

Abstract
Background:
Evaluation of the craniofacial bones is the oldest method to measure the facial proportion ratio in orthodontics.
Objectives:
The purpose of this study was to evaluate the effect of emboss enhancement on the reliability of landmark identification in digital lateral cephalometric images.
Materials and Methods:
Ten digital lateral cephalograms were selected from the archive of an oral and maxillofacial radiology center. Using DIGORA software, these images were saved in two formats; common images and 3D emboss images. On these images, 32 skeletal, dental, and soft tissue landmarks were marked at least twice with a 2-week interval by four observers (two radiologists and two orthodontists). In order to determine the position of the marked landmarks (in x and y coordinates), a software was designed. The statistical analysis was performed in SPSS software and the reliability of each observer was obtained by means of intraclass correlation coefficient (ICC).
Results:
In three skeletal landmarks [Orbit (Or), condyl top (Cond), and pogonion (Pog)], the enhancement caused significant reduction in the reliability, and in four skeletal [Anterior Nasal Spine (ANS), B, A, and Basion (Ba)], two dental (U1 root, L1 incisal), and one soft tissue landmark (Menton soft tissue), the enhancement increased the reliability of landmark detection between the two phases of the study. Totally, ICC of embossed images in both x and y coordinates were greater than the typical images, but the difference was not statistically significant. However, the effect of enhancement on the improvement of the reliability of landmark identification was higher in the x-axis than the y-axis.
Conclusions:
Using embossed images is only effective in increasing the reliability of detection in a few numbers of cephalometric landmarks.
Keywords: Cephalometry, Emboss Enhancement, Reliability
1. Background
Craniofacial evaluation has been the oldest method for the evaluation of facial proportion ratio in orthodontics. On the other hand, cephalometry is used to evaluate the craniofacial growth and to determine the treatment responses (1). Many surgeons and orthodontists use cephalometric analysis for diagnosis, treatment planning and evaluation of treatment results (2). In 1985, for the first time, Gijbels et al. and Jackson et al. reported that using enhancement techniques could increase the precision in some radiographic applications (3, 4). To this end, several software programs have been designed for enhancing images and facilitating detection of specific points (5, 6). Enhancement is a method for increasing image resolution using various techniques such as computer processing and digital filtering. Emboss radiography is a new radiographic technique with various applications.
However, using enhancement algorithms for cephalometric images is still questionable (7). So far, various enhancement methods such as edge enhancement have been used for cephalometry and neither has significantly increased the precision of cephalometric landmark determination (8). In 2006, Wiesemann et al. concluded that if emboss enhancement is used, hard tissue cephalometric landmarks will have a higher resolution compared to conventional cephalometry images (9). Emboss images are made by subtraction methods. In emboss radiography, before subtraction, the image shift is done by moving the x radiation source, moving the object or shifting the original image pixel by a software program. In other words, embossing process is making a three dimensional image from a two dimensional image. When emboss filter is applied, often an image similar to the original image but like an embossed image on a piece of paper or metal will be created. Image with sharp edges are graphically desirable. For this purpose, in this study, using embossing filter software, original images are shifted and then subtracted from the obtained image (10). Maximum contrast can be achieved using this method without decreasing spatial resolution. Therefore, the main advantage of this technique might be edge enhancement (11). So this method seems to be a useful method if the study confirms its accuracy. To date, there is little and conflicting information regarding the clinical benefits of digital cephalograms using emboss enhancement. Wiesemann et al. concluded that emboss enhancement gives a higher resolution to hard tissue cephalometric landmarks compared to conventional cephalometric images (9). However, Leonardi et al. did not report any advantages on a more precise landmark determination in emboss enhancement in 2010 (5). Therefore, further study in this regard seems necessary.
2. Objectives
Given the importance of facilitating cephalometric landmark determination to decrease individual errors, we aimed to investigate the effect of emboss enhancement on the reproducibility of cephalometric landmark determination.
