

Abstract
Background and aims
Despite the great effectiveness of antibiotics, no principle is more important in the care of open fractures than aggressive irrigation and debridement. Fixation of open fractures has a number of beneficial effects, including even the reduction of the risk of infection.
Materials and Methods
This prospective study of the treatment of 116 open fractures of the lower limb offered us the possibility to determine the ways to prevent the infection. All the patients were studied prospectively and the type of treatment and the rate of infection were evaluated.
Results
In the course of the treatment, 96 wounds were closed by primary closure (82.8%) and 2 wounds were closed by secondary closure on the 5th postoperative day (1.7%). There were 14 skin grafts (12.1%), 2 muscle flap closures (1.7%) and 2 healings by granulation (1.7%). The antibiotics used were ceftriaxone + gentamycin for type I, II fractures; metronidazole was added for type III fractures. The duration of the antibiotic therapy was 7–10 days, according to the severity of the fracture. The infection rate was 0% for type I, 0% for type II and 5.17% for type III fractures (6/116).
Conclusions
The treatment of open fractures by intensive debridement of the wound and immediate fixation, as well as by primary closure of the wound with prolonged use of antibiotics, led to a dramatic decrease of the rate of infections.
Keywords: open fracture, infection, primary closure of the skin, antibiotics
Introduction
One hundred and fifty years ago, mortality was common following open fractures [1,2]. Along with the advances in modern therapy however, the expected outcome has improved significantly.
Antibiotics have been considered as standard therapy since 1947. Patzakis et al reported their seminal randomized, controlled trial of cephalothin, a first generation cephalosporin for the management of open fractures [3]. In the past, cultures were routinely done before and after debridement of open fractures. Recent studies show that cultures of the wound specimen often fail to identify the organisms that subsequently cause the infection [4,5]. In fact, there is evidence that most infections at the site of open fractures are caused by nosocomial bacteria [6].
Despite the great effectiveness of antibiotics, no principle is more important in the care of open fractures than aggressive irrigation and debridement. Penetration of antibiotics into the necrotic tissue is still under investigation. Theories range from decreased penetration secondary to an interruption in the blood supply to an increased penetration related to local inflammatory mediators [7,8].
Fixation of open fractures has a number of beneficial effects, including protection of soft tissues from additional injury by fracture fragments, improvement of wound care and tissue healing, promotion of mobilization and rehabilitation and possibly even the reduction of the risk of infection [9].
In the multiply injured patient fractures, fixation also reduces the risk of acute respiratory distress by claiming the systemic inflammatory response [3].
Materials and Methods
Between January 2007 and January 2010, 108 patients with open fractures of the lower limb were admitted and treated in Alsafwa Hospital in Taiz - Yemen. All the patients were studied prospectively to evaluate the type of treatment and the rate of infection.
The average age of the patients was 28.11 years, in a range of 6–65 years; 98 patients were males (90.7%) and 10 patients were females (9.3%); 36 patients had open fractures of the femur shaft (33.3%), 70 patients had tibia fractures (64.8%) and 2 patients had open calcaneal fractures with Achilles tendon rupture (1.9%). Regarding the cause of the fracture, 40 patients had suffered car accidents (37%), 20 had fallen from a height (18.3%), 14 had suffered motorcycle accidents (12%), 4 had suffered industrial injuries (3.7%), 14 had suffered motorcycle collisions against pedestrians (13%), 2 patients had been struck by stones (1.9%) and 14 had suffered gun shots (13%).
The open fractures were classified according to the Gustilo-Anderson classification of open fractures – of the 116 open fractures in 108 patients, 20 open fractures were type I (17.2%), 32 were type II (27.6%), 20 were type IIIA (17.2%), 30 fractures were type IIIB (17.2%) and 14 fractures were type IIIC (12.1%).
The average time of fracture healing was 9.44 months, with a range of 3–18 months, standard deviation 3.2.
Ninety-six wounds were closed by primary closure (82.8%) and 2 wounds were closed by secondary closure, on the 5th postoperative day (1.7%). There were 14 skin grafts (12.1%), 2 muscle flaps (1.7%) and 2 healings by granulation (1.7%).
Time of debridement of the wound: 84 open fractures before 6 hours (72.4%) and 32 open fractures after 6 hours (27.6%), depending on the time of arrival of the patients to the hospital.
All the fractures were thoroughly irrigated and debrided in the operating room with the protocol from table I.
Table I.
