

Abstract
Context:
This article aims at demonstrating the effectiveness of day care centers in Indian setting. This is to provide impetus for an innovative approach in psychiatric practice in India.
Aims:
The aim was to narrate the experiences of a day care center being practiced in India.
Settings and Design:
The study provides the experiences gained in a day care center at Lucknow. The center was started in a hired building with a minimum of staff. The cost of the program is around 30,000/months.
Subjects and Methods:
The day care center has been run for nearly 5 years. During this period, 95 clients visited the center and 69 enrolled in the day care. Nearly 35 continued and 34 dropped out due to various reasons.
Statistical Analysis:
Descriptive study.
Results:
There were 49 patients suffering from schizophrenia, 11 from affective disorders, and 9 patients were clubbed in the miscellaneous group. The miscellaneous group consisted of pervasive developmental disorders, slow learners, obsessive compulsive disorders (OCD) and borderline subnormality with psychosis. Most patients had a long duration of illness. The patients of schizophrenia continued in the program more often than other group. Nearly 50% of patients have obtained jobs. The exposure to day care improved the patient's social and occupational behavior. The core symptoms did not change substantially. The families were greatly empowered, and they developed a positive attitude toward illness.
Conclusions:
Of the 59 patients who joined the day care program 35 could continue regularly. Among these patients, nearly 50% could take up jobs. Social and occupational behaviors improved remarkably. The families were empowered, and they developed a positive attitude toward mental illness. Such programs can be improvised with minimal costs and can be value addition in psychiatric practice. We need to develop indigenous know-how for such programs. This is a preliminary communication.
Keywords: Day care centers, India, innovative approach, psychiatric practice
INTRODUCTION
Day care was initially started in USSR in 1930's as a cheaper alternative to hospitalization.[1] The movement spread to Europe in 1950 and reached its peak in 1970 when it provided the main alternative to hospital admission. For some time, it was popular in U.K. and U.S.A but soon lost its relevance as home care was considered more appropriate and cost effective in these countries. The experience of high income and high technical resource countries may not be very relevant to our country with very restricted resource base both in terms of money as well as manpower. Western world is also concerned by two different models of day care:[2] One run by social services and is more attuned to welfare and rehabilitation of chronic mental patients and second more focused on acute illnesses and follows medical model. The latter has been found to produce quicker improvement and better rehabilitation. However, in this country where resource crunch is present, we may even look at the possibility of combining the two for more effective use of the existing resources.
Day care centers in India have generally been used to a limited extent in rehabilitation programs for chronic mental illness. The scarcity of mental health resources, money and trained personnel forces us to try innovative programs which could provide succor to ailing humanity. RFS (India) Lucknow branch started its rehabilitation center in the form of a day care center to help chronic mentally ill to develop skills that may help them to reintegrate in the society.
The experience gained in the last 5 years is the subject matter of this presentation.
Aims
The aim was to narrate the experiences of a day care center being practiced in India that could provide evidence of its affectivity.
SUBJECTS AND METHODS
Description of the day-care center
The center was started in a rented building consisting two bedrooms, two toilets, a kitchen, and living room. The building is located in a posh residential area of Lucknow and is well-connected with roads and public transport.
Staff
We had a counselor who was M.A. in psychology. The counselor was given on job training by senior psychiatrists and trained clinical psychologist. Later, this trained individual resigned, and two new counselors were appointed, both were given training by the same individuals.
The day care in charge at present is one of the parents of our clients who have made a huge impact on the program. He works in an honorary capacity, can communicate with patients and their parents effectively and appreciate their needs.
Cost
The total cost of the program is around Rs.30000/months. We initially started the program as a paid one, but we could not get many clients. We later changed it to a free program since then the membership has picked up.
Program
The patients come to the center by 9.30 a.m. And return to their homes by 4 p.m.
They have a structured day program.
The patients are encouraged to participate in all programs.
The patients bring their own lunch. Tea is provided by the center.
We do have cultural programs for important occasions such as Independence Day, World Mental Health Day, and annual function. Most patients showed remarkable interest in these programs and performed their roles with great interest.
There is a fixed daily routine. The routine varies from day to day. Details of the routine can be obtained from the authors.
Observations
During last 5 years, 95 clients visited the center of which 69 got enrolled.
Of the 69 clients who were enrolled, nearly 34 could not continue.