3. Materials and Methods
Ten digital lateral cephalometries prepared by Promax Dimax 3 Digital Pan/Ceph device (Planmeca, Finland) that met study requirements were selected from the images of the patients who were admitted to a private oral and maxillofacial radiology center for orthodontic radiography evaluation. The radiographs that had the following conditions were excluded:
Wrong position of head
Central incisors or unerupted or absent molars
Severe craniofacial deformity
Posterior teeth were not in maximum intercuspation
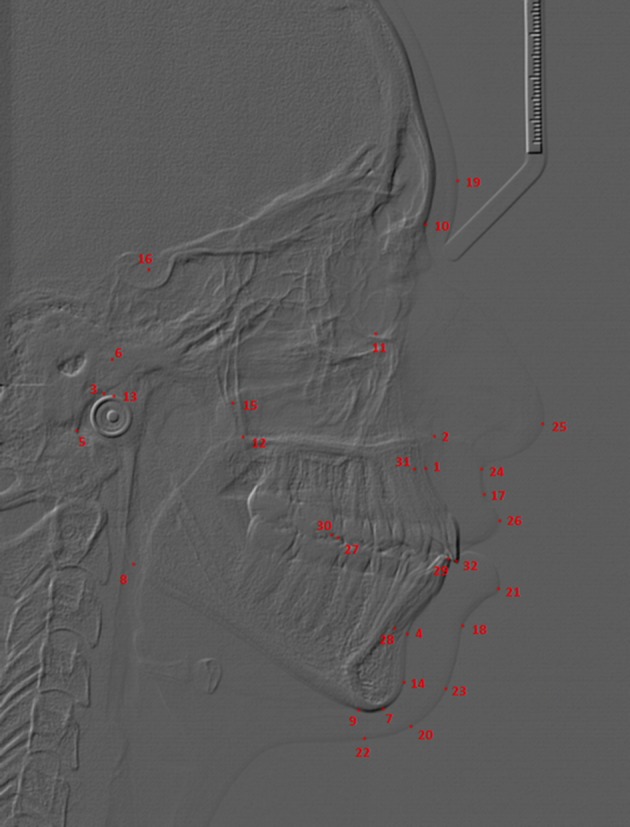
Emboss enhancement was performed on each of these radiographs using Digora software for windows and the new radiograph was saved as a separate file. Anatomic landmarks stated in Table 1 are indicated in figures with the same identification numbers. Both conventional images (Figure 1) and enhanced images (Figure 2) were saved in bitmap format (bmp) because it preserves more precise information. All images were resized to 1200 × 900 pixels and saved before being sent to evaluators for landmark determination. Two orthodontists and two radiologists with different working experiences determined 32 skeletal, soft tissue and dental cephalometric landmarks that are more common in conventional cephalometric analysis on each radiograph. These spots were marked using a specific size and red color in the Paint software. The evaluators were given standard definitions of landmarks before conducting the study to establish an agreement between them. Landmark determination was carried out on the same radiographs after two weeks by the evaluators so that the reliability of determining each landmark in each image format (conventional or embossed) was determined by each evaluator. The evaluators were asked to mark under the same conditions regarding the ambient light, monitor type and the screen settings in both stages.
Table 1. ICC of Two Methods of Marking Based on the Type of Anatomic Landmarks.
