

Abstract
The digastric muscle is composed by two muscle bellies: an anterior and a posterior, joined by an intermediate tendon. This muscle is situated in the anterior region of the neck. The region between the hyoid bone and the mandible is divided by an anterior belly into two triangles: the submandibular situated laterally and the submental triangle which is located medially. We found that the anatomical variations described in the literature relate mainly to the anterior belly and consist of differences in shape and attachment of the muscle. During routine dissection in February 2013 in the section hall of the Department of Anatomy and Histology in Medical University – Sofia we came across a very interesting variation of the digastric muscle. The digastric muscles that presented anatomical variations were photographed using a Sony Cyber-shot DSC-T1 camera, with a Carl Zeiss Vario-Tessar lens. We found out bilateral variation of the digastric muscle in one cadaver. The anterior bellies were very thin and insert to the hyoid bone. Two anterior bellies connect each other and thus they formed a loop. The anatomical variations observed of our study related only to the anterior belly, as previously described by other authors. It is very important to consider the occurrence of the above mentioned variations in the digastric muscle when surgical procedures are performed on the anterior region of the neck.
Keywords: neck muscles, variations, digastric muscle, hyoid bone
Introduction
The digastric muscle belongs to the group of suprahyoid muscles. It is formed by two bellies: an anterior and a posterior belly. The groups of suprahyoid muscles include four muscles: the digastric, the geniohyoid, stylohyoid and mylohyoid. These muscles insert to the hyoid bone. The bellies of the digastric are joined together by an intermediate tendon that passes through a fibrous sling that is attached to the body of the hyoid bone [6]. These muscle groups anchor the hyoid bone against the traction of the infrahyoid muscles[6]. The anterior belly of the digastric muscle inserts to the digastric fossa, in the lower interior of the mandible. The posterior belly originates in the mastoid notch, on the medial side of the mastoid process of the temporal bone. Two bellies of the digastric muscle are inserted in the body of the hyoid bone by means of a tendon. It is important to mention that when the mandible is fixed, the digastric muscle raises the hyoid bone, while when the hyoid is fixed, the digastric muscle opens the mouth by lowering the mandible [3]. The bellies of the digastric muscle are the borders of the submandibular, submental and carotid triangles. The submandibular (digastric) triangle is limited by the anterior and posterior bellies of the digastric muscle and by the inferior margin of the mandible. A few structuresare situated in this triangle. They are the submandibular gland, submandibular lymph nodes, hypoglossal nerve, facial vein, nerves and vessels for the mylohyoid muscle and the carotid sheath, which contains the external and internal carotid arteries, internal jugular vein and vagus nerve. The submental triangle is limited by the anterior belly of the digastric muscle, the hyoid bone and the anterior median line. The submental lymph nodes and the anterior jugular vein are located in the submental triangle. The carotid triangle is limited by and the superior belly of the omohyoid muscle, the posterior belly of the digastric muscle, and by the anterior margin of the sternocleidomastoid muscle. This triangle contains the carotid sheath, with the common carotid artery, branches of the external carotid artery, the internal jugular vein and its tributaries, the deep cervical lymph nodes and the vagus, accessory and hypoglossal nerves [3, 10, 11].
The embryonal development of the anterior belly of the digastric muscle begins in the fourth week of pregnancy, other hand originates from the second pharyngeal arch [7].
The anterior belly of the digastric muscle is innervated by the trigeminal nerve (fifth cranial pair), while the posterior belly is innervated by the facial nerve (seventhcranial pair) [3].
In the literature there have been data of anatomical variations in the digastric muscle ever since 1847, as pointed out by Bergman et al [2]. In 1905 Testut [12] pointed some variations in the anterior belly, with the presence of a supernumerary fascicle inserted in the raphe of the mylohyoid muscle, or in the hyoid bone or the digastric fossa of the opposite side. This variation was frequently unilateral and constituted a “trigastric” muscle. Other variations were described in accordance with the classifications of Zlabek [15], which took into account their phylogenetic and ontogenetic development, and the classifications of Yamada [14], which enumerated six different types of variations in the anterior belly: atavistic type, origin type, insertion type, mixed type, complex type and defect type. All these types may also be subdivided into other groups. Fujimura et al. [4] proposed that the classification of anatomical variations in the anterior belly of the digastric muscle should be based on the position of the attachments of the bellies of the muscle.
