

Abstract
Introduction
The aim of this study was to describe and compare the changes in ventilator management and complications over time, as well as variables associated with 28-day hospital mortality in patients receiving mechanical ventilation (MV) after cardiac arrest.
Methods
We performed a secondary analysis of three prospective, observational multicenter studies conducted in 1998, 2004 and 2010 in 927 ICUs from 40 countries. We screened 18,302 patients receiving MV for more than 12 hours during a one-month-period. We included 812 patients receiving MV after cardiac arrest. We collected data on demographics, daily ventilator settings, complications during ventilation and outcomes. Multivariate logistic regression analysis was performed to calculate odds ratios, determining which variables within 24 hours of hospital admission were associated with 28-day hospital mortality and occurrence of acute respiratory distress syndrome (ARDS) and pneumonia acquired during ICU stay at 48 hours after admission.
Results
Among 812 patients, 100 were included from 1998, 239 from 2004 and 473 from 2010. Ventilatory management changed over time, with decreased tidal volumes (VT) (1998: mean 8.9 (standard deviation (SD) 2) ml/kg actual body weight (ABW), 2010: 6.7 (SD 2) ml/kg ABW; 2004: 9 (SD 2.3) ml/kg predicted body weight (PBW), 2010: 7.95 (SD 1.7) ml/kg PBW) and increased positive end-expiratory pressure (PEEP) (1998: mean 3.5 (SD 3), 2010: 6.5 (SD 3); P <0.001). Patients included from 2010 had more sepsis, cardiovascular dysfunction and neurological failure, but 28-day hospital mortality was similar over time (52% in 1998, 57% in 2004 and 52% in 2010). Variables independently associated with 28-day hospital mortality were: older age, PaO2 <60 mmHg, cardiovascular dysfunction and less use of sedative agents. Higher VT, and plateau pressure with lower PEEP were associated with occurrence of ARDS and pneumonia acquired during ICU stay.
Conclusions
Protective mechanical ventilation with lower VT and higher PEEP is more commonly used after cardiac arrest. The incidence of pulmonary complications decreased, while other non-respiratory organ failures increased with time. The application of protective mechanical ventilation and the prevention of single and multiple organ failure may be considered to improve outcome in patients after cardiac arrest.
Electronic supplementary material
The online version of this article (doi:10.1186/s13054-015-0922-9) contains supplementary material, which is available to authorized users.
Introduction
Many studies in patients after cardiac arrest with return of spontaneous circulation (ROSC) focus on how to improve survival and neurological outcomes. Despite several interventions, such as targeted temperature management [1-4], vasopressor drugs [5], control of seizures and blood sugar level [6], poor neurological outcome and mortality are still as high as 50% [4,7,8].
However, other organ failures should be considered in addition to neurological damage. Roberts et al. reported that the highest cardiovascular- and respiratory-specific Sequential Organ Failure Assessment (SOFA) scores are associated with higher in-hospital mortality in 203 post-cardiac arrest patients [9], suggesting the value of hemodynamic and respiratory optimization. A recent study demonstrated that the outcomes of mechanically ventilated patients have improved over time [10]. The characteristics and the influence of ventilator settings, that is, tidal volume and positive end-expiratory pressure (PEEP), on organ failure and outcome of patients after cardiac arrest have not been previously described.
The main aim of this study was to describe and compare the changes in ventilator management and complications over time. Secondary objectives were to investigate the potential risk factors associated with 28-day hospital mortality and development of pulmonary complications, namely acute respiratory distress syndrome (ARDS) and pneumonia acquired during intensive care unit (ICU) stay, in patients without pre-existing lung injury at ICU admission.
Methods
Study design
We performed a secondary analysis of three prospective observational cohort studies conducted in 1998 [11], 2004 [12] and 2010 [10] on adult patients (≥18-years-old) who received mechanical ventilation for more than 12 hours, and was performed in a total of 927 ICUs in 40 countries. National coordinators recruited local investigators from eligible ICUs (see Additional file 1). In order to minimize practice changes in response to observation, only the investigator and research coordinators at each site were aware of the exact purpose and timing of the study. The research ethics board of each participating institution approved the protocol and need for informed consent was according to local rules [10-12]. Please see Additional file 1 for details of each participant institution.
Protocol and data collection
From the 18,302 patients enrolled, we included 812 patients (4.4%) who received mechanical ventilation after ROSC post-cardiac arrest for the purpose of this analysis. The eligible patients were those receiving mechanical ventilation caused by developing sudden cessation of cardiopulmonary function.
We collected data on baseline characteristics and blood gas measurements at ICU admission, daily ventilator settings, clinical management, and blood gas measurements, characteristics and observed complications while patients were ventilated or up to day 28. We also collected data on ICU, in-hospital and 28-day mortality and length of stay outcomes. Detailed descriptions of the variables collected, along with their definitions have previously been published [10-12]. In brief, complications arising during the course of the mechanical ventilation was defined as ARDS, pneumonia, sepsis and/or multiorgan failure (cardiovascular, respiratory, renal, hepatic and hematologic, defined as a score higher than two points on the SOFA scale. Pneumonia acquired during ICU stay was defined by modifying Centers for Disease Control and Prevention criteria which require the presence of a new radiographic infiltrate persistent for 48 hours or more plus a body temperature of more than 38.5°C or less than 35.0°C, a leukocyte count of more than 10,000/μL or less than 3,000/μL, purulent sputum or change in character of sputum, or isolation of pathogenic bacteria from an endotracheal aspirate [11].
In the 1998 cohort, data on height and Glasgow Coma Score (GCS) were not collected; therefore no data regarding tidal volume/kg predicted body weight (PBW) were available in that group. The use of neuromuscular blocking agents, sedatives and analgesic drugs was recorded daily for 28 days when the drugs were given daily for three or more hours. The onset of weaning was the time point when the physician considered the patient ready for spontaneous ventilation. Weaning was categorized as a trial of spontaneous breathing and gradual reduction in the level of ventilator support. We recorded date of extubation, date of any reintubation and tracheostomy, if and when performed. Patients were prospectively followed until hospital discharge.
Statistical analysis
Data are expressed as mean (standard deviation), median (interquartile range) and absolute and relative frequencies, as appropriate. One-way analysis of variance (ANOVA) were used to compare continuous variables, and chi-square tests were used for categorical variables. We rejected the null hypothesis of no difference among cohorts at a nominal significance level of 0.05.
Multivariate logistic regression analysis (backward stepwise) was performed to calculate odds ratios determining which variables within 24 hours of hospital admission were associated with 28-day hospital mortality. The variables with a P value less than 0.1 in univariate analysis were included in multivariate analysis. Variables considered for inclusion in multivariate analysis associated with 28-day mortality were age, PaO2, arterial pH (pHa), use of sedative agents, cardiovascular dysfunction and renal failure during the first 24 hours of mechanical ventilation.