| Landmarks | ICC in Images Without Enhancement, (95% CI) | ICC in Images With Enhancement, (95% CI) | Subtraction | |||
|---|---|---|---|---|---|---|
| Xo | Yo | Xe | Ye | Xo-Xe | Yo-Ye | |
| Skeletala | ||||||
| A | 0.9496 (0.8996-0.9996) | 0.8628 (0.7958-0.9298) | 0.9021 (0.8521-0.9521) | 0.9804 (0.9134-1) | 0.0475 | -0.1176 |
| ANS | 0.5511 (0.4131-0.6891) | 0.8607 (0.6758-1) | 0.9964 (0.8584-1) | 0.9504 (0.7655-1) | -0.4453 | -0.0897 |
| Ar | 0.8805 (0.7765-0.9845) | 0.9325 (0.7931-1) | 0.9595 (0.8555-1) | 0.9245 (0.7851-1) | -0.079 | 0.008 |
| B | 0.8105 (0.7005-0.9205) | 0.9877 (0.8403-1) | 0.9599 (0.8499-1) | 0.9952 (0.8478-1) | -0.1407 | -0.0075 |
| Ba | 0.9597 (0.9177-1) | 0.8807 (0.8244-0.937) | 0.9765 (0.9345-1) | 0.9888 (0.9325-1) | -0.0168 | -0.1075 |
| Cond | 0.8847 (0.8367-0.9327) | 0.9792 (0.9149-1) | 0.6559 (0.6079-0.7039) | 0.9119 (0.8476-0.9762) | 0.2288 | 0.0673 |
| Gn | 0.9941 (0.9321-1) | 0.9702 (0.8871-1) | 0.9951 (0.9331-1) | 0.9679 (0.8848-1) | -0.001 | 0.0023 |
| Go | 0.9727 (0.9367-1) | 0.9087 (0.8605-0.9569) | 0.9777 (0.9417-1) | 0.9717 (0.9235-1) | -0.005 | -0.063 |
| Me | 0.9261 (0.8881-0.9641) | 0.9268 (0.8759-0.9777) | 0.9826 (0.9446-1) | 0.9717 (0.9208-1) | -0.0565 | -0.0449 |
| N | 0.9247 (0.8767-0.9727) | 0.9946 (0.9303-1) | 0.9951 (0.9471-1) | 0.996 (0.9317-1) | -0.0704 | -0.0014 |
| Or | 0.9421 (0.9001-0.9841) | 0.9654 (0.9091-1) | 0.7617 (0.7197-0.8037) | 0.8112 (0.7549-0.8675) | 0.1804 | 0.1542 |
| PNS | 0.9633 (0.9393-0.9873) | 0.9802 (0.948-1) | 0.9914 (0.9674-1) | 0.9597 (0.9275-0.9919) | -0.0281 | 0.0205 |
| Po | 0.9114 (0.8654-0.9574) | 0.9974 (0.9358-1) | 0.9259 (0.8799-0.9719) | 0.9977 (0.9361-1) | -0.0145 | -0.0003 |
| Pog | 0.9695 (0.9315-1) | 0.9967 (0.9458-1) | 0.9803 (0.9423-1) | 0.8364 (0.7855-0.8873) | -0.0108 | 0.1603 |
| PTM | 0.8785 (0.8305-0.9265) | 0.9822 (0.9179-1) | 0.9753 (0.9273-1) | 0.9868 (0.9225-1) | -0.0968 | -0.0046 |
| S | 0.9968 (0.9748-1) | 0.9982 (0.9687-1) | 0.9977 (0.9757-1) | 0.9989 (0.9694-1) | -0.0009 | -0.0007 |
| Soft Tissue b | ||||||
| A st | 0.9058 (0.8778-0.9338) | 0.9832 (0.9457-1) | 0.991 (0.963-1) | 0.9587 (0.9212-1) | -0.0852 | -0.0254 |
| B st | 0.9689 (0.9429-0.9949) | 0.9992 (0.9644-1) | 0.9825 (0.9565-1) | 0.9922 (0.9574-1) | -0.0136 | 0.007 |
| Gl | 0.6123 (0.5603-0.6643) | 0.9919 (0.9222-1) | 0.6142 (0.5622-0.6662) | 0.9979 (0.9282-1) | -0.0019 | -0.006 |
| Gnst | 0.9647 (0.9407-0.9887) | 0.9692 (0.937-1) | 0.9522 (0.9282-0.9762) | 0.9229 (0.8907-0.9551) | 0.0125 | 0.0463 |
| Lower lip | 0.9828 (0.9608-1) | 0.9993 (0.9698-1) | 0.9256 (0.9036-0.9476) | 0.9923 (0.9628-1) | 0.0572 | 0.007 |
| Me st | 0.7875 (0.7455-0.8295) | 0.8818 (0.8255-0.9381) | 0.9945 (0.9525-1) | 0.9637 (0.9074-1) | -0.207 | -0.0819 |
| Pog st | 0.9141 (0.8701-0.9581) | 0.993 (0.934-1) | 0.9109 (0.8669-0.9549) | 0.9173 (0.8583-0.9763) | 0.0032 | 0.757 |
| Subnasal | 0.8982 (0.8482-0.9482) | 0.9695 (0.9025-1) | 0.9905 (0.9405-1) | 0.9758 (0.9088-1) | -0.0923 | -0.0063 |
| Tip of nose | 0.9878 (0.9658-1) | 0.9902 (0.9607-1) | 0.9962 (0.9742-1) | 0.9904 (0.9609-1) | -0.0084 | -0.0002 |
