

Abstract
Aim:
Aim of this study is to determine the levels of knowledge related with drug administration and drug administration errors of nurses who care for pediatric patients.
Material and Methods:
The study data were obtained from the nurses who were working in the departments of pediatrics in two education and research hospitals in the province of İstanbul and who accepted to participate in the study. The questionnaire form of the study was established by the investigators in accordance with the experiences and literature information. A total of 31 questions related with drug preparation, calculation and administration together with the general working properties of the individual were filled out by face to face interview. The data were evaluated using percent and chi-square tests. The study was initiated after ethics committee approval was obtained from Şişli Hamidiye Etfal Education and Research Hospital (365/2013).
Results:
The study was conducted with 98 nurses who accepted the questionnaire. The education levels of the participants were as follows: undergraduate (48%), high school (32.7%), associate degree (12.2%), master’s degree (6.1%) and postgraduate (1%). It was found that 88.8% of the participants worked in a patient-centered fashion and 11.2% worked in a work-centered fashion. The frequency of interruption/distraction during preparation of treatment was found to be 92.9%. It was found that the frequency of checking by two people during preparation or administration of high risk drugs was 64.3% and the conditions under which drugs should be kept were found to known correctly with a rate of 76.5%. It was found that undergraduate healthcare workers were more successful in converting units (p= 0.000). It was found that powder weight of drugs was considered with a rate of 85.7% in calculation.
Conclusions:
Conclusively, it was found that nurses who worked in pediatric wards did not receive a standard education in terms of drug administration and preparation. It was found that undergraduate nurses were more successful in calculating doses, the process of drug preparation was interrupted with a rate of >90% and the rate of checking by two people was low.
Keywords: Pediatric nursing, drug errors, drug administrations
Introduction
The most commonly observed error in the hospital setting is related with medication administration (1). Medication administration error is defined as any preventable event which occurs in the time period which starts with supply of a medication and includes the follow-up period after administration (2). The risk is higher in drug administrations in the childhood age group compared to adults. Many factors including reconstitution, preservation and interaction with other fluids in addition to inappropriate commercial format of the drugs which will be used in the childhood age group predispose to errors.
Nurses constitute the most important element in noticing and preventing the errors in order to decrease the risks in the process of administration of drugs to children (3). In our country, nurses are responsible for preparation and administration of drugs after the order is given in all therapeutical institutions (4). Since nurses are responsible of having information about drugs, drug preparation, checking drugs, administration of drugs and assessment of therapy, they should be continuously educated throughout their career (5).
In our study which was planned as a descriptive study, it was aimed to determine the level of knowledge related with drug administration and drug administration errors and to assess the relation of the data obtained with the demographic properties.
Material and Methods
The study was conducted in a cross-sectional and descriptive fashion in two education and research hospitals in the province of İstanbul between April 2013 and May 2013. A total of 98 nurses who were on duty on the days when the data were collected and who accepted to participate in the study were included in the study. The study was inititated after approval was obtained from the ethics committee of Şişli Etfal Training and Research Hospital (365/2013).
In collection of the data, a questionnaire form developed in the light of expert opinions and the information related with the subject in the literature was used by the investigators (two specialist nurses and two specialist physicians). The identity information of the participants were not included in the questionnaire. Interviews were conducted with the ones who accepted the questionnaire voluntarily. The questionnaire form prepared by the investigators was composed of a total of 31 questions 7 of which were related with the demographic properties of the individual, 6 of which were related with the work division, 8 of which were related with the level of kowledge of drug preparation, calculation and administration and 10 of which were related with medication administration errors and its prevention. The data obtained as a result of face to face interview performed by the investigators with the nurse who accepted the study were recorded.
Study group
The nurses who worked in the Department of Pediatric Emergency, Pediatric and Neonatology clinics and Pediatric Surgery clinics which served the pediatric patient group were included in the study.
