

Abstract
The illicit recreational drug of abuse, γ-hydroxybutyrate (GHB) is a potent central nervous system depressant and is often encountered during forensic investigations of living and deceased persons. The sodium salt of GHB is registered as a therapeutic agent (Xyrem®), approved in some countries for the treatment of narcolepsy-associated cataplexy and (Alcover®) is an adjuvant medication for detoxification and withdrawal in alcoholics. Trace amounts of GHB are produced endogenously (0.5-1.0 mg/L) in various tissues, including the brain, where it functions as both a precursor and a metabolite of the major inhibitory neurotransmitter γ-aminobutyric acid (GABA). Available information indicates that GHB serves as a neurotransmitter or neuromodulator in the GABAergic system, especially via binding to the GABA-B receptor subtype. Although GHB is listed as a controlled substance in many countries abuse still continues, owing to the availability of precursor drugs, γ-butyrolactone (GBL) and 1,4-butanediol (BD), which are not regulated. After ingestion both GBL and BD are rapidly converted into GHB (t½ ~1 min). The Cmax occurs after 20-40 min and GHB is then eliminated from plasma with a half-life of 30-50 min. Only about 1-5% of the dose of GHB is recoverable in urine and the window of detection is relatively short (3-10 h). This calls for expeditious sampling when evidence of drug use and/or abuse is required in forensic casework. The recreational dose of GHB is not easy to estimate and a concentration in plasma of ~100 mg/L produces euphoria and disinhibition, whereas 500 mg/L might cause death from cardiorespiratory depression. Effective antidotes to reverse the sedative and intoxicating effects of GHB do not exist. The poisoned patients require supportive care, vital signs should be monitored and the airways kept clear in case of emesis. After prolonged regular use of GHB tolerance and dependence develop and abrupt cessation of drug use leads to unpleasant withdrawal symptoms. There is no evidence-based protocol available to deal with GHB withdrawal, apart from administering benzodiazepines.
Keywords: Analogues, γ-hydroxybutyrate (GBH), intoxication, overdose, pharmacodynamics, pharmacokinetics, treatment, withdrawal syndrome
INTRODUCTION
Among recreational drugs of abuse γ-hydroxybutyrate (GHB) is a particularly troublesome substance, because of its ready availability, low cost, and risk of adverse interaction with other sedative drugs [1-3]. Mortality rates after abuse of GHB are high, because there is only a narrow safety margin between a recreational dose and a fatal dose, which is only 5:1 to 8:1 [4-8]. Accordingly, accidental poisoning after recreational use of GHB is not uncommon as evidenced by admissions to hospital emergency departments for treatment [9, 10] and during forensic medical investigations of drug intoxication deaths [11-14].
GHB emerged as a recreational drug of abuse in the early 1990s and attracted considerable attention, especially when it was implicated in cases of drug facilitated sexual assault (DFSA), which is often referred to by the media as “daterape” [15-18]. Known by various slang or street names, such as “Easy Lay”, Georgia Home Boy”, “Juice”, “Liquid Ecstasy”, "Mils”, “G”, “Liquid X”, “Liquid G” and “Fantasy”, the abuse of GHB continues to unfold as evidenced by a continuous stream of scientific publications and media reports [19-22].
The classification of GHB as a controlled substance in USA in 2000 (schedule I) and in EU nations in 2001 (schedule III or IV) helped to limit its potential for abuse. In the UK possession of GHB is illegal and the drug is included under Class C of the misuse of drugs legislation. However, the organic solvents γ-butyrolactone (GBL) and 1,4-butanediol (BD), which are not regulated, are used as alternative sources of GHB. Both GBL and BD have cosmetic and industrial applications and are therefore not easy to classify as controlled substances [10, 23, 24]. These pro-drugs are rapidly converted in-vivo into GHB with an absorption half-life of about 1 min [25]. The pharmacological and behavioral effects of GBL and BD stem from their rapid conversion into GHB and the latter drug is the main analytical target in forensic toxicology [26].
Pharmacologically, GHB is classified as a central nervous system depressant and its mechanism of action involves interaction and binding to receptors for the major inhibitory neurotransmitter γ-aminobutyric acid (GABA), in particular the GABA-B complex [27, 28]. This differs from other sedative-hypnotics, such as ethanol, barbiturates and benzodiazepines, which work via the GABA-A receptor subtype and its chloride ion channel [29, 30].
In the form of its sodium salt, GHB is classified as a schedule III controlled substance according to US federal law. This pharmaceutical product has the proprietary name Xyrem ® and the generic name is sodium oxybate [31-33]. Xyrem® is a medication prescribed to adults suffering from narcolepsy-associated cataplexy [34]. Narcolepsy is a neurological disorder characterized by excessive daytime sleepiness and cataplexy is a brief loss of muscle tone, usually in response to emotional arousal or stimuli, such as laughter [32]. The patient’s daily dose (4.5 g) of Xyrem® should be taken immediately before bedtime and the swift absorption and short elimination half-life of GHB ensures that next morning insignificant amounts of parent drug remain un-metabolized in the blood.
In some European nations (e.g. Italy and Austria) the sodium salt of GHB (sodium oxybate) is registered as Alcover ® and made available by Laboratorio Farmaceutico C.T. (Sanremo, Italy) for use as pharmacotherapy to support alcoholics during detoxification and withdrawal [35, 36]. The administration of sodium oxybate seems to be effective in maintaining abstinence, with less craving for alcohol and lower rates of relapse compared with placebo treatment [37]. In contrast to bedtime use of Xyrem® for narcolepsy, Alcover® is taken ~4 times daily to alleviate withdrawal symptoms and reduce the craving for alcohol [38].
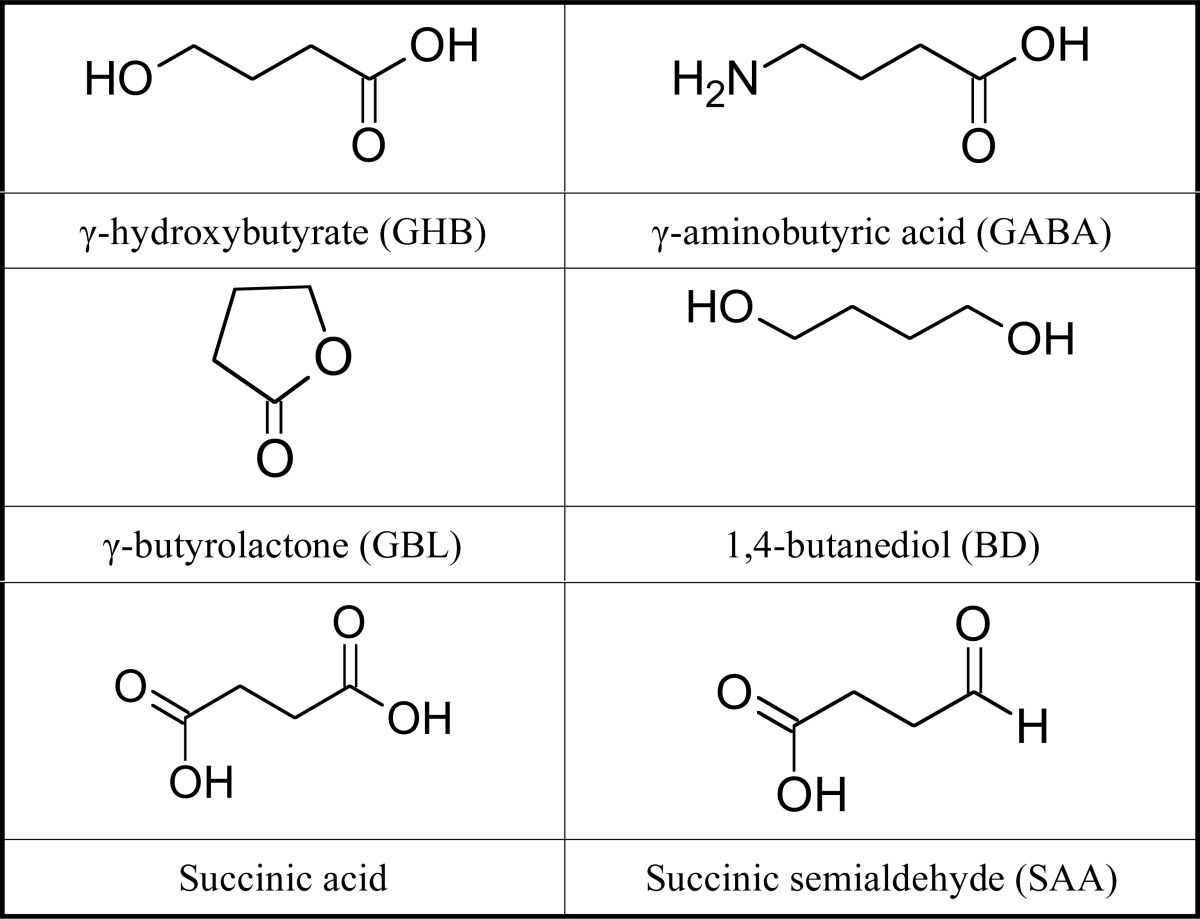
The chemical structures of GHB and related compounds including its precursors GBL and BD are shown in Table 1 in comparison with GABA and its metabolites. Another name for GHB is 4-hydroxybutyrate, which means that this short-chain carboxylic acid has a hydroxyl (-OH) group on carbon number four. The close proximity of an alcohol (-OH) and a carboxylic acid (-COOH) group within the same molecule allows cyclization to the corresponding lactone(γ-butyrolactone). This chemical conversion of GHB into GBL by intramolecular esterification is utilized when GHB is analyzed in blood and urine by GC-FID. The GBL derivative shows better solvent extraction and chromatographic properties compared with GHB [39].
Table 1.
Chemical structures of GHB and closely related low-molecular weight compounds
|
Clinical toxicologists are mainly concerned with acute intoxications caused by abuse of GHB and the best way to manage and treat the poisoned patient. However, there are no effective antidotes that can reverse the sedative effects of a GHB overdose. After recreational use of the drug it is not uncommon that people take an overdosing and suddenly become incapacitated with reduced levels of consciousness, which often requires emergency hospital treatment. This treatment is essentially supportive because rapid recovery is the norm as the drug is metabolized and blood concentrations decrease.
The quantitative analysis of GHB in blood and other body fluids is a relatively simple task and concentrations in blood of impaired drivers and intoxication deaths have been well documented. Care is needed when GHB concentrations in blood and urine samples are interpreted, because small amount of the drug is produced endogenously and whether the analytical result is indicative of exogenous intake is often not easy to answer [40, 41]. The concentrationsof GHB in blood and urine also seem to increase during storage of specimens, which requires use of realistic cut-off concentrations to distinguish intake of GHB from endogenous or post-sampling synthesis [42].
The interpretation of GHB concentrations is more tricky when dealing with specimens taken from dead bodies, because even higher concentrations are present in blood and urine without exposure to GHB during life [43]. Accordingly, in post-mortem toxicology higher cut-off concentrations are necessary to prevent any false accusations that a person had used GHB during the immediate ante-mortem period [44]. Much depends on the post-mortem interval, the amount of trauma to the body and addition of fluoride ions as an enzyme inhibitor and preservative and femoral or cardiac blood was taken for analysis [45-47].
This article is concerned with the pharmacology and toxicology of GHB with main focus on disposition and fate in the body, including pharmacokinetic and pharmacodynamic aspects. The endogenous concentrations of GHB in blood forensic cases including people arrested for driving under the influence of drugs (DUID), users of illicit drugs and medical examiner poisoning cases. The acute intoxication effects and clinical manifestations of GHB overdose are reviewed along with diagnosis and treatment of the withdrawal syndrome.
LITERATURE SEARCH
We searched Pubmed and Scopus data bases (from 1970 to 2014) using key-words γ-hydroxybutyrate; γ-butyrolactone; 1,4-butanediol; GHB; pharmacokinetics and pharma-codynamics of GHB. These key-words were searched alone or associated with GHB acute toxicity and GHB withdrawal syndrome. Several textbooks, non-indexed sources and government websites were also utilized. This search strategy located ~900 items, which were screened to find those deemed the most relevant for preparing the current review. Accordingly, ~300 articles were scrutinized in more detail and the main findings from the studies along with summary statistics are presented here.
The medical and forensic literature about GHB and its analogues is fairly extensive, including a number of fairly recent review articles. Worthy of note is a multi-national (France, New Zealand, Sweden and UK) review about the clinical toxicology of GHB, GBL and BD, which included 231 literature references [11]. Another newish review dealt with pharmacokinetic and pharmacodynamic aspects of GHB and included 84 references [13]. A third review focused more on acute toxicity and withdrawal syndromes after chronic use of GHB, GBL or BD and 124 references were cited [48]. A well written review from 2010 dealt with the involvement of GHB and its analogs in DFSA cases and the associated bibliography listed 164 references [49]. Two review articles, one about GHB and the other about BD, appeared in the prestigious New England Journal of Medicine [50, 51].
An important source of information about GHB, GBL and BD, as well as other drugs of abuse, comes from the reports published by the European Monitoring Center for Drugs and Drug Addiction (EMCDDA) in Lisbon, Portugal [52]. Their 2008 report on GHB and its precursor GBL should be essential reading for those interested in learning more about this class of recreational drug [53]. Likewise, the role of alcohol and other drugs, including GHB in DFSA cases was the subject of a 2008 report from EMCDDA [54]. The results showed that sedative-hypnotics were common “date-rape” drugs, probably because they make people less inhibited and more likely to take risks and after high doses they become drowsy and fall asleep. The victims of GHB intoxication tend to suffer from anterograde amnesia, making it difficult to recall events that precipitated the alleged sexual humiliation and abuse.
Another government body specializing in harmful effects of recreational drugs is the UK’s Advisory Council on the Misuse of Dugs (ADMD). This organization produced a well organized report about prevalence of GHB in alleged DFSA and the relative harmfulness as a recreational drug in society [55]. Likewise a joint WHO-EMCDDA report on GHB covered all aspects including the history, abuse potential, pharmacology, toxicology and dependence and withdrawal syndrome [56].
In 2011 the United Nations Office on Drugs and Crime (UNODC) produced a report with 204 supporting literature citations about the physiology, pharmacology and abuse of GHB. This report also contained guidelines for best possible sampling and analysis of body fluids in DFSA cases. This UN report concluded that ethanol was the psychoactive substance most often encountered in blood and/or urine from victims of sexual assault, but that use of other drugs also deserved consideration, especially when combined with ethanol [57]. Because of the short elimination half-life of GHB, it is imperative that samples of blood and urine for toxicology are obtained soon as possible. The report made the following statement [58].
“Due to the endogenous nature of GHB, caution must be taken in the interpretation of positive findings. GHB concentrations have been shown to increase in vitro in urine samples during the storage. Therefore, the actual recommended cut-off concentration for endogenous GHB in urine is 10 mg/L to help to distinguish endogenous from exogenous GHB.”
GHB TRENDS AND CONTEXT OF USE
In comparison with many other drugs of abuse, there is limited information available regarding trends and patterns of GHB use and its diffusion (including GHB analogues) in the general population [59, 60].
According to a recent EMCDDA report, the prevalence of GHB abuse is fairly low in most European nations and might be higher in specific areas (e.g. London) and more popular among sub-populations, such as those who frequent rave parties and gay nightclubs [61]. According to a 2003 survey by The Independent Drug Monitoring Unit (IDMU) abuse of GHB in UK peaked between 1994 and 2002, whereas only sporadic use was observed prior to 1994.
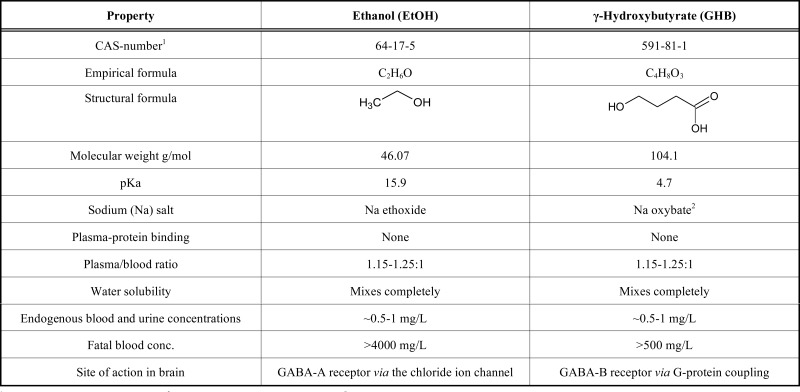
Because of the low cost of GHB compared with many other recreational drugs, adolescents who start to drink alcohol excessively switch to taking GHB, because in some respects the intoxicating effects are similar, including loss of inhibitions, euphoria etc. Table 2 gives a brief summary of the properties of ethanol and GHB and the way they act in the body.
Table 2.
Some characteristic properties of GHB compared with ethanol two recreational drugs often ingested together.
|
The average user of GHB is fairly young and many make their debut aged 15-22 y, although others start later in life, depending on their prior drug history, peer-group influences and their economic situation [62]. Among people arrested for driving under the influence of GHB in Norway [63] the average age of offenders was 28 y (range 21-41), which compares with an average age of 26 y (range 15-50 y) in Sweden [64].
The US National Institute of Drug Abuse (NIDA) sponsored a questionnaire survey to investigate prevalence of drug abuse throughout the 50 US states. Their 2013 report “Monitoring the Future” was recently released and part 1 dealt with secondary school students and part 2 college students and adults aged 19-50 y [65, 66]. In these reports, GHB is considered a “club drug” along with ketamine and rohypnol. The annual prevalence of GHB use was given as 1% and since 2000, the year when GHB was declared illegal, a steady decline in the consumption of this illegal drug by adolescents and young adults was noticed.
