

Abstract
Purpose
This study was designed to estimate the value of a second transurethral resection of bladder tumor (TURBT) procedure in patients with initially diagnosed T1 high-grade bladder cancer.
Materials and Methods
Between August 2009 and January 2013, a total of 29 patients with T1 high-grade bladder cancer prospectively underwent a second TURBT procedure. Evaluation included the presence of previously undetected residual tumor, changes to histopathological staging or grading, and tumor location. Recurrence-free and progression-free survival curves were generated to compare the prognosis between the groups with and without residual lesions by use of the Kaplan-Meier method.
Results
Of 29 patients, 22 patients (75.9%) had residual disease after the second TURBT. Staging was as follows: no tumor, 7 (24.1%); Ta, 5 (17.2%); T1, 6 (20.7%); Tis, 6 (20.7%); Ta+Tis, 1 (3.4%); T1+Tis, 1 (3.4%); and ≥T2, 3 (10.3%). The muscle layer was included in the surgical specimen after the initial TURBT in 24 patients (82.7%). In three patients whose cancer was upstaged to pT2 after the second TURBT, the initial surgical specimen contained the muscle layer. In the group with residual lesions, the 3-year recurrence-free survival and 3-year progression-free survival rates were 50% and 66.9%, respectively, whereas these rates were 68.6% and 68.6%, respectively, in the group without residual lesions. This difference was not statistically significant.
Conclusions
Initial TURBT does not seem to be enough to control T1 high-grade bladder cancer. Therefore, a routine second TURBT procedure should be recommended in patients with T1 high-grade bladder cancer to accomplish adequate tumor resection and to identify patients who may need to undergo prompt cystectomy.
Keywords: Neoplasm invasiveness, Recurrence, Urinary bladder neoplasms
INTRODUCTION
Approximately 75% to 85% of patients with bladder cancer are diagnosed with non-muscle-invasive bladder cancer (NMIBC) and 20% to 30% of NMIBCs invade the lamina propria and are staged as T1 [1]. Transurethral resection of bladder tumor (TURBT) is the cornerstone of diagnosis and the gold standard treatment for patients with NMIBC. However, NMIBC presents a therapeutic challenge because of factors such as the highly malignant potential of the disease itself and the possibility of incomplete tumor resection. If transurethral resection (TUR) is not complete, NMIBC could progress to muscle-invasive disease, or muscleinvasive lesions might be overlooked and the disease course would be aggressive.
Until now, few studies have investigated the efficacy of a second TURBT procedure for patients with T1 high-grade bladder cancer. In our clinic, we prospectively performed a second TURBT procedure for these patients according to recent guidelines [2,3]. We report the results of our analysis of a series of 29 consecutive patients with T1 high-grade bladder cancer who underwent a second TURBT. This review includes the presence and location of previously undetected remnant lesions, changes to the pathological grading or staging, and the rates of recurrence-free and progression-free survival after a second TURBT procedure.
MATERIALS AND METHODS
Between August 2009 and January 2013, a total of 29 patients with initially diagnosed T1 high-grade bladder cancer underwent a second TURBT procedure and were analyzed to report the number of patients with remnant lesions and the pertinency of the initial pathologic evaluation of tissue samples obtained from the first TURBT. The initial operation in all patients was performed by 2 experienced surgeons. The bladder was thoroughly examined with a 30° lens, and the number, location, and size of the bladder tumors were charted on a cystoscopy diagram. TUR of visible tumors was performed extending to the bladder muscle proper, and deep muscle layer specimens were obtained to assess if the bladder cancer invaded into the muscular layer (tumor base).
If the histopathological evaluation revealed a T1 high-grade tumor, a second TURBT procedure was conducted within 3 to 8 weeks following the first operation irrespective of the results of urine cytology. The previously resected sites and the peripheral area around them were resected when performing the second TURBT procedure. When carcinoma in situ was diagnosed after the initial TUR, the erythematous lesion on the bladder mucosa, which was salmon-pink in color, was also resected. Random biopsy was not performed. If no residual tumor was seen or a superficial tumor or Tis was detected, intravesical bacillus Calmette-Guerin treatment was scheduled. If muscle-invasive remnant cancer was found, subsequent radical cystoprostatectomy was planned. Recurrence was defined in this study as development and detection of urothelial carcinoma on the bladder with Ta or T1 stage regardless of grade, and progression was defined as any worsening of T stage during follow-up.