Irrigation volume of the wound in terms of wound classification.
| Gustilo-Anderson Classification | Irrigation volume/additives |
|---|---|
| I | 3L Normal saline with liquid soap additive |
| II | 6L Normal saline with liquid soap additive |
| III A,B,C | 9L Normal saline with liquid soap additive Local antibiotics for highly contaminated wounds, gentamycin in irrigation solution |
The antibiotics we used were ceftriaxone + gentamycin for type I and type II fractures, and intra-venous metronidazole added for type III fractures. The duration of antibiotic administration was for 7 to 10 days, according to the severity of the wound.
Prophylaxis against tetanus was also administered.
After resuscitation, irrigation and debridement, if the wound could be converted to a clean wound and if no soft tissue procedure was needed, immediate fixation of the fracture and primary closure of the wound was performed. If soft tissue procedure (skin graft or flap) was needed, a delayed closure of the wound (within 3–5 days) was performed. In rare cases (2 patients), the wounds were left to heal by secondary intention (granulation).
Out of 36 open femoral shaft fractures, 12 fractures were fixed by plates and screws (33.3%), 12 fractures were fixed with reamed intramedullary nails (33.3%) and 2 fractures with unreamed nails (5.6%), 8 fractures were fixed with external fixators (22.2%) and 2 cases of open fractures of femur medial condyle were fixed with 2 cancellous screws.
As regards open leg fractures, 42 were open fractures of tibia shaft. From these, 20 fractures were fixed by plates and screws (47.6%), 6 fractures were fixed with POP casts (14.2%), 2 fractures were fixed with unreamed intramedullary nails (4.8%) and 14 fractures were fixed with external fixators (33.3%).
Out of 36 open fractures of the tibia and fibula, 2 fractures were fixed with plates (5.61%), 6 fractures were fixed with unreamed intramedullary nails (16.7%) and 28 fractures were fixed with external fixators (77.8%).
As regards foot fractures, we had two open calcaneum fractures of type IIIB according to Gustilo classification, with Achilles tendon rupture. Each fracture was fixed with two k-wires.
Results
Ninety-six wounds were closed by primary closure (81.8%) (Table II). They included 36 wounds of open femoral shaft fractures (type I, II, IIIA, IIIB, IIIC), 58 wounds of open tibial shaft fractures (type I, II, IIIA, IIIB, IIIC) (fig. 1 and 2) and 2 open calcaneal fractures of type III. The wounds of primary closure were healed within 2 weeks.
Table II.
Methods of wound closure used in our cases.
| Frequency | Percentage | |
|---|---|---|
| Primary | 96 | 82.8 |
| Secondary | 2 | 1.7 |
| Skin graft | 14 | 12.1 |
| Granulation | 2 | 1.7 |
| Flap | 2 | 1.7 |
| Total | 116 | 100 |
Figure 1A.

Open fracture of the tibia, type II.
Figure 2A.

Open fracture of the tibia, type IIIB.
Two wounds of tibial shaft fracture of type II were healed by secondary wound closure within 3–5 days postoperatively (1.7%).
Two wounds of tibial shaft of type II were healed by granulation (1.7%), 14 wounds needed skin graft (12.1%) and 2 needed flap wound closure.
Infection
Six fractures had infections – four pin tract infections (3.44%) and two deep infections (1.7%), but neither of them progressed to osteomyelitis.
Discussion
The rate of infection of open fractures is associated with the fracture characteristics, antibiotics therapy and host parameters [10,11]. The infection risks differ by the type of fracture and they have been reported to be ranging from 0 to 2% for type I fractures, from 2 to 10% for type II fractures and from 10 to 50% for type III fractures [12,13].
More recent studies have shown that the rate of clinical infection increased to 1.4% (7/497) for type I fractures, 3.5% (25/695) for type II fractures and to 22.7% (45/198) for type III fractures [10].
In our series, the rate of infection was 0% for type I fractures, 0% for type II fractures and 5.17% for type III fractures (6/116). The prevalence of infection associated with open fractures of the tibia has been reported to be 10–20 times greater than that associated with other skeletal injury. This coincides with our results, 66.6% of infections occurred in open fractures of the tibia (2 pin infections of the external fixtor in femoral open fracture and 4 infections in tibial open fractures, from which 2 pin infections and 2 deep infections).
