

Abstract
We conducted a systematic literature review of the data on HIV testing, engagement in care, and treatment in incarcerated persons, and estimated the care cascade in this group.
We identified 2706 titles in MEDLINE, EBSCO, and Cochrane Library databases for studies indexed to January 13, 2015, and included 92 for analysis. We summarized HIV testing results by type (blinded, opt-out, voluntary); reviewed studies on HIV care engagement, treatment, and virological suppression; and synthesized these results into an HIV care cascade before, during, and after incarceration.
The HIV care cascade following diagnosis increased during incarceration and declined substantially after release, often to levels lower than before incarceration. Incarceration provides an opportunity to address HIV care in hard-to-reach individuals, though new interventions are needed to improve postrelease care continuity.
The 2010 National HIV/AIDS Strategy outlines 3 interdependent goals: (1) reducing HIV incidence, (2) increasing access to care and improving health outcomes for persons living with HIV, and (3) reducing HIV-related disparities and health inequities.1 To meet these goals, it is essential to measure and improve performance at every stage in the HIV care continuum (also known as the HIV treatment cascade) as supported by a 2013 executive order by President Obama2: diagnosis, linkage to care, retention in care, receipt of antiretroviral therapy (ART), and virological suppression.3
Evaluation of this cascade in the general US population according to 2008 data determined that only 80% of HIV-infected individuals were aware of their diagnosis, 62% were linked to care, 41% were retained in routine HIV care, 36% were receiving ART, and 28% had an undetectable viral load.4 Although more recent measures based on surveillance data indicate somewhat higher proportions achieving success in the steps in the cascade,5 significant gaps in the HIV care continuum remain, particularly in vulnerable subgroups. For example, African Americans and younger individuals (aged 25–34 years) are less likely than their counterparts to be aware of their diagnosis, engaged in care, receiving ART, or to have a suppressed viral load.6 These health disparities highlight the need for new approaches to HIV testing, linkage to care, and treatment, especially in hard-to-reach populations.
Because 1 in 7 HIV-infected individuals passes through correctional facilities every year,7 and most inmates come from minority and medically underserved communities, including many people younger than 35 years, jails and prisons are critical settings to address the HIV care continuum and health disparities.8,9 Among African American men aged 18 years or older, 1 in 15 is incarcerated, whereas this statistic is 1 in 36 for Hispanic men and 1 in 106 for White men.9 Incarceration provides a unique opportunity to offer HIV testing, linkage to HIV care, and antiretroviral treatment to individuals who may not be accessing medical services in the community. In addition to affecting individual outcomes by identifying and treating HIV, interventions in the correctional setting have the potential to affect community health by reducing HIV transmission to others through reduction of an HIV patient’s viral load, known as treatment as prevention.10
Although there have been multiple, well-conducted studies of HIV testing, linkage to care, and treatment in incarcerated individuals, there has been less focus on the HIV care continuum as a whole in this group or on how this cascade changes as an individual passes through the correctional system and back to the community. An improved understanding of the course of HIV identification, care, and treatment in this population will allow us to better direct resources to major gaps in the care continuum and to come closer to achieving the goals of the national HIV/AIDS strategy.
Therefore, we sought to perform a systematic literature review to (1) summarize HIV testing, treatment, and linkage to care efforts in the incarcerated and recently released population; (2) determine the estimates in the cascade of care for HIV-infected individuals before, during, and after incarceration; and (3) identify research gaps and targets for future interventions to improve outcomes in the HIV-infected population involved in the criminal justice system.
METHODS
We conducted a literature search with the Ovid MEDLINE database for English-language studies indexed up to January 13, 2015. We used the following medical subject heading (MeSH) terms: “prisoners,” “prisons,” “criminals,” and text words for “incarcerated within 3 words of men, women, male*, female*, patient*, youth, teen*, individual*, person*”; and “exoffender*, ex-offender*, releasee*, jail, criminal justice, correctional facility*, prison*, criminal*, inmate*,” combined with MeSH terms “HIV” (term exploded for comprehensive search), “HIV infections” (exploded), “HIV seroprevalence,” and title words for “HIV, AIDS, human immunodeficiency.” With text words and subject headings or keywords from the original search, on January 13, 2015, we also searched Ovid MEDLINE InProcess, EBSCO Academic Search Complete, the EBSCO Legal Collection, and 3 Cochrane Library databases: Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effect, and Cochrane Central Register of Controlled Trials. We developed all search strings with the assistance of a qualified librarian.
Study Selection
The 2 reviewing authors (P. A. I. and A. E. N.) independently assessed abstracts and titles from all database-generated articles for eligibility on the basis of the following criteria: (1) relevance to HIV and incarceration and (2) specifically addressing outcomes related to HIV testing, linkage to HIV care, retention in HIV care, HIV treatment, and virological suppression in inmates (jail or prison) or recently released individuals. We excluded studies that were not performed in the United States or Canada and limited our evaluation to studies involving adults aged 18 years and older. We excluded additional studies if they had an anonymous author, if they were classified as a nonexperimental study (e.g., opinion, review articles, non–peer-reviewed articles, case reports, legal cases), or if the study did not provide original quantitative data.
We reviewed full-text articles for all studies meeting these criteria. For 7 articles, only an abstract was available, which was used only if it contained all the data fields needed for data extraction. Primary authors were contacted for clarification on several articles. After full-text review, we excluded additional studies for a variety of reasons including unclear study design, study outcomes were not the outcomes of interest, the study population represented a selective group and not the general incarcerated population, or a study did not sufficiently differentiate between subgroups (e.g., HIV prevalence results combined for adults and juveniles).
We hand-searched additional studies from the cited references of those studies selected for full review, and identified supplemental references. We elected to include the Bureau of Justice Statistics Bulletin, which is published regularly and includes multiple years of testing results. For these bulletins, we decided a priori to look at 3 time periods, published in 1999, 2006, and 2009, each covering 3 to 5 years preceding publication, to obtain estimates from different time frames without overlapping data.
Data Extraction
We generated separate tables for the following categories: HIV testing (Table 1), engagement in HIV care (Table 2), and HIV treatment and virological outcomes (Table 3). We then subdivided the engagement and treatment tables into 3 different sections for studies measuring the outcome before, during, and after incarceration. We extracted the following data from each study for inclusion in all 3 tables: author(s), year of publication, correctional setting, geographical location by state or country, and proportion of individuals achieving the outcome of interest. For all tables, we noted missing data with a dash.