Materials and Methods
The material for this study was collected in the period 2010 – 2013. This work is a collaboration between the Department of Anatomy and Histology, the Department of Endocrine Surgery, the Department of Forensic Medicine and Deontology from Sofia’s Medical University, and the Department of General Surgery, State Hospital, Biala Slatina city, Bulgaria.
Digastric muscles of human material (of 80 cadavers and patients aged 21 to 82 years, 40 males and 40 females) were used for this morphological study. Experiments were conducted in strict compliance with the ethical principles for handling human and cadaveric material applied at the Medical University of Sofia and the legislative requirements for the protection of human rights.
Varieties in sublingual muscles were not found, except in one cadaver, in which we came across the described variety.
Fixation of cadaveric materials in the dissecting room used for training for students and graduates of each medical university in the European Union is very specific and is regulated by the state law.
All legislative requirements to protect human rights have been observed as well.
During a routine dissection in February 2013 in the section hall of the Department of Anatomy and Histology, we came across a very interesting variation of the digastric muscle.
After extraction of the skin from the neck, digastrics muscles were carefully analyzed from the some variation.
The digastric muscles that presented anatomical variations were photographed using a Sony Cyber-shot DSC-T1 camera with a Carl Zeiss Vario-Tessar lens.
Results and discussion
During routine dissection in the Department of Anatomy and Histology of the Medical University – Sofia, establish a very rare variation.
As seen on the Figures 1, 2, 3, and 4, the anterior belly of the digastric muscle originates from the original mesoderm of the first pharyngeal arch. The deficiency in the differentiation of this layer on one side may be responsible for unilateral variations, whereas deficiencies on both sides may be responsible for bilateral variations [7]. In our case the variation of the digastric muscle was bilateral. Thus we came to the conclusion that the deficiency in the differentiation of the first pharyngeal arch was bilateral. This does not correspond to the literature data according to which the unilateral variations are more frequent [9,8]. In some cases unilateral anatomical variations may be responsible for the asymmetry in the anterior region of the neck or even in the movement of the floor of the mouth [8] or the temporomandibular joint [1]. Thus they may present greater clinical importance because this may lead to an imbalance in the movement of the larynx. However, more recentl investigations [5] showed a balance between unilateral and bilateral variations. According to this study the percentage of unilateral and bilateral variations of the digastric muscle is equalized. It is important to note that the unilateral type of asymmetry may be able to be considered in clinical examinations and in imaging examinations like ultrasound, tomography and magnetic resonance, with lymph nodes, benign cervical masses like thyroglossal cysts, or neoplasia [13].
Figure 1.
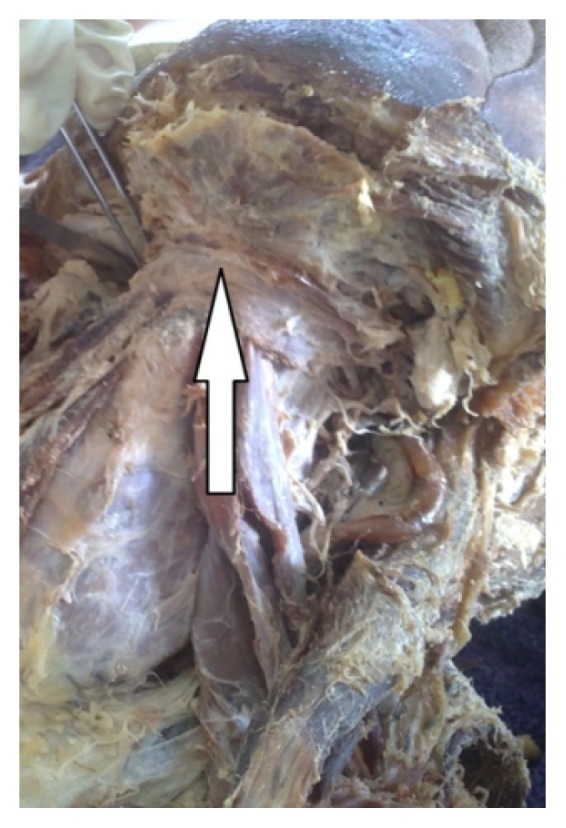
Digastric muscle with bilateral variation. The anterior bellies (caught with tweezers) are very thin and insert to the hyoid bone.