For the purpose of the analysis, we categorized pHa as the following: pHa <7.35, pHa 7.35 to 7.45 and pHa >7.45, according to the normal pHa range, which is 7.35 to 7.45. PaO2 was categorized as the following: PaO2 <60 mmHg, PaO2 60 to 300 mmHg and PaO2 ≥300 mmHg, according to recent publications which demonstrated that PaO2 <60 mmHg and PaO2 ≥300 mmHg were independently associated with in-hospital mortality [13-15]. We did not include GCS in the multivariate analysis because during mechanical ventilation with sedation, the GCS is unreliable. In addition, GCS data was not collected in 1998. Odds ratios with 95% confidence intervals were calculated for statistically significant variables to determine independent predictors of mortality. These analyses were performed using SPSS version 16.0, SPSS for Windows, SPSS Inc., Chicago, USA.
The development of pulmonary complications, namely ARDS and pneumonia acquired during ICU stay, in patients without pre-existing lung injury at ICU admission were collected. We also performed multivariate logistic regression analysis to determine which variables within 24 hours of hospital admission were associated with the occurrence of ARDS and pneumonia acquired during ICU stay at 48 hours after admission. We excluded patients with diagnosed ARDS at admission. The variables considered for inclusion in the analysis were age, pHa, plateau pressure, PaO2 and sepsis during the first 24 hours of hospital admission.
Results
Characteristics of included patients and management during mechanical ventilation
In Table 1, baseline characteristics between the three cohorts are shown. Baseline characteristics including age, body mass index, gender and Simplified Acute Physiology Score (SAPS) were not different across the cohort time periods. At admission, the most significant difference was the lower GCS in patients included in 2010 versus patients included in 2004 (in 1998 this variable was not registered).
Table 1.
Baseline characteristics and management during mechanical ventilation of included patients
| Cohort 1998 | Cohort 2004 | Cohort 2010 | P | |
|---|---|---|---|---|
| (N = 100) | (N = 239) | (N = 473) | ||
| Age, years, mean (SD) | 66 (14) | 63 (16) | 63 (16) | 0.261 |
| Female, n (%) | 37 (37) | 90 (38) | 174 (37) | 0.966 |
| Body mass index, kg/cm2, mean (SD) | na | 27 (8) | 27 (7) | 0.754 |
| SAPS II, points, mean (SD) | 61 (19) | 56 (20) | 59 (20) | 0.060 |
| Glasgow Coma Score at admission, median (IQR) | na | 6 (3-15) | 3 (3-8) | <0.001 |
| Arterial blood gases at admission | ||||
| pHa, mean (SD) | 7.17 (0.09) | 7.23 (0.20) | 7.23 (0.18) | 0.003 |
| PaCO2, mmHg, mean (SD) | 50 (13) | 48 (22) | 50 (23) | 0.733 |
| Ratio PaO2 to FiO2, mmHg, mean (SD) | 249 (78) | 233 (116) | 221 (186) | 0.367 |
| Ventilatory settings during mechanical ventilation | ||||
| Tidal volume, ml/kg ABW, mean (SD) | 8.9 (2) | 7.4 (2) | 6.7 (2) | <0.001 |
| Tidal volume/kg PBW mean (SD) | na | 9.04 (2.3) | 7.95 (1.7) | <0.001 |
| Respiratory rate, bpm, mean (SD) | 17 (4) | 18 (6) | 19 (6) | <0.001 |
| PEEP, cmH2O, mean (SD) | 3.5 (3) | 4.8 (4) | 6.5 (3) | <0.001 |
| Peak pressure, cmH2O, mean (SD) | 29.1 (7.5) | 27.1 (7.9) | 24.1 (7.9) | <0.001 |
| Plateau pressure, cmH2O, mean (SD) | 22.7 (3.7) | 21.5 (6.5) | 19.5 (6.3) | <0.001 |
| PaCO2, , mmHg, mean (SD) | 37.3 (7.4) | 38.8 (10.4) | 39.8 (11.7) | <0.001 |
| pHa, mean (SD) | 7.41 (0.08) | 7.39 (0.1) | 7.39 (0.1) | <0.001 |
| Ratio PaO2 to FiO2, mmHg, mean (SD) | 238 (95) | 242 (95) | 252 (114) | <0.05 |
| Sedation, n (%) | 50 (50) | 175 (73) | 332 (70) | <0.001 |
| Analgesia, n (%) | 20 (20) | na | 272 (58) | <0.001 |
| Neuromuscular blocking, n (%) | 8 (8) | 29 (12) | 99 (21) | <0.001 |
ABW, actual body weight; IQR, interquartile range; na, no data available, PCV, Pressure controlled ventilation; PEEP, Positive end-expiratory pressure; pHa, arterial pH; SAPS, Simplified Acute Physiology Score; SD, standard deviation.
As shown in Figure 1, the mode of mechanical ventilation, expressed as days of use per 1,000 days of invasive mechanical ventilation, changed over time with a significant increase of pressure support ventilation (PSV) and pressure regulated volume control (PRVC), and a significant decrease of other considered modes. Among ventilation settings over the years we found a significant reduction in tidal volume, peak and plateau pressure, and a significant increase of respiratory rate, PEEP and PaCO2. Sedation, analgesia and neuromuscular blocking were frequently used in 2010 (Table 1). At 24 hours after ICU admission, in patients with ARDS compared to those without ARDS at ICU admission, tidal volume and respiratory rate were similar (7.3 (standard deviation (SD) 1.8) ml/kg actual body weight (ABW) versus 7.5 (SD 2) ml/kg ABW, P = 0.613, and 18.1 (SD 5.9) rate/min versus 17.7 (SD 5.5) rate/min, P = 0.658), while applied PEEP was higher (7.3 (SD 4.5) cmH2O versus 5.2 (SD 3.1) cmH2O, P = 0.000).These results mentioned overall patients (including 1998, 2004 and 2010).
Figure 1.
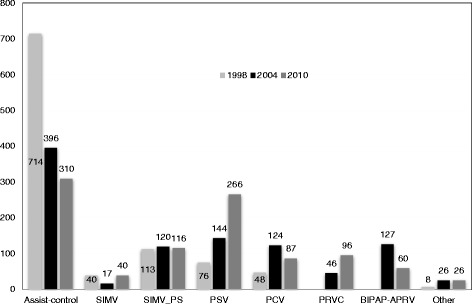
Mode of ventilation and days of use per 1,000 days of invasive mechanical ventilation from 1998, 2004 and 2010. Days during weaning from mechanical ventilation process are excluded (light gray square symbol = 1998, black square symbol = 2004 and dark gray square symbol = 2010)*. SIMV, synchronized intermittent mandatory ventilation; SIMV_PS, synchronized intermittent mandatory ventilation with pressure support; PSV, pressure support ventilation; PCV, pressure control ventilation; PRVC, pressure regulated volume control ventilation; APRV, airway pressure release ventilation; BIPAP, biphasic positive airway pressure. *Among three years, days of use per 1,000 days of invasive mechanical ventilation in each mode of ventilation are statistically significant difference (P <0.001).