For a long time GHB as sodium oxybate was considered an orphan drug, although has now been registered as a pharmaceutical product and given the proprietary name Xyrem® (Jass Pharmaceuticals, Palo Alto, CA). The medication is used to treat cataplexy, which is an important symptom in the disease complex narcolepsy. This legitimate use of GHB raises a concern about the possible diversion of Xyrem® from a patient population to illicit use in a similar way to opioids, such as methadone.
Another therapeutic use of GHB (sodium oxybate, Alcover®) is adjunctive therapy for treating the alcohol withdrawal syndrome. This application of GHB was recently reviewed and found to be just as effective as diazepam or chlormethiazole in alleviating initial withdrawal symptoms and also as effective as naltrexone or disulfiram (Antabuse®) in maintaining abstinence and preventing relapse [36]. However, GHB is not recommended for certain patient groups, such as poly-drug users and those co-addicted or recovering from cocaine or heroin abuse.
Sometimes referred to as a ”club-drug” GHB became popular among young people attending nightclubs and rave parties in various countries, such as Australia, Holland, UK, and USA [24, 67]. Suggestions have been made that GHB might have some therapeutic potential for the treatment of depression and anxiety in certain patient categories, although this remains controversial considering the drug’s high abuse potential [68].
HISTORY OF GHB
The Russian chemist Alexander Saytzeff (1841-1910) synthesized GBL in 1874 by the reduction of succinyl chloride as was described in Liebigs Ann Chem“Ueber die reduction des succinylchlorids” [69]. The modern period of interest in GHB research began in the 1960s when the French physician Dr. Henri Laborit (1914-1995), of chlorpromazine fame, took an interest in studying the physiological effects of GHB. He noticed that GHB was a structural analogue of GABA, and unlike the latter was orally active and crossed the blood-brain barrier and therefore wondered if this might furnish an indirect way to increase GABA levels in the brain [41].
GHB is a structural isomer of β-hydroxybutyrate (BHB), the major ketone body, which is generated in excess during food deprivation and starvation. BHB provides an alternative fuel for the brain when glucose is lacking and glycogen stores are depleted [70]. This raises interesting questions about the respective roles of BHB and GHB on brain chemistry and functioning in man and animals during ketosis.
The experiments of Laborit demonstrated that GHB was a potent pharmacological agent and high doses resulted in deep sedation and sleep. This created an interest in the use of GHB as an intravenous anesthetic, because it had minimal cardiovascular and respiratory depression effects and the liver and the kidney function appeared normal. However, the clinical trials with GHB were disappointing because the drug possessed insufficient analgesic effect and the proper dose was difficult to judge and control. Some patients vomited and other suffered from convulsions, so medical testing of GHB in anesthesiology was abandoned in favor of much safer intravenous anesthetic agents (e.g ketamine, propofol). Nevertheless, GHB was registered in Germany for use as intravenous anesthetic (Somsanit®) requiring doses of 60-80 mg/kg body weight [71].
The relationship between plasma concentrations of GHB and state of consciousness after intravenous administration was reported in 1964 the results of which are summarized in Table 3 [72].
Table 3.
Relationship between plasma concentrations of GHB and state of consciousness after intravenous adminsitration. N = 16 patients received 50-115 mg/kg of GHB and afterwards the hypnotic effect was observed for 20-300 min post-dosing [72].
| Mean (Range) of GHB Concentration, mg/L | Clinical Observations/Hypnotic Effects1 |
|---|---|
| 311 (244-395) | Deep sleep (no response to stimuli) |
| 224 (151-293) | Medium sleep (blinking) |
| 135 (63-162) | Light sleep (occasioanl eye opening) |
| 47 (0-99) | Awake |
1The clinical effects lagged behind the peak plasma concentration.
During the 1970-1980s GHB became popular as a dietary supplement and could be purchased over the counter at health-food stores. The product became popular with dieters and body-builders who believed that it helped them burn fat and build muscle and also stimulated the production of growth hormone. The use and abuse of GHB spread to other groups of individuals in society and reports began to describe its use in criminal activity and many people overdoses and needed emergency medical treatment.
Throughout the 1980s and 1990s, GHB gained a reputation of being able to enhance their sex-drive and libido, which made it popular among people frequenting gay clubs and rave parties. After the right dose, people become more talkative and physically active, some experienced euphoria, had less inhibitions, which prompted them to take risks including multiple sex partners [67].
More serious from a forensic and legal standpoint was the growing number of reports that GHB and its analogs were used to spike a person’s drink causing incapacitation so a perpetrator could engage in non-consensual sex [17, 73, 74]. However, obtaining unequivocal evidence that GHB was in fact used for this purpose was a challenge, owing to the rapid metabolism and clearance from the body [49]. The rapid elimination of GHB meant that waiting too long after the crime was committed concentrations of GHB were close to the endogenous levels.
Nevertheless, the considerable media attention given to illicit use of GHB and its potential as a “date-rape” drug motivated the US Food and Drug Administration (FDA) to make GHB a controlled substance Schedule I (March 2000). However, because there are also legitimate medical uses for GHB, such for cataplexy attacks in patients with narcolepsy, in the form of sodium oxybate GHB was placed in schedule III as Xyrem®. According to the UK Misuse of Drugs Act in 2001 GHB was placed in schedule IV. The 1971 UN convention on psychotropic substances also classified GHB, thus making it a controlled substance in all EU nations.
ANALYTICAL METHODS
The methods currently available for screening and quantitative analysis of GHB in biological specimens were recently the subject of a comprehensive review with 128 references [39]. The authors documented a wide variety of analytical methods for determination of GHB in urine and blood as well as other biological specimens. These alternative specimens included saliva [75], vitreous humor [76-78], blood spots [79, 80] and hair strands [81-84].
For forensic purposes, the analytical approach recommended involves gas chromatography (GC) coupled with a flame ionization detector (FID), or better still a mass detector (MS) [85]. Use of GC-MS to analyze GHB means that deuterium labeled d6-GHB can be used as an internal standard after making the trimethylsilyl (TMS) derivative [86, 87]. Several liquid chromatography-mass spectrometry methods (LC-MS) are described for analysis of GHB and such technology is becoming used more and more in forensic laboratories [88-90].
The analytical “gold standard” method recommended for forensic purposes involves GC-MS or LC-MS or hybrid technology GC-MS/MS or LS-MS/MS [91-93]. These procedures are highly sensitive, accurate, precise and specific for their intended purposes. Use of high resolution GC-MS or LC-MS/MS have become the norm in clinical and forensic laboratories worldwide along with liquid chromato-graphy time of flight (TOF) mass spectrometry (LC-TOF-MS) and identification by accurate mass. Such technology is proving extremely useful for making a rapid screening and verification analysis of licit and illicit drugs in toxicological specimens [89, 94].
The review of analytical methods cited above endorsed the simpler GC-FID method after conversion of GHB into GBL at acidic pH and then quantitative chromatographic analysis of the more volatile GBL [39]. Preparation of the GBL derivative has the advantage of easier extraction into organic solvents and better chromatographic separation properties with sharp peaks and good linearity over a wide concentration range of 5-1000 mg/L [95].
A validated procedure that permitted simultaneous analysis of toxic glycols and GHB in plasma and urine by GC-MS was described [96]. The possibility to screen for multi-toxins in a single run is especially useful in clinical toxicology and emergency medicine. Another recent article described a method to determine GHB, GBL, BHB, BD as well as pregablin together in the same sample by a highly sensitive and specific UPLC-MS-MS method [88].
A number of simpler and more economical enzymatic methods are available for the analysis of GHB in biological fluids [97, 98]. One of these involves oxidation with the enzyme GHB dehydrogenase and the co-factor NAD+ which becomes reduced to NADH, and the later is determined quantitatively by UV spectrometry at 340 nM [99].
A recent photometric procedure was adapted to work with a Thermo Scientific MGC-240 auto-analyzer and this furnished a rapid method for determination of GHB in blood, vitreous humor and urine [97]. The authors reported a good correlation when paired samples were analyzed with a more specific GC-MS method. They recommended making an initial screening by the enzyme method and then verification of all positives by LC-MS or GC-MS.
In forensic toxicology casework, a good laboratory practice is to identify drugs and metabolites in more than one bio-fluid as definite proof of intake, such as when GHB-related deaths or DFSA cases are investigated. The presence and concentration of GHB in urine is of particular interest because this reflects the concentrations in blood during the time urine was produced in the kidney and stored in the bladder before voiding. In post-mortem toxicology if GHB is verified positive in urine but is below the analytical cut-off concentrations in blood, this can be interpreted as evidence of exogenous intake.
The verification of a parent drug and its main metabolite in blood or other biological material also strengthens the conclusion of exogenous intake. In this connection, GHB was recently identified in urine conjugated with glucuronic acid [100]. The concentrations of urinary GHB-glucuronide ranged from 0.11 to 5 mg/L (mean 1.3 mg/L, N = 50). In the same way that ethyl glucuronide is widely used as a biomarker of ethanol exposure, in the future it might be possible to utilize GHB-glucuronide as marker of GHB exposure [101, 102].
PHARMACODYNAMICS OF GHB
Fig. 1 shows the biosynthesis and metabolism of endogenous GHB along with formation from its exogenous precursors GBL and BD. GHB interferes with GABAergic neurotransmission and this drug can be considered a GABA-B agonist [103, 104]. The neurons that release GABA are mostly localized in the hippocampus, cortex and amygdala. GHB receptors are located in these sites, in pre- and post-synaptic cells and shows high affinity for these G-protein coupled receptors [105-108].
Fig. (1).

Metabolic inter-relationships between GHB and its precursors GBL and BD and the biosynthesis and degradation of the inhibitory neurotransmitter GA.
Unlike most other CNS depressants (e.g. ethanol, ben-zodiazepines) that work via the GABA-A receptor complex to dampen neuronal activity, GHB exerts most of its effects through binding to the GABA-B receptor complex [108, 109]. However, endogenous levels of GHB in the brain are too low to permit any agonist activity [106, 110]. The effects of GHB are mediated predominantly by interaction with GABA-B receptors [111], although some older animal studies implicate also dopamine and serotonin neuro-transmission [112]. GHB initially acts as an inhibitor of dopamine release, although depending on the dose turnover of dopamine is later increased [113]. The involvement of glutamate receptors (NMDA) was also thought to explain GHB-induced cataplexy in animal studies [114]. The existence of high affinity receptor binding sites for GHB distinct from GABA-B has been postulated to explain some of the pharmacological effects produced by this depressant drug [115, 116].
The onset of GHB's effects on performance and behavior occurs 15-30 min after ingestion and lasts for up to 1-6 hours depending on the dose. The dose-effect curve for GHB is rather steep, which means that small increases in dose cause disproportionate increases in behavioral effects and toxicity. For recreational purposes, GHB doses of 1-2 gram are often sufficient to produce feelings of euphoria and well being, but after larger doses people tend to become drowsy and as concentrations of GHB in blood increase above 100 mg/L there is marked effects on speech and motor coordination. Also important for the effects of GHB is the route of administration and whether other depressants were co-ingested and the development of tolerance.
After two healthy volunteers consumed 1.5 mL GBL, they experienced mild central nervous effects after 15 min, but these subsided completely 30 min later [117]. There is a low margin of safety between a recreational dose and a fatal dose because blood concentrations of 80-100 mg/L causes inebriation whereas 300-500 mg/L might result in death from respiratory depression and circulatory collapse.
PHARMACOKINETICS OF GHB
Information about the disposition and fate of GHB in the body has been obtained from several controlled human dosing studies covering a range from 12.5-50 mg/kg body weight, usually as sodium oxybate. The general conclusions from these pharmacokinetic studies are summarized in Table 4.
Table 4.
Summary of the disposition of GHB in the body administered as Xyrem® (sodium oxybate) based on the results from a large number of controlled human dosing studies.
| Pharmacokinetic Property or Characteristic of GHB | Findings from Controlled Human Dosing Studies Ranging from 12.5 to 72 mg/kg GHB |
|---|---|
| Absorption and bioavailability | Rapidly absorbed after oral administration, tmax was reached 20-40 min although oral bioavailability is only 25-40%.1 |
| Dose-proportionality | Non-linear kinetics, doubling the dose from 4.5 to 9.0 g increased area under the curve 3.8 fold and Cmax was increased 2.4-2.9 times. |
| Distribution | Distributes into total body water with a Vd ranging from 0.19-0.38 L/kg and negligible amounts of drug (<1%) bind to plasma proteins. |
| Metabolism | Approximately 95-98% of dose is metabolized in the liver to end products carboSn dioxide and water, via the Krebs cycle, and there are no active metabolites. |
| Plasma elimination kinetics | Dose dependent pharmacokinetics after high (toxic) doses enzymes are saturated with substrate and zero-order kinetics operates. After low therapeutic doses GHB is eliminated with a terminal plasma t½ of 30-50 min. |
| Excretion | Approximately 1-2% (<5%) of the dose is excreted unchanged in the urine. |
| Accumulation and enzyme induction | After repeated nightly doses of sodium oxybate (4.5 g) for 8 weeks, there was no accumulation of GHB in plasma and t½ was about the same for the first dose (43 min) and the 56th dose (46 min). |
1Depends on fed or fasting state
Three important pharmacokinetic (PK) parameters are Cmax, tmax and t½ and can be derived from the concentration-time profiles. The most recent pharmacokinetic study involved an oral dose of 25 mg/kg and was published in 2012 [118]. Table 5 presents values for Cmax, tmax and t½ from all relevant PK studies of GHB. The overall findings are clear-cut, namely GHB is rapidly absorbed from the gut and also rapidly eliminated from the body with a t½ of 30-50 min. This means that after 150-250 min (5 x t½) the concentrationsof GHB in plasma are barely measurable and hence the description fast-in and fast-out [119].
Table 5.
Summary of pharmacokinetic parameters Cmax, tmax and t½ for GHB derived from controlled human dosing studies in which GHB was administered as its sodium salt (sodium oxybate). Concentration-time curves of GHB were constructed from analysis of plasma or serum and not whole blood.
| Study [Reference] Year | Dose | N1 | Cmax, mg/L Mean/Median | Tmax, Min Mean/Median | Elimination Half-Life t½ Min |
|---|---|---|---|---|---|
| Abanades et al [122] 2006 | 40 mg/kg 50 mg/kg 60 mg/kg 72 mg/kg |
8 8 8 8 |
79 83 114 130 |
42 36 36 54 |
44 43 40 34 |
| Abanades et al [130] 2007 | 50 mg/kg | 5 | 83 | 36 | 43 |
| Borgen et al [125] 2003 | 4.5 g | 18 18 34 34 |
88 (men) 83 (women) 142 (fasted) 60 (fed)2 |
60 60 45 1202 |
39 37 34 412 |
| Borgen et al [128] 2004 | 4.5 g | 13 | 90 1043 |
52 433 |
43 463 |
| Brenneisen et al [132] 2004 | 25 mg/kg | 8 | 40 | 41 | 30 |
| Ferrara et al [35] 1992 | 25 mg/kg | 10 | 54 554 |
30 304 |
27 264 |
| Ferrara et al [126] 1996 | 25 mg/kg | 85 86 |
68 47 |
45 45 |
32 56 |
| Palatini et al [142] 1993 | 12.5 mg/kg 25 mg/kg 50 mg/kg |
8 | 23 46 80 |
25 30 45 |
20 22 23 |
| Thai et al [131] 2006 | 50 mg/kg | 16 | 73 847 |
57 547 |
52 677 |
| Scharf et al [127] 1998 | 3.0 g | 6 | 63 | 40 | 53 |
| Brailsford et al [118] 2012 | 25 mg/kg | 12 | 59 | 23 | 32 |
1Number of subjects. 2After a high fat meal. 3After nightly treatment with GHB for 8 weeks in patients suffering from narcolepsy. 4After 13 daily doses of GHB to alcohol dependent patients. 5Cirrhotic patients without ascites. 6Cirrhotic patients with ascites. 7Together with 0.6 g/kg ethanol.
In most pharmacokinetic studies the concentrations of GHB are determined in plasma or serum and not in whole blood. The GHB concentrations in serum are expected to be higher than in blood in a similar way as ethanol distribution [120]. Both drugs are completely miscible with water, there is no binding to plasma proteins so the water content of plasma and erythrocytes is a deciding factor for serum/blood distribution ratios [121].
The pharmacokinetics of GABA appears to be dose-dependent and the metabolizing enzymes become saturated with substrate after massive (abuse) doses are taken and high concentrations are reached in plasma. After smaller recreational doses when Cmax in plasma is below 100 mg/L, first-order kinetics is an appropriate model to describe the post-absorptive phase of the C-T profile [122]. After large doses of GHB or its precursors when the hepatic enzymes are saturated the initial descending phase of the C-T profile is best described by zero-order kinetics [123].
The dose-dependent non-linear kinetics of GHB suggests that C-T profiles might be best described by the Michaelis-Menten equation [124]. This model would yield values of km and Vmax that are characteristic of substrate and the plasma concentration reached. When the concentration of GHB is more than double km the metabolizing enzymes are approaching saturation and zero-order kinetics applies. For drugs eliminated by non-linear kinetics the C-T profile spanning from high to low concentration looks more like a hockey stick rather than a straight line (zero-order slope) or a pure exponential decay function (first-order kinetics).
Examples of concentration-time profiles of GHB for health men (N = 18) and women (N = 18) after an oral dose of 4.5 g as sodium oxybate are shown in Fig. 2 [125]. The drug was rapidly absorbed in both sexes and for the first 1-2 h after passing the peak it appears that that rate of elimination occurs at a constant rate per unit time. As the concentrations of GHB in plasma decreases, there is a change in shape of the C-T profile towards an exponential function and first-order kinetic processes and t½ best describe the elimination from the body.
Fig. (2).