TABLE 1—
Summary of HIV Testing in Incarcerated and Recently Released Individuals by Testing Type: Systematic Review and Data Synthesis of the HIV Care Cascade Before, During, and After Incarceration Synthesis Indexed up to January 13, 2015, United States and Canada
| Author | Year | Setting | Location | No. Tested | No. Positive | Newly Diagnosed | Positivity Rate, % | Newly Diagnosed Positivity Rate, % | Type of testing | Method | Gender |
| Altice et al.11 | 1998 | Prison | CT | 975 | 59 | – | 6.1 | – | Blinded | Routine | Men |
| Altice et al.12 | 2005 | Prison | CT | 3 315 | 250 | 93 | 7.54 | 2.81 | Blinded | Routine | Women |
| Andrus et al.13 | 1989 | Prison | OR | 977 | 12 | – | 1.23 | – | Blinded | Routine | Both |
| Begier et al.14 | 2010 | Jail | NY | 6 411 | 389 | 104 | 6.07 | 1.62 | Blinded | Routine | Both |
| Behrendt et al.15 | 1994 | Prison | MD | 2 842 | 242 | – | 8.52 | – | Blinded | Routine | Both |
| Calzavara et al.16 | 1995 | Jail | Canada | 12 048 | 123 | – | 1.02 | – | Blinded | Routine | Both |
| Hammett et al.17 | 1995 | Both | Multiple sitesa | 72 399 | 2 491 | – | 3.44 | – | Blinded | Routine | Both |
| Hoxie et al.18 | 1990 | Prison | WI | 3 458 | 18 | – | 0.52 | – | Blinded | Routine | Men |
| Hoxie et al.19 | 1998 | Prison | WI | 3 681 | 26 | – | 0.71 | – | Blinded | Routine | Men |
| Macalino et al.20 | 2004 | Prison | RI | 3 932 | 70 | – | 1.78 | – | Blinded | Routine | Men |
| Singleton et al.21 | 1990 | Prison | CA | 6 179 | 160 | – | 2.59 | – | Blinded | Routine | Both |
| Smith et al.22 | 1991 | Prison | NY | 480 | 90 | – | 18.75 | – | Blinded | Routine | Women |
| Solomon et al.23 | 2004 | Prison | MD | 3 914 | 251 | – | 6.41 | – | Blinded | Routine | Both |
| Vlahov et al.24 | 1990 | Prison | MD | 5 262 | 415 | – | 7.89 | – | Blinded | Routine | Men |
| Weisfuse et al.25 | 1991 | Prison | NY | 2 236 | 413 | 18.47 | Blinded | Routine | Both | ||
| Wohl et al.26 | 2013 | Prison | NC | 23 200 | 356 | 20 | 1.53 | 0.09 | Blinded | Routine | Both |
| Wu et al.27 | 2001 | SAFPs, Jail, Prison | TX | 4 388 | 109 | – | 2.48 | – | Blinded | Routine | Both |
| Hammett et al.17 | 1995 | Prison | Multiple sitesb | 498 795 | 5 550 | – | 1.11 | – | Mandatory | Routine | Both |
| Maruschak28 | 1999 | Prison | Multiple sitesc | 217 449 | 2 608 | – | 1.20 | – | Mandatory | Routine | Both |
| Maruschak29 | 2006 | Prison | Multiple sitesd | 304 735 | 4 127 | – | 1.35 | – | Mandatory | Routine | Both |
| Maruschak30 | 2009 | Prison | Multiple sitese | 550 681 | 6 271 | – | 1.14 | – | Mandatory | Routine | Both |
| Rich et al.31 | 1999 | Prison | RI | 3 146 | 105 | – | 3.34 | – | Mandatory | Routine | Women |
| Beckwith et al.32 | 2010 | Jail | RI | 264 | 2 | 1 | 0.76 | 0.38 | Opt-out | Routine and rapid | Men |
| Beckwith et al.33 | 2011 | Jail | RI | 1 343 | 12 | 1 | 0.89 | 0.07 | Opt-out | Rapid | Both |
| Beckwith et al.34 | 2012 | Jail | PA | 27 000 | 156 | 75 | 0.58 | 0.28 | Opt-out | Rapid | Both |
| Beckwith et al.34 | 2012 | Jail | DC | 12 546 | 106 | 60 | 0.84 | 0.48 | Opt-out | Rapid | Both |
| Beckwith et al.34 | 2012 | Jail | MD | 2 066 | 42 | 7 | 2.03 | 0.34 | Opt-out | Rapid | Both |
| CDC35 | 2010 | Jail | RI | 102 229 | 1 259 | 169 | 1.23 | 0.17 | Opt-out | Routine | Both |
| CDC36 | 2011 | Prison | WA | 4 651 | – | 6 | – | 0.13 | Opt-out | Routine | Men |
| CDC37 | 2013 | Jail | GA | 12 141 | 120 | 52 | 0.99 | 0.43 | Opt-out | Rapid | Both |
| Kavasery et al.38 | 2009 | Jail | CT | 149 | – | 0 | – | 0.00 | Opt-out | Rapid | Women |
| Kavasery et al.39 | 2009 | Jail | CT | 130 | – | 1 | – | 0.77 | Opt-out | Rapid | Men |
| Spaulding et al.40 | 2014 | Jail | GA | 17 129 | 243 | 99 | 1.42 | 0.58 | Opt-out | Rapid | Both |
| VanHandel et al.41 | 2012 | Both | United States | 106 122 | 1 006 | 755 | 0.95 | 0.71 | Opt-out | Routine | Both |
| CDC36 | 2011 | Prison | WA | 12 174 | – | 13 | – | 0.11 | Opt-in | Routine | Both |
| Cocoros et al.42 | 2014 | Both | MA | 667 | 5 | – | 0.75 | – | Opt-in | Routine | Both |
| Bauserman et al.43 | 2001 | JD or Jail | MD | 1 314 | 14 | – | 1.07 | – | Voluntary | Routine | Both |
| Beckwith et al.44 | 2007 | Jail | RI | 95 | 0 | – | 0.00 | – | Voluntary | Rapid | Men |
| Calzavara et al.45 | 2007 | Jail | Canada | 1 578 | 25 | – | 1.58 | – | Voluntary | Routine | Both |
| Carpenter et al.46 | 1999 | Jail | CA | 2 169 | 71 | – | 3.27 | – | Voluntary | Routine | Both |
| CDC36 | 2011 | Prison | WA | 604 | – | 3 | – | 0.50 | Voluntary | Routine | Men |
| de Voux et al.47 | 2012 | Jail | Multiple sitesf | 210 267 | 1 312 | 822 | 0.62 | 0.39 | Voluntary | Routine | Both |
| Dufour et al.48 | 1996 | Prison | Canada | 618 | 20 | – | 3.24 | – | Voluntary | Routine | Both |
| Ford et al.49 | 1995 | Prison | Canada | 113 | 1 | – | 0.88 | – | Voluntary | Routine | Women |
| Gellert et al.50 | 1993 | Jail | CA | 3 015 | 82 | – | 2.72 | – | Voluntary | Routine | Women |
| Gordon et al.51 | 2013 | Pro/Par | Multiple sitesg | 364 | – | 2 | – | 0.55 | Voluntary | Rapid | Both |
| Hankins et al.52 | 1994 | Prison | Canada | 394 | 27 | – | 6.85 | – | Voluntary | Rapid | Women |
| Harawa et al.53 | 2009 | Jail | CA | 1 322 | – | 23 | – | 1.74 | Voluntary | Routine | Both |
| Kassira et al.54 | 2001 | Prison | MD | 7 159 | 405 | 236 | 5.66 | 3.30 | Voluntary | Routine | Both |
| Kendrick et al.55 | 2004 | Jail | IL | 988 | – | 9 | – | 0.91 | Voluntary | Rapid | Women |
| Klein et al.56 | 2002 | Prison | NY | 9 468 | 95 | – | 1.00 | – | Voluntary | Routine | Both |
| Liddicoat et al.57 | 2006 | Prison | MA | 734 | – | 2 | – | 0.27 | Voluntary | Routine | Both |
| Lyons et al.58 | 2006 | Jail | IL | 110 | 0 | – | 0.00 | – | Voluntary | Routine | Both |
| Macgowan et al.59 | 2009 | Jail | Multiple sitesh | 33 211 | 409 | 269 | 1.23 | 0.81 | Voluntary | Rapid | Both |
| McCusker et al.60 | 1996 | Prison | MA | 1 408 | 144 | – | 10.23 | – | Voluntary | Routine | Both |
| Oser et al.61 | 2006 | Pro/Par | KY | 800 | 0 | – | 0.00 | – | Voluntary | Rapid | Both |
| Poulin et al.62 | 2007 | Prison | Canada | 1 607 | 54 | 11 | 3.36 | 0.68 | Voluntary | Rapid | Both |
| Rosen et al.63 | 2009 | Prison | NC | 21 419 | 718 | 115 | 3.35 | 0.54 | Voluntary | Routine | Both |
| Sabin et al.64 | 2001 | Both | Multiple sitesi | 494 029 | 16 797 | 8 855 | 3.40 | 1.79 | Voluntary | Routine | Both |
| Tartaro and Levy65 | 2013 | Jail | NJ | 956 | 3 | 1 | 0.31 | 0.10 | Voluntary | Rapid | Both |
Note. CDC = Centers for Disease Control and Prevention; JD = juvenile detention; Pro/Par = probation or parole; SAFPs = substance abuse felony punishment units. Dash indicates missing data.