Complications during mechanical ventilation
As shown in Table 2, the incidence of pneumonia acquired during ICU stay decreased from 13% in 1998 to 4% in 2010 (P = 0.001). In the meantime, other non-respiratory organ failures like sepsis, cardiovascular dysfunction, neurological and hepatic failure significantly increased.
Table 2.
Comparison of complications emerged over the course of mechanical ventilation
| Cohort 1998 | Cohort 2004 | Cohort 2010 | P | |
|---|---|---|---|---|
| (N = 100) | (N = 239) | (N = 473) | ||
| Acute respiratory distress syndrome, n (%) | 4 (4) | 7 (3) | 31 (7) | 0.102 |
| Acquired intensive care unit pneumonia, n (%) | 13 (13) | 14 (6) | 18 (4) | 0.001 |
| Sepsis, n (%) | 3 (3) | 6 (6.5) | 89 (19) | <0.001 |
| Barotrauma, n (%) | 2 (2) | 6 (3) | 7 (2) | 0.62 |
| Cardiovascular failure, n (%) | 25 (25) | 46 (19) | 229 (48) | <0.001 |
| Renal failure, n (%) | 20 (20) | 60 (25) | 140 (30) | 0.104 |
| Hepatic failure, n (%) | 2 (2) | 30 (13) | 24 (5) | <0.001 |
| Hematological failure, n (%) | 11 (11) | 17 (7) | 31 (7) | 0.296 |
| Neurological failurea Glasgow coma scale, median (IQR) | na | 4 (3-10) | 3 (3–6) | <0.001 |
aLowest Glasgow Coma Scale during the ventilatory support.
na, no data available; IQR, interquartile range.
Withdrawal from mechanical ventilation
Table 3 demonstrates the characteristics of variables related to the weaning process across the three cohort time periods. The percentage of patients who were weaned and extubated was similar over time (47% in 1998, 44% in 2004 and 45% in 2010; P = 0.856). Among weaning methods, spontaneous breathing trial was more commonly used than gradual reduction of ventilator support. PSV was mostly used among gradual reduction of support methods, and its use tended to increase (12.5% in 1998, 78% in 2004 and 38% in 2010). In the spontaneous breathing trial group, the most common method was low-level PSV. Tracheostomy was performed in 13.8% of patients overall, and did not change significantly over time.
Table 3.
Comparison of variables related to weaning process
| Cohort 1998 | Cohort 2004 | Cohort 2010 | P | |
|---|---|---|---|---|
| (N = 100) | (N = 239) | (N = 473) | ||
| Accidental extubation, n (%)a | 3 (3) | 6 (3) | 29 (6) | 0.062 |
| Reintubation, % | 67 | 33 | 14 | 0.074 |
| Patients weaned and scheduled extubated, n (%) | 47 (47) | 104 (44) | 211 (45) | 0.856 |
| Method for first attempt | ||||
| Spontaneous breathing trial, n (%) | 33/47 (70) | 71/104 (68) | 154/211(73) | 0.675 |
| T-piece, % | 48.5 | 38 | 36 | 0.022 |
| CPAP, % | 6 | 34 | 24 | |
| Low level pressure support, % | 42 | 27 | 40 | |
| Other, % | 3 | 1 | 0 | |
| Gradual reduction of support, n (%) | 14/47 (30) | 33/104 (32) | 57/211 (27) | 0.675 |
| Pressure support, % | 14 | 61 | 89 | <0.001 |
| SIMV, % | 29 | 6 | 0 | |
| SIMV-PS, % | 50 | 18 | 9 | |
| Other, % | 7 | 15 | 2 | |
| Failure of first weaning attempt, n (%) | 24/47 (51) | 45/104 (43) | 95/211 (45) | 0.667 |
| Method for second attempt | ||||
| Spontaneous breathing trial, n (%) | 21 (87.5) | 10 (22) | 59 (62) | <0.001 |
| T-piece, % | 67 | 40 | 36 | 0.049 |
| CPAP, % | 5 | 20 | 34 | |
| Low level pressure support, % | 24 | 40 | 30 | |
| Other, % | 5 | 0 | 0 | |
| Gradual reduction of support, n (%) | 3 (12.5) | 35 (78) | 36 (38) | <0.001 |
| Pressure support, % | 0 | 66 | 94 | <0.001 |
| SIMV, % | 0 | 6 | 0 | |
| SIMV-PS, % | 100 | 14 | 3 | |
| Other, % | 0 | 14 | 3 | |
| Reintubation after scheduled extubation, % | 11 | 7 | 11 | 0.426 |
| Tracheotomy, n (%)a | 12 (12) | 30 (13) | 66 (14.5) | 0.758 |
aExcluded patients with prior tracheostomy: 1 patient in 1998, 7 patients in 2004 and 18 patients in 2010.
SIMV, synchronized intermittent mandatory ventilation; SIMV-PS, synchronized intermittent mandatory ventilation with pressure support; PSV, pressure support ventilation; CPAP, continuous positive airway pressure.
Outcomes
We observed significant differences in the duration of ventilatory support over time, with a longer duration of mechanical ventilation in the most recent study of 2010 (Table 4). There were no differences in length of stay in the ICU or in the hospital (Table 4).
Table 4.
Comparison of outcomes
| Cohort 1998 | Cohort 2004 | Cohort 2010 | P | |
|---|---|---|---|---|
| (N = 100) | (N = 239) | (N = 473) | ||
| Days of mechanical ventilation, median (IQR)a | 4 (3–7) | 5 (3–9) | 6 (4–10) | <0.001 |
| Length of stay in the intensive care unit, days, median (IQR) | 7 (3–11) | 6 (4–12) | 6 (3–12) | 0.925 |
| Length of stay in the hospital, days, median (IQR) | 14 (7–27) | 13 (6–24) | 12 (6–26) | 0.934 |
| Mortality in the intensive care unit, n (%) | 44 (44) | 115 (48) | 223 (49) | 0.785 |
| Mortality at day 28, n (%) | 52 (52) | 137 (57) | 246 (52) | 0.384 |
| Mortality in the hospital, n (%) | 57 (57) | 143 (60) | 259 (55) | 0.434 |
aIncluding time devoted to weaning from mechanical ventilation. IQR: interquartile range.