Continuous variables were expressed as either the mean±standard deviation or median. For statistical analysis, we used one-way analysis of variance to evaluate the relationship of remnant malignant lesions with the properties of the primary lesion. Recurrence-free and progression-free survival curves were generated by using the Kaplan-Meier log-rank test. All statistical outcomes were presented as odds ratios and 95% confidence intervals based on a two-sided test using IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA). We regarded p-values <0.05 as statistically significant.
The study was conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments; appropriate ethical review boards approved this retrospective study.
RESULTS
The patients' mean age was 68±10.4 years (range, 48-93 years), and 2 of the 29 patients were women. In the 29 patients with T1 high-grade bladder cancer, 6 patients (20.7%) had a solitary tumor, for which the size was less than 3 cm in diameter, and 23 patients (79.3%) had multiple tumors or a tumor 3 cm or greater than 3 cm in diameter. The clinicopathological properties of the patients after the first TUR are presented in Table 1. Cystoscopy performed 3 to 8 weeks after the first operation revealed that 11 patients (38%) had visible papillary tumors, 2 patients (6.9%) had erythematous lesions without visible tumors, and 16 patients (55%) had no macroscopic abnormalities.
Table 1. Clinicopathological characteristics of the patients after the first TURBT.
| Characteristic | Value |
|---|---|
| Total number of patients | 29 |
| Age (y), mean±SD (range) | 68±10.4 (48-93) |
| Gender | |
| Male | 27 |
| Female | 2 |
| Interval between transurethral resection (d), median (range) | 31 (20-60) |
| Muscular layer presence in initial TURBT specimen | |
| Included | 24 (82.7) |
| Not included | 5 (17.3) |
| Urine cytology result | |
| Malignant cell present | 6 (20.6) |
| Suspicious for malignancy | 7 (24.1) |
| Atypical cell present | 11 (37.9) |
| Negative for malignancy | 5 (17.4) |
| Macroscopic appearance | |
| Solitary | |
| <3 cm | 6 (20.7) |
| ≥3 cm | 7 (24.1) |
| Multifocal | |
| <3 cm | 6 (20.7) |
| ≥3 cm | 7 (24.1) |
| Nonavailable | 3 (10.3) |
| Concomitant Tis | 8 (27.6) |
Values are presented as number (%) unless otherwise indicated.
TURBT, transurethral resection of bladder tumor; SD, standard deviation.
Including the 11 patients with visible papillary tumors and 2 patients with erythematous lesions, remnant cancer was detected pathologically in a total of 22 patients (75.9%). In 18 of these patients, the tumor was detected at the primary lesion, whereas in 2 patients, the tumor was detected at other sites on the bladder or in multiple sites. The remaining 2 patients had residual lesions at both the site of the initial TUR and another site. Of the 22 patients with residual cancer, 3 patients (10.3%) had the disease upstaged to pT2 (the muscle layer was included after initial TURBT in all of these 3 patients), 6 patients (20.7%) had Tis, 1 patient (3.4%) had Tis in conjunction with residual pT1, and 1 patient (3.4%) had Tis in conjunction with pTa. The muscle layer was included in the surgical specimen after initial TURBT in 24 patients (82.7%). Therefore, the second TURBT procedure decidedly resulted in a primary change in the treatment plan for 3 patients. The stage distribution and pathologic results after the second TURBT procedure are shown in Table 2.
Table 2. Distributions of stages as assessed during the operation.
| Characteristic | No. (%) |
|---|---|
| Tumor stagea | |
| No residual tumor | 7 (24.1) / 7 |
| pTa | 5 (17.2) / 4 |
| pT1 | 6 (20.7) / 5 |
| pTis | 6 (20.7) / 4 |
| pTa & pTis | 1 (3.4) / 1 |
| pT1 & pTis | 1 (3.4) / 1 |
| ≥pT2 | 3 (10.3) / 3 |
| Site of tumor recurrence | |
| Original site | 18 (81.8) |
| The other site | 2 (9.1) |
| Both site | 2 (9.1) |
| Urine cytology result | |
| Malignant cell present | 0 (0) |
| Suspicious for malignancy | 5 (17.2) |
| Atypical cell present | 5 (17.2) |
| Negative for malignancy | 19 (65.6) |
| Macroscopic appearance | |
| Solitary | |
| <3 cm | 3 (50.0)b |
| ≥3 cm | 3 (42.8)b |
| Multifocal | |
| <3 cm | 4 (66.7)b |
| ≥3 cm | 6 (85.7)b |
TURBT, transurethral resection of bladder tumor.
a:Total number of specimens/number of muscle-included specimens.
b:No. of cases after 2nd TURBT.