Definitions
Duty-centered work:
This explains the study system performed by providing work distribution between nurses by specifying the duties to be performed in a clinic (fluid preparation, administration of antibiotics, patient care, etc.).
Patient-centered work:
This explains the study system in which the patients inside a clinic are distributed to nurses during the work period and all duties (fluid preparation, administration of antibiotics, patient care, etc.) related with these patients are performed only by the nurse who is responsible.
Statistical analysis
The data obtained were assessed using Statistical Package for the Social Sciences (SPSS) 11.5 program. The descriptive statistics of the general properties and findings were given as percentages. In comparison of the data, chi-square test and Fisher’s exact test were used for non-variable measurements and a p value of <0,05 was considered statistically significant.
Results
The study was conducted with 98 nurses who accepted the questionnaire. The flowchart of the study is given in Figure 1. Six of the participants (6.1%) were male. The distribution of the education status was as follows: undergraduate 48%, high-school 32.5%, associated degree 12.2%, graduate degree 6.1% and postgraduate 1%. The distribution of the work divisions was as follows: Neonatology clinic 44.9%, Department of Pediatric Emergency 26.5%, Pediatric clinic 18.4% and Pediatric surgery clinic 10.2%. The distribution of the total time of work of the participants in the career and in pediatric clinics is presented in Table 1.
Figure 1.
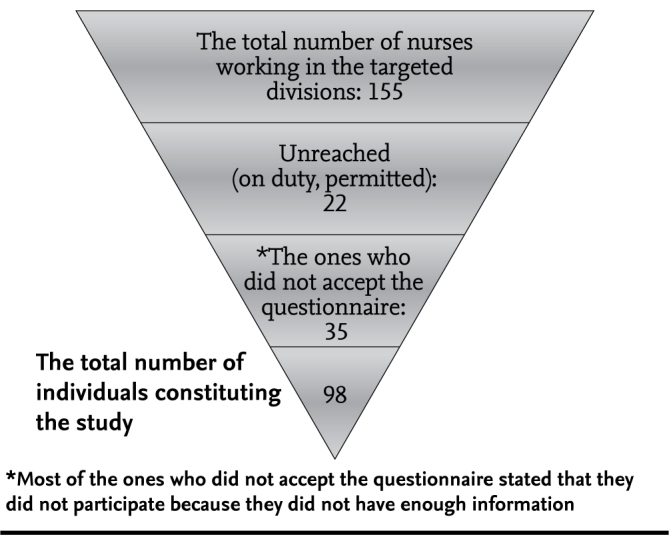
The flowchart of the participants
Table 1.
The distribution of the participants by the total working time in the career and pediatric clinics
| Working time | Total working time n % | Working time in pediatric clinics n % |
|---|---|---|
| <2 years | 32 (32.7) | 46 (46.9) |
| 2–5 years | 24 (24.5) | 25 (25.5) |
| 5–10 years | 25 (25.5) | 22 (22.5) |
| >10 years | 17 (17.3) | 5 (5.1) |
When the infrastructure related with the work divisions of the participants was examined, it was found that 53.1% of the clinic wards had no treatment preparation room, while a washbasin was present in all clinic wards with a treatment room. It was found that 88.8% of the participants worked in a patient-centered fashion and 11.2% worked in a duty-centered fashion and a calculator was not used with a rate of 22.24%. A response of “yes” was given to the question of “does interruption/distraction in the stage of treatment preparation occur during preparation of treatment?” with a rate of 92.9%. It was found that the rate of checking by two individuals while preparing or administering high-risk drugs was 64.3% and the conditions of appropriate storage for drugs were known with a rate of 76.5%. No relation was found between cheking by two individuals and the total working time and the working time in pediatric wards (p=0.255 and p=0.923, respectively).
While all participants knew the order of weight measurements and conversion of 1 gram to milligrams in calculation of doses, an error rate of 13.3% was found in conversion of milligram to microgram. It was found that undergraduates were more successful in converting units (p=0.000). The relation of the education level of the nurses and knowledge and attitudes in drug administration is presented in Table 2.