Figure 2.
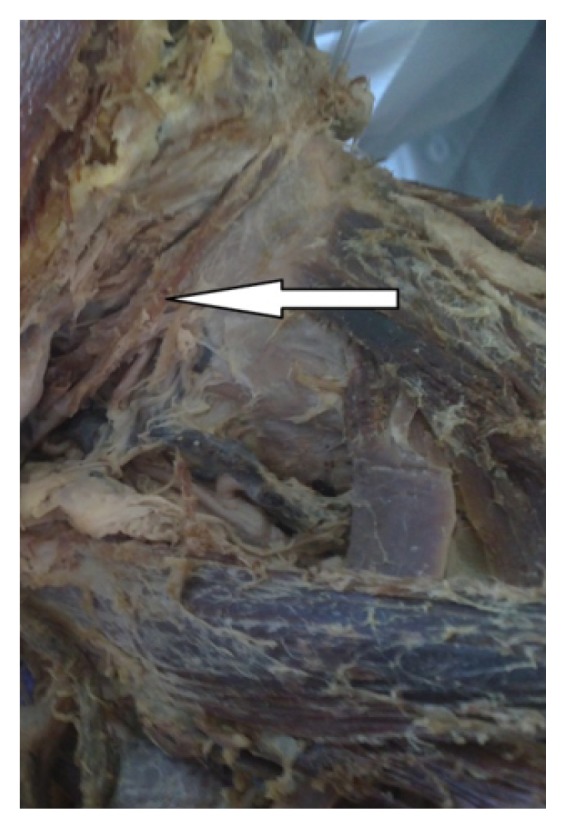
The intermediate tendon of the digastric muscle is covered by the stylohyoid muscle.
Figure 3.

Mylohyoid muscle is prepared bilateral. It is obviously the absence of the anterior belly of digastric muscle under the mylohyoid. Instead two anterior bellies of digastric are caught to
Figure 4.
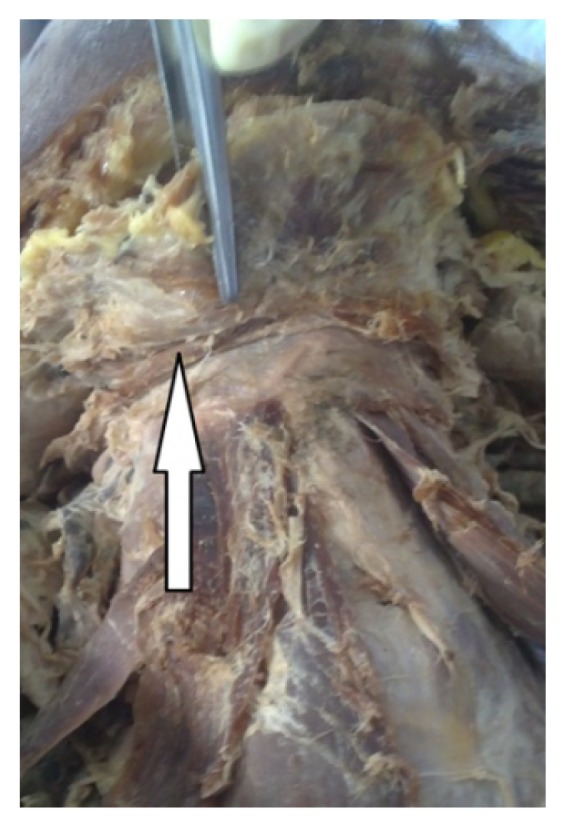
The anterior bellies of the right and the left digastric muscles insert to the hyoid bone, connect each other and thus way form a loop.