There was no difference in 28-day hospital mortality over time (52% in 1998, 57% in 2004 and 52% in 2010 (Table 4).
Factors associated with 28-day hospital mortality
Table 5 shows the univariate and logistic regression analysis for 28-day hospital mortality of cardiac arrest patients.
Table 5.
Univariate and logistic regression analysis for 28-day mortality of cardiac arrest patients
| Variable | Univariate analysis Odds ratio (95% CI) | P | Logistic regression Odds ratio (95% CI) | P |
|---|---|---|---|---|
| Age, yearsa | 1.02 (1.01–1.03) | 0.002 | 1.01 (1.00–1.03) | 0.010 |
| SAPS II score, pointsa | 1.03 (1.02–1.03) | <0.001 | ||
| Glasgow Coma Scale, pointsb | 0.92 (0.88–0.95) | <0.001 | ||
| PaO2 60–300 mmHgb | 1 (reference) | 1 (reference) | ||
| PaO2 <60 mmHg | 2.23 (1.05–4.72) | 0.036 | 2.71 (1.06–6.95) | 0.038 |
| PaO2 ≥300 mmHg | 1.19 (0.76–1.85) | 0.444 | 0.89 (0.54–1.46) | 0.640 |
| pHa 7.35–7.45b | 1 (reference) | 1 (reference) | ||
| Acidosis (pHa <7.35) | 1.48 (1.07–2.04) | 0.017 | 1.40 (0.98–2.02) | 0.068 |
| Alkalosis (pHa >7.45) | 1.07 (0.67–1.71) | 0.770 | 1.20 (0.71–2.02) | 0.491 |
| PaCO2 35–45 mmHgb | 1 (reference) | |||
| PaCO2 <35 mmHg | 1.20 (0.86–1.68) | 0.277 | ||
| PaCO2 >45 mmHg | 0.94 (0.70–1.41) | 0.973 | ||
| Tidal Volume/PBWml/kgb | ||||
| Tidal Volume/PBW 6–8 ml/kg | 1 (reference) | |||
| Tidal Volume/PBW <6 ml/kg | 1.01 (0.51–2.02) | 0.975 | ||
| Tidal Volume/PBW >8 ml/kg | 0.76 ( 0.55–1.06) | 0.111 | ||
| PEEP cmH2Ob | ||||
| PEEP 6–8 cmH2O | 1 (reference) | |||
| PEEP <6 cmH2O | 1.35 (0.94–1.95) | 0.100 | ||
| PEEP >8 cmH20 | 0.86 (0.52–1.42) | 0.556 | ||
| Pplat cmH2Ob | ||||
| Pplat 28–30 cmH2O | 1 (reference) | |||
| Pplat <28 cmH2O | 0.58 (0.28–1.22) | 0.149 | ||
| Pplat >30 cmH2O | 0.64 (0.22–1.89) | 0.421 | ||
| Use of sedative drugsb | 0.61 (0.46–0.81) | 0.001 | 0.51 (0.36–0.72) | 0.000 |
| Cardiovascular failure/shock (yes/no)b,c | 1.53 (1.15–2.03) | <0.001 | 1.65 (1.17–2.32) | 0.004 |
| ARDS (yes/no)b,c | 3.14 (1.41–6.97) | 0.005 | ||
| Renal failure (yes/no)b,c | 1.35 (0 .95–1.91) | 0.095 | 1.34 (0.91–1.95) | 0.135 |
| Hepatic failure (yes/no)b,c | 1.20 (0.72–2.00) | 0.483 | ||
| Sepsis (yes/no)b,c | 1.38 (0.88–2.18) | 0.163 | ||
| Hematologic failure (yes/no)b,c | 1.05 (0.51–2.17) | 0.885 |
SAPS, Simplified Acute Physiology Score; PBW, predicted body weight; ml, milliliters; kg, kilograms PEEP, positive end-expiratory pressure; Pplat, plateau pressure; pHa, arterial pH; ARDS, acute respiratory distress syndrome; PaO2, partial pressure of oxygen in arterial blood; PaCO2, partial pressure of carbon dioxide in arterial blood; CI, confidence interval.
aAge and SAPS score were collected as baseline characteristics, bValues within 24 hours from admission, cthe absence of organ failure as the reference value.
In the multivariate analysis, older age, PaO2 <60 mmHg, less use of sedative drugs and the presence of cardiovascular dysfunction within 24 hours from hospital admission were found to be associated with 28-day hospital mortality (odds ratio 1.01, 95% confidence interval 1.00 to 1.03; odds ratio 2.71, 95% confidence interval 1.06 to 6.95; odds ratio 0.51, 95% confidence interval 0.36 to 0.72; and odds ratio 1.65, 95% confidence interval 1.17 to 2.32, respectively).
Factors associated with acute respiratory distress syndrome and ICU-acquired pneumonia
At multivariate analysis, in patients without lung injury at admission, the potential risk factor for the development of ARDS 48 hours after ICU stay was higher plateau pressure (odds ratio 1.12, 95% confidence interval 1.04 to 1.21), while those associated with ICU pneumonia acquired during ICU stay were higher tidal volume and lower applied PEEP levels (odds ratio 1.003, 95% confidence interval 1.0003 to 1.01; and odds ratio 0.89, 95% confidence interval 0.80 to 0.99, respectively).
Discussion
In this large retrospective analysis of prospective observational cohort, we described the evolution of ventilator management, and the occurrence of pulmonary and other non-respiratory organ failure over time. Furthermore, we investigated variables associated with 28-day hospital mortality and the occurrence of ARDS and/or pneumonia acquired during ICU stay among cardiac arrest patients undergoing mechanical ventilation. We found that: the use of protective and assisted mechanical ventilation increased from 1998 to 2010; pulmonary complications decreased, while cardiovascular and neurological complications, and sepsis increased with years; independent risk factors for 28-day hospital mortality were older age, PaO2 <60 mmHg, less use of sedative drugs and the presence of cardiovascular dysfunction at 24 hours after ICU admission; and in patients without lung injury at ICU admission, higher tidal volume, higher plateau pressure and lower PEEP in the first 24 hours were independent potential risk factors for developing ARDS or pneumonia acquired during ICU stay.
To our knowledge, this is the first study describing ventilator management in a large sample of patients after cardiac arrest undergoing mechanical ventilation in ICU. Our results show that protective mechanical ventilation is increasingly used among patients after cardiac arrest. The implementation of protective mechanical ventilation was associated with a progressive reduction in pneumonia acquired during ICU stay over time, and a lower incidence of ARDS than that reported in mechanically ventilated patients [16,17]. Similar changes in ventilation pattern have recently been shown in a general population of critically ill patients, associated with a reduction of development of ARDS [10,18]. Protective ventilation with low tidal volume has been shown to be associated with a reduction in respiratory failure and mortality in non-ARDS lung patients [19,20], and postoperative complications after surgery [21,22]. In donors, protective mechanical ventilation increased the number of lungs eligible to be harvested compared to traditional mechanical ventilation [23]. The application of PEEP ranging from 5 to 8 cmH2O in non-hypoxemic patients decreased the incidence of ventilator-associated pneumonia [24]. Moreover, protocols aimed to prevent ventilator-associated pneumonia have been more widely implemented in recent years [25,26].