AR, CA, FL, HI, IL, LA, MA, NC, NJ, NY, OR, SC, TN, TX, VA, WA, Canada.
AL, CO, GA, IA, ID, MI, MO, ND, NE, NH, NV, OK, RI, UT, WY.
AL, AR, CO, GA, IA, ID, MI, MO, MS, ND, NE, NH, NV, OK, SD, VA, UT.
AL, AR, CO, GA, IA, ID, MI, MO, MS, ND, NE, NH, OH, OK, RI, SC, UT, WY.
AL, AR, CO, GA, IA, ID, IN, MI, MN, MS, ND, NE, NH, NV, OH, OK, RI, SC, TX, UT, WA, WY.
CT, GA, IL, MA, NY, OH, PA, SC, RI.
MD, RI.
FL, LA, NY, WI.
48 project areas in United States.
TABLE 2—
Summary of Engagement Into HIV Care Before, During, and After Release From Incarceration: Systematic Review and Data Synthesis Indexed up to January 13, 2015, United States and Canada
| Author | Year | Setting | Location | Intervention | No. Positive | No. Engaged Into Care | Proportion Engaged Into Care, % | Timeframe Relative to Incarceration |
| Upon entry or before incarceration | ||||||||
| White et al.66 | 2001 | Jail | CA | NA | 77 | 32 | 42 | Any time before |
| Harzke et al.67 | 2006 | Prison | Southwestern United States | NA | 51 | 31 | 61 | 1 y before |
| Althoff et al.68 | 2013 | Jail | Multiple sitesa | NA | 867 | 641 | 74 | 30 d before |
| Khawcharoenporn et al.69 | 2013 | Jail | IL | NA | 172 | 134 | 78 | Any time before |
| During incarceration | ||||||||
| Farley et al.70 | 2000 | Prison | RI | Yes | 172 | 110 | 64 | During |
| Zaller et al.71 | 2008 | Prison | RI | Yes | 59 | 54 | 92 | During |
| After incarceration | ||||||||
| Warren et al.72 | 1994 | Jail | NY | No | 40 | 15 | 38 | ≤ 95 d after |
| Farley et al.70 | 2000 | Prison | RI | Yes | 41 | 34 | 83 | 6 mo after |
| Rich et al.73 | 2001 | Prison | RI | Yes | 67 | 64 | 95 | 12 mo after |
| Harzke et al.67 | 2006 | Prison | Southwestern United States | No | 30 | 18 | 60 | 21 d after |
| Fontana and Beckerman74 | 2007 | Jail | FL | No | 105 | 77 | 73 | 12 mo after |
| Zaller et al.71 | 2008 | Prison | RI | Yes | 59 | 56 | 96 | 12 mo after |
| Baillargeon et al.75 | 2010 | Prison | TX | No | 1750 | 490 | 28 | ≤ 90 d after |
| Westergaard et al.76 | 2011 | Both | MD | No | 182 | 109 | 60 | 6 mo after |
| Wohl et al.77 | 2011 | Prison | NC | Both | 104 | 82 | 79 | 24 wk after |
| Althoff et al.68 | 2013 | Jail | Multiple sitesa | Yes | 867 | 572 | 66 | 6 mo after |
| Khawcharoenporn et al.69 | 2013 | Jail | IL | No | 95 | 66 | 69 | 6 mo after |
| Beckwith et al.78 | 2014 | Jail | RI | No | 64 | 37 | 58 | 6 mo after |
Note. NA = not applicable.
CT, GA, IL, MA, NY, OH, PA, SC, RI.
TABLE 3—
Summary of HIV Treatment Before, During, and After Release From Incarceration: Systematic Review and Data Synthesis Indexed up to January 13, 2015, United States and Canada
| Author | Year | Setting | Location | Intervention | No. HIV Positive | No. Treated | Proportion on Treatment, % | Undetectable VL, % | Treatment Timeframe Relative to Incarceration |
| Upon entry or before Incarceration | |||||||||
| Althoff et al.68 | 2013 | Jail | Multiple sitesa | NA | 867 | 449 | 52 | 31 | 7 d before |
| Clements-Nolle et al.79 | 2008 | Jail | CA | NA | 108 | 44 | 41 | – | 1 mo before |
| Springer et al.80 | 2004 | Prison | CT | NA | – | 292 | – | 1 | 3 mo before |
| Khawcharoenporn et al.69 | 2013 | Jail | IL | NA | 172 | 125 | 73 | 35 | Any time before |
| Meyer et al.81 | 2014 | Both | CT | NA | 882 | – | – | 30 | Any time before |
| During incarceration | |||||||||
| Arriola et al.82 | 2001 | Jail | FL, NJ, NY | Yes | 171 | 83 | 49 | – | During |
| Baillargeon et al.83 | 2000 | Prison | TX | No | 2360 | 1621 | 69 | – | During |
| Baillargeon et al.75 | 2010 | Prison | TX | No | 1750 | 827 | 47 | 37 | During |
| Beckwith et al.78 | 2014 | Jail | RI | No | 64 | 6 | 9 | – | During |
| Menezes et al.84 | 2013 | Prison | NC | No | 1911 | 1445 | 76 | – | During |
| Mostashari et al.85 | 1998 | Prison | CT | No | 102 | 76 | 75 | – | During |
| Warren et al.72 | 1994 | Jail | NY | No | 170 | 136 | 80 | – | During |
| Khawcharoenporn et al.69 | 2013 | Jail | IL | No | 172 | 132 | 77 | – | During (> 39 d) |
| White et al.66 | 2001 | Jail | CA | No | 77 | 45 | 58 | 25 | During (> 85 d) |
| Bingham86 | 2012 | Federal BOP | United States | No | 1445 | 858 | 59 | 46 | During (> 3 mo) |
| Wohl et al.87 | 2003 | Prison | NC | No | 31 | 45 | During (> 3 mo) | ||
| Pai et al.88 | 2009 | Jail | CA | No | 512 | 467 | 91 | 32 | During (> 104 d) |
| Altice et al.89 | 2001 | Prison | CT | No | 205 | 164 | 80 | – | During (6 mo) |
| Griffin et al.90 | 1996 | Jail | TX | No | 225 | 78 | 35 | – | During (> 6 mo) |
| Kirkland et al.91 | 2002 | Prison | United States | Yes | – | 108 | – | 68 | During (> 6 mo) |
| Springer et al.80 | 2004 | Prison | CT | No | – | 1866 | – | 59 | During (> 6 mo) |
| Stephenson et al.92 | 2005 | Prison | NC | No | – | 30 | – | 50 | During (> 9 mo) |
| Meyer et al.93 | 2012 | Prison | CT | Yes | – | 151 | – | 80 | Before release (> 90 d) |
| Springer et al.94 | 2010 | Prison | CT | Yes | – | 23 | – | 63 | Before release (> 90 d) |
| Wohl et al.77 | 2011 | Prison | NC | Both | 89 | 62 | 70 | 58 | Before release (> 3 mo) |
| Harzke et al.67 | 2006 | Prison | Southwestern United States | No | 30 | 14 | 47 | – | At release |
| Meyer et al.81 | 2014 | Both | CT | No | – | 882 | – | 70 | At release |
| Reznick et al.95 | 2013 | Both | CA | Yes | 151 | 89 | 59 | – | At release |
| After incarceration | |||||||||
| Warren et al.72 | 1994 | Jail | NY | No | 30 | 8 | 27 | – | Immediately after |
| Springer et al.94 | 2010 | Prison | CT | Yes | – | 23 | – | 61 | 12 wk |
| Baillargeon et al.96 | 2009 | Prison | TX | No | 2115 | 634 | 30 | – | 60 d after |
| Devereux et al.97 | 2002 | Prison | NV | Yes | 35 | 22 | 63 | – | 3 mo after |
| Reznick et al.95 | 2013 | Both | CA | Yes | 139 | 63 | 45 | – | 4 mo after |
| Meyer et al.98 | 2014 | Jail | Multiple sitesa | Yes | 867 | 450 | 52 | – | 6 mo after |
| Spaulding et al.99 | 2013 | Jail | Multiple sitesa | Yes | 1082 | – | – | 26 | 6 mo after |
| Westergaard et al.76 | 2011 | Both | MD | No | 182 | 67 | 37 | – | ∼7.6 mo after |
Note. BOP = Bureau of Prisons; NA = not applicable; VL = viral load. Dash indicates missing data.