Historically, the closure of open fracture wounds was delayed in order to prevent infection with clostridium and other contaminating organisms. While this strategy remains the generally accepted approach in settings characterized by substantial contamination (such as barnyard and battle field), many surgeons have begun to consider earlier closure of open fractures wounds that have been adequately debrided. Recently, a number of authors have investigated the feasibility of primary closure. In a study of 119 open fractures, De Long et al. did not find immediate closure (within twenty-four hours) to be associated with a higher rate of infection or non-union as compared with delayed closure (after more than 24 hours) [15]. In a double blind prospective study, Benson et al. [16] assessed the benefit of delaying primary closure of the wound associated with open fractures. Eighty-two fractures were divided into groups of primary closure (44 wounds) and delayed closure (38 wounds), on average 5 days after injury. Only 3 superficial wound infections were reported, having occurred in the primary closure wounds. Finally, Hertel et al. [17] performed a retrospective study of 29 open tibial fractures of type IIIA and type IIIB and found that immediate coverage was associated with a lower rate of infection: 0% (zero of 14), as compared with 27% (4 of 15) after late coverage.
These results were similar to our results, where 96 open fractures wounds were closed primarily after thorough debridement. The infection rate was 0% in type I, 0% in type II, 2.08% in type IIIA (2 pin infection/96 cases), 0% in type IIIB, 0% in type IIIC. In the delayed closure of the wound (20 cases) the infection rate was 0% in type I, II and IIIA, and 2.08% in each type IIIB and IIIC.
We believe that our results support the performance of primary closure of the wound of open fractures, where adequate debridement can be applied. The low rate of infection in our results may be due to the thorough debridement, the early closure of the wound and to the long duration of antibiotic therapy.
While there is ample evidence supporting the administration of antibiotics in open fractures, there is however a lack of evidence indicating an optimal regimen – whereas some authors recommend the treatment of all open fractures with a combination of a first generation cephalosporin for type I and type II fractures [3], most agree that penicillin or ampicyllin should be added when there is a high risk of anaerobic infection. The optimal duration of antibiotic administration is less clear. Many authors recommend an initial three-day course supplemented by an additional three-day course at the time of any subsequent procedures [18].
In our series we used ceftriaxone + gentamycin for type I and type II fractures and intravenous metronidazole added for type III fractures; the duration of antibiotic administration was from seven to ten days, according to the severity of the fracture.
Conclusion
The treatment of open fractures by intensive debridement of the wound and immediate fixation, as well as by primary closure of the wound with prolonged use of antibiotics, seven to ten days, led to a dramatic decrease of the rate of infections.
Figure 1B.

Open fracture of the tibia, type II, with fixation with unreamad intramedullary nail and primary closure.
Figure 1C.
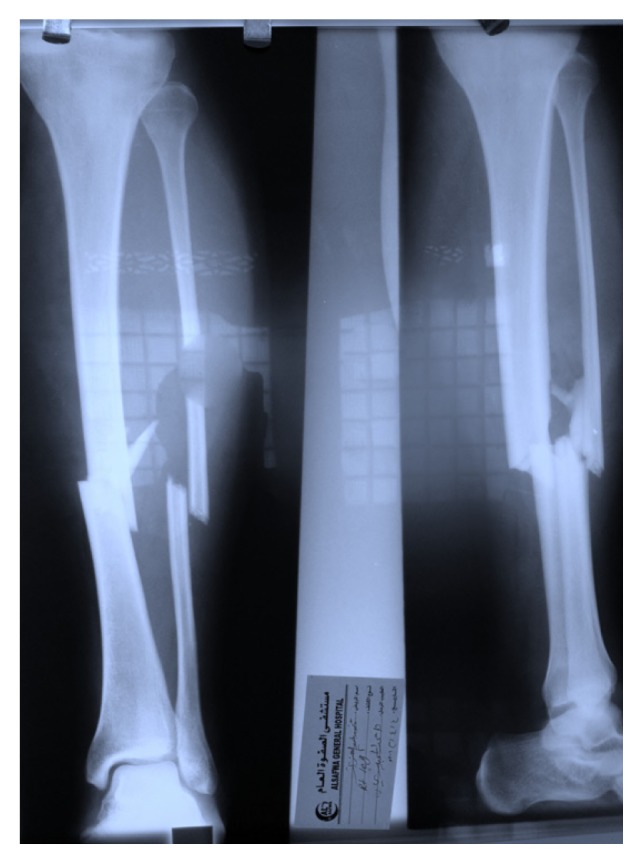
X-rays of the open fracture of the tibia.
Figure 1D.

Open fracture of the tibia, type II, with primary closure and fixation with unreamad intramedullary nail, X-rays after bone union.
Figure 2B.