On the other hand, we observed an increased incidence of non-pulmonary organ failure (sepsis, cardiovascular dysfunction and neurological failure) over time, which may increase the duration of mechanical ventilation. The increase in non-pulmonary complications may be explained by the implementation of targeted temperature management protocols, or by higher incidence of aspiration, and thus sicker patients [7], which might predispose to infection and consequent multiple organ failure [27]. The significant differences in the duration of ventilatory support over time, with a longer duration in the most recent study of 2010, is probably because of the implementation of targeted temperature management protocols, and thus longer sedation.
A previous study demonstrated that changes in mechanical ventilation practice were associated with a significant decrease in mortality [10]. In post-cardiac arrest patients, despite the introduction of temperature management, percutaneous coronary intervention and standard operating procedures, we did not observe any change in mortality over the years, likely due to the balance between decreased pulmonary and increased extra-pulmonary incidence of complication. We also found that the main independent predictors of 28-day in-hospital mortality were older age, PaO2 <60 mmHg, use of sedative drug, and cardiovascular dysfunction within 24 hours from admission, in line with previous reports [14,15].
In the present study, the analysis by logistic regression demonstrated that PaO2 <60 mmHg is a predictor of 28-day hospital mortality. This result is different from previous meta-analysis showing that not only hypoxemia but also hyperoxemia are associated with higher in-hospital mortality [28]. The effects of high oxygen tension to increase neuronal damage after cardiac arrest are conflicting [13,14,29-31]. We also found that higher or lower PaCO2 level had no detectable association with mortality. This was different from previous studies showing that hypocarbia defined by PaCO2 <35 mmHg was associated with higher in-hospital mortality [28,32], while hypercapnia defined by PaCO2 >45 mmHg was associated with better outcome [33,34].
Use of sedative drugs was associated with 28-day mortality in this cohort. This finding is in contrast to other studies showing that sedation protocols did not affect mortality in a general population of critically ill patients [35]. We have no completed value of GCS for the three cohort years. The lower GCS on admission in the most recent cohort would indicate more severe brain injury, and thus a lower need for sedation and a higher risk of death. On the other hand, our data suggest that higher sedation in the early phase after cardiac arrest might promote less secondary brain injury and better implementation of protective mechanical ventilation. Furthermore, the use of sedative drugs may be related to the implementation of therapeutic hypothermia, which was associated with the improvement of outcome in ROSC patients [7,8].
In Table 1, 26% (63 out of 239) of the patients in the 2004 study had a GCS of 15. The study population included patients who developed cardiac arrest and needed mechanical ventilation due to sudden and unexpected cessation of cardiopulmonary functions in any rhythms (referred to any rhythms that cause cessation of cardiopulmonary functions i.e. Pulseless electrical activity, asystole, ventricular fibrillation and ventricular tachycardia); this is not the population included in target temperature management studies, therefore we expect that a higher percentage of patients awake upon arrival in ICU. Our study is comparable with the study by Gold et al. [36] on patients with out-of-hospital cardiac arrest of any rhythm, which demonstrated that of the 185 survivors, 96 patients (50%) were sufficiently awake upon arrival to the ICU so they did not meet the targeted temperature management protocol inclusion criteria, but data on GCS were not reported.
In our study, we evaluated the potential independent risk factors for development of pulmonary complications in patients without pre-existing lung injury at ICU admission. We found that higher tidal volume and higher plateau pressure with lower PEEP were associated with occurrence of lung worsening during ICU stay. These findings are in line with those reported in patients without lung injury in the perioperative period [19-22], and in the ICU [19], showing that protective ventilation by low tidal volume and plateau pressure <20 cmH2O resulted in a decreased incidence of pulmonary complications after initiation of mechanical ventilation [19-22,37]. We also found that tidal volume was similar, while PEEP was slightly higher in patients with ARDS compared to those without ARDS at ICU admission. This suggests that protective ventilation should include lower tidal volume than actually used in daily clinical practice in cardiac arrest patients with ARDS.
The use of controlled mechanical ventilation decreased, while pressure support increased with years. The use of assisted ventilation may be associated with potential advantages like the use of less sedative agents [38-40], better hemodynamic stability [39,40], less atrophy of respiratory muscles [41] and ventilator-associated lung injury [42,43]. The rate of tracheostomy was 12 to 14.5% higher than that reported in a general population of critically ill patients (11%) [12], and comparable to that reported in neurological patients (13%) [44]. This might be explained by the possible occurrence of residual neurological deficits in cardiac arrest patients due brain hypoxia impairing cough, swallowing and secretion clearance [45].
Our study has some limitations. First, this was a post-hoc analysis of previously collected available data, where the statistically significant predictors of mortality might have been influenced by undefined confounding factors, that is, site, cause and initial rhythm of the cardiac arrest. A statistical post-hoc analysis on 28-day hospital mortality was performed to assess the power of mortality variation among the years, and showed a power of less than 50%, so the variation of mortality over years should be interpreted with caution. Second, our study focused on the details related to mechanical ventilation. Thus, we did not record possible implementation of targeted temperature management, including the details related to the causes of cardiac arrest [46]. However, a recent study showed that moderate hypothermia did not affect mortality compared to mild hypothermia [4]. Third, although the GCS was found to be associated with 28-day mortality in the univariate analysis, we did not include GCS in the multivariate analysis. Since the evaluation of GCS is not reliable within the first 72 hours during mechanical ventilation with sedation, and data were not collected in 1998. The lower GCS on admission in the most recent cohort would indicate more severe brain injury, and thus lower need for sedation and higher risk of death.
Fourth, we also did not have access to cardiac arrest-related variables, like whether the arrest was witnessed or not, whether bystander cardiopulmonary resuscitation was performed, initial presenting rhythm and the time of resuscitation commencement or return of spontaneous circulation. Fifth, in the multivariate logistic regression analysis defining risk factors associated with 28-day hospital mortality and the development of ARDS and/or pneumonia acquired in ICU, we used data collected within 24 hours after admission, therefore there were very few missing data. Nevertheless, we used variables regardless of the different years, which might have been affected by the change of clinical management, and the number of patients with development of ARDS and/or pneumonia acquired in ICU is a small portion of the whole population (5% of the total population). For this reason, the results of multivariate analysis should be interpreted with caution.