CT, GA, IL, MA, NY, OH, PA, SC, RI.
For Table 1, we included number of individuals tested overall, number of positive tests, and number of new positives. We calculated the positivity rate and newly diagnosed positivity rate based on these values. We recorded method of testing (routine or rapid) and grouped studies by how testing was offered (blinded, mandatory, opt-out, opt-in, voluntary). We defined blinded testing in the study methods as using available discarded or excess sera from routine phlebotomy performed on incoming inmates. Blinded testing is anonymized and performed for the purposes of epidemiological study, not for clinical care of inmates. Mandatory testing refers to programs in which all inmates are tested per protocol. In opt-out testing, an inmate is informed that an HIV test will be performed unless he or she declines the test, whereas opt-in testing is when an HIV test is offered routinely and those desiring testing need to actively give permission to be tested. Lastly, voluntary testing refers to testing for HIV that is made available to inmates, not necessarily through a direct offer of testing (may be advertised through posters or signs), and includes testing on patient request. Several studies initially offered voluntary testing and then completed blinded testing on all inmates who declined voluntary testing; these results were combined and included under the blinded category.13,18,26 For studies that allowed inmates known to be HIV-infected to opt out of testing, only new positives were recorded.36,38,39
The included studies in the engagement-in-care table defined engagement as having at least 1 medical visit during the timeframe indicated. Studies are grouped by year of publication. For the HIV treatment table, we defined treatment as receipt of antiretrovirals during the timeframe listed for each study. Undetectable viral load was defined differently in some studies; the majority defined this as less than 400, less than 50, or less than 20, although one study used less than 500.66 Therefore, for the purpose of this review, we considered a viral load less than 500 copies per milliliter undetectable.
Data Synthesis
To generate the different steps in the HIV treatment cascade for the 3 time periods—before, during, and after incarceration—we included data from all studies relevant to each respective step in the calculations by using weighted means. To estimate the proportion of HIV-infected individuals entering corrections who were known to be HIV-positive at the time of incarceration, we compiled the data from all HIV testing studies that performed blinded testing and reported the number of new diagnoses.12,14,26 The included studies defined an individual as previously undiagnosed with HIV if the inmate’s self-report or medical records indicated a previous negative HIV test or lack of awareness of HIV infection. There was no published literature on blinded testing for HIV during or after incarceration. For the proportion of new HIV diagnoses made during incarceration, we assumed that these diagnoses would be in addition to those already known at entry and, because most facilities only provide testing upon request after entry, would identify relatively few new HIV diagnoses. We extrapolated a 1% increase in known HIV infection based on HIV testing data from inmates tested during incarceration at the Dallas County Jail (written communication, E. Porsa, MD, MPH, CCHP, Parkland Jail Health, July 15, 2014). The proportion of new HIV diagnoses made after release from incarceration were also estimated to be few (< 1%) based on 2 studies involving individuals on probation or parole.51,61
For engagement in HIV care, we defined linkage to care upon entry to jail or prison as having received any HIV care before incarceration.66–69 For retention in care upon entry to jail or prison we used national data from the general population living with HIV in the United States.4 For linkage to and retention into care during incarceration, we compiled reports from the Dallas County Jail (written communication, E. Porsa, MD, MPH, CCHP, Parkland Jail Health, July 15, 2014) and 2 published studies.70,71 For the postrelease population, we defined linkage to care as 1 medical visit within 6 months after release from incarceration, which included both newly diagnosed and known HIV-infected individuals.67–70,75–78 We considered retention in care to be 2 medical visits over 6 months, an outcome reported in 1 multicenter study.68
To estimate the proportion of HIV-infected individuals receiving ART upon entry to jail or prison, we compiled data from multiple studies that assessed treatment before incarceration.68,69,79 For the proportion receiving ART while incarcerated, we included all studies reporting HIV treatment during incarceration or at the time of release.66,67,69,72,75,77,78,85,88,89,95 For estimates of released inmates on ART, we summarized data from studies with follow-up within a 6-month period.72,76,81,95,96 Finally, we estimated the proportion of HIV-infected individuals with an undetectable viral load (< 500 copies/mL) upon entry,68,69,80,98 during,66,75,77,80,86,87,91–94,98 and after release from incarceration.99,100
RESULTS
The electronic search process for article selection is summarized in Figure 1. The search identified 2706 titles, of which we excluded 2406 for not meeting criteria on the basis of review of the title and abstract. We retrieved the remaining 300 full-text articles for review. Of these, we excluded 201 on the basis of our eligibility criteria and we excluded an additional 19 because of reporting results from selective study populations not representative of the entire incarcerated population, the same study population was examined by different articles reporting on related outcomes of interest, or the HIV treatment timeframe was unclear or insufficient for the outcome measure. For inclusion in the final review, we identified an additional 5 titles from hand-searching references along with 2 conference proceedings, 4 Bureau of Justice Statistics HIV testing bulletins, and a report from the local county jail (written communication, E. Porsa, MD, MPH, CCHP, Parkland Jail Health, July 15, 2014).17,28–30,40,78,81,89,98–100
FIGURE 1—
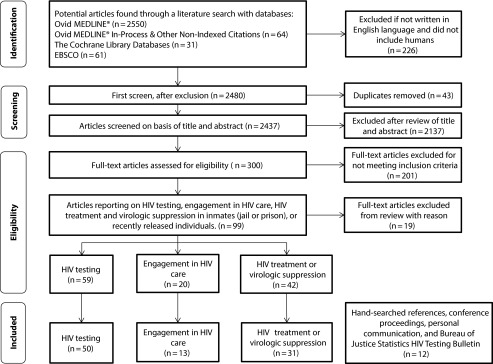
Flow diagram of study selection in a systematic review and data synthesis indexed up to January 13, 2015, of the HIV care cascade before, during, and after incarceration: United States and Canada.