Table 2.
The relation between the education levels of the nurses and their knowledge and attitutes related with drug administration
| Education level | ||||||
|---|---|---|---|---|---|---|
| High-school | Associate degree | Undergraduate | Postgraduate | Total | p | |
| Number of nurses, n (%) | 32 (32.7) | 12 (12.2) | 47 (48) | 7 (7.1) | 98 (100) | |
| Using calculator in calculating doses, n (%) | 23 (71.8) | 10 (83.3) | 38 (80.8) | 5 (71.4) | 76 (77.6) | 0.740 |
| Interrupting in the stage of treatment preparation, n (%) | 30 (93.7) | 11 (91.6) | 43 (91.4) | 7 (100) | 91 (92.9) | 1.000 |
| Checking by two individuals in preparation of high risk drugs, n (%) | 20 (62.5) | 10 (83.3) | 30 (63.8) | 3 (42.8) | 63 (64.3) | 0.356 |
| Knowing the rules of drug storage, n (%) | 23 (71.8) | 11 (91.6) | 34 (72.3) | 7 (100) | 75 (76.5) | 0.264 |
| Able to convert drug dose units to each other, n (%) | 25 (78.1) | 8 (66.6) | 47 (100) | 5 (71.4) | 85 (86.7) | 0.000 |
| Able to calculate doses after drugs are reconstituted, n (%) | 29 (90.6) | 10 (83.3) | 38 (80.8) | 7 (100) | 84 (85.7) | 0.533 |
| Knowing the relation between drug administration routes and drug incompatibilities, n (%) | 18 (56.2) | 8 (66.6) | 31 (65.9) | 6 (85.7) | 63 (64.3) | 0.542 |
| Reporting the physician in case of administration of inappropriate dose, n (%) | 28 (87.5) | 12 (100) | 40 (85.1) | 7 (100) | 87 (89) | 0.572 |
| Knowing the drug prescription errors on the card of treatment, n (%) | 18 (56.2) | 5 (41.6) | 30 (63.8) | 6 (85.7) | 59 (60.2) | 0.266 |
It was found that the definition of intravenous drug concentration was known correctly with a rate of 49% and use of the powder weight in calculation was known with a rate of 85.7%. Our question related with the conditions where drug incompatibility might be present was answered correctly with a rate of 64.3% and the questions related with drug incompatibility prevention methods were answered correctly with a rate of 68.4%. It was found that the question related with preparation of an oral drug which is commonly used in pediatric patients and which should be reconstituted was answered correctly with a rate of 79.6%. The methods used by the participants as assistive sources in drug administration are presented in Figure 2. 89% of the nurses were reported to stop infusion and reported the issue to the physician when an error was found at the time of prescription or administration of drugs. It was found that the conditions which would lead to error related with doses of administration on the medication chart were known with a rate of 60.2% in the open-ended question included in the questionnaire. It was found that the time of working in pediatric clinics and total working times of the nurse did not have an impact on the level of knowledge of erroneous conditions related with administration doses (p=0.722 and p=0.670, respectively). The relation of the total working times and the working times in the pediatric wards and the information and attitutes related with drug administration is presented in Table 3. The open-ended question “what are the administration errors observed in the last one year?” was answered as set portion calculation error (47.9%), drug concentration (30.6%) and dose error (29.5%).
Figure 2.

The rates of usage of assistive codes in drug administrations
Table 3.