Plasma concentration-time profiles of GHB after a single oral dose of 4.5 g sodium oxybate in healthy adult males (n = 18) and females (N = 18). The graph was redrawn from reference [125].
The overall shape of C-T profiles of GHB for men and women are therefore very similar with a median time to peak of 1 h and Cmax of 88 mg/L (men) and 83 mg/L (women) [125]. The elimination half-life of GHB did not depend on gender, being 0.65 ± 0.23 h (men) and 0.61 ± 0.12 h (women). The area under the curve (AUC) was slightly greater in men (241 mg x h/L) than in women (233 mg x h/L).
Other studies have reported pharmacokinetic profiles of GHB in sober alcoholics [35], in patients with liver dysfunction [126] and in people suffering from narcolepsy [127] and the findings are not much different from healthy controls, rapid absorption, early occurring tmax and short plasma elimination half-life.
In a chronic dosing study, the pharmacokinetic profile of GHB (sodium oxybate) was studied in patients suffering from narcolepsy before and after 8 consecutive weeks of drug treatment (4.5 g before bedtime). The mean peak GHB concentration was higher after 8 weeks of treatment (p<0.05) with a Cmax of 104 ± 31 mg/L compared with 90 ± 31 mg/L for the first dose [128]. However this study gave no evidence of drug accumulation in plasma after multiple daily doses and both tmax and t½ were about the same after the first and last dose of GHB.
Similar conclusions were reached regarding lack of accumulation when GHB when alcohol-dependent patients received 25 mg/kg GHB daily every 12 h for 7 consecutive days [35]. The results of these chronic dosing studies also speak against the notion of induction of GHB metabolizing enzymes, principally cytosolic GHB dehydrogenase.
ABSORPTION
A low molecular weight, the high solubility in water and the lack of binding to plasma proteins means that GHB is rapidly absorbed from the gut and peak concentration in plasma are reached by 20-40 min post-ingestion. However, oral bioavailability of GHB is fairly low corresponding to 25-40% according to some authorities with a major influence of taking the drug on an empty stomach or after eating a meal.
One of the first controlled dosing studies of GHB pharmacokinetics originated from Italy because sodium oxybate was being used in that country in clinical medicine for alcohol withdrawal. Eight healthy male volunteers participated in a randomized cross-over design experiment and received increasing oral doses of 12.5, 25 and 50 mg/kg [124]. The tmax of GHB increased with increasing dosage (25, 30 and 45 min, respectively) with a range from 20 to 60 min. Likewise, Cmax also increased in relation to dose 23 mg/L (12.5 mg/kg), 46 mg/L (25 mg/kg) and 92 mg/L (50 mg/kg). The plasma elimination t½ was 20 min, 22 min or 23 min and thus independent of dose despite a four-fold variation (12.5 to 50 mg/kg), which fits with the assumption of first-order elimination kinetics.
This Italian study concluded that both oral absorption and elimination kinetics of GHB were capacity limited and that AUC increased disproportionally with dose. The existence of non-linear kinetic meant that doubling the dose from 4.5 to 9.0 g increased the AUC 3.8 fold and Cmax 2.4-2.9 fold.
A more recent study of GHB pharmacokinetics involved 12 healthy volunteers (6 males and 6 females) and a dose of 25 mg/kg given as sodium oxybate. The study was particularly impressive because of a good experimental design, use of a highly reliable method of analysis and taking an adequate number of blood samples so that C-T profiles could be plotted unequivocally. The absorption of GHB was rapid with Cmax occurring after 24.6 min at a concentration of 59.4 ± 10.2 mg/L [118].
As with many other drugs, the concomitant intake of food delays the rate of absorption after oral intake and in the case of GHB this effect was rather dramatic as shown in Fig. 3. After a dose of 4.5 g sodium oxybate the Cmax was 60.1 mg/L (n = 34) after subjects had eaten a fat-rich meal compared with 142 mg/L (N = 34) when the drug was taken on an empty stomach. The median tmax was increased from 45 min to 120 min in the fed state, whereas t½ was not much influence by the postprandial state [125].
Fig. (3).

Plasma concentration-time profiles of GHB in healthy adult females (N = 34) following a single oral dose of 4.5 g sodium oxybate after a fat-rich meal or after an overnight fast. The graph was redrawn from reference [125].
DISTRIBUTION
The distribution of GHB in the body fluids and tissues depends on the distribution of total body water because there is negligible binding of the drug to plasma proteins. According to several studies, the volume of distribution (Vd) of GHB in healthy subjects ranges from 0.19 to 0.33 L/kg, although higher values have also been found. In patients suffering from narcolepsy or liver failure the Vd was not much different (0.23-0.32 L/kg) from healthy controls.
The speed and extent of distribution of GHB from the bloodstream to tissue compartments depends on water content and ratio of blood flow to tissue mass. Since GHB distributes into total body water, this suggests that Vd should be lower in females compared with males, although this has not been verified by experiment. Furthermore, Vd for GHB should be lower in the elderly and in obesity, owing to less water per kg body weight in these individuals.
SERUM/BLOOD CONCENTRATION RATIO
During pharmacokinetics of GHB the C-T profiles were plotted from results of analyzing near simultaneous samples of serum and blood [118]. The 12 volunteers (6 men and 6 women) ingested a dose of 25 mg/kg GHB as sodium oxybate and a reliable GC-MS method with d6-GHB as internal standard was used for analysis.
The concentrations of GHB in serum were always higher than in whole blood, as expected from differences in water content of the specimens as shown by the plots in Fig. 4 [118].
Fig. (4).

Serum and whole-blood concentration-time profiles of GHB after a single oral dose of 25 mg/kg as sodium oxybate in 12 healthy volunteer (6 men and 6 women). The dashed horizontal line at a GHB concentration of 5 mg/L represents the analytical reporting limit. The graph was redrawn from reference [118]
The mean Cmax (± SD) for GHB in serum was 59.4 ± 10.2 mg/L (N = 12) compared with Cmax of 48.8 ± 8.8 mg/L in whole blood (N = 12). Thus the mean serum/blood ratio of GHB is 1.23:1 under these conditions and stands in good agreement with the water content of serum (~92-94%) and blood (~78-80%). There were no gender differences in the distribution of GHB between serum and blood.
After two male volunteers ingestion of a single dose of GBL (1.5 mL), the concentrations of GHB were determined in serum and blood by a liquid chromatography tandem mass spectrometric (LC-MS/MS) method. The Cmax in serum (blood) were 95 mg/L (58 mg/L) for the first subject and 106 mg/L (83 mg/L) for the second person, giving serum-to-blood distribution ratios of 1.63 and 1.28:1, respectively. With an analytical detection limit of 1 mg/L, the detection window of GHB in serum was 4-5 h compared with 8-10 h for the analysis of urine.
Animal studies have been performed to test the distribution of GHB between plasma and erythrocytes in whole blood and the mean plasma/blood concentration ratio was 1.33 (N = 74), being in good agreement with the human studies [129].
METABOLISM
The bulk of the dose of GHB administered (95-98%) undergoes hepatic metabolism by a series of enzymatic pathways (Fig. 1). A major route of metabolism is oxidation by GHB dehydrogenase to give succinic semialdehyde, by which further oxidation is converted into succinic acid, entering the intermediary metabolism and via the Krebs cycle transformed into end-products carbon dioxide and water.
The biosynthesis and metabolism of GHB is also closely linked to GABA metabolism and GHB can be considered both a metabolite and a precursor of GABA. The amino acid glutamate passes the blood-brain barrier and is decarboxylated to produce GABA. Metabolism of GABA is accomplished by an aminotransferase enzyme to give succinic semialdehyde, which can either become oxidized to give succinic acid or alternatively reduced to form GHB.
Whatever the exact metabolic pathways involved, most published studies verify that the terminal plasma elimination half-life for GHB in humans ranges from 30-50 min. There is no evidence that the metabolic enzymes that clear GHB from the blood are boosted after chronic exposure to substrate.
EXCRETION
Only a small fraction of ingested GHB (~2-5%) is excreted unchanged in the urine according to several human dosing and recovery studies.
Urine voids were collected from 12 volunteers (6 men and 6 women) for up to 12 hours after they had received a GHB dose of 25 mg/kg dosing [118]. In 11 of 12 subjects, the tmax in urine was reached after 1 h and the urinary Cmax ranged from 32.6 to 161.3 mg/L (mean 67.3 mg/L). Urinary concentrations decreased fairly and rapidly thereafter in all subjects and were below 10 mg/L, a commonly used cut-off concentration, 4 hours post-dosing. The results confirmed that 0.6-2.5% (mean 1.3%) of the administered dose (25 mg/kg) was excreted in urine [118].
Abanadas et al [130] recovered <2% of the dose of GHB (50 mg/kg), whereas Thai et al [131] found between 4-5 % of the dose of 50 mg/kg GHB in urine. In one of these studies GHB was administered together with ethanol (0.6 g/kg), although the excretion characteristics of GHB were unchanged. Seemingly any diuresis caused by consumption of ethanol was unimportant for the urinary excretion pattern of GHB. Other studies gave quantitative results for GHB excretion in urine as 0.2-2.1% of a dose of 25 mg/kg and a mean of 1.2% [132]. Another study showed that the window of detection of GHB from analysis of urine was < 10 h and that 0.6-1.16% of the dose was recoverable [133].
All the above results confirm that ~2-5% of the dose was recoverable in urine samples as GHB and that the window of detection was fairly short. This reinforces the need to be prompt and expeditious when sampling blood and urine in forensic cases to maximize the change of verifying exogenous intake of GHB [58]. If more than 10-12 hours have elapsed after the alleged attack there is little hope of detecting and measurable amounts of GHB as evidence in DFSA and other criminal cases.
GHB-ETHANOL INTERACTIONS
Because GHB is often abused or taken by people consuming ethanol, this raises the possibility of an adverse interaction between these two sedative drugs. This question was studied in a double-blind placebo controlled cross-over design involving 16 health volunteers [131]. They drank ethanol 0.6 g/kg with or without GHB (50 mg/kg). The resulting mean C-T profiles of GHB in the two arms of the study are shown in Fig. 5.
Fig. (5).

Serum and whole-blood concentration-time profiles of GHB after a single oral dose of 25 mg/kg as sodium oxybate in 12 healthy volunteer (6 men and 6 women). The dashed horizontal line at a GHB concentration of 5 mg/L represents the analytical reporting limit. The graph was redrawn from reference [118].
In one study, the co-ingestion of ethanol resulted in a 16% higher plasma Cmax for GHB (84 vs 73 mg/L), whereas tmax remained about the same (54 vs 57 min). The plasma elimination half-life was 29% longer (67 vs 52 min) after the co-ingested ethanol although these differences in pharmacokinetic parameters were not statistically significant (p>0.05). Neither were the C-T profiles of ethanol influenced by the presence of GHB in blood (Fig. 6).
Fig. (6).

Plasma concentration-time profiles of GHB alone (50 mg/kgas Xyrem) compared with the same dose taken 15 min after the subjects drank a moderate dose of ethanol (0.6 g/kg). Mean curves for N = 16 subjects are plotted. The graph was redrawn from reference [131].
In the GHB + ethanol arm of the study subjects reported experiencing more adverse effects and two subjects suffered from hypotension and six had episodes of vomiting [131]. In the same study, the window of detection of GHB in urine was investigated using the widely used cut-off concentration of 10 mg/L. The results showed that 12.5% of samples collected from 3-6 h, 81.3% of samples voided from 6-12 h and 100% of samples from 12-24 h would have been reported as negative for GHB at a threshold of 10 mg/L.
The interaction between ethanol and GHB has also been studied in various animal models, such as rats and baboons [134]. The combined influences of ethanol and GHB prolonged sleep time without having any influence on the pharmacokinetics of either GHB or ethanol.
METABOLIC CONVERSION OF BD TO GHB
Both GBL and BD are rapidly converted in the body into GHB and because these pro-drugs are not classified as controlled substances, they represent a more easily available and legal source of GHB [117, 135, 136].
An example of the rapid and extensive conversion of BD into GHB is seen in the graphs drawn in Fig. 7 showing mean C-T profiles in 8 healthy volunteer after a dose of 25 mg/kg 1.4-butanediol was taken mixed with orange or cranberry juice [135]. The maximum plasma concentration of GHB was 45.6 ± 19.7 mg/L and occurred at 39.4 ± 11.2 min after ingestion of BD. The average t½ of GHB derived from BD was 32.3 ± 6.6 min in good agreement with results when 25 mg/kg GHB was administered.
Fig. (7).

Plasma concentration-time profiles of GHB in 8 volunteers after they ingested 1,4-butanediol (25 mg/kg) in orange juice. The graph was redrawn from reference [135].
ENDOGENOUS CONCENTRATIONS OF GHB
Trace amounts of GHB are present in body fluids and tissues from healthy individuals never exposed to GHB. Hence GHB is a normal endogenous product of metabolism, presumably formed via GABA or the even endogenous presence of GBL or BD. Using reliable analytical methods, most investigators report endogenous urinary GHB concentration in the range 0.5-2 mg/L with some outliers as high as 5 mg/L [137, 138].
The range of endogenous GHB concentrations in N = 670 urines donated by people never exposed to GHB were 0.34 mg/L to 5.7 mg/L (median 3.0 mg/L). Similarly, in N = 240 blood samples the endogenous GHB concentration ranged from 0.17 mg/L to 1.51 mg/L (median 0.8 mg/L) [138]. These results were used to support threshold concentrations for reporting of 5 mg/L for blood and 10 mg/L for urine. However, concentrations of GHB in urine tend to increase after voiding and during storage of specimens at elevated temperatures, which also needs consideration [43, 139].
A toxicologist has to distinguish endogenous GHB from exogenous intake and therefore practical cut-off limits must be established [44]. The unequivocal identification of GHB in biological specimens from living and deceased persons is not a problem, the trick is to be able to state with certainty that the person ingested an illicit drug [84, 140]. There represents a difficult balance the dangers of reporting a false-positive or false-negative result of GHB analysis in forensic casework. The benefit of the doubt in criminal cases should be given to the suspect, which speaks towards use of conservative cut-off concentrations.
The endogenous concentrations of GHB are higher in urine than in blood when the samples are obtained from living subjects, although the opposite holds for autopsy specimens. This requires different urinary and blood cut-off concentrations depending on whether analytical results refer to living or deceased persons [141-143]. Other factors of importance for the stability of GHB include urinary tract infections, duration and temperature of storage and whether any sodium fluoride was as present as an enzyme inhibitor and preservative [45].
Urines samples were voided by 1126 healthy female subjects and endogenous GHB concentrations were determined by a GC-MS method. The mean concentration of GHB was 0.84 mg/L (median 0.68 mg/L) with an overall range from 0-5.5 mg/L [144]. These concentrations did not seem to depend on urinary pH, the person’s body mass index (BMI) nor the donor’s racial origin. A weak correlation (R2 = 0.3) was established between urinary specific gravity and GHB concentration, although making corrections for urine dilution is probably not necessary.
Because of the large sample size this study provides useful information and supports use of a cut-off between 5 mg/L and 10 mg/L to distinguish endogenous levels from exogenous intake of GHB in living subjects. The corresponding cut-off concentration for GHB analyzed in venous blood samples is lower and many laboratories endorse a level of 3-5 mg/L, because fresh blood show very low GHB levels (<0.5 mg/L). In another study of 50 urine samples from normal healthy women, the highest concentration of endogenous GHB was 1.46 mg/L and the authors considered 5 mg/L as a suitable cut-off concentration for use in forensic casework [137].
Analysis of alcoholic and nonalcoholic beverages found they contained small amounts of GHB, although these lack forensic significance because of massive dilution that occurs with total body water after drinking usually amounts [145]. The endogenous concentrations of GHB in urine did not depend on the person’s gender, smoking or alcohol drinking habits and concentrations in most people were < 10 mg/L /L [146]. Urinary GHB concentrations in people suffering from diabetes (N = 20) ranged from 0.17-3.03 mg/L compared with 0.16-2.14 mg/L in healthy control individuals (N = 30). In pregnancy mean GHB, GBL and BD in urine were 0.36, 0.34 and 1.92 mg/L compared with 0.24, 0.08 and 0.40 mg/L in non-pregnant women [147]. The general consensus is that a practical and robust urinary cut-off concentration for GHB is 5-10 mg/L for clinical and forensic purposes when samples are from living individuals [142].
GHB concentrations were determined in N = 100 forensic urine preserved with sodium fluoride (1%) when no evidence suggested intake of exogenous GHB. After storage at room temperature for 1 year, the mean and median concentrations of GHB were 1.8 mg/L and 1.6 mg/L, respectively, although some individual reached 7 mg/L. More than 95% of urine samples stored at room temperature for 12 months contained less than 5 mg/L GHB and 100% were less than 10 mg/L. These results also supports the use of an administrative cutoff concentration of 10 mg/L for routine analysis of GHB in ante-mortem urine samples [148].
Urine samples from N = 207 people who claimed no prior intake of GHB were analyzed in duplicate by a GC-MS method [140]. The urinary GHB concentrations ranged from 0 to 2.70 mg/L with a median concentration of 0.24 mg/L. The average GHB concentration in male donors (n = 130) was 0.27 mg/L (range 0-2.70 mg/L), compared with 0.29 mg/L (range 0-0.98 mg/L) from females (n = 77); no significant gender difference.
In 55 healthy people aged from 6-59 y, the median concentration of GHB in urine was 1.3 mg/L (mean 1.65 mg/L and range 0.9-3.5 mg/L), further supporting use of a 10 mg/L cut-off concentration in forensic toxicology casework [141].