Study Characteristics
Overall, we included 92 unique studies for review, of which 10 were included in more than 1 HIV care cascade category.66–69,72,75,76,78,99 Eleven studies reported HIV outcome data obtained from multiple geographic sites.41,47,51,59,64,67,68,72,82,86,99 Fifty-five percent of the studies reviewed were surveillance studies of HIV testing upon entry into the correctional setting. Twenty-one were retrospective cohort studies of HIV-infected inmates66,69,75,78,83,84,86,88,90,92,101 or releasees.69–71,73,75,78 Three studies used a longitudinal design, assessing HIV outcomes in this population at multiple time points.67,72,76 Other study designs included descriptive studies,74,85,87,89 multisite prospective demonstration projects,68,81,82,99 nonrandomized trials,32,38,39,91 and randomized trials.51,77,94,95
Of the 50 studies, and 1 conference proceeding40 that addressed HIV testing, 21 were in the jail setting, 24 in the prison setting, 4 in combined settings, and 2 at probation or parole offices. The Bureau of Justice Statistics HIV testing bulletins predominately reported results from the prison setting.17,28–30 The majority of testing was implemented upon entry to a correctional facility; however, a few compared testing at different time points during incarceration.57–59 We identified 13 studies addressing engagement in HIV care. Lastly, we reviewed 31 studies and 1 conference proceeding100 on HIV treatment and virological suppression in prisoners.
HIV Testing, Engagement in Care, and Treatment
We summarized HIV testing by testing type (Table 1). Eighteen studies, and 4 summary reports indicated testing of inmates in a blinded or mandatory fashion upon entry into the correctional facilities. All but 2 were performed in a prison setting. In general, incarcerated women had higher rates of HIV than incarcerated men, though most studies reported combined results for men and women. The average HIV positivity rate among blinded and mandatory studies combined was 1.39% (range = 0.52%–18.75%), and average newly diagnosed positivity rate (only reported in 3 studies) was 0.66% (range = 0.09%–2.81%).
The majority of opt-out testing was implemented in jails with rapid testing methods. The proportion of positive tests averaged 1.05% (range = 0.58%–2.03%), and all studies reported the proportion newly diagnosed, averaging 0.43% (range = 0%–0.77%).
Opt-in HIV screening was reported by only 2 studies; 1 compared its results to the later adoption of an opt-out screening program,36 and the other integrated an HCV-screening initiative into an existing HIV-screening program.42 Twenty-four studies conducted voluntary HIV screening. When we combined the opt-in and voluntary testing efforts, the average HIV-positivity rate was 2.55% (range = 0%–10.23%) and the newly diagnosed positivity rate was 1.32% (range = 0.10%–3.30%).
Engagement in HIV care was summarized in 15 different studies, which ranged from observational descriptive studies to randomized controlled interventions (Table 2). At the time of incarceration, an average of 72% (42%–78%) of inmates who were HIV-positive were reported to have visited an HIV care provider before entering jail or prison. There were 2 studies that specifically reported on engagement in care during incarceration.70,71 Twelve studies followed up with inmates after release from incarceration and had varying timeframes for engagement in HIV care, ranging from 21 days to a year. Engagement in care, defined as a single medical visit after release, was lower in observational studies, 28% by 3 months, 58% to 59% by 6 months, and 73% by 12 months compared with studies that conducted directed interviews or employed an intervention, 38% to 60% at 3 months, 66% to 85% at 6 months, and 95% to 96% at 12 months.
Receipt of antiretrovirals before, during, and after incarceration is summarized in Table 3. Approximately 54% (41%–73%) of HIV-positive patients were receiving ART before incarceration. On average, 65% (9%–91%) received ART during incarceration and 37% (27%–63%) received ART after release. Rates of virological suppression varied at entry to a correctional facility, 27% (1%–35%), then on average up to 51% (25%–80%) during incarceration, and 26% at 6 months postrelease (based on a multicenter demonstration project).99 Several studies assessed adherence to ART, defined as missing no more than 1 dose per week or taking at least 80% of prescribed medications. We assessed adherence only in those prescribed ART and it was measured by directly observed therapy, through electronic monitoring caps, by pill counts, or by self-reported adherence questionnaire. Before incarceration, adherence was estimated at 34% (33%–48%)68,79; during incarceration, adherence was 58% (30%–94%)85,87,89,91,99; and after release, adherence was 40% (39%–49%).81,95
Cascade
Figure 2 depicts the HIV care cascade before, during, and after release from incarceration. Overall, all steps of the cascade improved substantially during incarceration, often to rates higher than the national average, but dropped to below those rates for each step of the cascade after release from jail or prison, to levels that were equal to or lower than before incarceration. The largest declines were in postincarceration engagement in care, with a drop from 76% to 36% for linkage to care and from 76% to 30% for retention in care. Receipt of ART dropped from 51% to 29% after release, and virological suppression dropped from 40% to 21% after release.
FIGURE 2—

HIV care cascade—before, during, and after release from incarceration: systematic review and data synthesis indexed up to January 13, 2015, United States and Canada.
Note. ART = antiretroviral therapy; VL = viral load.
aReferences 4, 14, 69–71, and 76.
bReferences 4, 67, 75, 77–79, 82, 83, 86, 89, and 90.
cReferences 4 and 77.
dReferences 4, 65, 67, 72, 75, 77, 78, 80–86, 88, 90–96, and 98.
eReferences 4, 17, 28–30, 38, 40, 67, 72, 75, 77, 78, 80, 83, 87, 90, 99, and 100.
Specific gaps identified in the literature, where only limited or no data were available, include testing after release from corrections (and the potential for identifying new positives in the recently released population), rates of linkage to and retention in care before incarceration, and virological outcomes in the released population.
DISCUSSION
Through a systematic review of the literature, we have demonstrated that the HIV care cascade in incarcerated and recently released individuals reflects low rates of HIV awareness, engagement in care, retention in care, and virological suppression in this population. Specifically, upon entry to jail and prison, many individuals who are HIV-infected are not aware of their diagnosis, reinforcing the importance of offering routine, opt-out testing at the time of intake. Of those who are aware of their HIV, many are not engaged in routine care and not taking ART, and few are virologically suppressed. Rates of all of these steps in the cascade increase considerably during incarceration, highlighting the important public health opportunity jails and prisons have to make an impact on this underserved population. However, not only are these gains lost after release, but outcomes for the cascade are also generally worse after incarceration than before, underscoring the urgent need for stronger re-entry and linkage-to-care programs as inmates transition to the community.
We found that the results of HIV testing in jails and prisons varied widely among studies. Because of the heterogeneity of HIV-testing studies and the wide time frame in which they were conducted, it is difficult to draw conclusions about which testing techniques may result in the greatest number of HIV-positive individuals identified. Among the blinded studies, there were several outliers15,22,24,25 that had been conducted in New York and Maryland in the early 1990s that identified very high rates of infection (7.89%–18.75%). Subsequent blinded studies still identified relatively high rates in these states (6.07%–6.41%),14,23 though they were much reduced over previous, which may be related to high mortality early in the AIDS epidemic, changes in the epidemiology of injection drug use, prevention efforts, and the introduction of ART. The blinded results provide the best estimate of HIV prevalence in these settings, though this is not a practical approach to offering HIV testing. Eight of the published voluntary testing studies also found high positivity rates greater than 3%46,48,54,60,62–64,70; however, it is unknown how many infections were missed among those who did not volunteer for testing. In general, the results among voluntary tests vary widely in part because of variability in how this testing is offered and accepted across sites. Opt-out testing found comparatively lower rates of positive results, though results were relatively consistent across sites and represent testing of a large proportion of the incarcerated population in each setting, including high- and low-risk individuals.