| Upper lip | 0.9216 (0.8636-0.9796) | 0.9963 (0.9186-1) | 0.9919 (0.9339-1) | 0.9942 (0.9165-1) | -0.0703 | 0.0021 |
| Dental c | ||||||
| L6 mc | 0.9152 (0.8432-0.9872) | 0.9198 (0.8233-1) | 0.9773 (0.9053-1) | 0.8644 (0.7679-0.9609) | -0.062 | 0.0554 |
| L1 root | 0.9225 (0.8405-1) | 0.8683 (0.7584-0.9782) | 0.8833 (0.8013-0.9653) | 0.8336 (0.7237-0.9435) | 0.0392 | 0.0347 |
| L1 incisal | 0.8836 (0.7816-0.9856) | 0.9892 (0.8525-1) | 0.9974 (0.8954-1) | 0.9978 (0.8611-1) | -0.1138 | -0.0086 |
| U6 mc | 0.9699 (0.9379-1) | 0.9365 (0.8936-0.9794) | 0.9751 (0.9431-1) | 0.8922 (0.8493-0.9351) | -0.0052 | 0.0443 |
| U1 root | 0.8407 (0.7847-0.8967) | 0.9969 (0.9219-1) | 0.9608 (0.9048-1) | 0.9301 (0.8551-1) | -0.1201 | 0.0668 |
| U1 incisal | 0.9936 (0.9396-1) | 0.8958 (0.8234-0.9682) | 0.9982 (0.9442-1) | 0.9801 (0.9077-1) | -0.0046 | -0.0843 |
aSkeletal Landmarks, P, Porio: Most Superior Point of the External Auditory Canal; S, Sella: Center of the Hypophyseal Fossa; N, Nasion: Frontonasal Suture; Or, Orbitale: Most Inferior Point of the Infraorbital Rim; Ba, Basion: Most Anterior Point of the Foramen Magnum; PNS: Tip of the Posterior Nasal Spine; ANS: Tip of the Anterior Nasal Spine; A, A Point: Deepest Point of the Anterior Border of the Maxillary Alveolar Ridge Concavity; B, B Point: Deepest Point in the Concavity of the Anterior Border of the Mandible; Pog, Pogonion: Most Anterior Point of the Symphysis; Gn, Gnathion: Midpoint of the Symphysis Outline Between Pogonion and Menton; Me, Menton: Most Inferior Point of the Symphysis; Ar, Articulare: Point of Intersection Between the Basisphenoid and the Posterior Border of the Condylar Head; Cond, Condyle Top: Most Superior Point of the Condyle.
bSoft Tissue Landmarks, Gl, Soft Tissue Glabella: Most Anterior Point of the Soft Tissue Covering the Frontal Bone; Tip of Nose: Most Anterior Point of the Nose; Subnasal: Soft Tissue Point Where the Curvature of the Upper Lip Connects to the Floor of the Nose; A st, Soft Tissue A Point: Most Concave Point of the Upper Lip Between the Subnasale and the Upper Lip Point; Upper lip: Most Anterior Point of the Upper Lip; Lower Lip: Most Anterior Point of the Lower Lip; B st, Soft Tissue B Point: Most Concave Point of the Lower Lip Between the Chin and Lower Lip point; pog st, Soft Tissue Pogonion: Most Anterior Point of the Soft Tissue of the Chin; Gn st, Soft Tissue Gnathion: Midpoint of the Chin Soft Tissue Outline Between the Soft Tissue Pogonion and Soft Tissue Menton; Me st, Soft Tissue Menton: Most Inferiorx.
cDental Landmarks, U6 mc, U6 Mesial Cusp: Tip of the Maxillary First Molar Mesial Buccal Cusp; L6 mc, L6 Mesial Cusp: Tip of the Mandibular First Molar Mesial Buccal Cusp; Ul Incisal: Incisal Edge of Maxillary Central Incisor; Ul Root: Root Tip of the Maxillary Central Incisor; LI Incisal: Incisal Edge of Mandibular Central Incisor; LI Root: Root tip of the Mandibular Central Incisor.
Figure 1. Anatomic landmarks on cephalometric view.