Oral fluid (saliva) also contains measurable amounts of endogenous GHB at roughly the same concentrations as in urine. In 120 individuals, the mean, median and range of GHB concentrations in mixed saliva were 1.29 mg/L, 1,13 mg/L and 0.15-3.33 mg/L [75].
DRIVING UNDER THE INFLUENCE OF GHB
GHB is a common recreational drug of abuse in many countries and accordingly is often encountered when blood and urine samples are analyzed from people arrested by the police for DUID. In this connection, it is important to consider that between 30-120 min usually elapses after the time of arrest until time of drawing blood for toxicological analysis. During this time appreciable amounts of GHB are removed from the body by metabolism in the liver so the concentration reported are probably a lot less than existed at the time of driving.
The very short elimination half-life of GHB and rapid metabolism might be used to argue that it is more correct for legal purposes to make a back-estimation of GHB concentration as is sometimes done for blood-ethanol. However, to the best of our knowledge back calculation of GHB concentrations in blood to the time of driving has never been done in criminal cases.
Table 6 compares the concentrations of GHB in blood of apprehended drivers in Sweden and results are shown when GHB was the only psychoactive substance detected and when other drugs were present in blood samples. Poly-drug use is common among apprehended drivers in most nations and can have considerable influence on drug-induced impairment and risk of involvement in a traffic crash. The median concentration of GHB of DUID suspects in Sweden (81 and 83 mg/L) were similar to drivers arrested in Washington State [149] and in Norway [63]. Abuse of GHB by drivers in Germany was less prevalent, although the laboratory strategy usually dictates that GHB is analyzed when all other drugs are negative [150].
Table 6.
Age, gender and concentrations of GHB in blood in three forensic toxicology materials including, impaired drivers, people arrested for abuse of drugs (non-traffic cases) and GHB related deaths [19, 20, 64].
| Forensic Blood Samples from | N | Gender, N (%) Men Women |
Age, y (Mean ± SD) Men Women |
GHB Conc. mg/L Mean (Median) Highest |
||
|---|---|---|---|---|---|---|
| Impaired drivers, GHB only drug | 215 | 209 (97) | 6 (3) | 25 ± 4.9 | 33 ± 6.2 | 91 (83) 270 |
| Impaired drivers, GHB + other drugs | 333 | 314 (94) | 19 (6) | 26 ± 5.1 | 32 ± 7.2 | 88 (81) 340 |
| Users of illicit drugs (non-traffic) | 1061 | 935 (88) | 122 (12) | 25 ± 5.4 | 23 ± 6.5 | 118 (110) 840 |
| Post-mortem, GHB-related deaths | 37 | 30 (81) | 7 (19) | 27 ± 7.4 | 21 ± 5.0 | 249 (190) 2200 |
The average age of motorists arrested in Sweden with GHB in blood was 23-25 y and there was a clear predominance of males (Table 6). The proportion of female users of GHB was higher among those arrested for petty drug offences and also in fatalities after overdosing with GHB.
POST-MORTEM CONCENTRATIONS OF GHB
The endogenous concentrations of GHB are higher in blood and urine samples collected during autopsies compared with specimens from living people. According to a Japanese study, one of the mechanisms accounting for biosynthesis of GHB after death is the foul smelling substance putrecine (tetramethylenediamine) derived from decaying animal tissues. This diamine molecule is the product of protein breakdown after death and gets converted into 4-amino-butylaldehyde [151]. Further oxidation yields GABA and via succinic semialdehyde GHB can be generated. The concentrations of GHB in blood from charred bodies were lower than in non-burnt corpses and the authors suggested that heat degeneration of enzyme protein might have prevented the synthesis of GHB in the early post-mortem period [151].
Because of the wide variation in endogenous GHB concentrations in post-mortem blood and urine higher cut-off concentrations are needed to differentiate ante-mortem ingestion from post-mortem production of GHB. The proposed thresholds from different investigations and from different countries are 20 mg/L in urine and 30-50 mg/L in blood samples [46, 47].
An early report by Elliot [152] determined GHB in 13 cadavers and mean concentration in blood was 57 mg/L (range 0-197 mg/L) and mean in urine was 56 mg/L (range 0-217 mg/L). These results were challenged as being unusually high and because information about cause or manner of death and condition of the bodies was lacking, and post-mortem interval and use of fluoride preservative was not mentioned [153]. This prompted a follow-up study by Elliot [47] and he now reported a mean endogenous GHB concentration 12.3 mg/L (range 2-29 mg/L, N = 38) in non-preserved blood compared with 12.6 mg/L (range 4-25 mg/L, N = 17) with fluoride.
Concentrations of GHB in post-mortem urine samples were lower than in blood averaging 5.5 mg/L (range 0-18 mg/L, N = 39) without fluoride and 4.8 mg/L (range 0-10 mg/L, N = 15) with fluoride. Others have verified that urine is less susceptible to post-mortem synthesis of GHB and this is the reason for lower threshold concentrations in this bio-fluid. Most investigators also recommend addition 1-2% fluoride to improve stability of GHB during transport and storage [154].
The axiom in post-mortem toxicology “an analytical results should not be interpreted in isolation” certainly rings true when it comes to interpreting GHB concentrations. The entire case scenario should be considered, including demographics of the deceased, circumstances surrounding the death, findings at the scene, police reports, the person’s medical records and whether any life-saving treatment was given. Furthermore, much can be gained by analysis of GHB in specimens collected from different anatomical sites (blood, urine, CSF or vitreous humor). Finding concentrations above the reporting thresholds in several or all specimens analyzed speaks strongly towards ante-mortem ingestion of an illicit drug [78].
The blood samples submitted for analysis in post-mortem toxicology should if possible be taken from a peripheral (femoral) vein after clamping proximally to avoid drawing in blood from the central compartment. The GHB cut-off concentration for reporting positive results in death investigations are 30 mg/L for femoral blood and 50 mg/L for heart blood [78].
Table 7 summarizes the results of a recent study of GHB concentration in blood and urine in relation to post-mortem interval and temperature of storage. GHB was analyzed by a LC-MS method before and after storage of specimens at 4oC for 4 months without any fluoride preservative added. The endogenous concentrations of GHB increased with post-mortem interval and also with time of storage, but were still less than the established and recommended cut-off concentrations of 20 mg/L for urine and 30 mg/L for blood off [155].
Table 7.
Effect of post-mortem interval on endogenous concentrations of GHB in femoral blood and urine before and after storage of specimens at 4 °C for four weeks.
| Post-Mortem Interval, h | N | Blood GHB, mg/L (Mean ± SD) Autopsy 4 Weeks at 4°C |
Urinary GHB, mg/L (Mean ± SD) 4 Weeks at 4°C |
||
|---|---|---|---|---|---|
| 24-36 | 10 | 2.1 ± 1.1 | 2.3 ± 1.1 | 3.9 ± 1.7 | 4.2 ± 1.9 |
| 37-72 | 10 | 5.1 ± 2.8 | 5.6 ± 2.8 | 3.9 ± 2.6 | 4.2 ± 2.6 |
| 73-192 | 10 | 11.8 ± 5.5 | 13.0 ± 5.6 | 9.8 ± 5.1 | 11.1 ± 5.2 |
The concentrations of GHB were determined in various body specimens taken from a verified overdose death [77]. A targeted analysis revealed GHB in urine, brain, vitreous fluid, femoral blood, heart blood, and liver at concentrations of 1665 mg/L, 102 mg/kg, 48 mg/L, 461 mg/L, 276 mg/L, and 52 mg/kg, respectively. The confirmation of GHB in urine and vitreous fluid is important in death investigations, because the risk of post-mortem synthesis is lower than for blood. In another single GHB fatality the concentrations of GHB were 330 mg/L in femoral blood and 221 in brain tissue from the frontal cortex [156].
Different site-dependent production of GHB was verified in a study of 25 corpses and short post-mortem interval of only 2 days [78]. The mean concentrations of endogenous GHB in femoral blood, cerebrospinal fluid (CSF), vitreous humor, bile, and urine were 4.6 ± 3.4 mg/L, 1.8 ± 1.5 mg/L, 0.9 ± 1.7 mg/L and 1.0 ± 1.1 mg/L, respectively. These findings led to the suggestion of using cut-off concentrations to discriminate between exogenous and endogenous GHB of 30 mg/L for blood and 10 mg/L for urine in death investigations and in bodies without any decomposition [78]. Kintz et al [44] recommended a 50 mg/L GHB cut-off concentration if the drug is analyzed in heart blood in order to discriminate between endogenous production and ante-mortem ingestion.
Table 8 presents the analytical toxicology results from investigations of GHB intoxication deaths in Sweden and shows the age and gender of the victims and other relevant drug-use information. The toxicity of GHB is enhanced if taken together with other CNS depressants and relatively high concentrations of ethanol were reported in several of these cases.
Table 8.
Analytical toxicology findings in GHB-related intoxication deaths shown in decreasing order of the concentrations in femoral blood. More information about these GHB-related deaths is available as electronic supplementary material in reference [20] .
| Case | Age, y (Gender) M/F |
GHB in Blood, mg/L |
GHB in Urine mg/L |
Other Relevant Toxicology Findings |
|---|---|---|---|---|
| 1 | 24 (F) | 390 | 1700 | Ethanol negative in blood, flunitrazepam + metabolite, tramadol, and amphetamine positive. |
| 2 | 20 (M) | 260 | 4600 | Ethanol negative in blood, flunitrazepam + metabolite positive. |
| 3 | 32 (M) | 210 | 1700 | Ethanol negative in blood, morphine (heroin), codeine amphetamine benzoylecgonine, THC and citalopram positive. |
| 4 | 21 (M) | 190 | 2300 | Ethanol negative in blood, diazepam, nordiazepam and propiomazine + metabolite positive. |
| 5 | 15 (M) | 180 | 3000 | Blood ethanol 1.0 g/L, urine ethanol 1.3 g/L. |
| 6 | 31 (M) | 170 | 300 | Blood ethanol 1.7 g/L, urine ethanol 2.5 g/L, nordiazepam positive in blood |
| 7 | 30 (F) | 140 | 620 | Blood ethanol 1.6 g/L, urine ethanol 2.0 g/L, fenfluramine + metabolite positive in blood |
An appreciable overlap exists between GHB concentrations in femoral blood in intoxication deaths and other causes of death and also between living cases (DUID suspects) and autopsy cases [5, 6]. This means that blood concentration alone is not sufficient to state that a person died of GHB intoxication [20]. The average concentration of GHB in autopsy blood in 10 deaths in Australia was 231 mg/L and the range was 77-370 mg/L [4], which compares well with a mean and median concentration of 190 mg/L and 294 mg/L in 37 deaths reported from Sweden [20].
By far the largest case series of GHB-associated deaths was compiled by Zvosec et al [21] and details were presented of 226 fatalities. Most victims (N = 213) died from cardiopulmonary arrest before arrival at hospital for life-saving treatment and 13 deaths were the results of some type of accident. Without any co-ingested drugs the median GHB concentration in post-mortem blood was 347 mg/L and the range was from 18-4400 mg/L, although the source of blood whether central or peripheral was not stated. The same authors identified three deaths associated with use and/or abuse of Xyrem® [14].
ACUTE GHB INTOXICATION
Clinical Presentation
The clinical presentation of GHB intoxication depends on the dose, the route of administration and individual tolerance to depressant drugs. Treatment of poisoned patients represents a medical challenge because the signs and symptoms are nonspecific and might be confused with gross ethanol intoxication or intake of other sedative-hypnotic drugs such as barbiturates or benzodiazepines.
The typical signs and symptoms associated with acute GHB intoxication are presented in Table 9 as was observed and documented in people admitted to hospital for treatment of GHB intoxication and recorded by the police in connection with arresting impaired drivers or users of illicit drugs.
Table 9.
Neurological symptoms related to acute GHB intoxication and overdose.
| Occurrence | Symptoms of GHB Intoxication after Oral Ingestion of Intoxicating Doses |
|---|---|
| Very often | Relaxation, disinhibition, feelings of inebriation, ataxia, disorientation, dizziness, euphoria, confusion, hallucinations, somnolence, slurred speech, nausea, miosis, hypothermia. |
| Often | Dysarthria, confusion, headache, incoordination, euphoria, amnesia, hypotonia, hyporeflexia, tremor, myoclonus, horizontal and vertical gaze nystagmus. |
| Seldom | Bruxism, vertigo, increased sexual arousal, delusions, extrapyramidal side effects, dystonias, athetoid posturing, mydriasis |
The clinical course of GHB intoxication was studied in 88 patients (61 males and 27 female, mean age 28 years) admitted for treatment [157]. As many as 67% of patients (N = 59) had co-ingested other drugs, mainly alcohol (39% of cases), and second lace was amphetamines (28%). The Glasgow Coma Scale (GCS) in 53 subjects was lower than 9 (25 patients had GCS score = 3; 28 had a score from 4 to 8). Most patients regained consciousness spontaneously within 5 hours after they were admitted to hospital.
The commonest clinical manifestations of GHB intoxication in emergency service patients with GCS less or equal to eight were bradycardia and hypotension. Other things noted were hypothermia and acute respiratory acidosis with tachycardia and hypertension between 15 and 30 min post-ingestion.
In an investigation of drug emergencies in Spain, 104 GHB overdose cases were documented (3.1% of all toxicological emergencies). The typical patient profile was a person aged 23 ± 5.1 y mainly male (64%) and presenting on weekends (90%). Poly-drug use is common including ethanol (73%) or illicit drugs (86%) or both and 16% of those admitted were unconscious with a GCS of 3 [158]. Complete recovery occurred without sequelae in all patients. Clearly there is a need to consider types of co-ingested drugs when GHB overdose patients are treated, because this might influence the clinical presentation and severity of intoxication.
The mean age of patients admitted to a hospital in Washington State for overdosing with GHB was 28 y (range 17-59 y) and the vast majority (83%) were male [159]. The mean (median) and range of GHB concentrations in blood were 137 mg/L (193 mg/L) and 29-490 mg/L, respectively. Other drugs besides GHB were identified in 67% of patients particularly ethanol in 41% of patients. Typical signs and symptoms of GHB overdose were vomiting, ataxia, no gag reflex, respiratory depression, coma and sudden altered states of consciousness. Many patients required intubation and on regaining consciousness they became combative and needed to be restrained. The vast majority were sufficiently alert to be discharged 6 h after hospital admission.
The first symptoms of GHB intoxication occur within 15-50 minutes after intake and users feel less inhibited and experience a mild euphoria. The gastrointestinal disturbances include vomiting in 20-55% of cases, abdominal pain and excessive production of saliva (sialorrhea). Rapid recovery is the rule when it comes to acute GHB intoxication and this fits with the short plasma elimination half-life of this sedative drug, although hospital treatment may be necessary [160].
Seventy-six past users of GHB in Australia were given a structured interview to investigate their experiences about harmfulness of the drug [161]. A large majority reported experiencing adverse effects (99%) at least once with 52% becoming unconscious, 53% vomiting, 58% reporting profound sweating, and 8% said they had a fit or seizure. Clearly GHB use and abuse represents a medical risk for many recreational drug users.
Accidental exposure to GHB was documented in toddlers in the UK, Australia and USA from an unexpected innocent source, namely a child’s toy. The children showed signs and symptoms of intoxication including depressed consciousness, some became non-responsive and comatose, but all showed rapid recovery with no long-term neurological consequences. Investigations showed that the source of GHB was brightly colored beads, which were coated with a glue-based product made from BD. The toys were manufactured in China and it appears BD had mistakenly been used as solvent for the plastic instead of 1,5-pentanediol [162, 163].
TREATMENT OF GHB INTOXICATION
The strategy used to treat people admitted to hospital emergency departments intoxicated with GHB/GBL/BD is essentially supportive and requires monitoring vital signs and ensuring the airways are clear, because emesis is common. Physicians should pay particular attention to cardiovascular and respiratory symptoms and if the patients are unconscious then intubation should be considered for the first few hours of recovery. According to different studies the prevalence of intubation of GHB poisoned patients varies from 10 to 57%, whereas the mean duration of intubation ranges from 80 to 210 minutes [157, 164].
Cardiovascular symptoms resulting from overdosing with GHB don’t normally require invasive therapy although the bradycardia might be treated by administration of atropine. ECG anomalies are not typical of GHB intoxication and if they do occur are probably caused by co-ingestion of other drugs [19].
Table 10 gives examples of the types of drugs used in attempts to reverse the intoxication and sedative effects of GHB in emergency department patients and also in various animal studies. In one study, physostigmine showed some promise in reversing GHB-induced altered states of consciousness [165, 166], although its efficacy was later challenged [167]. Neither naloxone, a pure opiate antagonist [168], nor the selective benzodiazepine receptor antagonist flumazenil [169] were effective in reversing GHB sedation. A novel GABA-B antagonist was tested in mice as a way of lowering mortality caused by massive doses of GHB, but it did not seem to have any beneficial effects [170]. Taken together, these investigations and the types of drugs used have so far not provided a practically useful antidote to treat patients heavily intoxicated with GHB.
Table 10.
Examples of drugs used in the treatment and reversal of acute GHB intoxication.
| Drug (Trade Name in USA) | Class of Medication | Limitations/Comments |
|---|---|---|
| Phenytoin (Dilantin®) Phenobarbital (Luminal®) |
Anticonvulsant/antiepileptic. | No apparent effect on coma induced by GHB. |
| Clonazepam (Klonopin®) Diazepam (Valium®) Lorazepam (Ativan®) |
GABA-A receptor agonists. | Effective to treat withdrawal effects of GHB. |
| Flumazenil (Anexate®) | GABA-A receptor antagonist. | No influence on CNS depression. |
| Naloxone (Narcan®) | Pure µ-opiate receptor antagonist. | No effect on GHB-induced respiratory depression. |
| Physostigmine (Antilirium®) | Cholinesterase inhibitor and thus a potential antidote to reverse effects of anticholinergic agents. | No major benefit and after GHB overdose and this treatment might precipitate seizures or cardiac arrhythmias. |
GHB WITHDRAWAL SYNDROME
Clinical Presentation
The acute pharmacological effects of GHB and GBL are of relatively short duration because of the rapid clearance of parent drug from the bloodstream and also the lack of any active metabolites. After regular use of increasing doses, the signs and symptoms of GHB withdrawal become apparent usually within 1-6 hours after taking the last dose. It should be pointed out that the clinical course of GHB withdrawal symptoms might be fairly long, lasting 14 days or more. After detoxification, some patients suffer from continuous anxiety and depression with cognitive deficits and persistent insomnia.