With regard to new HIV diagnoses, certain settings, such as the North Carolina and Rhode Island prison systems,26,33 or low-prevalence areas such as Wisconsin or Washington state,18,36 had low rates of newly diagnosed individuals, whereas in other settings,14,40,52,54,59,64 many more previously undiagnosed individuals were identified. This may reflect the previous success of longstanding testing efforts in correctional systems, which have already identified a large proportion of HIV in those involved in the criminal justice system compared with new testing efforts in places, such as jails and high-prevalence areas in the southern United States, where there has historically been less HIV testing.40,59,64,102 The Centers for Disease Control and Prevention recommends offering routine, opt-out testing in correctional medical clinics,103 as this may reduce the stigma of testing, identify new infections, identify infections earlier, and improve access to treatment and prevention services.47,103 However, per a recent survey, only 19% of prison systems and 35% of jails provide opt-out HIV testing.104 Although routine HIV testing in the correctional setting may be cost-effective from a societal perspective,105 the cost of treatment of HIV-positive inmates is expensive,106 and could deter correctional facilities from providing testing. Future partnerships between state departments of corrections and departments of health are needed to expand testing in jails and prisons to reduce the estimated 22% of HIV-infected individuals entering corrections who are unaware of their HIV infection (Figure 2).
For incoming inmates, overall rates of linkage to care were 6 percentage points lower than the general population, (Figure 2; 56% vs 62%).107 This underscores the role of correctional institutions in improving rates of engagement (and re-engagement) in care for this population. During incarceration, the majority of HIV-infected inmates has access to HIV care and ART and surpasses the general population in this step of the cascade. However, after release from incarceration, rates of linkage to care and retention in care drop dramatically resulting in a decline in treatment and virological suppression rates. Multiple factors have been identified that contribute to linkage to HIV care after release from jail or prison. Facilitators of linkage include HIV education during incarceration, discharge planning, transportation, and stable housing68,108 and barriers include drug use,109 mental illness, stigma, lack of social support, and unemployment.110 Accordingly, successful interventions have addressed many of these issues, including opiate replacement therapy,94,111 enhanced case management,73,112,113 patient navigation,114 or combinations thereof.68 However, results of some interventions have been mixed and a randomized controlled trial of intensive case management versus standard of care did not show a significant difference in rates of linkage to care,77 though overall rates of linkage to HIV care in this study were quite high.
Nonetheless, nationwide, there is room for improvement in linkage to HIV care after release from incarceration. Fewer than 20% of prisons and jails provide discharge planning services for inmates transitioning to the community per Centers for Disease Control and Prevention guidelines, including making an appointment with a community health care provider, assisting with enrollment in an entitlement program, and providing a copy of the medical record and a supply of HIV medication.104 Under the Affordable Care Act, states that are expanding Medicaid will have new opportunities to link individuals to community health care after release from jail.115
With regard to virological suppression, among individuals known to be HIV-infected, nearly 50% had received treatment before incarceration, though only 27% of them had an undetectable viral load upon entry to jail or prison. However, the majority of inmates do achieve virological suppression during incarceration (52% of total, 65% of those on ART), and suppression rates are higher with longer duration of incarceration.76,116 Compared with the general population, and with the proportion of those on therapy with undetectable viral load as a proxy for adherence, inmates’ average adherence during incarceration, 58% (30%–94%), is not as high as adherence among the general population (78%–87%),117,118 suggesting a need for education and adherence counseling. This may be especially true in the reincarcerated population, who have lower rates of virological suppression overall,80,98,119 consistent with a dose–response effect of incarceration on nonadherence.120 Lastly, we found that the largest gap in the literature on HIV in the criminal justice system is clinical outcomes among released inmates, with only 2 published studies reporting HIV viral loads after release.94,99 Of these, the Enhancelink study, a multicenter demonstration project, found that 26% had an undetectable viral load 6 months after release by using a missing equals failure analysis. Further study is needed in this area, and a series of ongoing projects on “seek, test, treat, and retain” may provide additional data and insight to this outcome.121 With the increase in sexual and drug use risk behavior after release from incarceration,122–125 increasing virological suppression in these individuals has direct implications for secondary HIV prevention.
Along the continuum in the incarcerated and recently released, racial disparities persist. For example, Blacks were less likely to have an HIV provider 30 days before jail entry and more likely to have advanced HIV disease.126 In addition, Hispanics and Blacks were less likely to fill an initial prescription for ART within 10 and 30 days after release, compared with non-Hispanic Whites.96 To reduce such health disparities, additional efforts need to be directed at incarcerated individuals and those returning to the community, including specific interventions tailored to minority patients.
Limitations
There are several limitations inherent to our systematic review. Using what is available in the published literature likely biases toward jails and prisons that have extra efforts aimed at identifying HIV, engaging HIV patients in care, and providing treatment. In addition, our systematic review is limited by varied definitions of each care cascade step by different studies. We included observational studies as well as those that implemented interventions to present all of the available published data. Therefore, our cascade may overestimate some of these outcomes because of publication bias, indicating that the disparities in outcomes between this population and the general HIV-infected population may be even greater than our estimates.
The heterogeneity of studies made it challenging to summarize some of the outcomes; however, this was accounted for whenever possible. For example, for testing studies that excluded known HIV-infected individuals, we reported these as new infections only. For engagement in care studies in which missing data (e.g., individuals who do not follow-up after release) was not considered failure, we used the original study group as the denominator. For treatment, guidelines have changed over time with regard to when to initiate therapy, and, therefore, the number eligible for treatment was based on what was provided by each study, following time period–appropriate guidelines.
Conclusions
Overall, this is the first systematic review to our knowledge to address the HIV care cascade in the incarcerated and recently released population. We have summarized HIV testing, engagement in care, and treatment at 3 stages—before, during, and after incarceration—and have found that the care cascade is dynamic, with large increases during and even larger declines after incarceration. This net negative effect on HIV outcomes is consistent with previous studies, which identified incarceration as disruptive to HIV treatment117 and virological suppression, though our 3-stage model provides more detail about where and when the gaps in care are most pronounced. Specifically, new efforts are needed to (1) increase opt-out HIV testing for inmates and recently released individuals because of the high rates of unidentified HIV-positive individuals in the criminal justice system; (2) improve continuity of care after release from corrections, because of the sharp decline in HIV medical visits and treatment during this interval, a time period characterized by high-risk sexual and drug-use behaviors leading to HIV transmission and death; and (3) measure and increase virological suppression after release, so that HIV-infected released inmates realize the same benefits of ART as others with HIV.
These targets are directly aligned with the goals of the national HIV/AIDS strategy to decrease HIV incidence, improve health outcomes, and reduce HIV-related health disparities and will require significant shifts in current local and national policies. Specific actions include reducing incarceration overall, reassessing discriminatory sentencing laws, increasing diversion to substance abuse and mental health treatment programs, expanding access to medical care through Medicaid and other benefit programs, incentivizing collaborations between public health and corrections agencies, and disseminating best practices.
Acknowledgments
Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award KL2TR001103 (A. N.) and by 5R01DA030778 (principal investigator, A. N.).
Note. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Human Participant Protection
Institutional review board approval was not needed, as our research did not involve human participant interactions or identifiable private information.
References
- 1.National HIV/AIDS Strategy for the United States. Washington, DC: The White House; 2010. [Google Scholar]
- 2.Obama B. Washington, DC: The White House, Office of the Press Secretary; 2013. HIV care continuum initiative. [Google Scholar]
- 3.Gardner EM, McLees MP, Steiner JF, Del Rio C, Burman WJ. The spectrum of engagement in HIV care and its relevance to test-and-treat strategies for prevention of HIV infection. Clin Infect Dis. 2011;52(6):793–800. doi: 10.1093/cid/ciq243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Centers for Disease Control and Prevention. Vital signs: HIV prevention through care and treatment—United States. MMWR Morb Mortal Wkly Rep. 2011;60(47):1618–1623. [PubMed] [Google Scholar]
- 5.Centers for Disease Control and Prevention. Monitoring selected national HIV prevention and care objectives by using HIV surveillance data—United States and 6 dependent areas—2011. HIV Surveillance Supplemental Report. 2013;18(5) [Google Scholar]
- 6. Hall I, Frazier E, Holtgrave D, et al. Continuum of HIV care: difference in care and treatment by sex and race/ethnicity in the United States. Oral abstract presented at: 19th International AIDS Conference; July 27, 2012; Washington, DC.