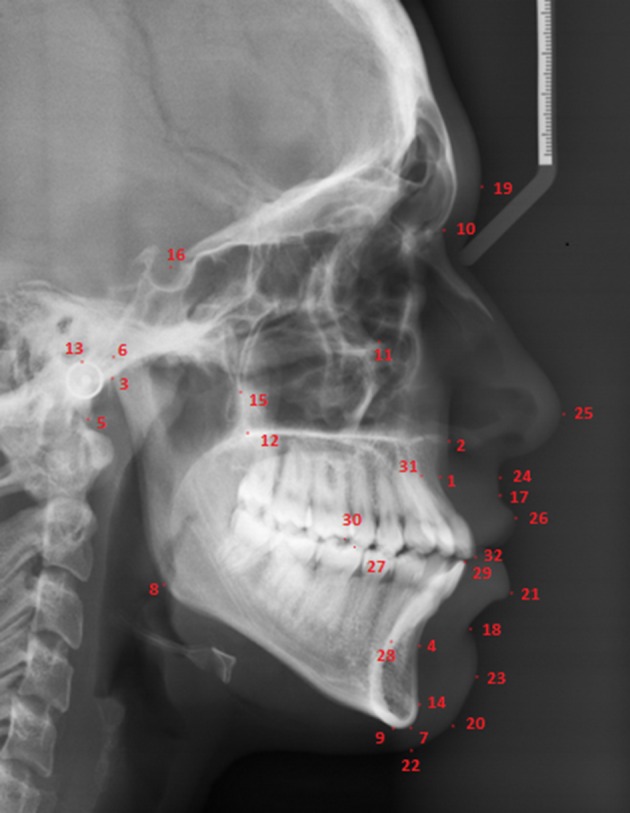
Figure 2. Anatomic landmarks on emboss enhanced cephalometric view.
In order to determine the coordinates of the marked points (place of them on x and y axes), a software program was designed. Then images were transferred to the software. The left corner at the bottom of each image was considered as the origin point of coordinate (the point x=0, y=0). Landmark situation data (x, y) in each image was arranged based on the situation on x and y-axes and then saved in an excel file.
Each of these marked points, which were detected by the software, had a circular shape and the center was considered as the exact location of the landmark. The bottom left corner of each image was considered as the zero coordinate.
The advantage of the designed software in this study compared to previous software programs, in which the evaluator has to click on a point so that the coordinates of the point are recorded on the software, is that in the present study, human error caused by clicking is eliminated due to auto detection of the red points by the software. The data in this study were analyzed using SPSS software ver. 16 (SPSS Inc., Chicago, IL, USA). Reliability of each observer was calculated by intraclass correlation coefficient (ICC) index. ICC above 0.9 was considered as good reliability, between 0.7 and 0.9 as average reliability, and less than 0.7 as poor reliability. Similarly, if the ICC difference between the two methods was less than -0.1 or above 0.1, it was considered statistically significant.
4. Results
Table 1 shows the ICC of determined landmarks in all studied parts (regardless of the evaluators). Table 2 shows the mean ICC in x and y coordinates for both methods, with and without enhancement in each of the evaluators, and in the whole study. In the first evaluator, enhancement in one of the skeletal landmarks (location A) resulted in a significant decrease of reliability in x dimension. The significant increase of reliability was observed in both x and y dimensions of ANS point and x dimension of nasion (N) point, condyl top (Cond), articular (Ar) and menton (Me). In soft tissue landmarks, both x and y dimensions of soft tissue Me point and x dimension of sub nasal and upper lip and in teeth landmarks after x, L6 mesial cusp, L1 incisal and U1 root showed a significant reliability increase.
Table 2. Average ICCa in X and Y Dimensions in Two Methods in Terms of Different Evaluators.
| Evaluators | Mean ICC in Images Without Emboss Enhancement | Mean ICC in Images With Emboss Enhancement | Subtraction of the Two ICCs | |||
|---|---|---|---|---|---|---|
| Xo | Yo | Xe | Ye | Xo-Xe | Yo-Ye | |
| Evaluator 1 | 0.845 | 0.967 | 0.952 | 0.980 | -0.107 | -0.013 |
| Evaluator 2 | 0.915 | 0.941 | 0.977 | 0.951 | -0.062 | -0.01 |
| Evaluator 3 | 0.941 | 0.936 | 0.973 | 0.971 | -0.032 | -0.035 |
| Evaluator 4 | 0.963 | 0.956 | 0.942 | 0.961 | 0.021 | -0.005 |
| Total | 0.916 | 0.956 | 0.961 | 0.966 | -0.045 | -0.01 |
a intraclass Correlation Coefficient.