Table 11 classifies as mild, moderate and severe the most common GHB withdrawal symptoms. The most prevalent were anxiety, insomnia, tremor, tachycardia, affect liability, confusion, paranoia, agitation, delirium and hallucinations [171]. Less commonly observed was fever, fatigue, diaphoresis, arrhythmias and itching. Other clinical manifestations frequently described are confusion, disorientation, hyper-tension and paranoia. All these symptoms have an average duration between 3 and 21 days.
Table 11.
Typical symptoms of GHB withdrawal classified as mild, moderate and severe.
| Severity | Typically Observed Symptoms of GHB Withdrawal |
|---|---|
| Mild | Anxiety, agitation, sweating, restlessness, insomnia, mild hypertension. |
| Moderate | Tremor, tachycardia, nausea, vomiting, abdnominal cramps, diarrhea. |
| Severe | Tachycardia, hallucinations, delusions and pranoia, delirium, hypertension, rhabdomyolysis, seziures. |
The first symptoms of GHB withdrawal tend to appear within 24 hours after the last exposure when people start to become nervous and anxious and have difficulties in sleeping. Vomiting is common in the early withdrawal period. The withdrawal symptomatology changes over the following 5 days (from 24 hours to 6 days after last dose) with clinical manifestations of anxiety, delirium, confusion, insomnia and visual hallucinations being documented. Only episodic symptoms (anxiety, confusion, insomnia and visual hallucinations) occur from 7 to 15 days after the last dose.
Some symptoms of GHB withdrawal, such as delirium, is more often encountered after chronic drug use on average every 2-3 hours, with a range of 0.5-8 hours, compared with less intensive usage on average every 7 hours, with a range of 1-24 hours. The clinical presentation of GHB withdrawal shares common features with ethanol and/or benzodiazepines dependence.
WITHDRAWAL THERAPY
There is overwhelming evidence that long-term abuse of GHB and GBL leads to addiction and development of tolerance and physical dependence, which means that abrupt cessation of intake triggers the withdrawal syndrome [48, 172, 173]. This requires medical intervention and appropriate in-patient treatment at a hospital or a psychiatric facility, because the seizures that develop might be life-threatening, as they sometimes are during ethanol withdrawal [174].
The signs and symptoms of GHB withdrawal vary from patient to patient depending on extent and duration of prior drug exposure [175-178]. Based on numerous clinical reports and case studies in the medical literature some general guidelines are available. However, there is no official evidence-based treatment protocol for use during withdrawal from GHB and/or its analogues [171, 179, 180].
The best proven therapy seems to be administration of high-doses of certain benzodiazepines (e.g. diazepam, lorazepam) for 1-7 days depending on the severity of withdrawal symptoms [181-183]. When benzodiazepine administration alone is not effective, co-medication, including the use of anticonvulsants such as barbiturates, or the newer GABA-B receptor agonist baclofen or even an antipsychotic, such as olanzapin might be indicated [184].
Abrupt withdrawal from long-term abuse of GHB represents a medical emergency requiring an intervention from specialists in addiction medicine and psychiatric rehabilitation is motivated because very often the patient abuses several drugs, not only GHB [178]. Depending on the frequency of intake of GHB or the total daily dose consumed an algorithm was proposed for best possible treatment outcome [180]. For those taking three or more doses of GHB per day or more than 30 g of GHB in 24 hours, the administration of diazepam (80-150 mg) daily for up to 7 days is recommended. If delirium is present the dose of diazepam should be raised and if symptomatology persists for more than 24 hours, administration of pentobarbital might be considered [184].
The withdrawal protocol suggested by McDonough et al [180] depends on duration of GHB abuse and amounts of drug normally taken per day. In less severe cases (<3 doses per day) or <30 g of GHB in 24 hours, lower doses of diazepam (20-40 mg) should be administered for up to 7 days (Table 12).
Table 12.
Typical symptoms of GHB withdrawal classified as mild, moderate and severe.
CONCLUDING REMARKS
Reliable information about the popularity and extent of GHB use as a recreational drug in various countries around the world and its diffusion (including GHB precursors) in the general population is not easy to find in the literature. Nevertheless, the abuse of GHB continues to unfold as evidenced by hospital admissions for treatment of poisoned patients’ and forensic toxicology casework as well as scores of publications in the medical and toxicology literature. Use of GHB is dangerous when skilled tasks, such as driving, are performed and many traffic offenders have GHB in blood or are involved in road-traffic crashes [19].
Evidence that GHB or its analogues are used in cases of DFSA is difficult to obtain, owing to the time that elapses after the crime is committed before body fluids are taken for toxicological analysis. In recent surveys of DFSA cases in the Netherlands and Canada, forensic evidence for involvement of GHB was available in only 2% of cases [185, 186]. Another large review of drug-facilitated crimes implicated GHB in 0.2-4.4% of cases, being much lower than involvement of other incapacitating drugs, such as ethanol [57, 187]. This rapid clearance of GHB from blood after ingestion means that concentrations return to endogenous levels within 4-6 h after intake [49]. The analysis of GHB in hair strands offers an alternative specimen to verify a single exposure to GHB [102]. But care is needed to avoid external contamination of the hair and special washing procedures and cut-off concentrations are necessary to differentiate passive exposure from exogenous intake.
Treatment of acute GHB intoxication represents a medical challenge because symptoms are nonspecific and can be confused with intoxication caused by other CNS depressants, such as ethanol and/or benzodiazepines. The clinical features of GHB intoxication resemble over-consumption of alcohol excitement, agitation, sleepiness and unconsciousness depending on the dose. The oft reported cardiovascular disturbances include bradycardia and hypotension and respiratory failure and circulatory collapse occur after massive doses. The therapy is essentially supportive including monitoring of vital signs and ensuring no aspiration of stomach contents when in an unconscious or comatose state the person vomits.
Some emergency physicians advocate endotracheal intubation of comatose patients to protect against aspiration and gastric insufflations. Use of activated charcoal or gastric lavage is unlikely to help matters because GHB is absorbed very rapidly after oral administration reaching peak plasma concentrations in 20-40 min. Moreover, intoxicated patients mostly present for treatment late and at a time when the drug is fully absorbed and distributed in all body fluids. Moreover, gastrointestinal decontamination itself might induce vomiting, and heighten the risk for aspiration pneumonia.
The rapid clearance of GHB compared with other poisons, such as methanol and ethylene glycol, also means that invasive treatments, such as hemodialysis or hemofiltration, are hardly beneficial [188]. Treatment with the alcohol dehydrogenase inhibitor formepizole (4-methyl pyrazole) was suggested when people ingested 1.4-butanediol (BD) solvent as an alternative to GHB [189]. But whether this treatment actually influenced the clinical course of intoxication is doubtful considering the very rapid conversion of BD into GHB (see Fig. 7).
The clinical presentation of GHB intoxication and withdrawal shows common features with alcohol and/or benzodiazepine abuse, although the mechanism of active is different [175]. Making a differential diagnosis between GHB and ethanol intoxication often rests on the results of toxicological screening analysis. Although there is no official detoxification protocol for GHB withdrawal the most widely used treatment is to give high doses of benzodiazepines (lorazepam or diazepam) for the first few days after admission. Depending on response, this medication might be supplemented with barbiturates or antipsychotics.
GHB is an endogenous substance and low concentrations are present in blood and urine from healthy individuals never exposed to GHB or its congeners. These so-called “normal” GHB concentrations are usually less than 2 mg/L in urine and barely measurable in venous blood samples (<0.5 mg/L), although occasional higher concentrations in urine < 5 mg/L have been reported. Much depends on temperature and duration of storage of the specimens and whether a fluoride preservative was added. The in-vitro production of GHB is more of a problem when dealing with specimens taken from corpses as in post-mortem toxicology. This makes it imperative to use conservative cut-off limits before a person is accused of taking an illicit drug, such as GHB, or when bereaved relatives or next of kin are told that results of post-mortem toxicology were indicative of ante-mortem intake of GHB.
The usual analytical cut-off concentrations of GHB in living subjects are 3-5 mg/L for blood and 5-10 mg/L for urine and higher results point towards exogenous exposure to GHB. For post-mortem specimens the corresponding GHB concentrations are 30 mg/L for femoral blood and 30 mg/L for bladder urine are usually recommended. Moreover, all the circumstances surrounding the death need to be considered, including condition of the body (post-mortem interval), extent of trauma and any decomposition, discovery at the scene of death, age, gender and occupation of the deceased and prior medical history. The stability of GHB is improved by keeping the specimens in a refrigerator or frozen and sodium fluoride (1-2 %) should be added as enzyme inhibitor to help stabilize GHB concentrations.
Use of sodium oxybate medication as a treatment for alcohol withdrawal has a 20-year history in some countries, such as Italy. There is good evidence that GHB taken several times daily helps to reduce craving and prevent relapse to drinking alcohol [190]. The most effective pharmacotherapy for alcohol withdrawal is an open question, although available evidence suggests that GHB is just as effective as naltrexone or acamprosate [37, 191]. To our knowledge there does not appear to be any diversion of sodium oxybate (GHB) from the licit to illicit market as has happened on such a large scale with other medications subject to abuse, such as methadone and oxycodone [192] both widely used for pain management [192, 193].
Although the newer “club drugs” or “legal highs” such as spice (synthetic cannabinoids) and bath salts (synthetic catinones), currently attract a lot of attention from the news media and many publications in the medical and forensic literature [194-197], GHB and its analogues continue to represent a public health problem and are commonly encountered in DUID investigations and in post-mortem toxicology when poisoning deaths are investigated [7, 8]. Forensic practitioners need to appreciate the difficulties in interpreting GHB concentrations and be able to differentiate post-mortem synthesis from ante-mortem ingestion of this illicit drug.
DECLARATION
There was no external funding applied for or received to prepare this manuscript and the authors do not consider they have any conflicts of interest in publishing the results and conclusions in this review.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.
REFERENCES
- 1.Couper F.J, Marinetti L.J. Gamma-hydroxybutyrate - effects on human performance and behavior. Forensic Sci. Rev. 2002;14:101–121. [PubMed] [Google Scholar]
- 2.Timby N, Eriksson A, Boström K. Gamma-hydroxybutyrate associated deaths. Am. J. Med. 2000;108(6):518–519. doi: 10.1016/S0002-9343(99)00468-4. [DOI] [PubMed] [Google Scholar]
- 3.Nicholson K.L, Balster R.L. GHB: a new and novel drug of abuse. Drug Alcohol Depend. 2001;63(1):1–22. doi: 10.1016/S0376-8716(00)00191-5. [DOI] [PubMed] [Google Scholar]
- 4.Caldicott D.G, Chow F.Y, Burns B.J, Felgate P.D, Byard R.W. Fatalities associated with the use of gamma-hydroxybutyrate and its analogues in Australasia. Med. J. Aust. 2004;181(6):310–313. doi: 10.5694/j.1326-5377.2004.tb06295.x. [DOI] [PubMed] [Google Scholar]
- 5.Knudsen K, Greter J, Verdicchio M. High mortality rates among GHB abusers in Western Sweden. Clin. Toxicol. (Phila.) 2008;46(3):187–192. doi: 10.1080/15563650701263633. [DOI] [PubMed] [Google Scholar]
- 6.Knudsen K, Jonsson U, Abrahamsson J. Twenty-three deaths with gamma-hydroxybutyrate overdose in western Sweden between 2000 and 2007. Acta Anaesthesiol. Scand. 2010;54(8):987–992. doi: 10.1111/j.1399-6576.2010.02278.x. [DOI] [PubMed] [Google Scholar]
- 7.Gable R.S. Comparison of acute lethal toxicity of commonly abused psychoactive substances. Addiction. 2004;99(6):686–696. doi: 10.1111/j.1360-0443.2004.00744.x. [DOI] [PubMed] [Google Scholar]
- 8.Schulz M, Iwersen-Bergmann S, Andresen H, Schmoldt A. Therapeutic and toxic blood concentrations of nearly 1,000 drugs and other xenobiotics. Crit. Care. 2012;16(4):R136. doi: 10.1186/cc11441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Elliott S.P. Nonfatal instances of intoxication with gamma-hydroxybutyrate in the United Kingdom. Ther. Drug Monit. 2004;26(4):432–440. doi: 10.1097/00007691-200408000-00014. [DOI] [PubMed] [Google Scholar]
- 10.Galicia M, Nogue S, Miró O. Liquid ecstasy intoxication: clinical features of 505 consecutive emergency department patients. Emerg. Med. J. 2011;28(6):462–466. doi: 10.1136/emj.2008.068403. [DOI] [PubMed] [Google Scholar]
- 11.Schep L.J, Knudsen K, Slaughter R.J, Vale J.A, Mégarbane B. The clinical toxicology of γ-hydroxybutyrate, γ-butyrolactone and 1,4-butanediol. Clin. Toxicol. (Phila.) 2012;50(6):458–470. doi: 10.3109/15563650.2012.702218. [DOI] [PubMed] [Google Scholar]
- 12.Anderson IB, Kim SY, Dyer JE, Burkhardt CB, Iknoian JC, Walsh MJ, Blanc PD. Trends in gamma-hydroxybutyrate (GHB) and related drug intoxication: 1999 to 2003. Ann. Emerg. Med. 2006;47 (2):177–83. doi: 10.1016/j.annemergmed.2005.10.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Andresen H, Aydin B.E, Mueller A, Iwersen-Bergmann S. An overview of gamma-hydroxybutyric acid: pharmacodynamics, pharmacokinetics, toxic effects, addiction, analytical methods, and interpretation of results. Drug Test. Anal. 2011;3(9):560–568. doi: 10.1002/dta.254. [DOI] [PubMed] [Google Scholar]
