

Abstract
A 30-year-old man with a history of epilepsy and substance misuse presented to the hospital with status epilepticus. Difficult seizure control necessitated anaesthetising the patient followed by intubation and ventilation. A clonidine infusion was started as the patient developed withdrawal syndrome and was difficult to wean off mechanical ventilation. Once the withdrawal syndrome was controlled, the clonidine was abruptly stopped. Two hours after stopping the infusion, the patient developed high-grade fever, severe hypertension, tachycardia, profound sweating and lacrimation. The patient then developed respiratory distress syndrome secondary to acute pulmonary oedema. Clonidine withdrawal as a cause of such response was proposed. Reversal of symptoms and successful reweaning was achieved by restarting a low-dose clonidine infusion followed by slow downward titration and use of oral clonidine as a step-down measure. The patient was subsequently discharged from the intensive care unit.
Background
Clonidine is a centrally acting α-agonistic agent often used on an unapproved basis-to-treat withdrawal syndrome in critical care. It is also used as an antihypertensive agent. Clonidine withdrawal, although mentioned as a potential side effect of cessation, is not common and hence few reports exist. This case of clonidine withdrawal demonstrates a life-threatening withdrawal response. Therefore, this case is presented to characterise a catastrophic sympathetic surge that, if not rapidly diagnosed, can lead to significant morbidity and mortality.
Case presentation
A 31-year-old man was brought to the intensive care unit (ICU) after admission with status epilepticus. This was on a history of poorly controlled epilepsy, alcohol abuse and frequent cannabis use. The patient was initially kept sedated using propofol and alfentanil with clonidine. The clonidine was started to aid weaning of sedation as he developed agitated withdrawal syndrome. The propofol and alfentanil were stopped on day 5 and the patient successfully extubated. The clonidine was weaned down from 120 µg/h to nil over a subsequent 10 h period. Approximately 3 h postcessation, the patient developed a blood pressure of 330/90 mm Hg, a heart rate of 155 bpm and respiratory rate of 44 breaths/min. His temperature rapidly climbed to 40.9°C and he acutely desaturated to 86% despite oxygen therapy with an arterial blood gas (table 1) revealing type 1 respiratory failure.
Table 1.
Arterial blood gas results
| pH | pO2 | pCO2 | BE | HCO3− | Lactate |
|---|---|---|---|---|---|
| 7.55 | 6.80 kPa | 2.33 kPa | −6.7 mmol/L | 20.3 mmol/L | 1.4 mmol/L |
Investigations
Pre-event, the patient’s C reactive protein and white cell count were 113 mg/L and 7.8×109/L, respectively. Postevent these had surged to 308 mg/L and 31.8×109/L, respectively. Creatine kinase and troponin were both normal. A chest radiograph performed during the crisis revealed acute-onset features of widespread bilateral pulmonary oedema (figure 1A, B). A CT of his head was normal, while a CT of the thorax confirmed features of pulmonary oedema (figure 2).
Figure 1.
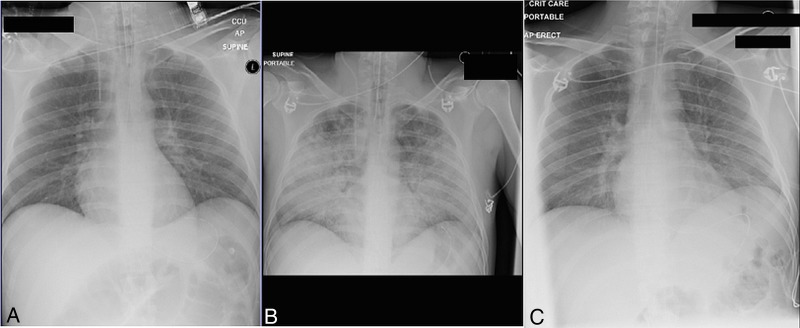
Chest radiograph series before (A), during (B) and after (C) sympathetic surge.
Figure 2.
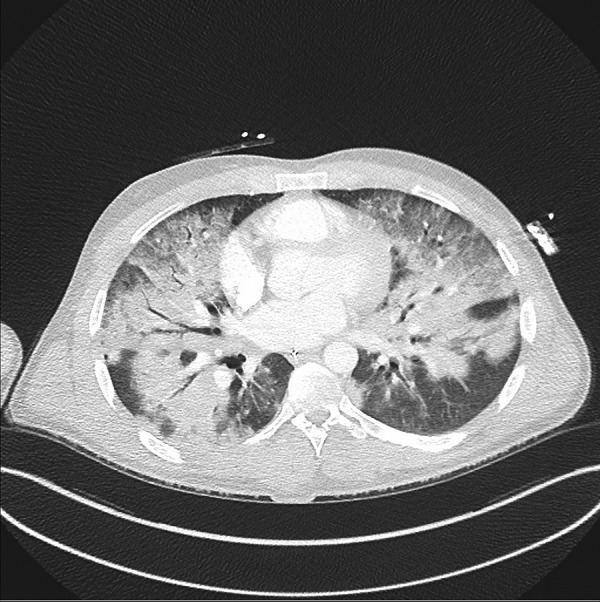
CT of the thorax revealing widespread pulmonary oedema immediately after initial surge stabilisation.