Conclusions
Protective mechanical ventilation with lower tidal volume and higher PEEP is more commonly used after cardiac arrest. The incidence of pulmonary complications decreased, while other non-respiratory organ failures increased with time. The application of protective mechanical ventilation and the prevention of single and multiple organ failure may be considered to improve outcome in patients after cardiac arrest.
Key messages
The use of protective mechanical ventilation in patients after cardiac arrest increased from 1998 to 2010, and is associated with a decrease in pulmonary complications.
Variables independently associated with 28-day in-hospital mortality were: older age, PaO2 <60 mmHg, cardiovascular dysfunction and less use of sedative agents.
The application of protective mechanical ventilation and the prevention of single and multiple organ failures may be considered to improve outcome in patients after cardiac arrest.
Acknowledgments
We are grateful to all investigators of the VENTILA study group for collecting data for this article (see Additional file 1). The VENTILA study was supported by Centro de Investigación Biomédica en Red de Enfermedades Respiratorias (CIBERES), Instituto de Salud Carlos III, Madrid, Spain. Dr Ferguson is supported by a Canadian Institutes of Health Research New Investigator Award (Ottawa, Canada). The funding organizations had no role in the design or conduct of the study, collection, management, analysis, or interpretation of the data, or preparation, review, or approval of the manuscript.
Abbreviations
- ABW
Actual body weight
- ARDS
Acute respiratory distress syndrome
- pHa
Arterial pH
- GCS
Glasgow Coma Score
- ICU
Intensive care unit
- PBW
Predicted body weight
- PEEP
Positive end-expiratory pressure
- PRVC
Pressure regulated volume control
- PSV
Pressure support ventilation
- ROSC
Return of spontaneous circulation
- SAPS
Simplified acute physiology score
- SOFA
Sequential organ failure assessment score
- SD
standard deviation
Additional file
Participants in three international cohort studies on mechanical ventilation (1998, 2004 and 2010). National coordinators recruited local investigators from eligible intensive care units. The research ethics board of each participating institution approved the protocol and need for informed consent was according to local rules.
Footnotes
Competing interests
Dr Bernd W Böttiger is a director of Science and Research of European Resuscitation Council. Dr Niklas Nielsen received payment for lecture from BARD medical (not related to the current article). Dr Pravin Amin is the consultant of CIPLA, was the consultant of Boehringer Ingelheim and Smiths Medical, and received payment for lecture from MSD, Fresenius Kabi and Aventis (not related to the current article). The remaining authors have disclosed that they do not have any potential conflicts of interest.
Authors’ contributions
YS was responsible for conception and design, analysis and interpretation, manuscript writing and final approval of the manuscript. OP, FF and AE were responsible for conception and design, data interpretation and final approval of the manuscript. AM was responsible for data analysis and interpretation. MV, IB and DD were responsible for data analysis and interpretation, and final approval of the manuscript. NN, NF and BB were responsible for manuscript writing, review of the manuscript, study design and analysis of the data. KR, AT, AD, JH, FR, CA, DV, NC, MG, BD, MK, AS, YK, RM, PA, VT, LS, HB and AA were responsible for data acquisition and review of the manuscript. PP was responsible for conception and design, data interpretation, manuscript writing and final approval of the manuscript. All authors read and approved the final manuscript.
Contributor Information
Yuda Sutherasan, Email: sutherasan_yuda@yahoo.com.
Oscar Peñuelas, Email: openuelas@gmail.com.
Alfonso Muriel, Email: alfonso.muriel@hrc.es.
Maria Vargas, Email: vargas.maria82@gmail.com.
Fernando Frutos-Vivar, Email: ffrutos@ucigetafe.com.
Iole Brunetti, Email: ibrunetti@tin.it.
Konstantinos Raymondos, Email: raymondos@ards.eu.
Davide D’Antini, Email: davide.dantini@hotmail.it.
Niklas Nielsen, Email: niklas.nielsen@med.lu.se.
Niall D Ferguson, Email: n.ferguson@utoronto.ca.
Bernd W Böttiger, Email: bernd.boettiger@uk-koeln.de.
Arnaud W Thille, Email: aw.thille@gmail.com.
Andrew R Davies, Email: andrew.davies@monash.edu.
Javier Hurtado, Email: jhurtado@hc.edu.uy.
Fernando Rios, Email: fernandrios@gmail.com.
Carlos Apezteguía, Email: capez@intramed.net.
Damian A Violi, Email: damianalejandro.violi@gmail.com.
Nahit Cakar, Email: cakarn@istanbul.edu.tr.
Marco González, Email: mga@une.net.co.
Bin Du, Email: dubin98@gmail.com.
Michael A Kuiper, Email: mi.kuiper@wxs.nl.
Marco Antonio Soares, Email: marcreis@uai.com.br.
Younsuck Koh, Email: yskoh@amc.seoul.kr.
Rui P Moreno, Email: r.moreno@mail.telepac.pt.
Pravin Amin, Email: pamin@vsnl.com.
Vinko Tomicic, Email: vtomicic@alemana.cl.
Luis Soto, Email: lusoro@ctcinternet.cl.
Hans-Henrik Bülow, Email: hhbulow@dadlnet.dk.
Antonio Anzueto, Email: anzueto@uthscsa.edu.
Andrés Esteban, Email: aesteban@ucigetafe.com.
Paolo Pelosi, Email: ppelosi@hotmail.com.
