;286:180–7. doi: 10.1001/jama.286.2.180. [DOI] [PubMed] [Google Scholar]
- 18.Costa J, Borges M, Oliveira E, Gouveia M, Carneiro AV. Incidence and prevalence of hypercholesterolemia in Portugal: A systematic review. Part III. Rev Port Cardiol. 2003;22:829–36. [PubMed] [Google Scholar]
- 19.Kouda K, Nakamura H, Fan W, Takeuchi H. Negative relationships between growth in height and levels of cholesterol in puberty: A 3-year follow-up study. Int J Epidemiol. 2003;32:1105–10. doi: 10.1093/ije/dyg207. [DOI] [PubMed] [Google Scholar]
- 20.Gostynski M, Gutzwiller F, Kuulasmaa K, Döring A, Ferrario M, Grafnetter D, et al. Analysis of the relationship between total cholesterol, age, body mass index among males and females in the WHO MONICA Project. Int J Obes Relat Metab Disord. 2004;28:1082–90. doi: 10.1038/sj.ijo.0802714. [DOI] [PubMed] [Google Scholar]
- 21.Sherpa LY, Deji, Stigum H, Chongsuvivatwong V, Luobu O, Thelle DS, et al. Lipid profile and its association with risk factors for coronary heart disease in the highlanders of Lhasa, Tibet. High Alt Med Biol. 2011;12:57–63. doi: 10.1089/ham.2010.1050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Selected Findings of the 2011 National Population and Housing Census in I. R. of Iran. [Last accessed 2012 June 10]. Available from: http://www.amar.org.ir/Portals/1/Iran/census-2.pdf .
- 23.Gutiérrez-Fisac JL, Guallar-Castillón P, León-Muñoz LM, Graciani A, Banegas JR, Rodríguez-Artalejo F. Prevalence of general and abdominal obesity in the adult population of Spain, 2008-2010: The ENRICA study. Obes Rev. 2012;13:388–92. doi: 10.1111/j.1467-789X.2011.00964.x. [DOI] [PubMed] [Google Scholar]
- 24.Erem C, Hacihasanoglu A, Deger O, Kocak M, Topbas M. Prevalence of dyslipidemia and associated risk factors among Turkish adults: Trabzon lipid study. Endocrine. 2008;34:36–51. doi: 10.1007/s12020-008-9100-z. [DOI] [PubMed] [Google Scholar]
- 25.Hubert HB, Eaker ED, Garrison RJ, Castelli WP. Life-style correlates of risk factor change in young adults: An eight-year study of coronary heart disease risk factors in the Framingham offspring. Am J Epidemiol. 1987;125:812–31. doi: 10.1093/oxfordjournals.aje.a114598. [DOI] [PubMed] [Google Scholar]
- 26.Ledoux M, Lambert J, Reeder BA, Després JP. A comparative analysis of weight to height and waist to hip circumference indices as indicators of the presence of cardiovascular disease risk factors. Canadian Heart Health Surveys Research Group. CMAJ. 1997;157(Suppl 1):S32–8. [PubMed] [Google Scholar]
- 27.Ghassemi H, Harrison G, Mohammad K. An accelerated nutrition transition in Iran. Public Health Nutr. 2002;5:149–55. doi: 10.1079/PHN2001287. [DOI] [PubMed] [Google Scholar]