Among 6 patients with solitary tumors less than 3 cm, 5 patients (83.3%) had residual tumors at the second TURBT, and 16 of 20 patients (80%) with tumors that were multifocal or 3 cm or greater in size were found to have remnant lesions. The second TURBT procedure was performed without major complications in all patients with initial T1 high-grade bladder cancer. Minor complications including urethral injury and prolonged bleeding were managed conservatively in 7 patients.
Sixteen of 29 patients (55.2%) remained free of disease during the entire period, whereas 9 of 29 patients (31%) had recurrences at a different time: 4 patients in the first year and 5 patients at 1 to 5 years. Median time to recurrence was 9 months (range, 3-19 months). Recurrences appeared with dominant frequency in the group with residual cancer; 77.8% (7 of 9 patients) with residual cancer experienced recurrence, whereas 22.2% (2 of 9 patients) in the group without residual cancer experienced recurrence. In the residual tumor group, the recurrence-free survival rate at 3 years was 68.6%, whereas the value for the group without residual tumor was 50%. There was no statistically significant difference between the two groups (p=0.500). Analysis of Kaplan-Meier curves for the recurrence-free survival of the two groups showed that most recurrences appeared within 3 years in the 9 patients (Fig. 1A).
Fig. 1. (A) Kaplan-Meier curves of recurrence-free survival (RFS) in patients with residual tumor (green) and without residual tumor (blue) at the second transurethral resection of bladder tumor (TURBT). Three-year RFS was 68.6% and 50%, respectively (p=0.5). (B) Kaplan-Meier curves of progression-free survival (PFS) in patients with residual tumor (green) and without residual tumor (blue) at the second TURBT. Three-year PFS was 66.9% and 68.6%, respectively (p=0.976).
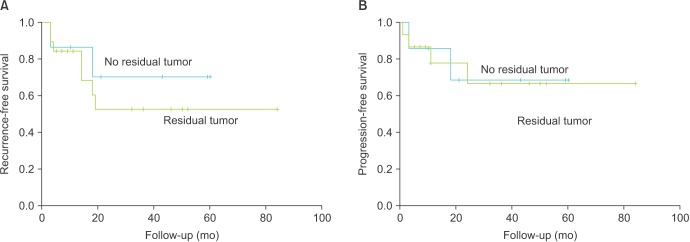
Progression occurred in four patients (8%) within 2 years after injection of Bacillus Calmette-Guerin treatment. Median time to progression was 13.5 months (range, 1-24 months). Four patients progressed from T1 high-grade to pT2 disease and there were multiple metastases in one patient; all of these patients had residual cancer after their initial TURBT. For the residual tumor group, the progression-free survival rate at 3 years was 66.9%, whereas the value for the group without residual tumors was 68.6%. There was no statistical difference between the two groups (p=0.976). Analysis of Kaplan-Meier curves for progression-free survival for the two groups showed that all progressions appeared within 3 years (Fig. 1B). The median period of follow-up was 25 months (interquartile range, 9-43 months).
DISCUSSION
The rate of residual bladder tumors perceived in a second TURBT ranges from 33% to 76% [4]. The risk is higher with high-grade lesions and multiple sites and appears to be elevated with the pathologic stage of the initial lesion. In four studies that respectively assessed Ta and T1 bladder tumors, the presence of residual disease was detected in 27%-72% of Ta and 33%-78% of T1 tumors [4]. That result was confirmed in a clinical trial performed by the Nordic Association of Urology in which about 40% of patients with T1 bladder tumors had remnant disease after an initial resection [3]. Table 3 summarizes the previous studies on a second TURBT procedure for T1 high-grade bladder cancer; the data indicate that the rate of recurrence ranges from 35% to 40% and the rate of progression ranges from 4% to 25% after the second TURBT [5,6,7,8,9,10].
Table 3. Review of published studies on second TURBT for T1 high-grade bladder cancer.
| Source | Year | No. of patients | No. of residual tumors (%) | Recurrence rate (%) | Progression rate (%) |
|---|---|---|---|---|---|
| Herr [6] | 2005 | 36 | 12 (33.3) | Unknown | 25.0 |
| Ali et al. [5] | 2010 | 91 | 37 (40.1) | Unknown | Unknown |
| Yucel et al. [10] | 2010 | 33 | 14 (42.4) | Unknown | 18.2 |
| Katumalla et al. [7] | 2011 | 50 | 18 (36.0) | 35.0 | 4.0 |
| Takaoka et al. [9] | 2013 | 73 | 37 (51.0) | 40.0 | 16.0 |
| Lazica et al. [8] | 2013 | 167 | 97 (58.1) | Unknown | Unknown |
| Current study | 2015 | 29 | 22 (75.9) | 34.5 | 24.1 |
TURBT, transurethral resection of bladder tumor.