Regarding the second evaluator, who was an experienced radiologist, the enhancement also in two skeletal landmarks (pogonion (Po) and basion (Ba)) resulted in a significant increase in reliability in x dimension. In the soft tissue, the reliability of Me soft tissue point increased in x dimension. In teeth landmarks, enhancement resulted in reliability decrease in y dimension of U6 mesial cusp and L6 mesial cusp and a significant increase was observed in Na (nasion) points.
Regarding the third evaluator, the enhancement in skeletal landmarks resulted in a decrease in reliability in x and y dimensions of Or point and a reliability increase in x and y points of Ar and ANS, x dimension of point B and y dimension of point A. In soft tissue, due to enhancement reliability in x dimension of the lower lip and y dimension of Me point, the soft tissue showed a decrease and in both x and y dimensions of point A an increase was observed.
The fourth evaluator was an expert orthodontist. The enhancement resulted in a significant reliability decrease in skeletal landmarks in Or point in x and y dimension and regarding Po, Cond, Ar and B in x dimension. However, enhancement in Ba and gonion (Go) had a significant reliability increase. In soft tissue, enhancement in x dimension of gnathion (Gn) point and Y dimension of pogonion (pog) point resulted in reliability decrease in landmark determination. Yet, both x and y of A point in soft tissue and x dimension of subnasal and Me soft tissue showed a reliability increase. Regarding teeth landmarks, enhancement resulted in reliability decrease in y dimension of L6 mesial cusp point and the reliability increase in x dimension of L1 root point.
Based on Table 1, enhancement resulted in reliability decrease. Of course this reliability decrease was statistically significant only in x and y dimensions of Or point, x dimension of Cond point and y dimension of Pog (which are all skeletal landmarks).
Likewise, the enhancement resulted in a reliability increase in 16 points and a decrease of errors in landmark determination in x and y dimensions (Table 1). However, this reliability increase in skeletal landmarks was statistically significant only in x dimension of ANS and B and y dimension of A and Ba. Regarding the soft tissue, the reliability increase was observed only in x dimension of Me soft tissue point and in teeth landmarks, in x dimension of U1 root and L1 incisal landmarks.
In radiographs without enhancement, the least ICC in x dimension was observed in ANS and Gl but reliability was poor (ICC < 0.7). In y dimension, the least ICC was observed in ANS point that had an average reliability (ICC = 0.86). Therefore, generally, most errors in landmark determination in non-enhanced radiographs were seen in ANS.
In radiographs with enhancement, the least ICC in x dimension was observed in GI and Cond points that had a poor reliability (ICC < 0.7). In y dimension, the least ICC was observed in Or, L1 root and L6 mesial cusp that had an average reliability (0.7 < ICC < O.9). Moreover, based on ICC mean in 2 dimensions, most landmark errors in enhanced radiographs were in or point. In all, the highest reliability coefficient either in non-enhanced radiographs or the enhanced ones was in S anatomical landmark.
After S point, the highest reliability was observed in lower lip landmarks in non-enhanced radiographs, and in N, tip of the nose and upper lip points in enhanced radiographs (mean ICC of x and y > 0.99).
In all, except x dimension for the fourth evaluator, in other states, enhancement resulted in an increase in landmark determination. Such a reliability increase was statistically significant in x dimension in the first evaluator.
5. Discussion
The advent of digital radiography in the dental field in the 1970s revolutionized clinical works and research methods in craniofacial cephalometry. Lateral cephalometric radiographs are routinely used in orthodontics, diagnosis, treatment planning, and follow-up of craniofacial problems and evaluation of treatment plan results (12). A study conducted by Chen et al. in 2000 showed that errors in landmark determination in digital cephalometric radiographs are significantly lower compared to the conventional ones (13). Moreover, previous studies revealed significantly lower radiation doses in digital cephalometry than conventional method without causing negative impact on the reliability of anatomical landmark determination (14, 15).