Differential diagnosis
Although, in this case, with the clinical information provided clonidine withdrawal is likely, other differential diagnoses could not initially be discounted. Malignant hyperthermia is characterised by high oxygen requirements, tachypnoea and tachycardia. If not treated early, patients will go on to develop muscle rigidity, hyperthermia and rhabdomyolysis. While this patient had the majority of these features, there was no muscle rigidity observed and his creatine kinase levels remained normal. Importantly, as well, the patient had not received any depolarising muscle relaxants in excess of 4 days prior to the event and had not received any inhalational anaesthetic agents, the two most common causes of malignant hyperthermia.1
Neuroleptic malignant syndrome is another well-identified adverse drug reaction, related to the start or abrupt dosage increase of dopamine antagonists. It is typified by four cardinal features: muscle rigidity, hyperpyrexia, mental status changes and autonomic stability. ‘Lead pipe’ rigidity is commonly described, which is accompanied by an elevated creatine kinase in the vast majority of cases.2 Mental status changes involve stupor, coma, delirium and catatonia. This patient remained in a distressed, but unaltered, mental state during this acute episode. He had no history of dopamine antagonist use, nor had he been prescribed any during his admission. Another possible adverse drug reaction related to psychiatric medication is serotonin syndrome, which is associated with serotonin agonist polypharmacy. It causes a triad of neuromuscular hyperactivity, autonomic instability and altered mental state. Patients typically present within 6 h of starting a second drug with serotonergic effects.3 This patient was not on serotonin agonists either prior to, or during his admission, nor did he develop muscle rigidity.
Sudden cessation of clonidine is associated with agitation, headache and a rapid sympathetic surge. Acute withdrawal is documented in case reports going as far back as the 1970s.4 However, these generally relate to patients who had been taking the drug orally for years followed by abrupt cessation. Since awareness regarding the risks of sudden withdrawal are high, this outcome is increasingly rare. In this case, the patient received treatment for a total duration of 43 h prior to cessation, and over the final 10 h this dose was gradually titrated downwards from 120 µg/h. Inspite of this, in this scenario, the most likely underlying cause is that of clonidine withdrawal.
Treatment
The patient was immediately given 40 mg of labetalol, and resedated and reintubated using propofol, midazolam and alfentanil. The clonidine infusion was restarted. He was actively cooled using ice packs, intravenous fluid and an ‘Arctic Sun’ targeted temperature control system. This was successful with normalisation of physiology within 2 h of onset. An acute hypertensive crisis has the ability to precipitate aortic dissection in individuals with an already diseased aorta.5 A coincidental undiagnosed diseased aorta would have been extremely unlikely, but due to the potentially catastrophic circumstances of this being allowed to go undiagnosed, the patient was taken for a CT of his thorax, which revealed no dissection.
Outcome and follow-up
In the following 24 h there were significant amounts of pink frothy secretions consistent with pulmonary oedema. This improved rapidly over 72 h with intravenous furosemide (figure 1C). A bedside echocardiogram revealed no cardiogenic cause for the pulmonary oedema and no other abnormality. Post-event, the patient was kept sedated with the aid of a clonidine infusion. He was successfully weaned off sedation and extubated 5 days postevent. The same day, the clonidine was weaned to a rate of 90 µg/h and the patient was stepped down to an oral dose of 600 µg four times per day (with overlap of approximately 2 h to allow the oral clonidine to take effect). The patient remained stable throughout this transition period. The clonidine dose was subsequently reduced every 2–3 days by 100 µg per dose without any subsequent withdrawal signs or symptoms.