- 14.Zvosec D.L, Smith S.W, Hall B.J. Three deaths associated with use of Xyrem. Sleep Med. 2009;10(4):490–3. doi: 10.1016/j.sleep.2009.01.005. [DOI] [PubMed] [Google Scholar]
- 15.Kintz P. Bioanalytical procedures for detection of chemical agents in hair in the case of drug-facilitated crimes. Anal. Bioanal. Chem. 2007;388(7):1467–1474. doi: 10.1007/s00216-007-1209-z. [DOI] [PubMed] [Google Scholar]
- 16.Negrusz A, Gaensslen R.E. Analytical developments in toxicological investigation of drug-facilitated sexual assault. Anal. Bioanal. Chem. 2003;376(8):1192–1197. doi: 10.1007/s00216-003-1896-z. [DOI] [PubMed] [Google Scholar]
- 17.Stillwell M.E. Drug-facilitated sexual assault involving gamma-hydroxybutyric acid. J. Forensic Sci. 2002;47(5):1133–1134. [PubMed] [Google Scholar]
- 18.Schwartz R.H, Milteer R, LeBeau M.A. Drug-facilitated sexual assault (‘date rape’) South. Med. J. 2000;93(6):558–561. doi: 10.1097/00007611-200006000-00002. [DOI] [PubMed] [Google Scholar]
- 19.Jones A.W, Holmgren A, Kugelberg F.C. Driving under the influence of gamma-hydroxybutyrate (GHB) Forensic Sci. Med. Pathol. 2008;4(4):205–211. doi: 10.1007/s12024-008-9040-1. [DOI] [PubMed] [Google Scholar]
- 20.Kugelberg F.C, Holmgren A, Eklund A, Jones A.W. Forensic toxicology findings in deaths involving gamma-hydroxybutyrate. Int. J. Legal Med. 2010;124(1):1–6. doi: 10.1007/s00414-008-0299-2. [DOI] [PubMed] [Google Scholar]
- 21.Zvosec D.L, Smith S.W, Porrata T, Strobl A.Q, Dyer J.E. Case series of 226 γ-hydroxybutyrate-associated deaths: lethal toxicity and trauma. Am. J. Emerg. Med. 2011;29(3):319–332. doi: 10.1016/j.ajem.2009.11.008. [DOI] [PubMed] [Google Scholar]
- 22.Brunt T.M, van Amsterdam J.G, van den Brink W. GHB, GBL and 1,4-BD addiction. Curr. Pharm. Des. 2014;20(25):4076–4085. doi: 10.2174/13816128113199990624. [DOI] [PubMed] [Google Scholar]
- 23. Wood DM, Warren-Gash C, Ashraf T, Greene SL, Shather Z, Trivedy C, Clarke S, Ramsey J, Holt DW, Dargan PI. Medical and legal confusion surrounding gamma-hydroxybutyrate (GHB) and its precursors gamma-butyrolactone (GBL) and 1 4-butanediol (1 4BD) QJM. 2008;101 (1):23–9. doi: 10.1093/qjmed/hcm117. [DOI] [PubMed] [Google Scholar]
- 24.Krul J, Girbes A.R. γ-Hydroxybutyrate: experience of 9 years of γ-hydroxybutyrate (GHB)-related incidents during rave parties in The Netherlands. Clin. Toxicol. (Phila.) 2011;49(4):311–315. doi: 10.3109/15563650.2011.576253. [DOI] [PubMed] [Google Scholar]
- 25.Drasbek K.R, Christensen J, Jensen K. Gamma-hydroxybutyrate--a drug of abuse. Acta Neurol. Scand. 2006;114(3):145–156. doi: 10.1111/j.1600-0404.2006.00712.x. [DOI] [PubMed] [Google Scholar]
- 26.Palmer R.B. Gamma-butyrolactone and 1,4-butanediol: abused analogues of gamma-hydroxybutyrate. Toxicol. Rev. 2004;23(1):21–31. doi: 10.2165/00139709-200423010-00003. [DOI] [PubMed] [Google Scholar]
- 27.Wong C.G, Chan K.F, Gibson K.M, Snead O.C. Gamma-hydroxybutyric acid: neurobiology and toxicology of a recreational drug. Toxicol. Rev. 2004;23(1):3–20. doi: 10.2165/00139709-200423010-00002. [DOI] [PubMed] [Google Scholar]
- 28.Tunnicliff G. Sites of action of gamma-hydroxybutyrate (GHB)--a neuroactive drug with abuse potential. J. Toxicol. Clin. Toxicol. 1997;35(6):581–590. doi: 10.3109/15563659709001236. [DOI] [PubMed] [Google Scholar]
- 29.Trudell J.R, Messing R.O, Mayfield J, Harris R.A. Alcohol dependence: molecular and behavioral evidence. Trends Pharmacol. Sci. 2014;35(7):317–323. doi: 10.1016/j.tips.2014.04.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Whiting P.J. GABA-A receptor subtypes in the brain: a paradigm for CNS drug discovery? Drug Discov. Today. 2003;8(10):445–450. doi: 10.1016/S1359-6446(03)02703-X. [DOI] [PubMed] [Google Scholar]
- 31.Pardi D, Black J. gamma-Hydroxybutyrate/sodium oxybate: neurobiology, and impact on sleep and wakefulness. CNS Drugs. 2006;20(12):993–1018. doi: 10.2165/00023210-200620120-00004. [DOI] [PubMed] [Google Scholar]
- 32.Robinson D.M, Keating G.M. Sodium oxybate: a review of its use in the management of narcolepsy. CNS Drugs. 2007;21(4):337–354. doi: 10.2165/00023210-200721040-00007. [DOI] [PubMed] [Google Scholar]
- 33.Carter LP, Pardi D, Gorsline J, Griffiths RR. Illicit gammahydroxybutyrate (GHB) and pharmaceutical sodium oxybate (xyrem) Differences in characteristics and misuse. Drug Alcohol Depend. 2009;104(1-2):1–10. doi: 10.1016/j.drugalcdep.2009.04.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Dauvilliers Y, Arnulf I, Mignot E. Narcolepsy with cataplexy. Lancet. 2007;369(9560):499–511. doi: 10.1016/S0140-6736(07)60237-2. [DOI] [PubMed] [Google Scholar]
- 35.Ferrara S.D, Zotti S, Tedeschi L, Frison G, Castagna F, Gallimberti L, Gessa G.L, Palatini P. Pharmacokinetics of gamma-hydroxybutyric acid in alcohol dependent patients after single and repeated oral doses. Br. J. Clin. Pharmacol. 1992;34(3):231–235. doi: 10.1111/j.1365-2125.1992.tb04129.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Keating G.M. Sodium oxybate: a review of its use in alcohol withdrawal syndrome and in the maintenance of abstinence in alcohol dependence. Clin. Drug Investig. 2014;34(1):63–80. doi: 10.1007/s40261-013-0158-x. [DOI] [PubMed] [Google Scholar]
- 37.Skala K, Caputo F, Mirijello A, Vassallo G, Antonelli M, Ferrulli A, Walter H, Lesch O, Addolorato G. Sodium oxybate in the treatment of alcohol dependence: from the alcohol withdrawal syndrome to the alcohol relapse prevention. Expert Opin. Pharmacother. 2014;15(2):245–257. doi: 10.1517/14656566.2014.863278. [DOI] [PubMed] [Google Scholar]
- 38.Chick J, Nutt D.J. Substitution therapy for alcoholism: time for a reappraisal? J. Psychopharmacol. 2012;26(2):205–212. doi: 10.1177/0269881111408463. [DOI] [PubMed] [Google Scholar]
- 39.Ingels A.S, Wille S.M, Samyn N, Lambert W.E, Stove C.P. Screening and confirmation methods for GHB determination in biological fluids. Anal. Bioanal. Chem. 2014;406(15):3553–3577. doi: 10.1007/s00216-013-7586-6. [DOI] [PubMed] [Google Scholar]
- 40.Mari F, Politi L, Trignano C, Di Milia M.G, Di Padua M, Bertol E. What constitutes a normal ante-mortem urine GHB concentration? J. Forensic Leg. Med. 2009;16(3):148–151. doi: 10.1016/j.jflm.2008.08.014. [DOI] [PubMed] [Google Scholar]
- 41.Bessman S.P, Fishbein W.N. Gamma-hydroxybutyrate, a normal brain metabolite. Nature. 1963;200:1207–1208. doi: 10.1038/2001207a0. [DOI] [PubMed] [Google Scholar]
- 42.Andresen H, Sprys N, Schmoldt A, Mueller A, Iwersen-Bergmann S. Gamma-hydroxybutyrate in urine and serum: additional data supporting current cut-off recommendations. Forensic Sci. Int. 2010;200(1-3):93–99. doi: 10.1016/j.forsciint.2010.03.035. [DOI] [PubMed] [Google Scholar]
- 43.Berankova K, Mutnanska K, Balikova M. Gammahydroxybutyric acid stability and formation in blood and urine. Forensic Sci. Int. 2006;161(2-3):158–62. doi: 10.1016/j.forsciint.2006.01.017. [DOI] [PubMed] [Google Scholar]
- 44.Kintz P, Villain M, Cirimele V, Ludes B. GHB in postmortem toxicology. Discrimination between endogenous production from exposure using multiple specimens. Forensic Sci. Int. 2004;143(2-3):177–181. doi: 10.1016/j.forsciint.2004.02.036. [DOI] [PubMed] [Google Scholar]
- 45.Elliott S, Lowe P, Symonds A. The possible influence of micro-organisms and putrefaction in the production of GHB in post-mortem biological fluid. Forensic Sci. Int. 2004;139(2-3):183–190. doi: 10.1016/j.forsciint.2003.10.018. [DOI] [PubMed] [Google Scholar]
- 46.Elliott S.P. Gamma hydroxybutyric acid (GHB) concentrations in humans and factors affecting endogenous production. Forensic Sci. Int. 2003;133(1-2):9–16. doi: 10.1016/S0379-0738(03)00043-4. [DOI] [PubMed] [Google Scholar]
- 47.Elliott S.P. Further evidence for the presence of GHB in postmortem biological fluid: implications for the interpretation of findings. J. Anal. Toxicol. 2004;28(1):20–26. doi: 10.1093/jat/28.1.20. [DOI] [PubMed] [Google Scholar]
- 48.Wood D.M, Brailsford A.D, Dargan P.I. Acute toxicity and withdrawal syndromes related to γ-hydroxybutyrate (GHB) and its analogues γ-butyrolactone (GBL) and 1,4-butanediol (1,4-BD) Drug Test. Anal. 2011;3(7-8):417–425. doi: 10.1002/dta.292. [DOI] [PubMed] [Google Scholar]
- 49.Marinetti L.J, Lebeau M.A. The use of GHB and analogs to facilitate sexual assault. Forensic Sci. Rev. 2010;22:41–59. [PubMed] [Google Scholar]
- 50.Snead O.C, III, Gibson K.M. Gamma-hydroxybutyric acid. N. Engl. J. Med. 2005;352(26):2721–2732. doi: 10.1056/NEJMra044047. [DOI] [PubMed] [Google Scholar]
- 51.Zvosec D.L, Smith S.W, McCutcheon J.R, Spillane J, Hall B.J, Peacock E.A. Adverse events, including death, associated with the use of 1,4-butanediol. N. Engl. J. Med. 2001;344(2):87–94. doi: 10.1056/NEJM200101113440202. [DOI] [PubMed] [Google Scholar]
- 52.EMCDDA, GHB and its precursor GBL; An emerging trend case study European Monitoring Centre for Drugs and Drug Addiction; Lisbon. 2008. [Google Scholar]
- 53.EMCDDA. Report on risk assessment of GHB in the framework of the joint action on new synthetic drugs. 2002.
- 54.Sexual assaults facilitated by drugs and alcohol European Monitoring Centre for Drugs and Drug Addiction. Lisbon: 2008. EMCDDA. [Google Scholar]
- 55.ACMD; Drug facilitated sexual assault; London, UK. 2007. [Google Scholar]
- 56.WHO; Gamma-hydroxybutyric acid (GHB) critical review report; Geneva, Switzerland. 2012. [Google Scholar]
- 57.Jones A.W, Holmgren A, Ahlner J. Toxicological analysis of blood and urine samples from female victims of alleged sexual assault. Clin. Toxicol. (Phila.) 2012;50(7):555–561. doi: 10.3109/15563650.2012.702217. [DOI] [PubMed] [Google Scholar]
- 58.Parkin M.C, Brailsford A.D. Retrospective drug detection in cases of drug-facilitated sexual assault: challenges and perspectives for the forensic toxicologist. Bioanalysis. 2009;1(5):1001–1013. doi: 10.4155/bio.09.70. [DOI] [PubMed] [Google Scholar]
- 59. Mccambridge J, Mitcheson L, Winstock A, Hunt N. Fiveyear trends in patterns of drug use among people who use stimulants in dance contexts in the united kingdom. Addiction. 2005;100(8):1140–9. doi: 10.1111/j.1360-0443.2005.001127.x. [DOI] [PubMed] [Google Scholar]
- 60.Wood D.M, Nicolaou M, Dargan P.I. Epidemiology of recreational drug toxicity in a nightclub environment. Subst. Use Misuse. 2009;44(11):1495–1502. doi: 10.3109/10826080802543580. [DOI] [PubMed] [Google Scholar]
- 61.Talbert JJ. Club drugs Coming to a patient near you. Nurse Pract . 2014;39 (3):20–25. doi: 10.1097/01.NPR.0000443227.72357.72. [DOI] [PubMed] [Google Scholar]
- 62.Gonzalez A, Nutt D.J. Gamma hydroxy butyrate abuse and dependency. J. Psychopharmacol. 2005;19(2):195–204. doi: 10.1177/0269881105049041. [DOI] [PubMed] [Google Scholar]
- 63.Al-Samarraie M.S, Karinen R, Mørland J, Stokke Opdal M. Blood GHB concentrations and results of medical examinations in 25 car drivers in Norway. Eur. J. Clin. Pharmacol. 2010;66(10):987–998. doi: 10.1007/s00228-010-0870-x. [DOI] [PubMed] [Google Scholar]
- 64.Jones A.W, Holmgren A, Kugelberg F.C. Gamma-hydroxybutyrate concentrations in the blood of impaired drivers, users of illicit drugs, and medical examiner cases. J. Anal. Toxicol. 2007;31(9):566–572. doi: 10.1093/jat/31.9.566. [DOI] [PubMed] [Google Scholar]
- 65.Johnston L.D, O'Malley P.M, Bachman J.G, Schulenberg J.E. Monitoring the future, national survey results on drug use 1975-volume 1, secondary school students The National Institute of Drug Abuse; Ann Arbor. 2013. [Google Scholar]
- 66.Johnston L.D, O'Malley P.M, Bachman J.G, Schulenberg J.E. Monitoring the future, national survey results on drug use 1975-2013 volume 2, college students and adults The National Institute of Drug Abuse ; Ann Arbor. 2013. [Google Scholar]
- 67.Britt G.C, McCance-Katz E.F. A brief overview of the clinical pharmacology of “club drugs”. Subst. Use Misuse. 2005;40(9-10):1189–1201. doi: 10.1081/JA-200066730. [DOI] [PubMed] [Google Scholar]
- 68.Bosch O.G, Quednow B.B, Seifritz E, Wetter T.C. Reconsidering GHB: orphan drug or new model antidepressant? J. Psychopharmacol. (Oxford) 2012;26(5):618–628. doi: 10.1177/0269881111421975. [DOI] [PubMed] [Google Scholar]
- 69.Saytzeff A. Ueber die reduction des succinylchlorids. 1874. [DOI]
- 70.Brown A.J. Low-carb diets, fasting and euphoria: Is there a link between ketosis and gamma-hydroxybutyr . 2007;68(2):268–71. doi: 10.1016/j.mehy.2006.07.043. [DOI] [PubMed] [Google Scholar]
- 71.Vickers M.D. Gamma hydroxybutyric acid. Clinical pharmacology and current status. Proc. R. Soc. Med. 1968;61(8):821–824. [PMC free article] [PubMed] [Google Scholar]
- 72.Helrich M, McAslan T.C, Skolnik S, Bessman S.P. Correlation of blood levels of 4-hydroxybutyrate with state of consciousness. Anesthesiology. 1964;25:771–775. doi: 10.1097/00000542-196411000-00007. [DOI] [PubMed] [Google Scholar]
- 73.Abramowitz M.Z. GHB and date rape. Br. J. Psychiatry. 2004;185:176–177. doi: 10.1192/bjp.185.2.176. [DOI] [PubMed] [Google Scholar]
- 74.Varela M, Nogué S, Orós M, Miró O. Gamma hydroxybutirate use for sexual assault. Emerg. Med. J. 2004;21(2):255–256. doi: 10.1136/emj.2002.002402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.De Paoli G, Walker K.M, Pounder D.J. Endogenous γ-hydroxybutyric acid concentrations in saliva determined by gas chromatography-mass spectrometry. J. Anal. Toxicol. 2011;35(3):148–152. doi: 10.1093/anatox/35.3.148. [DOI] [PubMed] [Google Scholar]
- 76.Marinetti L.J, Isenschmid D.S, Hepler B.R, Kanluen S. Analysis of GHB and 4-methyl-GHB in postmortem matrices after long-term storage. J. Anal. Toxicol. 2005;29(1):41–47. doi: 10.1093/jat/29.1.41. [DOI] [PubMed] [Google Scholar]
- 77.Mazarr-Proo S, Kerrigan S. Distribution of GHB in tissues and fluids following a fatal overdose. J. Anal. Toxicol. 2005;29(5):398–400. doi: 10.1093/jat/29.5.398. [DOI] [PubMed] [Google Scholar]
- 78.Moriya F, Hashimoto Y. Site-dependent production of gammahydroxybutyric acid in the early postmortem period. Forensic Sci. Int. 2005;148(2-3):139–42. doi: 10.1016/j.forsciint.2004.05.002. [DOI] [PubMed] [Google Scholar]
- 79.Stove C.P, Ingels A.S, Lambert W.E. Quantitation of gamma-hydroxybutyric acid in dried blood spots in newborn screening. Mol. Genet. Metab. 2013;110(1-2):195. doi: 10.1016/j.ymgme.2013.06.009. [DOI] [PubMed] [Google Scholar]
- 80.Ingels A.S, Lambert W.E, Stove C.P. Determination of gamma-hydroxybutyric acid in dried blood spots using a simple GC-MS method with direct “on spot” derivatization. Anal. Bioanal. Chem. 2010;398(5):2173–2182. doi: 10.1007/s00216-010-4183-9. [DOI] [PubMed] [Google Scholar]