To enhance residual tumor detection, a second TURBT performed after 3 to 8 weeks was conducted according to clinical guidelines [4,9,11,12]. The latest version of the European Association of Urology guidelines recommends considering a second TUR if there is concern that the initial resection was incomplete (multiple lesions or large tumors or no muscularis propria in the sample) [11]. Also, a repeat TUR should be recommended when a high-grade, non-muscleinvasive tumor or a T1 tumor is detected in the first TUR [4,9,12].
Some urologists do not routinely perform a second TURBT. The main dispute against a second TURBT is that it requires readmission and repeat anesthesia, thus increasing the risk of morbidity as well as costs [5]. Also, according to existing data, a second TURBT procedure appears to be useless for detecting infiltrative tumors for most cases because they will undergo radical cystectomy [13].
Despite the preceding arguments, the value of a second TURBT procedure is considerable. The remnant tumor, which might be the source of the recurrent lesion, can be resected by a second TURBT. Additionally, the tumor burden will be decreased, and this could reduce the frequency of tumor recurrence and delay early progression. In many cases, the second TURBT might be the only method to reveal the "real" tumor burden, the existence of muscle-invasive lesions, or extensive T1 high-grade tumor, all of which could lead to a change in the eventual treatment strategy. In our analysis, muscularis propria invasion was established at the second TURBT in 10.3% of cases who had a diagnosis of T1 bladder cancer at the initial operation, in accordance with the results of previous trials [14,15,16,17].
Other methods for diagnosis of remnant lesions after an initial operation, such as urine cytology or early flexible cystoscopy, lack the sensitivity to be of important clinical use [18]. In our trial, 30% of patients with no macroscopically visible tumors by endoscopic examination were found to have residual tumor on the second TURBT. This finding supports the evidence that cystoscopy is not sufficient to find remnant lesions.
It was formerly conveyed that the absence of muscle layer in the resected specimen is an implication of clinical understaging [15,19]. Also, undervaluation of the depth of cancer invasion is an important error, especially when a muscle-invasive lesion is present. In a previous study, 14% of patients with stage T1 disease containing muscularis propria in the specimen were upstaged to T2 versus 49% of patients who were upstaged to T2 if no muscular layer existed in the resected tissue [20]. Additionally, Dutta et al. [21] reported a 64% rate of understaging in T1 tumors if muscularis propria was absent in the specimen versus 30% if it was present. In our study, we could not find a definite relationship contingent upon muscle inclusion, which may have been due to that large portion of specimens contain muscular layer after the first TURBT.
Meanwhile, no consensus exists regarding the technique for the repeat resection. However, it is acknowledged that the second TURBT should be performed at the same site as the initial procedure. Additionally, it is indispensable to include the muscularis propria in the resected specimen and to avoid perforation of the bladder wall. By rotating the resection loop, the operator can easily control the tissue depth of resection by using the lateral resecting portion of the conventional right-angle loop electrode [22]. We did not perform random biopsy because we were concerned that random biopsy might result in tumor seeding. It has been reported that random biopsy rarely results in the identification of additional neoplasms and may increase tumor seeding [4,23].
From the point of view of not only urologists but also patients, a second resection is not easy to perform or accept, because no one can know in advance whether residual disease exists in the bladder. However, recent data support the necessity of a second TURBT for bladder cancer, especially T1 high-grade disease, and several guidelines reflect those findings [1,4,6,24]. In the author's experience, explanation about a second TURBT procedure before the initial resection is very helpful for patients' and guardians' decision making. Without the explanation before the first operation, the patients or guardians may be suspicious when they hear that the patient needs another surgery. However, if they are told that a second TURBT is already planned if T1 high-grade disease is diagnosed and that this is totally consistent with state-of-the-art guidelines, they more readily follow the doctor's decision for a second TURBT.
This study had several limitations. The number of subjects was relatively small and the follow-up period was short-term. However, our series was based on patients with T1 high-grade bladder cancer only, for which incidence is known to be very low. A recent study described that 3% to 4% of NMIBC is diagnosed as T1 high-grade bladder cancer [25]. Moreover, the second TURBT procedure was performed prospectively by the same operator in this study. This makes it clear that a second TURBT is necessary, especially for patients with T1 high-grade bladder cancer.