In 2006, Wiesemann et al. reported that by using different methods of enhancement and filtering techniques, digital cephalometric image quality improves (9). In this study, 11 landmarks were investigated. Emboss enhancement was preferred in determination of 9 hard tissue landmarks and pseudo-color enhancement was preferred in soft tissue landmarks. However, the result of their study was based on the preference of the evaluator on enhanced rather than non-enhanced radiographs and they were not assessed regarding the effect of enhancement on the validity of landmark determination in these radiographs. In addition, many landmarks used in the cephalometric analysis were not evaluated in this study.
Therefore, because improving visibility by manipulating digital radiographs does not necessarily mean improved clinical performance, conducting a study to evaluate the impact of these manipulations on the accuracy of diagnostic procedures such as determination of cephalometric landmarks is essential.
In 2010, Leonardi et al. used the mean of determined point coordinates as the gold standard for comparing the accuracy of landmarks for both methods, and reported no significant difference in the accuracy of 22 cephalometric landmarks determined in enhancement radiographs (5). Only at the Po point, mean geometric error in radiographs with enhancement was significantly lower than that of conventional images.
Generally, regarding factors effective on cephalometric landmark determination, the advantage of the present study compared to previous studies could be in selecting evaluators, the statistical methods, the number of landmarks and the use of digital radiographs.
Unlike other studies in which the evaluators were all orthodontic specialists or residents (2, 5-7, 9), in this study, they were selected from two disciplines namely radiology and orthodontics having varying levels of work experience. Therefore, the effects of expertise and experience could be investigated in this study.
According to the results, the orthodontic specialists (the third and the fourth evaluator) were more reliable in determining the landmarks particularly in non-enhanced radiographs, and enhancement was less effective in increasing the ICC in both evaluators. This issue could be justified considering the skill and the training of people in using conventional cephalometric radiographs. Furthermore, the experience was effective in both expertise, so the second and the fourth evaluators who were more experienced in clinical practice compared to their peer evaluators, on average, showed a higher reliability in determining the landmarks. This can be attributed to the importance of experience in the accuracy of clinical practices.
Regarding the number of landmarks studied, 32 landmarks were investigated in this study. This number is higher compared to previous studies (2, 5-7) and provides the possibility to generalize the results. In Leonardi’s and Wiesemann study, enhancement did not result in an increase in landmark determination accuracy and the evaluator’s preference (5, 7) and this finding is in line with that of the present study.
In general, based on the present and previous studies, it can be concluded that emboss enhancement in cephalometric tracing of some important landmarks could act as a tool used in addition to conventional cephalometric radiographs.
Although in this research we considered the minimum sample size regarding to our limitations and previous studies, larger sample size is highly suggested for more accurate further studies.
Yet, it should be noted that in these enhanced 3-dimensional radiographs, lines and shadows are created due to enhancement. Therefore, more studies are essential in this area. It can be concluded that emboss enhancement can be an effective tool in more reliable determination of some skeletal, soft tissue and teeth landmarks (A, ANS, B, Ba, Me soft tissue, L1 incisal and U1 root). In contrast, Cond, Or, and Pog points are recognized better in conventional radiographs rather than the enhanced ones. In general, emboss radiographs in both x and y dimensions have a higher ICC coefficient compared to conventional radiographs, but the difference was not statistically significant. In addition, the effect of enhancement in improving the reliability of landmarks was more powerful in x dimension compared to y dimension. In this study, we considered the minimum sample size regarding to our limitations. Larger sample sizes for future studies are highly recommended for more accuracy.
Footnotes
Authors’ Contributions:Study concept and design: Sima Nikneshan. Acquision of data: Sudeh Mohseni. Analysis and interparation: Mahtab Nouri. Drafting of manuscript: Hoora Hadian. Critical revision and intellectual content: Hoora Hadian and Sima Nikneshan. Statistical analysis: Mohammad Javad Kharazifard. Tecchnical and material support: Mahtab Nouri.
Funding/Support:This project was supported financially by Shahid Beheshti University of Medical Sciences.