The relation of the total working times and working times in pediatric clinics of the nurses with the knowledge and attituted related with drug administration
| Time (years) | Total working time | The working time in pediatric clinics | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
||||||||||
| <2 | 2–5 | 5–10 | >10 | p | <2 | 2–5 | 5–10 | >10 | p | Total n (%) | |
| Number of nurses, n (%) | 32 (32.7) | 24 (24.5) | 25 (25.5) | 17 (17.3) | 46 (46.9) | 25 (25.5) | 22 (22.5) | 5 (5.1) | 98 (100) | ||
| Using calculator in calculating doses, n (%) | 24 (75) | 20 (83.3) | 19 (76) | 13 (76.5) | 0.677 | 32 (69.5) | 21 (84) | 18 (81.8) | 5 (100) | 0.363 | 66 (77.6) |
| Interrupting in the stage of treatment preparation, n (%) | 29 (90.6) | 21 (87.5) | 25 (100) | 16 (94.1) | 0.348 | 41 (89.1) | 23 (92) | 22 (100) | 5 (100) | 0.451 | 91 (92.9) |
| Checking by two individuals in preparation of high risk drugs, n (%) | 21 (65.6) | 19 (79.1) | 14 (56) | 9 (52.9) | 0.255 | 30 (65.2) | 17 (68) | 13 (59.1) | 3 (60) | 0.923 | 63 (64.3) |
| Knowing the rules of drug storage, n (%) | 23 (71.8) | 18 (75) | 20 (80) | 14 (82.3) | 0.708 | 31 (67.3) | 21 (84) | 19 (86.4) | 4 (80) | 0.275 | 75 (76.5) |
| Able to convert drug dose units to each other, n (%) | 26 (81.2) | 21 (87.5) | 23 (92) | 15 (88.2) | 0.411 | 38 (82.6) | 22 (88) | 20 (90.9) | 5 (100) | 0.815 | 85 (86.7) |
| Able to calculate doses after drugs are reconstituted, n (%) | 26 (81.2) | 22 (91.6) | 23 (92) | 13 (76.5) | 0.184 | 38 (82.6) | 22 (88) | 20 (90.9) | 4 (80) | 0.735 | 84 (85.7) |
| Knowing the relation between drug administration routes and drug incompatibilities, n (%) | 21 (65.6) | 10 (41.7) | 19 (76) | 13 (76.5) | 0.031 | 29 (63.1) | 13 (52) | 17 (77.3) | 4 (80) | 0.307 | 63 (64.3) |
| Reporting the physician in case of administration of inappropriate dose, n (%) | 29 (90.6) | 19 (79.1) | 23 (92) | 16 (94.1) | 0.300 | 39 (84.7) | 22 (88) | 21 (95.5) | 5 (100) | 0.610 | 87 (89) |
| Knowing the drug prescription errors on the card of treatment, n (%) | 22 (68.7) | 13 (54.1) | 13 (52) | 11 (64.7) | 0.670 | 29 (63.1) | 14 (56) | 14 (63.6) | 2 (40) | 0.722 | 59 (60.2) |
Discussion
It has been reported that 20% of medication administration errors which occur in hospitals are drug administration errors, 39% of drug administration errors occur at the time of prescription and order, 38% occur at the time of drug administration, 12% occur at the time of drug preparation and 11% occur at the time of recording (6). The most common errors in drug administrations include administration of wrong doses, missing a dose and wrong administration speed (7–9). It has been reported that drug administration errors have a significant place among medical errors which increase health expenditure and lead to morbidity and mortality (10).
There are no sufficient data related with drug administration errors in children. The frequency of drug administration errors is higher in pediatric patients compared to adults (11). The harming potential of drug errors is higher in children compared to adults. The most important factor which increases the possibility of error related with drugs in children includes the fact that the doses of drugs are calculated differently according to the age, gestational age, body weight and surface area of the child (3). The facts that the same drug has differenet doses, most pediatric drugs are awailable in fluid or adult forms increase the risk of error (3). In administration of drugs, the role of the nurse is not only administering drugs as prescribed. The nurse should have information about the drug given, administer the drugs in a correct and safe way, observe and interprete the response of the patient to the drug and educate the patient about the drug (12).