References
- 1.Kim YM, Yim HW, Jeong SH, Klem ML, Callaway CW. Does therapeutic hypothermia benefit adult cardiac arrest patients presenting with non-shockable initial rhythms?: a systematic review and meta-analysis of randomized and non-randomized studies. Resuscitation. 2012;83:188–96. doi: 10.1016/j.resuscitation.2011.07.031. [DOI] [PubMed] [Google Scholar]
- 2.Lundbye JB, Rai M, Ramu B, Hosseini-Khalili A, Li D, Slim HB, et al. Therapeutic hypothermia is associated with improved neurologic outcome and survival in cardiac arrest survivors of non-shockable rhythms. Resuscitation. 2012;83:202–7. doi: 10.1016/j.resuscitation.2011.08.005. [DOI] [PubMed] [Google Scholar]
- 3.Peberdy MA, Callaway CW, Neumar RW, Geocadin RG, Zimmerman JL, Donnino M, et al. Part 9: post-cardiac arrest care: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122:S768–86. doi: 10.1161/CIRCULATIONAHA.110.971002. [DOI] [PubMed] [Google Scholar]
- 4.Nielsen N, Wetterslev J, Cronberg T, Erlinge D, Gasche Y, Hassager C, et al. Targeted temperature management at 33 degrees C versus 36 degrees C after cardiac arrest. N Engl J Med. 2013:2197–206. doi:10.1056/NEJMoa1310519 [DOI] [PubMed]
- 5.Mentzelopoulos SD, Malachias S, Chamos C, Konstantopoulos D, Ntaidou T, Papastylianou A, et al. Vasopressin, steroids, and epinephrine and neurologically favorable survival after in-hospital cardiac arrest: a randomized clinical trial. JAMA. 2013;310:270–9. doi: 10.1001/jama.2013.7832. [DOI] [PubMed] [Google Scholar]
- 6.Morrison LJ, Neumar RW, Zimmerman JL, Link MS, Newby LK, McMullan PW, Jr, et al. Strategies for improving survival after in-hospital cardiac arrest in the United States: 2013 consensus recommendations: a consensus statement from the American Heart Association. Circulation. 2013;127:1538–63. doi: 10.1161/CIR.0b013e31828b2770. [DOI] [PubMed] [Google Scholar]
- 7.Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–63. doi: 10.1056/NEJMoa003289. [DOI] [PubMed] [Google Scholar]
- 8.Hypothermia after Cardiac Arrest Study G Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549–56. doi: 10.1056/NEJMoa012689. [DOI] [PubMed] [Google Scholar]
- 9.Roberts BW, Kilgannon JH, Chansky ME, Mittal N, Wooden J, Parrillo JE, et al. Multiple organ dysfunction after return of spontaneous circulation in postcardiac arrest syndrome. Crit Care Med. 2013;41:1492–501. doi: 10.1097/CCM.0b013e31828a39e9. [DOI] [PubMed] [Google Scholar]
- 10.Esteban A, Frutos-Vivar F, Muriel A, Ferguson ND, Penuelas O, Abraira V, et al. Evolution of mortality over time in patients receiving mechanical ventilation. Am J Respir Crit Care Med. 2013;188:220–30. doi: 10.1164/rccm.201212-2169OC. [DOI] [PubMed] [Google Scholar]
- 11.Esteban A, Anzueto A, Frutos F, Alia I, Brochard L, Stewart TE, et al. Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study. JAMA. 2002;287:345–55. doi: 10.1001/jama.287.3.345. [DOI] [PubMed] [Google Scholar]
- 12.Esteban A, Ferguson ND, Meade MO, Frutos-Vivar F, Apezteguia C, Brochard L, et al. Evolution of mechanical ventilation in response to clinical research. Am J Respir Crit Care Med. 2008;177:170–7. doi: 10.1164/rccm.200706-893OC. [DOI] [PubMed] [Google Scholar]
- 13.Kilgannon JH, Jones AE, Parrillo JE, Dellinger RP, Milcarek B, Hunter K, et al. Relationship between supranormal oxygen tension and outcome after resuscitation from cardiac arrest. Circulation. 2011;123:2717–22. doi: 10.1161/CIRCULATIONAHA.110.001016. [DOI] [PubMed] [Google Scholar]
- 14.Kilgannon JH, Jones AE, Shapiro NI, Angelos MG, Milcarek B, Hunter K, et al. Association between arterial hyperoxia following resuscitation from cardiac arrest and in-hospital mortality. JAMA. 2010;303:2165–71. doi: 10.1001/jama.2010.707. [DOI] [PubMed] [Google Scholar]
- 15.Bellomo R, Bailey M, Eastwood GM, Nichol A, Pilcher D, Hart GK, et al. Arterial hyperoxia and in-hospital mortality after resuscitation from cardiac arrest. Crit Care. 2011;15:R90. doi: 10.1186/cc10090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Irish Critical Care Trials G. Acute lung injury and the acute respiratory distress syndrome in Ireland: a prospective audit of epidemiology and management. Crit Care. 2008;12:R30. doi:10.1186/cc6808. [DOI] [PMC free article] [PubMed]
- 17.Brun-Buisson C, Minelli C, Bertolini G, Brazzi L, Pimentel J, Lewandowski K, et al. Epidemiology and outcome of acute lung injury in European intensive care units. Results from the ALIVE study. Intensive Care Med. 2004;30:51–61. doi: 10.1007/s00134-003-2022-6. [DOI] [PubMed] [Google Scholar]
- 18.Yilmaz M, Keegan MT, Iscimen R, Afessa B, Buck CF, Hubmayr RD, et al. Toward the prevention of acute lung injury: protocol-guided limitation of large tidal volume ventilation and inappropriate transfusion. Crit Care Med. 2007;35:1660–6. doi: 10.1097/01.CCM.0000269037.66955.F0. [DOI] [PubMed] [Google Scholar]
- 19.Serpa Neto A, Cardoso SO, Manetta JA, Pereira VG, Esposito DC, Pasqualucci Mde O, et al. Association between use of lung-protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syndrome: a meta-analysis. JAMA. 2012;308:1651–9. doi: 10.1001/jama.2012.13730. [DOI] [PubMed] [Google Scholar]
- 20.Sutherasan Y, Vargas M, Pelosi P. Protective mechanical ventilation in the non-injured lung: review and meta-analysis. Crit Care. 2014;18:211. doi: 10.1186/cc13778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Futier E, Constantin JM, Paugam-Burtz C, Pascal J, Eurin M, Neuschwander A, et al. A trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Engl J Med. 2013;369:428–37. doi: 10.1056/NEJMoa1301082. [DOI] [PubMed] [Google Scholar]
- 22.Severgnini P, Selmo G, Lanza C, Chiesa A, Frigerio A, Bacuzzi A, et al. Protective mechanical ventilation during general anesthesia for open abdominal surgery improves postoperative pulmonary function. Anesthesiology. 2013;118:1307–21. doi: 10.1097/ALN.0b013e31829102de. [DOI] [PubMed] [Google Scholar]
- 23.Mascia L, Pasero D, Slutsky AS, Arguis MJ, Berardino M, Grasso S, et al. Effect of a lung protective strategy for organ donors on eligibility and availability of lungs for transplantation: a randomized controlled trial. JAMA. 2010;304:2620–7. doi: 10.1001/jama.2010.1796. [DOI] [PubMed] [Google Scholar]