References
- 1.Macri V, Wenzel A. Reliability of landmark recording on film and digital lateral cephalograms. Eur J Orthod. 1993;15(2):137–48. doi: 10.1093/ejo/15.2.137. [DOI] [PubMed] [Google Scholar]
- 2.Chen YJ, Chen SK, Huang HW, Yao CC, Chang HF. Reliability of landmark identification in cephalometric radiography acquired by a storage phosphor imaging system. Dentomaxillofac Radiol. 2004;33(5):301–6. doi: 10.1259/dmfr/85147715. [DOI] [PubMed] [Google Scholar]
- 3.Gijbels F, Bou Serhal C, Willems G, Bosmans H, Sanderink G, Persoons M, et al. Diagnostic yield of conventional and digital cephalometric images: a human cadaver study. Dentomaxillofac Radiol. 2001;30(2):101–5. doi: 10.1038/sj/dmfr/4600585. [DOI] [PubMed] [Google Scholar]
- 4.Jackson PH, Dickson GC, Birnie DJ. Digital image processing of cephalometric radiographs: a preliminary report. Br J Orthod. 1985;12(3):122–32. doi: 10.1179/bjo.12.3.122. [DOI] [PubMed] [Google Scholar]
- 5.Leonardi RM, Giordano D, Maiorana F, Greco M. Accuracy of cephalometric landmarks on monitor-displayed radiographs with and without image emboss enhancement. Eur J Orthod. 2010;32(3):242–7. doi: 10.1093/ejo/cjp122. [DOI] [PubMed] [Google Scholar]
- 6.Ryu HS, Hwang HS. Reproducibility of Lateral Cephalometric Landmarks According to Radiographic Image Enhancement. Korean J Orthod. 2002;32(1):59–69. [Google Scholar]
- 7.Weisemann RB, Scheetz JP, Silveira AM, Farman TT, Farman AG. Effect of pixel histogram distribution on perceived anatomical landmark clarity of photostimulable phosphor cephalograms. Int J Comput Assist Radiol Surg. 2006;1(2):97–103. [Google Scholar]
- 8.Menig JJ. The DenOptix digital radiographic system. J Clin Orthod. 1999;33(7):407–10. [PubMed] [Google Scholar]
- 9.Wiesemann RB, Scheetz JP, Sanderink G, Farman AG. Cephalometric landmark clarity in photostimulable phosphor images using pseudo-color and emboss enhancements. Int J Comput Assist Radiol Surg. 2006;1(2):105–12. [Google Scholar]
- 10.Sato E, Osawa A, Matsukiyo H, Enomoto T, Watanabe M, Sato S, et al. Embossed radiography utilizing an image-shifting subtraction program. Nucl Instrum Methods . 2010;619(1-3):133–9. doi: 10.1016/j.nima.2009.11.028. [DOI] [Google Scholar]
- 11.Osawa A, Watanabe M, Sato E, Matsukiyo H, Enomoto T, Nagao J, et al. Embossed radiography utilizing energy subtraction. Radiol Phys Technol. 2009;2(1):77–86. doi: 10.1007/s12194-008-0048-8. [DOI] [PubMed] [Google Scholar]
- 12.Shin JW, Choi HM, Heo MS, Lee SS, Choi HB, Choi SC. Reproducibility of lateral cephalometric landmarks on conventional radiographs and spatial frequency-processed digital images. Korean J Oral Maxillofac Radiol. 2002 [Google Scholar]
- 13.Chen YJ, Chen SK, Chang HF, Chen KC. Angle Orthod. 2000;70(5):387–92. doi: 10.1043/0003-3219(2000)070<0387:COLIIT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 14.Chien PC, Parks ET, Eraso F, Hartsfield JK, Roberts WE, Ofner S. Comparison of reliability in anatomical landmark identification using two-dimensional digital cephalometrics and three-dimensional cone beam computed tomography in vivo. Dentomaxillofac Radiol. 2009;38(5):262–73. doi: 10.1259/dmfr/81889955. [DOI] [PubMed] [Google Scholar]
- 15.Visser H, Rodig T, Hermann KP. Dose reduction by direct-digital cephalometric radiography. Angle Orthod. 2001;71(3):159–63. doi: 10.1043/0003-3219(2001)071<0159:DRBDDC>2.0.CO;2. [DOI] [PubMed] [Google Scholar]