- 81.Bertol E, Argo A, Procaccianti P, Vaiano F, Di Milia M.G, Furlanetto S, Mari F. Detection of gamma-hydroxybutyrate in hair: validation of GC-MS and LC-MS/MS methods and application to a real case. J. Pharm. Biomed. Anal. 2012;70:518–522. doi: 10.1016/j.jpba.2012.07.009. [DOI] [PubMed] [Google Scholar]
- 82. Mion G, Tourtier JP, Diraison Y. Gamma-hydroxybutyric acid in hair. N. Engl. J. Med. 2006;354 (1):96–7. doi: 10.1056/NEJMc053116. [DOI] [PubMed] [Google Scholar]
- 83.Kintz P, Cirimele V, Jamey C, Ludes B. Testing for GHB in hair by GC/MS/MS after a single exposure. Application to document sexual assault. J. Forensic Sci. 2003;48(1):195–200. [PubMed] [Google Scholar]
- 84.Goullé J.P, Chèze M, Pépin G. Determination of endogenous levels of GHB in human hair. Are there possibilities for the identification of GHB administration through hair analysis in cases of drug-facilitated sexual assault? J. Anal. Toxicol. 2003;27(8):574–580. doi: 10.1093/jat/27.8.574. [DOI] [PubMed] [Google Scholar]
- 85.Couper F.J, Logan B.K. Determination of gamma-hydroxybutyrate (GHB) in biological specimens by gas chromatography--mass spectrometry. J. Anal. Toxicol. 2000;24(1):1–7. doi: 10.1093/jat/24.1.1. [DOI] [PubMed] [Google Scholar]
- 86.Ingels A.S, Neels H, Lambert W.E, Stove C.P. Determination of gamma-hydroxybutyric acid in biofluids using a one-step procedure with “in-vial” derivatization and headspace-trap gas chromatography-mass spectrometry. J. Chromatogr. A. 2013;1296:84–92. doi: 10.1016/j.chroma.2013.04.023. [DOI] [PubMed] [Google Scholar]
- 87.Elian A.A. GC-MS determination of gamma-hydroxybutyric acid (GHB) in blood. Forensic Sci. Int. 2001;122(1):43–47. doi: 10.1016/S0379-0738(01)00441-8. [DOI] [PubMed] [Google Scholar]
- 88.Dahl S.R, Olsen K.M, Strand D.H. Determination of γ-hydroxybutyrate (GHB), β-hydroxybutyrate (BHB), pregabalin, 1,4-butane-diol (1,4BD) and γ-butyrolactone (GBL) in whole blood and urine samples by UPLC-MSMS. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2012;885-886:37–42. doi: 10.1016/j.jchromb.2011.12.009. [DOI] [PubMed] [Google Scholar]
- 89.Elian A.A, Hackett J. Anion exchange SPE and liquid chromatography-tandem mass spectrometry in GHB analysis. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2011;879(31):3752–3758. doi: 10.1016/j.jchromb.2011.09.018. [DOI] [PubMed] [Google Scholar]
- 90.Sørensen L.K, Hasselstrøm J.B. A hydrophilic interaction liquid chromatography electrospray tandem mass spectrometry method for the simultaneous determination of γ-hydroxybutyrate and its precursors in forensic whole blood. Forensic Sci. Int. 2012;222(1-3):352–359. doi: 10.1016/j.forsciint.2012.07.017. [DOI] [PubMed] [Google Scholar]
- 91.Blair S, Song M, Hall B, Brodbelt J. Determination of gamma-hydroxybutyrate in water and human urine by solid phase microextraction-gas chromatography/quadrupole ion trap spectrometry. J. Forensic Sci. 2001;46(3):688–693. [PubMed] [Google Scholar]
- 92.Stout P.A, Simons K.D, Kerrigan S. Quantitative analysis of gamma-hydroxybutyrate at endogenous concentrations in hair using liquid chromatography tandem mass spectrometry. J. Forensic Sci. 2010;55(2):531–7. doi: 10.1111/j.1556-4029.2009.01304.x. [DOI] [PubMed] [Google Scholar]
- 93.Johansen S.S, Windberg C.N. Simultaneous determination of γ-Hydroxybutyrate (GHB) and its analogues (GBL, 1.4-BD, GVL) in whole blood and urine by liquid chromatography coupled to tandem mass spectrometry. J. Anal. Toxicol. 2011;35(1):8–14. doi: 10.1093/anatox/35.1.8. [DOI] [PubMed] [Google Scholar]
- 94.Kaufmann E, Alt A. Determination of GHB in urine and serum by LC/MS using a simple one-step derivative. Forensic Sci. Int. 2007;168 (2-3):133–7. doi: 10.1016/j.forsciint.2006.07.002. [DOI] [PubMed] [Google Scholar]
- 95.Lebeau MA, Montgomery MA, Miller ML, Burmeister SG. Analysis of biofluids for gamma-hydroxybutyrate (GHB) and gamma-butyrolactone (GBL) by headspace GC-FID and GC-MS. J. Anal. Toxicol. 2000;24 (6):421–8. doi: 10.1093/jat/24.6.421. [DOI] [PubMed] [Google Scholar]
- 96.Meyer M.R, Weber A.A, Maurer H.H. A validated GC-MS procedure for fast, simple, and cost-effective quantification of glycols and GHB in human plasma and their identification in urine and plasma developed for emergency toxicology. Anal. Bioanal. Chem. 2011;400(2):411–414. doi: 10.1007/s00216-011-4760-6. [DOI] [PubMed] [Google Scholar]
- 97.Grenier V, Huppé G, Lamarche M, Mireault P. Enzymatic assay for GHB determination in forensic matrices. J. Anal. Toxicol. 2012;36(7):523–528. doi: 10.1093/jat/bks053. [DOI] [PubMed] [Google Scholar]
- 98.Hasan L, Jermann T.M, Weber J.M, Abrahamsson L, Sciotti M.A, Böttcher M, Jöchle W, Gygax D, Scholer A. An enzymatic method to determine γ-hydroxybutyric acid in serum and urine. Ther. Drug Monit. 2011;33(6):757–765. doi: 10.1097/FTD.0b013e318239a41a. [DOI] [PubMed] [Google Scholar]
- 99.Bravo D.T, Harris D.O, Parsons S.M. Reliable, sensitive, rapid and quantitative enzyme-based assay for gamma-hydroxybutyric acid (GHB) J. Forensic Sci. 2004;49(2):379–387. doi: 10.1520/JFS2003165. [DOI] [PubMed] [Google Scholar]
- 100.Petersen I.N, Tortzen C, Kristensen J.L, Pedersen D.S, Breindahl T. Identification of a new metabolite of GHB: gamma-hydroxybutyric acid glucuronide. J. Anal. Toxicol. 2013;37(5):291–297. doi: 10.1093/jat/bkt027. [DOI] [PubMed] [Google Scholar]
- 101.Crunelle C.L, Cappelle D, Covaci A, van Nuijs A.L, Maudens K.E, Sabbe B, Dom G, Michielsen P, Yegles M, Neels H. Hair ethyl glucuronide as a biomarker of alcohol consumption in alcohol-dependent patients: role of gender differences. Drug Alcohol Depend. 2014;141:163–166. doi: 10.1016/j.drugalcdep.2014.05.014. [DOI] [PubMed] [Google Scholar]
- 102.Bertol E, Mari F, Vaiano F, Romano G, Zaami S, Baglìo G, Busardò F.P. Determination of GHB in human hair by HPLC-MS/MS: Development and validation of a method and application to a study group and three possible single exposure cases. Drug Test. Anal. 2014 doi: 10.1002/dta.1679. [DOI] [PubMed] [Google Scholar]
- 103.Carai M.A, Colombo G, Brunetti G, Melis S, Serra S, Vacca G, Mastinu S, Pistuddi A.M, Solinas C, Cignarella G, Minardi G, Gessa G.L. Role of GABA(B) receptors in the sedative/hypnotic effect of gamma-hydroxybutyric acid. Eur. J. Pharmacol. 2001;428(3):315–321. doi: 10.1016/S0014-2999(01)01334-6. [DOI] [PubMed] [Google Scholar]
- 104.Crunelli V, Emri Z, Leresche N. Unravelling the brain targets of gamma-hydroxybutyric acid. Curr. Opin. Pharmacol. 2006;6(1):44–52. doi: 10.1016/j.coph.2005.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Carai M.A, Colombo G, Reali R, Serra S, Mocci I, Castelli M.P, Cignarella G, Gessa G.L. Central effects of 1,4-butanediol are mediated by GABA(B) receptors via its conversion into gamma-hydroxybutyric acid. Eur. J. Pharmacol. 2002;441(3):157–163. doi: 10.1016/S0014-2999(02)01502-9. [DOI] [PubMed] [Google Scholar]
- 106.Chalifoux J.R, Carter A.G. GABAB receptor modulation of synaptic function. Curr. Opin. Neurobiol. 2011;21(2):339–344. doi: 10.1016/j.conb.2011.02.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Snead O.C., III The ontogeny of GABAergic enhancement of the gamma-hydroxybutyrate model of generalized absence seizures. Epilepsia. 1990;31(4):363–368. doi: 10.1111/j.1528-1157.1990.tb05489.x. [DOI] [PubMed] [Google Scholar]
- 108.Snead O.C., III Evidence for a G protein-coupled gamma-hydroxybutyric acid receptor. J. Neurochem. 2000;75(5):1986–1996. doi: 10.1046/j.1471-4159.2000.0751986.x. [DOI] [PubMed] [Google Scholar]
- 109.Tabakoff B, Hoffman P.L. The neurobiology of alcohol consumption and alcoholism: an integrative history. Pharmacol. Biochem. Behav. 2013;113:20–37. doi: 10.1016/j.pbb.2013.10.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Tyacke R.J, Lingford-Hughes A, Reed L.J, Nutt D.J. GABAB receptors in addiction and its treatment. Adv. Pharmacol. 2010;58:373–396. doi: 10.1016/S1054-3589(10)58014-1. [DOI] [PubMed] [Google Scholar]
- 111.Carter L.P, Koek W, France C.P. Behavioral analyses of GHB: receptor mechanisms. Pharmacol. Ther. 2009;121(1):100–114. doi: 10.1016/j.pharmthera.2008.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Snead O.C., III Gamma hydroxybutyrate in the monkey. IV. Dopaminergic mechanisms. Neurology. 1978;28(11):1179–1182. doi: 10.1212/WNL.28.11.1179. [DOI] [PubMed] [Google Scholar]
- 113.Feigenbaum J.J, Howard S.G. Gamma hydroxybutyrate is not a GABA agonist. Prog. Neurobiol. 1996;50(1):1–7. doi: 10.1016/0301-0082(96)00029-9. [DOI] [PubMed] [Google Scholar]
- 114.Koek W, France C.P. Cataleptic effects of gamma-hydroxybutyrate (GHB) and baclofen in mice: mediation by GABA(B) receptors, but differential enhancement by N-methyl-d-aspartate (NMDA) receptor antagonists. Psychopharmacology (Berl.) 2008;199(2):191–198. doi: 10.1007/s00213-008-1160-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Bay T, Eghorn LF, Klein AB, Wellendorph P. GHB receptor targets in the CNS Focus on high-affinity binding sites. Biochem. Pharmacol. 2014;87 (2):220–8. doi: 10.1016/j.bcp.2013.10.028. [DOI] [PubMed] [Google Scholar]
- 116.Kaupmann K, Cryan J.F, Wellendorph P, Mombereau C, Sansig G, Klebs K, Schmutz M, Froestl W, van der Putten H, Mosbacher J, Bräuner-Osborne H, Waldmeier P, Bettler B. Specific gamma-hydroxybutyrate-binding sites but loss of pharmacological effects of gamma-hydroxybutyrate in GABA(B)(1)-deficient mice. Eur. J. Neurosci. 2003;18(10):2722–2730. doi: 10.1111/j.1460-9568.2003.03013.x. [DOI] [PubMed] [Google Scholar]
- 117.Schröck A, Hari Y, König S, Auwärter V, Schürch S, Weinmann W. Pharmacokinetics of GHB and detection window in serum and urine after single uptake of a low dose of GBL - an experiment with two volunteers. Drug Test. Anal. 2014;6(4):363–366. doi: 10.1002/dta.1498. [DOI] [PubMed] [Google Scholar]
- 118.Brailsford A.D, Cowan D.A, Kicman A.T. Pharmacokinetic properties of γ-hydroxybutyrate (GHB) in whole blood, serum, and urine. J. Anal. Toxicol. 2012;36(2):88–95. doi: 10.1093/jat/bkr023. [DOI] [PubMed] [Google Scholar]
- 119.Hefele B, Naumann N, Trollmann R, Dittrich K, Rascher W. Fast-in, fast-out. Lancet. 2009;373(9672):1398. doi: 10.1016/S0140-6736(09)60570-5. [DOI] [PubMed] [Google Scholar]
- 120.Charlebois R.C, Corbett M.R, Wigmore J.G. Comparison of ethanol concentrations in blood, serum, and blood cells for forensic application. J. Anal. Toxicol. 1996;20(3):171–178. doi: 10.1093/jat/20.3.171. [DOI] [PubMed] [Google Scholar]
- 121.Iffland R, West A, Bilzer N, Schuff A. Zur zuverlässigkeit der blutalkohol bestimmung. Das verkeilungsverhältnis des wassers zwischen serum und vollblut. Rechtsmedizin. 1999;9:123–130. doi: 10.1007/s001940050094. [DOI] [Google Scholar]
- 122.Abanades S, Farré M, Segura M, Pichini S, Barral D, Pacifici R, Pellegrini M, Fonseca F, Langohr K, De La Torre R. Gamma-hydroxybutyrate (GHB) in humans: pharmacodynamics and pharmacokinetics. Ann. N. Y. Acad. Sci. 2006;1074:559–576. doi: 10.1196/annals.1369.065. [DOI] [PubMed] [Google Scholar]
- 123.Jones A.W, Eklund A, Kronstrand R. Concentration-time profiles of gamma-hydroxybutyrate in blood after recreational doses are best described by zero-order rather than first-order kinetics. J. Anal. Toxicol. 2009;33(6):332–335. doi: 10.1093/jat/33.6.332. [DOI] [PubMed] [Google Scholar]
- 124.Palatini P, Tedeschi L, Frison G, Padrini R, Zordan R, Orlando R, Gallimberti L, Gessa G.L, Ferrara S.D. Dose-dependent absorption and elimination of gamma-hydroxybutyric acid in healthy volunteers. Eur. J. Clin. Pharmacol. 1993;45(4):353–356. doi: 10.1007/BF00265954. [DOI] [PubMed] [Google Scholar]
- 125.Borgen L.A, Okerholm R, Morrison D, Lai A. The influence of gender and food on the pharmacokinetics of sodium oxybate oral solution in healthy subjects. J. Clin. Pharmacol. 2003;43(1):59–65. doi: 10.1177/0091270002239707. [DOI] [PubMed] [Google Scholar]
- 126.Ferrara S.D, Tedeschi L, Frison G, Orlando R, Mazzo M, Zordan R, Padrini R, Palatini P. Effect of moderate or severe liver dysfunction on the pharmacokinetics of gamma-hydroxybutyric acid. Eur. J. Clin. Pharmacol. 1996;50(4):305–310. doi: 10.1007/s002280050113. [DOI] [PubMed] [Google Scholar]
- 127.Scharf M.B, Lai A.A, Branigan B, Stover R, Berkowitz D.B. Pharmacokinetics of gammahydroxybutyrate (GHB) in narcoleptic patients. Sleep. 1998;21(5):507–514. doi: 10.1093/sleep/21.5.507. [DOI] [PubMed] [Google Scholar]
- 128.Borgen L.A, Okerholm R.A, Lai A, Scharf M.B. The pharmacokinetics of sodium oxybate oral solution following acute and chronic administration to narcoleptic patients. J. Clin. Pharmacol. 2004;44(3):253–257. doi: 10.1177/0091270003262795. [DOI] [PubMed] [Google Scholar]
- 129.Morse B.L, Felmlee M.A, Morris M.E. γ-Hydroxybutyrate blood/plasma partitioning: effect of physiologic pH on transport by monocarboxylate transporters. Drug Metab. Dispos. 2012;40(1):64–69. doi: 10.1124/dmd.111.041285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Abanades S, Farré M, Segura M, Pichini S, Pastor A, Pacifici R, Pellegrini M, de la Torre R. Disposition of gamma-hydroxybutyric acid in conventional and nonconventional biologic fluids after single drug administration: issues in methodology and drug monitoring. Ther. Drug Monit. 2007;29(1):64–70. doi: 10.1097/FTD.0b013e3180307e5e. [DOI] [PubMed] [Google Scholar]
- 131.Thai D, Dyer J.E, Benowitz N.L, Haller C.A. Gamma-hydroxybutyrate and ethanol effects and interactions in humans. J. Clin. Psychopharmacol. 2006;26(5):524–529. doi: 10.1097/01.jcp.0000237944.57893.28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Brenneisen R, Elsohly M.A, Murphy T.P, Passarelli J, Russmann S, Salamone S.J, Watson D.E. Pharmacokinetics and excretion of gamma-hydroxybutyrate (GHB) in healthy subjects. J. Anal. Toxicol. 2004;28(8):625–630. doi: 10.1093/jat/28.8.625. [DOI] [PubMed] [Google Scholar]
- 133.Kavanagh P.V, Kenny P, Feely J. The urinary excretion of gamma-hydroxybutyric acid in man. J. Pharm. Pharmacol. 2001;53(3):399–402. doi: 10.1211/0022357011775460. [DOI] [PubMed] [Google Scholar]
- 134.Morse B.L, Morris M.E. Toxicokinetics/Toxicodynamics of γ-hydroxybutyrate-ethanol intoxication: evaluation of potential treatment strategies. J. Pharmacol. Exp. Ther. 2013;346(3):504–513. doi: 10.1124/jpet.113.206250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135. Thai D, Dyer JE, Jacob P, Haller CA. Clinical pharmacology of 1 4-butanediol and gamma-hydroxybutyrate after oral 1 4-butanediol administration to healthy volunteers. Clin. Pharmacol. Ther. 2007;81 (2):178–84. doi: 10.1038/sj.clpt.6100037. [DOI] [PubMed] [Google Scholar]
- 136.Ciolino L.A, Mesmer M.Z, Satzger R.D, Machal A.C, McCauley H.A, Mohrhaus A.S. The chemical interconversion of GHB and GBL: forensic issues and implications. J. Forensic Sci. 2001;46(6):1315–1323. [PubMed] [Google Scholar]