CONCLUSIONS
A large number of patients with T1 high-grade bladder cancer had a higher tumor burden than initially determined on the basis of a single operation. A second TURBT can detect residual cancer and provide accurate pathological information. A second TURBT procedure should be recommended in all cases with T1 high-grade bladder cancer to accomplish adequate tumor resection and to identify patients who may need to undergo prompt radical cystectomy. Three-year recurrence-free survival and progression-free survival rates were not significantly different between the groups with and without residual lesions. In addition, sufficient explanation of the possibility of a second TURBT procedure before the initial TURBT can be helpful for rapport between doctors and patients.
ACKNOWLEDGMENTS
This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIP) (No. 2011-0020128).
Footnotes
CONFLICTS OF INTEREST: The authors have nothing to disclose.
References
- 1.Divrik RT, Sahin AF, Yildirim U, Altok M, Zorlu F. Impact of routine second transurethral resection on the long-term outcome of patients with newly diagnosed pT1 urothelial carcinoma with respect to recurrence, progression rate, and diseasespecific survival: a prospective randomised clinical trial. Eur Urol. 2010;58:185–190. doi: 10.1016/j.eururo.2010.03.007. [DOI] [PubMed] [Google Scholar]
- 2.Babjuk M, Oosterlinck W, Sylvester R, Kaasinen E, Bohle A, Palou-Redorta J, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder. Eur Urol. 2008;54:303–314. doi: 10.1016/j.eururo.2008.04.051. [DOI] [PubMed] [Google Scholar]
- 3.Clark P, Agarwal N, Biagioli M. NCCN clinical practice guidelines in oncology: bladder cancer. Fort Washington (PA): National Comprehensive Cancer Network; 2013. [Google Scholar]
- 4.Babjuk M. Second resection for non-muscle-invasive bladder carcinoma: current role and future perspectives. Eur Urol. 2010;58:191–192. doi: 10.1016/j.eururo.2010.04.019. [DOI] [PubMed] [Google Scholar]
- 5.Ali MH, Ismail IY, Eltobgy A, Gobeish A. Evaluation of second-look transurethral resection in restaging of patients with nonmuscle-invasive bladder cancer. J Endourol. 2010;24:2047–2050. doi: 10.1089/end.2010.0319. [DOI] [PubMed] [Google Scholar]
- 6.Herr HW. Restaging transurethral resection of high risk superficial bladder cancer improves the initial response to bacillus Calmette-Guerin therapy. J Urol. 2005;174:2134–2137. doi: 10.1097/01.ju.0000181799.81119.fc. [DOI] [PubMed] [Google Scholar]
- 7.Katumalla FS, Devasia A, Kumar R, Kumar S, Chacko N, Kekre N. Second transurethral resection in T1G3 bladder tumors - Selectively avoidable? Indian J Urol. 2011;27:176–179. doi: 10.4103/0970-1591.82833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lazica DA, Bottcher S, Degener S, von Rundstedt FC, Brandt AS, Roth S, et al. T1 high-grade bladder cancer - value of second operation with prognostuic parameters of first operation: analysis of 167 cases. Aktuelle Urol. 2013;44:124–128. doi: 10.1055/s-0033-1334962. [DOI] [PubMed] [Google Scholar]
- 9.Takaoka E, Matsui Y, Inoue T, Miyazaki J, Nakashima M, Kimura T, et al. Risk factors for intravesical recurrence in patients with high-grade T1 bladder cancer in the second TUR era. Jpn J Clin Oncol. 2013;43:404–409. doi: 10.1093/jjco/hyt016. [DOI] [PubMed] [Google Scholar]
- 10.Yucel M, Hatipoglu NK, Atakanli C, Yalcinkaya S, Dedekarginoglu G, Saracoglu U, et al. Is repeat transurethral resection effective and necessary in patients with T1 bladder carcinoma? Urol Int. 2010;85:276–280. doi: 10.1159/000316073. [DOI] [PubMed] [Google Scholar]
- 11.Babjuk M, Burger M, Zigeuner R, Shariat SF, van Rhijn BW, Comperat E, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder: update 2013. Eur Urol. 2013;64:639–653. doi: 10.1016/j.eururo.2013.06.003. [DOI] [PubMed] [Google Scholar]