It has been reported that the causes of occurence of drug errors primarily include distraction of the interest of the nurse during drug administration and interruption of the work (13). The other causes include insufficient number of nurses and lack of cheking the drug for two times (13). In our study, it was found that treatments were interrupted because of different causes in the drug preparation and administration period in a significant portion of the participants (92.9%) and the frequency of checking the drug for two times was 64.3%. Therefore, it was concluded that the potential of drug administration error was high in the present study group.
The powder volume is the difference between the amount of fluid added to a vial to reconstitute a drug and the final amount of fluid. If the dry powder volume is not considered in children, the drug dose prepared may be lower than the ordered dose and lead to dosing error. To prevent dosing errors the nurse should keep the dry powder volume in mind in administration of vial drugs. It has been reported that the dry powder weight is not calculated with a rate of 86.7% in our country (14). In our study which included only the nurses who cared for children, the rate of calculating dry powder weight was found to be 85.7%. This supports the view that pediatric nurses are more sensitive in calculating powder volume.
The American Society of Health-System Pharmacists (ASHP) reported that drug administration errors included neglect, giving overdose, erroneous preparation of drugs, administration of a wrong dose, administration of a wrong or defected drug, administration of drugs by a wrong route and with a wrong speed (15). In a study conducted with these criteria, the most common error in antibiotic administration in our country was reported to be dosing error (40%) (4). In a study including nursing students, the rate of drug administration error was reported to be 14.3% and a wrong dose was administered with a rate of 4% (16). In our study, the most common errors were found to include lack of calculation of set portion and errors related with drug concentrations and dosage similar to the other studies reported.
Studies have reported that the units and abbreviations used by physicians while writing drugs on the card of treatment predispose to drug administration errors (3). Abbreviations including D5 (5% dextrose), IU (unit), μg (microgram) and using comma in unnecessary places mathematically (5 or 1.0) increase the risk of occurence of errors. In our study, it was found that this was known with a rate of 60%.
Conclusively, it was found that the nurses working in pediatric divisions did not receive a regular training in relation with drug administration and preparation. It was found that undergraduates were more successful in dose calculations, the treatment preparation process was interrupted with a rate of above 90%, the rate of checking by two individuals was low and the most common error was lack of calculation of the set portion. In the childhood age group, administration of drugs at accurate doses and at appropriate times is vital. In planning of treatment, the highest level of education should be targeted for nurses. Specification of the present status in planning in-service training will be directive for future adjustments.
Footnotes
Ethics Committee Approval: Ethics committee approval was received for this study from the ethics committee of Şişli Etfal Training and Research Hospital.
Informed Consent: The patient consent was not considered necessary because of the study was made with health professionals.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - A.B., A.K.; Design - A.B., A.K.; Supervision - M.S., Ş.S.; Funding - A.K., M.S.; Materials - A.K., M.S.; Data Collection and/or Processing -A.B., M.S., Ş.S.; Analysis and/or Interpretation - A.B., S.U., A.N.; Literature Review - A.K., M.S., Ş.S.; Writer - A.B., A.K., M.S.; Critical Review - A.B., A.N., S.U.; Other - A.K., M.S., Ş.S.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