- 137.Crookes C.E, Faulds M.C, Forrest A.R, Galloway J.H. A reference range for endogenous gamma-hydroxybutyrate in urine by gas chromatography-mass spectrometry. J. Anal. Toxicol. 2004;28(8):644–649. doi: 10.1093/jat/28.8.644. [DOI] [PubMed] [Google Scholar]
- 138.Elian A.A. Determination of endogenous gamma-hydroxybutyric acid (GHB) levels in antemortem urine and blood. Forensic Sci. Int. 2002;128(3):120–122. doi: 10.1016/S0379-0738(02)00183-4. [DOI] [PubMed] [Google Scholar]
- 139.Zörntlein S.W, Kopp A, Becker J, Kaufmann T.J, Röhrich J, Urban R. In vitro production of GHB in blood and serum samples under various storage conditions. Forensic Sci. Int. 2012;214(1-3):113–117. doi: 10.1016/j.forsciint.2011.07.030. [DOI] [PubMed] [Google Scholar]
- 140.LeBeau M.A, Montgomery M.A, Morris-Kukoski C, Schaff J.E, Deakin A, Levine B. A comprehensive study on the variations in urinary concentrations of endogenous gamma-hydroxybutyrate (GHB) J. Anal. Toxicol. 2006;30(2):98–105. doi: 10.1093/jat/30.2.98. [DOI] [PubMed] [Google Scholar]
- 141.Yeatman D.T, Reid K. A study of urinary endogenous gamma-hydroxybutyrate (GHB) levels. J. Anal. Toxicol. 2003;27(1):40–42. doi: 10.1093/jat/27.1.40. [DOI] [PubMed] [Google Scholar]
- 142.Shima N, Miki A, Kamata T, Katagi M, Tsuchihashi H. Urinary endogenous concentrations of GHB and its isomers in healthy humans and diabetics. Forensic Sci. Int. 2005;149(2-3):171–179. doi: 10.1016/j.forsciint.2004.05.017. [DOI] [PubMed] [Google Scholar]
- 143.LeBeau M.A, Christenson R.H, Levine B, Darwin W.D, Huestis M.A. Intra- and interindividual variations in urinary concentrations of endogenous gamma-hydroxybutyrate. J. Anal. Toxicol. 2002;26(6):340–346. doi: 10.1093/jat/26.6.340. [DOI] [PubMed] [Google Scholar]
- 144.Brailsford A.D, Cowan D.A, Kicman A.T. Urinary gamma-hydroxybutyrate concentrations in 1126 female subjects. 2010. [DOI] [PubMed]
- 145.Elliott S, Burgess V. The presence of gamma-hydroxybutyric acid (GHB) and gamma-butyrolactone (GBL) in alcoholic and non-alcoholic beverages. Forensic Sci. Int. 2005;151(2-3):289–292. doi: 10.1016/j.forsciint.2005.02.014. [DOI] [PubMed] [Google Scholar]
- 146.Moriya F, Nishimura H, Furumiya J, Hashimoto Y. Effects of drinking and smoking on endogenous levels of urinary gamma-hydroxybutyric acid, a preliminary study. Leg Med (Tokyo) 2006;8(4):231–234. doi: 10.1016/j.legalmed.2006.05.001. [DOI] [PubMed] [Google Scholar]
- 147.Raknes G, Aronsen L, Fuskevag O.M. Urinary concentrations of gamma-hydroxybutyric acid and related compounds in pregnanc. J. Anal. Toxicol. 2010;34(7):394–399. doi: 10.1093/jat/34.7.394. [DOI] [PubMed] [Google Scholar]
- 148.Kerrigan S. In vitro production of gamma-hydroxybutyrate in antemortem urine samples. J. Anal. Toxicol. 2002;26(8):571–574. doi: 10.1093/jat/26.8.571. [DOI] [PubMed] [Google Scholar]
- 149.Couper F.J, Logan B.K. GHB and driving impairment. J. Forensic Sci. 2001;46(4):919–923. [PubMed] [Google Scholar]
- 150.Dresen S, Kempf J, Weinmann W. Prevalence of gammahydroxybutyrate (GHB) in serum samples of amphetamine metamphetamine and ecstasy impaired drivers. Forensic Sci. Int. 2007;173 (2-3):112–6. doi: 10.1016/j.forsciint.2007.02.009. [DOI] [PubMed] [Google Scholar]
- 151.Nishimura H, Moriya F, Hashimoto Y. Mechansim of gamma-hydroxybutyic acid production during the early postmortem period. Forensic Toxicol. 2009;27:55–60. doi: 10.1007/s11419-009-0067-0. [DOI] [Google Scholar]
- 152.Elliot S. The presence of gamma-hydroxybutyric acid (GHB) in postmortem biological fluids. J. Anal. Toxicol. 2001;25(2):152. doi: 10.1093/jat/25.2.152. [DOI] [PubMed] [Google Scholar]
- 153.Marinetti L.J, Isenschmid D.S, Hepler B.R, Commissaris R.L. Response to the presence of gamma-hydroxybutyric acid (GHB) in postmortem biological fluids. J. Anal. Toxicol. 2001;25(5):356–357. doi: 10.1093/jat/25.5.356. [DOI] [PubMed] [Google Scholar]
- 154.Stephens B.G, Coleman D.E, Baselt R.C. In vitro stability of endogenous gamma-hydroxybutyrate in postmortem blood. J. Forensic Sci. 1999;44(1):231. [PubMed] [Google Scholar]
- 155.Busardò F.P, Bertol E, Vaiano F, Baglio G, Montana A, Barbera N, Zaami S, Romano G. Post mortem concentrations of endogenous gamma hydroxybutyric acid (GHB) and in vitro formation in stored blood and urine samples. Forensic Sci. Int. 2014;243:144–148. doi: 10.1016/j.forsciint.2014.07.019. [DOI] [PubMed] [Google Scholar]
- 156.Kalasinsky K.S, Dixon M.M, Schmunk G.A, Kish S.J. Blood, brain, and hair GHB concentrations following fatal ingestion. J. Forensic Sci. 2001;46(3):728–730. [PubMed] [Google Scholar]
- 157.Chin R.L, Sporer K.A, Cullison B, Dyer J.E, Wu T.D. Clinical course of gamma-hydroxybutyrate overdose. Ann. Emerg. Med. 1998;31(6):716–722. doi: 10.1016/S0196-0644(98)70230-6. [DOI] [PubMed] [Google Scholar]
- 158.Miró O, Nogué S, Espinosa G, To-Figueras J, Sánchez M. Trends in illicit drug emergencies: the emerging role of gamma-hydroxybutyrate. J. Toxicol. Clin. Toxicol. 2002;40(2):129–135. doi: 10.1081/CLT-120004400. [DOI] [PubMed] [Google Scholar]
- 159.Couper F.J, Thatcher J.E, Logan B.K. Suspected GHB overdoses in the emergency department. J. Anal. Toxicol. 2004;28(6):481–484. doi: 10.1093/jat/28.6.481. [DOI] [PubMed] [Google Scholar]
- 160.Van Sassenbroeck D.K, De Neve N, De Paepe P, Belpaire F.M, Verstraete A.G, Calle P.A, Buylaert W.A. Abrupt awakening phenomenon associated with gamma-hydroxybutyrate use: a case series. Clin. Toxicol. (Phila.) 2007;45(5):533–538. doi: 10.1080/15563650701365818. [DOI] [PubMed] [Google Scholar]
- 161.Degenhardt L, Darke S, Dillon P. GHB use among Australians: characteristics, use patterns and associated harm. Drug Alcohol Depend. 2002;67(1):89–94. doi: 10.1016/S0376-8716(02)00017-0. [DOI] [PubMed] [Google Scholar]
- 162.Ortmann L.A, Jaeger M.W, James L.P, Schexnayder S.M. Coma in a 20-month-old child from an ingestion of a toy containing 1,4-butanediol, a precursor of gamma-hydroxybutyrate. Pediatr. Emerg. Care. 2009;25(11):758–760. doi: 10.1097/PEC.0b013e3181bec93b. [DOI] [PubMed] [Google Scholar]
- 163.Gunja N, Doyle E, Carpenter K, Chan O.T, Gilmore S, Browne G, Graudins A. Gamma-hydroxybutyrate poisoning from toy beads. Med. J. Aust. 2008;188(1):54–55. doi: 10.5694/j.1326-5377.2008.tb01508.x. [DOI] [PubMed] [Google Scholar]
- 164.Li J, Stokes S.A, Woeckener A. A tale of novel intoxication: a review of the effects of gamma-hydroxybutyric acid with recommendations for management. Ann. Emerg. Med. 1998;31(6):729–736. doi: 10.1016/S0196-0644(98)70232-X. [DOI] [PubMed] [Google Scholar]
- 165.Caldicott DG, Kuhn M. Gamma-hydroxybutyrate overdose and physostigmine: Teaching new tricks to an old drug. Ann. Emerg. Med. 2001;37 (1):99–102. doi: 10.1067/mem.2001.111642. [DOI] [PubMed] [Google Scholar]
- 166.Yates S.W, Viera A.J. Physostigmine in the treatment of gamma-hydroxybutyric acid overdose. Mayo Clin. Proc. 2000;75(4):401–402. doi: 10.4065/75.4.401. [DOI] [PubMed] [Google Scholar]
- 167.Zvosec D.L, Smith S.W, Litonjua R, Westfal R.E. Physostigmine for gamma-hydroxybutyrate coma: inefficacy, adverse events, and review. Clin. Toxicol. (Phila.) 2007;45(3):261–265. doi: 10.1080/15563650601072159. [DOI] [PubMed] [Google Scholar]
- 168.Devoto P, Colombo G, Cappai F, Gessa G.L. Naloxone antagonizes ethanol- but not gamma-hydroxybutyrate-induced sleep in mice. Eur. J. Pharmacol. 1994;252(3):321–324. doi: 10.1016/0014-2999(94)90179-1. [DOI] [PubMed] [Google Scholar]
- 169.Lee D.C, Satz W.A, Dougherty T, Greene T. An investigation of flumazenil to antagonize gamma-hydroxybutyrate intoxication in a murine model. J. Med. Toxicol. 2006;2(2):68–70. doi: 10.1007/BF03161174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 170.Carai M.A, Colombo G, Gessa G.L. Resuscitative effect of a gamma-aminobutyric acid B receptor antagonist on gamma-hydroxybutyric acid mortality in mice. Ann. Emerg. Med. 2005;45(6):614–619. doi: 10.1016/j.annemergmed.2004.12.013. [DOI] [PubMed] [Google Scholar]
- 171.Mcdaniel CH, Miotto KA. Gamma hydroxybutyrate (GHB) and gamma butyrolactone (GBL) withdrawal: Five case studies. J. Psychoactive Drugs. 2001;33 (2):143–9. doi: 10.1080/02791072.2001.10400479. [DOI] [PubMed] [Google Scholar]
- 172.Goodwin AK, Gibson KM, Weerts EM. Physical dependence on gamma-hydroxybutrate (GHB) prodrug 1 4-butanediol (1 4-BD) Time course and severity of withdrawal in baboons. Drug Alcohol Depend. 2013;132 (3):427–33. doi: 10.1016/j.drugalcdep.2013.02.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 173.Galloway G.P, Frederick S.L, Staggers F.E, Jr, Gonzales M, Stalcup S.A, Smith D.E. Gamma-hydroxybutyrate: an emerging drug of abuse that causes physical dependence. Addiction. 1997;92(1):89–96. doi: 10.1111/j.1360-0443.1997.tb03640.x. [DOI] [PubMed] [Google Scholar]
- 174.Ghio L, Cervetti A, Respino M, Belvederi Murri M, Amore M. Management and treatment of gamma butyrolactone withdrawal syndrome: a case report and review. J. Psychiatr. Pract. 2014;20(4):294–300. doi: 10.1097/01.pra.0000452567.84825.07. [DOI] [PubMed] [Google Scholar]
- 175.Wojtowicz J.M, Yarema M.C, Wax P.M. Withdrawal from gamma-hydroxybutyrate, 1,4-butanediol and gamma-butyrolactone: a case report and systematic review. CJEM. 2008;10(1):69–74. doi: 10.1017/s1481803500010034. [DOI] [PubMed] [Google Scholar]
- 176.Schneir A.B, Ly B.T, Clark R.F. A case of withdrawal from the GHB precursors gamma-butyrolactone and 1,4-butanediol. J. Emerg. Med. 2001;21(1):31–33. doi: 10.1016/S0736-4679(01)00324-9. [DOI] [PubMed] [Google Scholar]
- 177.Chew G, Fernando A., III Epileptic seizure in GHB withdrawal. Australas. Psychiatry. 2004;12(4):410–411. doi: 10.1080/j.1440-1665.2004.02142.x. [DOI] [PubMed] [Google Scholar]
- 178.Rosenberg M.H, Deerfield L.J, Baruch E.M. Two cases of severe gamma-hydroxybutyrate withdrawal delirium on a psychiatric unit: recommendations for management. Am. J. Drug Alcohol Abuse. 2003;29(2):487–496. doi: 10.1081/ADA-120020529. [DOI] [PubMed] [Google Scholar]
- 179.Dyer J.E, Roth B, Hyma B.A. Gamma-hydroxybutyrate withdrawal syndrome. Ann. Emerg. Med. 2001;37(2):147–153. doi: 10.1067/mem.2001.112985. [DOI] [PubMed] [Google Scholar]
- 180.McDonough M, Kennedy N, Glasper A, Bearn J. Clinical features and management of gamma-hydroxybutyrate (GHB) withdrawal: a review. Drug Alcohol Depend. 2004;75(1):3–9. doi: 10.1016/j.drugalcdep.2004.01.012. [DOI] [PubMed] [Google Scholar]
- 181. Bennett WR, Wilson LG, Roy-Byrne PP. Gamma-hydroxybutyric acid (GHB) withdrawal: A case report. J. Psychoactive Drugs. 2007;39 (3):293–6. doi: 10.1080/02791072.2007.10400616. [DOI] [PubMed] [Google Scholar]
- 182.Perez E, Chu J, Bania T. Seven days of gamma-hydroxybutyrate (GHB) use produces severe withdrawal. Ann. Emerg. Med. 2006;48 (2):219–20. doi: 10.1016/j.annemergmed.2006.03.040. [DOI] [PubMed] [Google Scholar]
- 183.Quang L.S, Colombo G, Lobina C, Maccioni P, Orru A, Gessa G.L, Maher T.J, Carai M.A. Evaluation for the withdrawal syndrome from gamma-hydroxybutyric acid (GHB), gamma-butyrolactone (GBL), and 1,4-butanediol (1,4-BD) in different rat lines. Ann. N. Y. Acad. Sci. 2006;1074:545–558. doi: 10.1196/annals.1369.055. [DOI] [PubMed] [Google Scholar]
- 184.Sivilotti M.L, Burns M.J, Aaron C.K, Greenberg M.J. Pentobarbital for severe gamma-butyrolactone withdrawal. 2001. [DOI] [PubMed]
- 185.Bosman I.J, Lusthof K.J. Forensic cases involving the use of GHB in The Netherlands. Forensic Sci. Int. 2003;133(1-2):17–21. doi: 10.1016/S0379-0738(03)00044-6. [DOI] [PubMed] [Google Scholar]
- 186.Du Mont J, Macdonald S, Rotbard N, Bainbridge D, Asllani E, Smith N, Cohen MM. Drug-facilitated sexual assault in Ontario, Canada: Toxicological and DNA findings. J. Forensic Leg Med. 2010;17 (6):333–8. doi: 10.1016/j.jflm.2010.05.004. [DOI] [PubMed] [Google Scholar]
- 187.Németh Z, Kun B, Demetrovics Z. The involvement of gamma-hydroxybutyrate in reported sexual assaults: a systematic review. J. Psychopharmacol. 2010;24(9):1281–1287. doi: 10.1177/0269881110363315. [DOI] [PubMed] [Google Scholar]
- 188.Porter W.H. Ethylene glycol poisoning: quintessential clinical toxicology; analytical conundrum. Clin. Chim. Acta. 2012;413(3-4):365–377. doi: 10.1016/j.cca.2011.10.034. [DOI] [PubMed] [Google Scholar]
- 189.Mégarbane B, Fompeydie D, Garnier R, Baud F.J. Treatment of a 1,4-butanediol poisoning with fomepizole. J. Toxicol. Clin. Toxicol. 2002;40(1):77–80. doi: 10.1081/CLT-120002888. [DOI] [PubMed] [Google Scholar]
- 190.Caputo F, Bernardi M. Sodium oxybate to treat alcohol dependence: 20 years of clinical experience. Addict. Biol. 2013;18(6):901–903. doi: 10.1111/adb.12113. [DOI] [PubMed] [Google Scholar]
- 191.Caputo F, Vignoli T, Maremmani I, Bernardi M, Zoli G. Gamma hydroxybutyric acid (GHB) for the treatment of alcohol dependence: a review. Int. J. Environ. Res. Public Health. 2009;6(6):1917–1929. doi: 10.3390/ijerph6061917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 192.Belcher J, Nielsen S, Campbell G, Bruno R, Hoban B, Larance B, Lintzeris N, Degenhardt L. Diversion of prescribed opioids by people living with chronic pain: results from an Australian community sample. Drug Alcohol Rev. 2014;33(1):27–32. doi: 10.1111/dar.12084. [DOI] [PubMed] [Google Scholar]
- 193.Wikner B.N, Öhman I, Seldén T, Druid H, Brandt L, Kieler H. Opioid-related mortality and filled prescriptions for buprenorphine and methadone. Drug Alcohol Rev. 2014;33(5):491–498. doi: 10.1111/dar.12143. [DOI] [PubMed] [Google Scholar]
- 194.Ross E.A, Reisfield G.M, Watson M.C, Chronister C.W, Goldberger B.A. Psychoactive “bath salts” intoxication with methylenedioxypyrovalerone. Am. J. Med. 2012;125(9):854–858. doi: 10.1016/j.amjmed.2012.02.019. [DOI] [PubMed] [Google Scholar]
- 195.Wohlfarth A, Weinmann W. Bioanalysis of new designer drugs. Bioanalysis. 2010;2(5):965–979. doi: 10.4155/bio.10.32. [DOI] [PubMed] [Google Scholar]
- 196.Zawilska J.B, Wojcieszak J. Designer cathinones--an emerging class of novel recreational drugs. Forensic Sci. Int. 2013;231(1-3):42–53. doi: 10.1016/j.forsciint.2013.04.015. [DOI] [PubMed] [Google Scholar]
- 197.Zawilska J.B, Wojcieszak J. Spice/K2 drugs--more than innocent substitutes for marijuana. Int. J. Neuropsychopharmacol. 2014;17(3):509–525. doi: 10.1017/S1461145713001247. [DOI] [PubMed] [Google Scholar]
- 198.Craig K, Gomez H.F, McManus J.L, Bania T.C. Severe gamma-hydroxybutyrate withdrawal: a case report and literature review. J. Emerg. Med. 2000;18(1):65–70. doi: 10.1016/S0736-4679(99)00163-8. [DOI] [PubMed] [Google Scholar]
- 199.Chin R.L. A case of severe withdrawal from gamma-hydroxybutyrate. Ann. Emerg. Med. 2001;37(5):551–552. doi: 10.1067/mem.2001.114466. [DOI] [PubMed] [Google Scholar]