- 12.Han KS, Joung JY, Cho KS, Seo HK, Chung J, Park WS, et al. Results of repeated transurethral resection for a second opinion in patients referred for nonmuscle invasive bladder cancer: the referral cancer center experience and review of the literature. J Endourol. 2008;22:2699–2704. doi: 10.1089/end.2008.0281. [DOI] [PubMed] [Google Scholar]
- 13.Dalbagni G, Herr HW, Reuter VE. Impact of a second transurethral resection on the staging of T1 bladder cancer. Urology. 2002;60:822–824. doi: 10.1016/s0090-4295(02)01920-9. [DOI] [PubMed] [Google Scholar]
- 14.Brauers A, Buettner R, Jakse G. Second resection and prognosis of primary high risk superficial bladder cancer: is cystectomy often too early? J Urol. 2001;165:808–810. [PubMed] [Google Scholar]
- 15.Novara G, Ficarra V. Does routine second transurethral resection affect the long-term outcome of patients with T1 bladder cancer? Why a flawed randomized controlled trial cannot address the issue. Eur Urol. 2010;58:193–194. doi: 10.1016/j.eururo.2010.04.012. [DOI] [PubMed] [Google Scholar]
- 16.Schips L, Augustin H, Zigeuner RE, Galle G, Habermann H, Trummer H, et al. Is repeated transurethral resection justified in patients with newly diagnosed superficial bladder cancer? Urology. 2002;59:220–223. doi: 10.1016/s0090-4295(01)01522-9. [DOI] [PubMed] [Google Scholar]
- 17.Zurkirchen MA, Sulser T, Gaspert A, Hauri D. Second transurethral resection of superficial transitional cell carcinoma of the bladder: a must even for experienced urologists? Urol Int. 2004;72:99–102. doi: 10.1159/000075961. [DOI] [PubMed] [Google Scholar]
- 18.Sivalingam S, Probert JL, Schwaibold H. The role of repeat transurethral resection in the management of high-risk superficial transitional cell bladder cancer. BJU Int. 2005;96:759–762. doi: 10.1111/j.1464-410X.2005.05710.x. [DOI] [PubMed] [Google Scholar]
- 19.Holmang S. High-grade non-muscle-invasive bladder cancer: is re-resection necessary in all patients before intravesical bacillus Calmette-Guérin treatment? Scand J Urol. 2013;47:363–369. doi: 10.3109/21681805.2013.769461. [DOI] [PubMed] [Google Scholar]
- 20.Oosterlinck W, Solsona E, van der Meijden AP, Sylvester R, Bohle A, Rintala E, et al. EAU guidelines on diagnosis and treatment of upper urinary tract transitional cell carcinoma. Eur Urol. 2004;46:147–154. doi: 10.1016/j.eururo.2004.04.011. [DOI] [PubMed] [Google Scholar]
- 21.Dutta SC, Smith JA, Jr, Shappell SB, Coffey CS, Chang SS, Cookson MS. Clinical under staging of high risk nonmuscle invasive urothelial carcinoma treated with radical cystectomy. J Urol. 2001;166:490–493. [PubMed] [Google Scholar]
- 22.Chen WM, Cheng CL, Yang CR, Chung V. Surgical tip to prevent bladder perforation during transurethral resection of bladder tumors. Urology. 2008;72:667–668. doi: 10.1016/j.urology.2008.04.042. [DOI] [PubMed] [Google Scholar]
- 23.Jocham D, Witjes F, Wagner S, Zeylemaker B, van Moorselaar J, Grimm MO, et al. Improved detection and treatment of bladder cancer using hexaminolevulinate imaging: a prospective, phase III multicenter study. J Urol. 2005;174:862–866. doi: 10.1097/01.ju.0000169257.19841.2a. [DOI] [PubMed] [Google Scholar]
- 24.Babjuk M, Oosterlinck W, Sylvester R, Kaasinen E, Bohle A, Palou-Redorta J, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder, the 2011 update. Eur Urol. 2011;59:997–1008. doi: 10.1016/j.eururo.2011.03.017. [DOI] [PubMed] [Google Scholar]
- 25.Kulkarni GS, Hakenberg OW, Gschwend JE, Thalmann G, Kassouf W, Kamat A, et al. An updated critical analysis of the treatment strategy for newly diagnosed high-grade T1 (previously T1G3) bladder cancer. Eur Urol. 2010;57:60–70. doi: 10.1016/j.eururo.2009.08.024. [DOI] [PubMed] [Google Scholar]