In conclusion, it is important that our case refers only to the variation of the anterior belly. Other studies in literature also refer mainly to the anterior belly of the digastric. During some surgical procedures in the anterior region of the neck especially in the submandibular and submental triangles it is important to consider the presence of variations in the digastric muscle. For example when performing submandibulectomy the digastric muscle and its tendon serve for anatomical orientation.
References
- 1.Andreo JC, Navarro JAC, Toledo Filho JL. Anatomical study on the variations of the anterior belly of the digastric uscle. Rev Chil Anat. 1997;15(1):111–114. [Google Scholar]
- 2.Bergman RA, Afifi AK, Miyauchi R. Digastricus. Illustrated Encyclopedia of Human Anatomic Variation. Opus I: Muscular system. 2002. Available from: http://www.anatomyatlases.org.
- 3.Drake RL, Vogl W, Mitchell AWM. Cabeça e pescoço. In: Drake RL, Vogl W, Mitchell AWM, editors. Gray’s Anatomia para estudantes. 1ª ed. Rio de Janeiro: Elsevier; 2005. pp. 905–907. [Google Scholar]
- 4.Fujimura A, Onodera M, Feng X, et al. Abnormal anterior belly of the digastric muscle: A proposal for the classification of abnormalities. Anat Science Inter. 2003;78:185–188. doi: 10.1046/j.0022-7722.2003.00049.x. [DOI] [PubMed] [Google Scholar]
- 5.Liquidato BM, Barros MD, Alves AL, Pereira CSB. Anatomical study of the digastric muscle: Variations in the anterior belly. Int J Morphol. 2007;25(4):797–800. [Google Scholar]
- 6.Lockhart RD, Hamilton GF, Fyfe FW. Músculos. In: Lockhart RD, Hamilton GF, Fyfe FW, editors. Anatomia do corpo humano. 2ª ed. Rio de Janeiro: Guanabara Koogan; 1983. pp. 156–157. [Google Scholar]
- 7.Moore KL, Persaud TVN. Aparelho Faríngeo. In: Moore KL, Persaud TVN, editors. Embriologia clínica. 7ª ed. Rio de Janeiro: Editora Elsevier; 2004. pp. 226–235. [Google Scholar]
- 8.Peker T, Turgut HB, Anil A. Bilateral anomaly bellies of digastric muscle. Surg Radiol Anat. 2000;22:119–121. doi: 10.1007/s00276-000-0119-y. [DOI] [PubMed] [Google Scholar]
- 9.Sargon MF, Celik HH. An abnormal digastric muscle with three bellies. Surg Radiol Anat. 1994;16:215–216. doi: 10.1007/BF01627599. [DOI] [PubMed] [Google Scholar]
- 10.Snell RS. A cabeça e o pescoço. In: Snell RS, editor. Anatomia clínica para estudantes de Medicina. 5ª ed. Rio de Janeiro: Guanabara Koogan; 1999. pp. 611–617. [Google Scholar]
- 11.Sociedade Brasileira de Anatomia. Terminologia Anatômica Internacional. 1ª ed. São Paulo: Manole; 2001. Terminologia Anatômica; pp. 3–4. [Google Scholar]
- 12.Testut L. Traité D’Anatomie Humaine. Paris: Octave Doin; 1905. pp. 752–755. [Google Scholar]
- 13.Turan-Ozdemir S, Oygucu IH, Kafa IM. Bilateral abnormal anterior bellies of digastric muscles. Anat Science Int. 2004;79:95–97. doi: 10.1111/j.1447-073x.2004.00065.x. [DOI] [PubMed] [Google Scholar]
- 14.Yamada S. Beobachfunger über der Venter anterior des Musculus digastricus mandibulae bei japanisher Erwachsenen und Foeter. Acta Anat Nippon. 1935;8:303–347. [Google Scholar]
- 15.Zlabek K. Contribution a la connaissance des anomalies du ventre anterieur du digastrique de l’Homme. Arch Anat Histol Embryol. 1933;16:357–406. [Google Scholar]