Discussion
Clonidine is an antagonist of α-adrenergic receptors in the brain causing inhibition of sympathetic vasomotor centres and therefore reduces blood pressure and heart rate. However, as well as doing this, clonidine will reduce noradrenergic signalling, which is often upregulated during acute withdrawal from opioids and benzodiazepines.6 Clonidine induces a mild sedative state from which patients are easily roused and therefore is widely used in ICUs to reduce the duration of sedation required, ease the transition between sedation and wakefulness and help facilitate ventilator weaning. The main potentially adverse effect of clonidine use is withdrawal. This is a well-described phenomenon and is attributed to cessation of adrenal catecholamine secretion blockade and a subsequent surge in their circulating levels.7 In many cases, this reaction can be retrospectively confirmed through the measurement of urinary catecholamines, which may be elevated for up to 5 days post event. As previously alluded to, withdrawal is mainly seen in patients with sudden cessation of clonidine treatment lasting in excess of months.4 The incidence of such withdrawal is difficult to ascertain and the occurrence of withdrawal hypertensive crises when weaning is carried out is almost certainly extraordinarily rare.8
The recommended initial management is through concurrent α and β-adrenergic receptor blockade. Only using non-selective β-blockade will have the effect of increasing peripheral resistance and therefore worsen hypertension in this scenario. Dual blockade is easiest achieved using a drug such as labetalol, but phentolamine and propranolol is an alternative option discussed in much of the literature.4 7 8 Alternatives in using these agents include hydralazine and diazoxide. Once initial blood pressure control has been regained, the most effective treatment is restarting of clonidine. The most common adverse effects of a hypertensive crisis such as this are cerebral infarction/haemorrhage, encephalopathy, congestive heart failure and pulmonary oedema. These should be managed according to routine protocols. Inspite of the similarities with malignant hyperthermia and neuroleptic malignant syndrome, in terms of presenting symptoms, there is no evidence that the use of dantrolene provides any benefit as the pathological processes are unrelated.
There is no guidance as to what rate weaning should be undertaken in general, let alone in individuals who have had previous withdrawal reactions. Weaning regimes as conservative as reducing the dose at a rate of 50 µg every third day have been reported to induce acute withdrawal reactions.9 The reality of practice is that for the greater majority, weaning rates far exceeding this take place without incident. The literature suggests that one should consider both the previous duration of clonidine use and the previous dosing prior to starting a weaning regime. In general, the longer patients have been on clonidine the longer the weaning period. Inspite of the lack of recommended weaning rates, the use of oral clonidine as a step-down agent is a reasonable intermediate step. This is ideally undertaken when the total intravenous or infusion dose falls below that of the oral dose to ensure there is no drop in clonidine levels during this transition. This can then be reduced in a stepwise approach over an individually assessed period, most likely in the region of days to weeks. Blood pressure monitoring on each reduction in dose can be carried out to monitor for the onset of any adverse reaction.
Learning points.
Clonidine is an important drug in facilitating ventilator weaning and extubation.
Weaning regimes will vary with individuals but all should be closely monitored during this phase for acute withdrawal reactions.
Concurrent α and β-blockade is the recommended first-line treatment if withdrawal occurs.
Future weaning should be carried out cautiously, with oral clonidine a useful intermediate step down.
Footnotes
Contributors: RM originally managed this case. MS wrote the report. RM was involved in overseeing and editing.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Hopkins P. Malignant hyperthermia: advances in clinical management and diagnosis. Br J Anaesth 2000;28:118–28. 10.1093/bja/85.1.118 [DOI] [PubMed] [Google Scholar]
- 2.Perry P, Wilborn C. Serotonin syndrome vs neuroleptic malignant syndrome: a contrast of causes, diagnoses and management. Ann Clin Psychiatry 2012;24:155–62. [PubMed] [Google Scholar]
- 3.Thanacoody R. Serotonin syndrome. Medicine 2012;40:63–4. 10.1016/j.mpmed.2011.11.005 [DOI] [Google Scholar]
- 4.Sachdev Y, Evered D, Hall R. Rapid clonidine withdrawal with blood pressure overshoot exaggerated by beta-blockade. BMJ 1976;1:942–3. 10.1136/bmj.1.6015.942 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Criado F, Coselli J. Aortic dissection. Tex Heart Inst J 2011;38:694–700. [PMC free article] [PubMed] [Google Scholar]
- 6.Liatsi D, Tsapas B, Smaro P et al. Respiratory, metabolic and hemodynamic effects of clonidine in ventilated patients presenting with withdrawal syndrome. Intensive Care Med 2009;35:275–81. 10.1007/s00134-008-1251-0 [DOI] [PubMed] [Google Scholar]
- 7.Hunyor S, Hannson L, Harrison T et al. Effects of clonidine withdrawal: possible mechanisms and suggestions for management. BMJ 1973;2:209–11. 10.1136/bmj.2.5860.209 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Karachalios G, Charalabopoulos A, Papalimneou V et al. Withdrawal syndrome following cessation of antihypertensive drug therapy. Int J Clin Pract 2005;59:562–70. 10.1111/j.1368-5031.2005.00520.x [DOI] [PubMed] [Google Scholar]
- 9.Ahuja A. Rebound hypertension following withdrawal of clonidine. Psychiatr Bull 2007;31:274–5. 10.1192/pb.31.7.274c [DOI] [Google Scholar]