General characteristics of the patients which continued and dropped out are given in Table 1.
Table 1.
General characteristics of sample
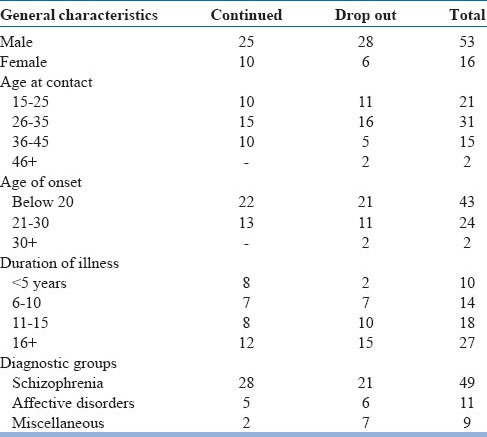
Miscellaneous included pervasive developmental disorder (1), borderline subnormality with psychosis (1), OCD (4), attention deficit hyperactivity disorder with autism (1) and slow learners (2).
Reasons for drop-out
Though there were multiple factors that led to discontinuation. The major factor that was responsible for discontinuation could be obtained in each case. Economic factors were responsible for discontinuation in 30% patients as the families found it difficult to pay for the transport. The second most common reason was lack of response in 24%. This occurred mainly inpatients of OCD, autism, and slow learners. Other factors were; the family left city, patient disruptive, not suitable for day care, and family problems.
Final outcome
Nearly 49% have taken up jobs; 15% resumed studies others were searching jobs. Nearly 23% were continuing to come to the day care center.
General observations
The patients and relatives were generally satisfied with the progress made by the clients during their stay in the day care center. Many parents complained that the patients behave better in the center but revert to abnormal behavior as soon as they return home. The patients in general had improved social behavior, but their basic problems of poverty of thoughts and delusions persisted. The patients could control these symptoms in social situations. Another major advantage was that the relapses were identified promptly by the change in behavior, and these could be improved by modifying the dosage.
Family members were also empowered by their contact with the day care center. They could understand the nature of the disease and the disabilities associated with the disorders. They also took an interest in the welfare of others and thus a cohesive group has been formed which is instrumental in reducing the stigma and development of confidence.
DISCUSSION
The result shows that nearly 50% of patients who enrolled were able to continue in the day care. Most of the patients who joined and continued were benefited. There was hardly any difference between the group that continued and that dropped out. The long duration patients are slightly more in the drop-out group.
Looking at the diagnostic categories, there is no difference in the drop-out rate between affective disorders and schizophrenia. More patients with schizophrenia continued than affective disorders. The miscellaneous group consisting OCD and slow learners did not benefit much. It may be because of inadequate training of staff as well as overwork due to which enough time could not be given to individual patients. The patients with OCD dropped out as they were not benefited.
Studying the reasons of drop-out, it becomes very clear that the majority of patients could be involved in such programs if we had better finances and more staff. Only three patients were considered untreatable. Patients with family problems could be involved if we had more staff.
The purpose of this presentation is to familiarize mental health professional with the concept of day care in Indian setting. The clinical care so far is mainly restricted to acute care and medication for most mentally ill mostly in outpatient department settings. This did not provide social support to the families or skill training which led to a restrictive life for quite a number of patients. What we plan to demonstrate by this presentation is that a large number of patients can be benefited by such non expensive programs which could be started by one or two psychiatrists at their own place.
These centers would provide psychosocial skills to the patients and empowerment to the families.
Depending on the expertise, these day care centers can also help treat conditions such as Dissociative disorders, chronic anxiety states, panic disorders, and OCD.
CONCLUSIONS
Of the 59 patients who joined the day care program, 35 could continue regularly. Among these patients, nearly 50% could take up jobs. Social and occupational behaviors improved remarkably. The families were empowered, and they developed a positive attitude toward mental illness. Such programs can be improvised with minimal costs and can be value addition in psychiatric practice. We need to develop indigenous know-how for such programs. This is a preliminary communication.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Marshall M. Acute psychiatric day hospitals. BMJ. 2003;327:116–7. doi: 10.1136/bmj.327.7407.116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Catty J, Goddard K, Burns T. Social services day care and health services day care in mental health: do they differ? Int J Soc Psychiatry. 2005;51:151–61. doi: 10.1177/0020764005056764. [DOI] [PubMed] [Google Scholar]