- 7.Spaulding AC, Seals RM, Page MJ, Brzozowski AK, Rhodes W, Hammett TM. HIV/AIDS among inmates of and releasees from US correctional facilities, 2006: declining share of epidemic but persistent public health opportunity. PLoS ONE. 2009;4(11):e7558. doi: 10.1371/journal.pone.0007558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rich JD, DiClemente R, Levy J et al. Correctional facilities as partners in reducing HIV disparities. J Acquir Immune Defic Syndr. 2013;63(suppl 1):S49–S53. doi: 10.1097/QAI.0b013e318292fe4c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Washington, DC: Pew Charitable Trusts; 2008. One in 100 behind bars in America 2008. Report no. 1. [Google Scholar]
- 10.Cohen MS, Chen YQ, McCauley M et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493–505. doi: 10.1056/NEJMoa1105243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Altice FL, Mostashari F, Selwyn PA et al. Predictors of HIV infection among newly sentenced male prisoners. J Acquir Immune Defic Syndr Hum Retrovirol. 1998;18(5):444–453. doi: 10.1097/00042560-199808150-00005. [DOI] [PubMed] [Google Scholar]
- 12.Altice FL, Marinovich A, Khoshnood K, Blankenship KM, Springer SA, Selwyn PA. Correlates of HIV infection among incarcerated women: implications for improving detection of HIV infection. J Urban Health. 2005;82(2):312–326. doi: 10.1093/jurban/jti055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Andrus JK, Fleming DW, Knox C et al. HIV testing in prisoners: is mandatory testing mandatory? Am J Public Health. 1989;79(7):840–842. doi: 10.2105/ajph.79.7.840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Begier EM, Bennani Y, Forgione L et al. Undiagnosed HIV infection among New York City jail entrants, 2006: results of a blinded serosurvey. J Acquir Immune Defic Syndr. 2010;54(1):93–101. doi: 10.1097/QAI.0b013e3181c98fa8. [DOI] [PubMed] [Google Scholar]
- 15.Behrendt C, Kendig N, Dambita C, Horman J, Lawlor J, Vlahov D. Voluntary testing for human immunodeficiency virus (HIV) in a prison population with a high prevalence of HIV. Am J Epidemiol. 1994;139(9):918–926. doi: 10.1093/oxfordjournals.aje.a117098. [DOI] [PubMed] [Google Scholar]
- 16.Calzavara LM, Major C, Myers T et al. Reducing volunteer bias: using left-over specimens to estimate rates of HIV infection among inmates in Ontario, Canada. AIDS. 1995;9(6):631–637. [PubMed] [Google Scholar]
- 17.Hammett TM, Widom R, Epstein J, Gross M, Sifre S, Enos T. 1994 Update: HIV/AIDS and STDs in Correctional Facilities. Washington, DC: US Department of Justice, Office of Justice Programs, National Institute of Justice; 1995. [Google Scholar]
- 18.Hoxie NJ, Vergeront JM, Frisby HR, Pfister JR, Golubjatnikov R, Davis JP. HIV seroprevalence and the acceptance of voluntary HIV testing among newly incarcerated male prison inmates in Wisconsin. Am J Public Health. 1990;80(9):1129–1131. doi: 10.2105/ajph.80.9.1129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hoxie NJ, Chen MH, Prieve A, Haase B, Pfister J, Vergeront JM. HIV seroprevalence among male prison inmates in the Wisconsin Correctional System. WMJ. 1998;97(5):28–31. [PubMed] [Google Scholar]
- 20.Macalino GE, Vlahov D, Sanford-Colby S et al. Prevalence and incidence of HIV, hepatitis B virus, and hepatitis C virus infections among males in Rhode Island prisons. Am J Public Health. 2004;94(7):1218–1223. doi: 10.2105/ajph.94.7.1218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Singleton JA, Perkins CI, Trachtenberg AI, Hughes MJ, Kizer KW, Ascher M. HIV antibody seroprevalence among prisoners entering the California correctional system. West J Med. 1990;153(4):394–399. [PMC free article] [PubMed] [Google Scholar]
- 22.Smith PF, Mikl J, Truman BI et al. HIV infection among women entering the New York State correctional system. Am J Public Health. 1991;81(suppl):35–40. doi: 10.2105/ajph.81.suppl.35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Solomon L, Flynn C, Muck K, Vertefeuille J. Prevalence of HIV, syphilis, hepatitis B, and hepatitis C among entrants to Maryland correctional facilities. J Urban Health. 2004;81(1):25–37. doi: 10.1093/jurban/jth085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Vlahov D, Munoz A, Brewer F, Taylor E, Canner C, Polk BF. Seasonal and annual variation of antibody to HIV-1 among male inmates entering Maryland prisons: update. AIDS. 1990;4(4):345–350. doi: 10.1097/00002030-199004000-00010. [DOI] [PubMed] [Google Scholar]
- 25.Weisfuse IB, Greenberg BL, Back SD et al. HIV-1 infection among New York City inmates. AIDS. 1991;5(9):1133–1138. doi: 10.1097/00002030-199109000-00013. [DOI] [PubMed] [Google Scholar]
- 26.Wohl DA, Golin C, Rosen DL, May JM, White BL. Detection of undiagnosed HIV among state prison entrants. JAMA. 2013;310(20):2198–2199. doi: 10.1001/jama.2013.280740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wu ZH, Baillargeon J, Grady JJ, Black SA, Dunn K. HIV seroprevalence among newly incarcerated inmates in the Texas correctional system. Ann Epidemiol. 2001;11(5):342–346. doi: 10.1016/s1047-2797(01)00210-1. [DOI] [PubMed] [Google Scholar]
- 28.Maruschak L. Washington, DC: US Department of Justice, Bureau of Justice Statistics; 1999. HIV in prisons, 1997. Report no. 178284. [Google Scholar]
- 29.Maruschak L. Washington, DC: US Department of Justice, Office of Justice Programs; 2006. HIV in prisons, 2004. Report no. 213897. [Google Scholar]
- 30.Maruschak L. Washington, DC: US Department of Justice, Bureau of Justice Statistics; 2009. HIV in prisons, 2007–08. Report no. 228307. [Google Scholar]
- 31.Rich JD, Dickinson BP, Macalino G et al. Prevalence and incidence of HIV among incarcerated and reincarcerated women in Rhode Island. J Acquir Immune Defic Syndr. 1999;22(2):161–166. doi: 10.1097/00126334-199910010-00008. [DOI] [PubMed] [Google Scholar]
- 32.Beckwith CG, Liu T, Bazerman LB et al. HIV risk behavior before and after HIV counseling and testing in jail: a pilot study. J Acquir Immune Defic Syndr. 2010;53(4):485–490. doi: 10.1097/QAI.0b013e3181c997b1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Beckwith CG, Bazerman L, Cornwall AH et al. An evaluation of a routine opt-out rapid HIV testing program in a Rhode Island jail. AIDS Educ Prev. 2011;23(3, suppl):96–109. doi: 10.1521/aeap.2011.23.3_supp.96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Beckwith CG, Nunn A, Baucom S et al. Rapid HIV testing in large urban jails. Am J Public Health. 2012;102(suppl 2):S184–S186. doi: 10.2105/AJPH.2011.300514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Centers for Disease Control and Prevention. Routine jail-based HIV testing—Rhode Island, 2000–2007. MMWR Morb Mortal Wkly Rep. 2010;59(24):742–745. [PubMed] [Google Scholar]
- 36.Centers for Disease Control and Prevention. HIV screening of male inmates during prison intake medical evaluation—Washington, 2006–2010. MMWR Morb Mortal Wkly Rep. 2011;60(24):811–813. [PubMed] [Google Scholar]
- 37.Centers for Disease Control and Prevention. Routine HIV screening during intake medical evaluation at a County Jail—Fulton County, Georgia, 2011–2012. MMWR Morb Mortal Wkly Rep. 2013;62(24):495–497. [PMC free article] [PubMed] [Google Scholar]
- 38.Kavasery R, Maru DS, Cornman-Homonoff J, Sylla LN, Smith D, Altice FL. Routine opt-out HIV testing strategies in a female jail setting: a prospective controlled trial. PLoS ONE. 2009;4(11):e7648. doi: 10.1371/journal.pone.0007648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kavasery R, Maru DS, Sylla LN, Smith D, Altice FL. A prospective controlled trial of routine opt-out HIV testing in a men’s jail. PLoS ONE. 2009;4(11):e8056. doi: 10.1371/journal.pone.0008056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Spaulding A, Mustaafaa G, Kim MJ, John K, Bowden C. Doubling the yield of voluntary HIV testing in an Atlanta jail. Poster presented at: 7th Academic and Health Policy Conference on Correctional Health; March 21, 2014; Houston, TX.