Open fracture of the tibia, type IIIB, with fixation with external fixator and primary closure of the skin.
References
- 1.Lister J. On a new method at treating compound fractures, abscess, etc. The Lancet. 1867;1:326, 357, 387, 507. [Google Scholar]
- 2.Patrick JH, Smelt GJ. Surgical progress- 100years ago. An assessment of Listerism at St. Thomas’s Hospital, London. Ann R Coll Surg Engl. 1977;59:456–462. [PMC free article] [PubMed] [Google Scholar]
- 3.Patzakis MJ, Harvey JP, Jr, Ivler D. The role of antibiotics in the management of open fracture. J Bone Joint Surg (Am) 1974;56:532–541. [PubMed] [Google Scholar]
- 4.Patzakin MJ, Bains RS, Lee J, et al. Prospective randomized, double blind study comparing single agent antibiotics therapy, ciprofloxacine, to combination antibiotics therapy in open fracture wounds. J Orthop Trauma. 2000;14:529–533. doi: 10.1097/00005131-200011000-00002. [DOI] [PubMed] [Google Scholar]
- 5.Fischer MD, Gustilo RB, Varecka TF. The timing of flap coverage, bone grafting, and intramedullary nailing in patients who have a fracture of the tibial shaft with extensive soft tissue injury. J Bone Joint Surg (Am) 1991;73:1316–1322. [PubMed] [Google Scholar]
- 6.Carsenti-Etesse H, Doyon F, et al. Epidemiology of bacterial infection during management of open leg fractures. Eur J Clin Microbio Infect Dis. 1999;18:315–323. doi: 10.1007/pl00015012. [DOI] [PubMed] [Google Scholar]
- 7.Nix DE, Goodwin SD, et al. Antibiotic tissue penetration and its relevance: impact of tissue penetration on infection response. Antimicrobial agents chemother. 1991;35:1953–1959. doi: 10.1128/aac.35.10.1953. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gross A, Cutright DE, et al. Effectiveness of pulsating water jet lavage in the treatment of contaminated crushed wounds. Am Surg. 1972;124:373–377. doi: 10.1016/0002-9610(72)90044-x. [DOI] [PubMed] [Google Scholar]
- 9.Worlock P, Slack R, et al. The prevention of infection in open fractures, an experimental study of the effect of fracture stability. Injury. 1994;25:1–8. doi: 10.1016/0020-1383(94)90181-3. [DOI] [PubMed] [Google Scholar]
- 10.Patzakis MJ, Wilkins J. Factors influencing infection rate in open fracture wounds. Clin Orthop Relat Res. 1989;243:6–40. [PubMed] [Google Scholar]
- 11.Bewen TR, Widmaier JC. Host classification predicts infection after open fracture. Clin Orthop Relat Res. 2005;433:205–211. doi: 10.1097/01.blo.0000150345.51508.74. [DOI] [PubMed] [Google Scholar]
- 12.Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty five open fracture of long bones, retrospective and prospective analysis. J Bone Joint Surg (Am) 1976;58-A:453–458. [PubMed] [Google Scholar]
- 13.Gustilo RB, Gruninger RP, Davis T. Classification of type III (severe) open fracture relative to treatment and results. Orthopedics. 1987;10:1781–1788. [PubMed] [Google Scholar]
- 14.Patzakis MJ, Wilkins J, Moor TM. The consideration in reducing the infection rate in open tibial fractures. Clin Orthop Relat Res. 1983;178:36–41. [PubMed] [Google Scholar]
- 15.De Long WG, Jr, Born CT, et al. Aggressive treatment of 119 open fracture wounds. J Trauma. 1999;46:1049–1054. doi: 10.1097/00005373-199906000-00012. [DOI] [PubMed] [Google Scholar]
- 16.Benson DR, Riggins RS, et al. Treatment of open fractures: A prospective study. J Trauma. 1983;23:25–30. doi: 10.1097/00005373-198301000-00005. [DOI] [PubMed] [Google Scholar]
- 17.Hartel R, Lambert SM, et al. On the timing of soft tissue reconstruction for open fractures of the lower leg. Arch Orthop Trauma Surg. 1999;119:7–12. doi: 10.1007/s004020050346. [DOI] [PubMed] [Google Scholar]
- 18.Zalavras CG, Petzakis MJ, et al. Management of open fractures. Infect Dis Clin North Am. 2005;19:915–929. doi: 10.1016/j.idc.2005.08.001. [DOI] [PubMed] [Google Scholar]