References
- 1.Kohn LT, Corrigan JM, Donaldson MS, editors. To err ıs human: Bulding a safer health system. Washington: DC: National Academy Press; 2000. pp. 1–48. [PubMed] [Google Scholar]
- 2.American Academy of Pediatrics (AAP) Prevention of medication errors in the pediatric inpatient setting. Pediatrics. 2003;112:431–6. doi: 10.1542/peds.112.2.431. http://dx.doi.org/10.1542/peds.112.2.431. [DOI] [PubMed] [Google Scholar]
- 3.Kılıçarslan Törüner E, Erdemir F. Pediatrik hastalarda ilaç uygulama hatalarının önlenmesi. Sağlık Bilimleri Fakültesi Hemşirelik Dergisi. 2010;17:63–71. [Google Scholar]
- 4.Alparslan Ö, Erdemir F. Pediatri servislerinde kullanılan antibiyotiklerin sulandırılması, saklanamaması ve hastaya verilmesi konusunda hemşirelerin bilgi ve uygulamalarının belirlenmesi. C.Ü. Hemşirelik Yüksekokulu Dergisi. 1997;1:41–52. [Google Scholar]
- 5.Kuğuoğlu S, Çövener Ç, Kürtüncü Tanır M, Aktaş E. İlaç uygulamalarında hemşirenin mesleki ve yasal sorumluluğu. Maltepe üniversitesi Hemşirelik Bilim ve Sanat Dergisi. 2009;2:86–93. [Google Scholar]
- 6.Leape LL. Error in medicine. JAMA. 1994;272:1851–7. http://dx.doi.org/10.1001/jama.272.23.1851. [PubMed] [Google Scholar]
- 7.Tang FI, Sheu SJ, Yu S, Wei IL, Chen CH. Nurses relate the contributing factors involved in medication errors. J Clin Nurs. 2007;16:447–57. doi: 10.1111/j.1365-2702.2005.01540.x. http://dx.doi.org/10.1111/j.1365-2702.2005.01540.x. [DOI] [PubMed] [Google Scholar]
- 8.Frey B, Buettiker EV, Hug EM, Waldvogel K, Gessler EP, Ghelfi ED. Does critical encident reporting contribute to medication error prevention. Eur J Pediatr. 2002;161:594–9. doi: 10.1007/s00431-002-1055-0. http://dx.doi.org/10.1007/s00431-002-1055-0. [DOI] [PubMed] [Google Scholar]
- 9.Otero P, Leyton A, Mariani G, Ceriani J. Medication errors in pediatric inpatients: prevalence and results of a prevention program. pediatrics. 2008;22:737–43. doi: 10.1542/peds.2008-0014. http://dx.doi.org/10.1542/peds.2008-0014. [DOI] [PubMed] [Google Scholar]
- 10.Özkan S, Kocaman G, Ozturk C. Pediatrik ilaç uygulama hatalarının sıklığı, tipleri, nedenleri ve önleme girişimleri: literatür incelemesi. Dokuz Eylül Üniversitesi Hemşirelik Yüksekokulu Elektronik Dergisi. 2008;1:51–65. [Google Scholar]
- 11.Ferranti J, Horvath M, Cozart H, Whitehurst J, Eckstrand J. Reevaluating the safety profile of pediatrics: A comparison of computerized adverse drug even surveillance and voluntary reporting in the pediatric environment. Pediatrics. 2008;121:1201–7. doi: 10.1542/peds.2007-2609. http://dx.doi.org/10.1542/peds.2007-2609. [DOI] [PubMed] [Google Scholar]
- 12.Aştı T, Acaroğlu R. Hemşirelikte sık karşılaşılan hatalı uygulamalar. Cumhuriyet Üniversitesi Hemşirelik Yüksekokulu Dergisi. 2000;4:22–6. [Google Scholar]
- 13.Stratton KM, Blegen MA, Pepper G, Vaughn T. Reporting of medication errors by pediatric nurses. J Ped Nur. 2004;19:385–92. doi: 10.1016/j.pedn.2004.11.007. http://dx.doi.org/10.1016/j.pedn.2004.11.007. [DOI] [PubMed] [Google Scholar]
- 14.Savaşer S, Çimen S, Yıldız S. Flakon şeklinde antibiyotiklerde kuru toz hacminin uygulana- cak doz üzerine etkisi. İÜFN Hem Derg. 2008;16:7–15. [Google Scholar]
- 15.Raja Lope RJ, Boo NY, Rohana J, Cheah FC. A quality assurance study on the administration of medication by nurses in a neonatal intensive care unit. Singapore Med J. 2009;50:68–72. [PubMed] [Google Scholar]
- 16.Ayık G, Altuğ Özsoy S, Çetinkaya A. Hemşirelik öğrencileri-nin ilaç uygulama hataları. İÜFN Hem Derg. 2010;18:136–43. [Google Scholar]