- 24.Manzano F, Fernandez-Mondejar E, Colmenero M, Poyatos ME, Rivera R, Machado J, et al. Positive-end expiratory pressure reduces incidence of ventilator-associated pneumonia in nonhypoxemic patients. Crit Care Med. 2008;36:2225–31. doi: 10.1097/CCM.0b013e31817b8a92. [DOI] [PubMed] [Google Scholar]
- 25.Resar R, Pronovost P, Haraden C, Simmonds T, Rainey T, Nolan T. Using a bundle approach to improve ventilator care processes and reduce ventilator-associated pneumonia. Jt Comm J Qual Patient Saf. 2005;31:243–8. doi: 10.1016/s1553-7250(05)31031-2. [DOI] [PubMed] [Google Scholar]
- 26.Ricard JD, Conti G, Boucherie M, Hormann C, Poelaert J, Quintel M, et al. A European survey of nosocomial infection control and hospital-acquired pneumonia prevention practices. J Infect. 2012;65:285–91. doi: 10.1016/j.jinf.2012.06.016. [DOI] [PubMed] [Google Scholar]
- 27.Geurts M, Macleod MR, Kollmar R, Kremer PH, van der Worp HB. Therapeutic hypothermia and the risk of infection: a systematic review and meta-analysis. Crit Care Med. 2013:231–42. doi:10.1097/CCM.0b013e3182a276e8 [DOI] [PubMed]
- 28.Sutherasan Y, Vargas M, Brunetti I, Pelosi P. Ventilatory targets after cardiac arrest. Minerva Anestesiol. 2015;81:39–51. [PubMed] [Google Scholar]
- 29.Pilcher J, Weatherall M, Shirtcliffe P, Bellomo R, Young P, Beasley R. The effect of hyperoxia following cardiac arrest - A systematic review and meta-analysis of animal trials. Resuscitation. 2012;83:417–22. doi: 10.1016/j.resuscitation.2011.12.021. [DOI] [PubMed] [Google Scholar]
- 30.Neumar RW. Optimal oxygenation during and after cardiopulmonary resuscitation. Curr Opin Crit Care. 2011;17:236–40. doi: 10.1097/MCC.0b013e3283454c8c. [DOI] [PubMed] [Google Scholar]
- 31.Vaahersalo J, Bendel S, Reinikainen M, Kurola J, Tiainen M, Raj R, et al. Arterial blood gas tensions after resuscitation from out-of-hospital cardiac arrest: associations with long-term neurologic outcome. Crit Care Med. 2014;42:1463–70. doi: 10.1097/CCM.0000000000000228. [DOI] [PubMed] [Google Scholar]
- 32.Schneider AG, Eastwood GM, Bellomo R, Bailey M, Lipcsey M, Pilcher D, et al. Arterial carbon dioxide tension and outcome in patients admitted to the intensive care unit after cardiac arrest. Resuscitation. 2013;84:927–34. doi: 10.1016/j.resuscitation.2013.02.014. [DOI] [PubMed] [Google Scholar]
- 33.Eastwood GM, Young PJ, Bellomo R. The impact of oxygen and carbon dioxide management on outcome after cardiac arrest. Current opinion in critical care. 2014;20(3):266–72. doi: 10.1097/MCC.0000000000000084. [DOI] [PubMed] [Google Scholar]
- 34.Roberts BW, Kilgannon JH, Chansky ME, Mittal N, Wooden J, Trzeciak S. Association between postresuscitation partial pressure of arterial carbon dioxide and neurological outcome in patients with post-cardiac arrest syndrome. Circulation. 2013;127:2107–13. doi: 10.1161/CIRCULATIONAHA.112.000168. [DOI] [PubMed] [Google Scholar]
- 35.de Wit M, Gennings C, Jenvey WI, Epstein SK. Randomized trial comparing daily interruption of sedation and nursing-implemented sedation algorithm in medical intensive care unit patients. Crit Care. 2008;12:R70. doi: 10.1186/cc6908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Gold B, Puertas L, Davis SP, Metzger A, Yannopoulos D, Oakes DA, et al. Awakening after cardiac arrest and post resuscitation hypothermia: are we pulling the plug too early? Resuscitation. 2014;85:211–4. doi: 10.1016/j.resuscitation.2013.10.030. [DOI] [PubMed] [Google Scholar]
- 37.Futier E, Constantin JM, Jaber S. Protective lung ventilation in operating room: a systematic review. Minerva Anestesiol. 2014;80:726–35. [PubMed] [Google Scholar]
- 38.Fan E, Khatri P, Mendez-Tellez PA, Shanholtz C, Needham DM. Review of a large clinical series: sedation and analgesia usage with airway pressure release and assist-control ventilation for acute lung injury. J Intensive Care Med. 2008;23:376–83. doi: 10.1177/0885066608324293. [DOI] [PubMed] [Google Scholar]
- 39.Henzler D, Pelosi P, Bensberg R, Dembinski R, Quintel M, Pielen V, et al. Effects of partial ventilatory support modalities on respiratory function in severe hypoxemic lung injury. Crit Care Med. 2006;34:1738–45. doi: 10.1097/01.CCM.0000218809.49883.54. [DOI] [PubMed] [Google Scholar]
- 40.Kaplan LJ, Bailey H, Formosa V. Airway pressure release ventilation increases cardiac performance in patients with acute lung injury/adult respiratory distress syndrome. Crit Care. 2001;5:221–6. doi: 10.1186/cc1027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Demoule A, Jung B, Prodanovic H, Molinari N, Chanques G, Coirault C, et al. Diaphragm dysfunction on admission to the intensive care unit. Prevalence, risk factors, and prognostic impact-a prospective study. Am J Respir Crit Care Med. 2013;188:213–9. doi: 10.1164/rccm.201209-1668OC. [DOI] [PubMed] [Google Scholar]
- 42.Spieth PM, Carvalho AR, Pelosi P, Hoehn C, Meissner C, Kasper M, et al. Variable tidal volumes improve lung protective ventilation strategies in experimental lung injury. Am J Respir Crit Care Med. 2009;179:684–93. doi: 10.1164/rccm.200806-975OC. [DOI] [PubMed] [Google Scholar]
- 43.Spieth PM, Guldner A, Beda A, Carvalho N, Nowack T, Krause A, et al. Comparative effects of proportional assist and variable pressure support ventilation on lung function and damage in experimental lung injury. Crit Care Med. 2012;40:2654–61. doi: 10.1097/CCM.0b013e3182592021. [DOI] [PubMed] [Google Scholar]
- 44.Pelosi P, Ferguson ND, Frutos-Vivar F, Anzueto A, Putensen C, Raymondos K, et al. Management and outcome of mechanically ventilated neurologic patients. Crit Care Med. 2011;39:1482–92. doi: 10.1097/CCM.0b013e31821209a8. [DOI] [PubMed] [Google Scholar]
- 45.Gurkin SA, Parikshak M, Kralovich KA, Horst HM, Agarwal V, Payne N. Indicators for tracheostomy in patients with traumatic brain injury. Am Surg. 2002;68:324–8. [PubMed] [Google Scholar]
- 46.Dumas F, Grimaldi D, Zuber B, Fichet J, Charpentier J, Pene F, et al. Is hypothermia after cardiac arrest effective in both shockable and nonshockable patients?: insights from a large registry. Circulation. 2011;123:877–86. doi: 10.1161/CIRCULATIONAHA.110.987347. [DOI] [PubMed] [Google Scholar]