- 41.VanHandel M, Beltrami JF, MacGowan RJ, Borkowf CB, Margolis AD. Newly identified HIV infections in correctional facilities, United States, 2007. Am J Public Health. 2012;102(suppl 2):S201–S204. doi: 10.2105/AJPH.2011.300614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Cocoros N, Nettle E, Church D et al. Screening for Hepatitis C as a Prevention Enhancement (SHAPE) for HIV: an integration pilot initiative in a Massachusetts County correctional facility. Public Health Rep. 2014;129(suppl 1):5–11. doi: 10.1177/00333549141291S102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Bauserman RL, Ward MA, Eldred L, Swetz A. Increasing voluntary HIV testing by offering oral tests in incarcerated populations. Am J Public Health. 2001;91(8):1226–1229. doi: 10.2105/ajph.91.8.1226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Beckwith CG, Atunah-Jay S, Cohen J et al. Feasibility and acceptability of rapid HIV testing in jail. AIDS Patient Care STDS. 2007;21(1):41–47. doi: 10.1089/apc.2006.006. [DOI] [PubMed] [Google Scholar]
- 45.Calzavara L, Ramuscak N, Burchell AN et al. Prevalence of HIV and hepatitis C virus infections among inmates of Ontario remand facilities. CMAJ. 2007;177(3):257–261. doi: 10.1503/cmaj.060416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Carpenter CL, Longshore D, Annon K, Annon JJ, Anglin MD. Prevalence of HIV-1 among recent arrestees in Los Angeles County, California: serial cross-sectional study, 1991–1995. J Acquir Immune Defic Syndr. 1999;21(2):172–177. [PubMed] [Google Scholar]
- 47.de Voux A, Spaulding AC, Beckwith C et al. Early identification of HIV: empirical support for jail-based screening. PLoS ONE. 2012;7(5):e37603. doi: 10.1371/journal.pone.0037603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Dufour A, Alary M, Poulin C et al. Prevalence and risk behaviours for HIV infection among inmates of a provincial prison in Quebec City. AIDS. 1996;10(9):1009–1015. doi: 10.1097/00002030-199610090-00012. [DOI] [PubMed] [Google Scholar]
- 49.Ford PM, White C, Kaufmann H et al. Voluntary anonymous linked study of the prevalence of HIV infection and hepatitis C among inmates in a Canadian federal penitentiary for women. CMAJ. 1995;153(11):1605–1609. [PMC free article] [PubMed] [Google Scholar]
- 50.Gellert GA, Maxwell RM, Higgins KV, Pendergast T, Wilker N. HIV infection in the Women’s Jail, Orange County, California, 1985 through 1991. Am J Public Health. 1993;83(10):1454–1456. doi: 10.2105/ajph.83.10.1454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Gordon MS, Kinlock TW, McKenzie M, Wilson ME, Rich JD. Rapid HIV testing for individuals on probation/parole: outcomes of an intervention trial. AIDS Behav. 2013;17(6):2022–2030. doi: 10.1007/s10461-013-0456-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Hankins CA, Gendron S, Handley MA, Richard C, Tung MT, O’Shaughnessy M. HIV infection among women in prison: an assessment of risk factors using a nonnominal methodology. Am J Public Health. 1994;84(10):1637–1640. doi: 10.2105/ajph.84.10.1637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Harawa NT, Bingham TA, Butler QR et al. Using arrest charge to screen for undiagnosed HIV infection among new arrestees: a study in Los Angeles County. J Correct Health Care. 2009;15(2):105–117. doi: 10.1177/1078345808330038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Kassira EN, Bauserman RL, Tomoyasu N, Caldeira E, Swetz A, Solomon L. HIV and AIDS surveillance among inmates in Maryland prisons. J Urban Health. 2001;78(2):256–263. doi: 10.1093/jurban/78.2.256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Kendrick SR, Kroc KA, Couture E, Weinstein RA. Comparison of point-of-care rapid HIV testing in three clinical venues. AIDS. 2004;18(16):2208–2210. doi: 10.1097/00002030-200411050-00017. [DOI] [PubMed] [Google Scholar]
- 56.Klein SJ, O’Connell DA, Devore BS, Wright LN, Birkhead GS. Building an HIV continuum for inmates: New York State’s criminal justice initiative. AIDS Educ Prev. 2002;14(5, suppl B):114–123. doi: 10.1521/aeap.14.7.114.23856. [DOI] [PubMed] [Google Scholar]
- 57.Liddicoat RV, Zheng H, Internicola J et al. Implementing a routine, voluntary HIV testing program in a Massachusetts county prison. J Urban Health. 2006;83(6):1127–1131. doi: 10.1007/s11524-006-9095-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Lyons T, Goldstein P, Kiriazes J. HIV in correctional facilities: role of self-report in case identification. AIDS Patient Care STDS. 2006;20(2):93–96. doi: 10.1089/apc.2006.20.93. [DOI] [PubMed] [Google Scholar]
- 59.Macgowan R, Margolis A, Richardson-Moore A et al. Voluntary rapid human immunodeficiency virus (HIV) testing in jails. Sex Transm Dis. 2009;36(2, suppl):S9–S13. doi: 10.1097/OLQ.0b013e318148b6b1. [DOI] [PubMed] [Google Scholar]
- 60.McCusker J, Willis G, McDonald M, Sereti SM, Lewis BF, Sullivan JL. Community-wide HIV counselling and testing in central Massachusetts: who is retested and does their behavior change? J Community Health. 1996;21(1):11–22. doi: 10.1007/BF01682760. [DOI] [PubMed] [Google Scholar]
- 61.Oser CB, Smiley McDonald HM, Havens JR, Leukefeld CG, Webster JM, Cosentino-Boehm AL. Lack of HIV seropositivity among a group of rural probationers: explanatory factors. J Rural Health. 2006;22(3):273–275. doi: 10.1111/j.1748-0361.2006.00045.x. [DOI] [PubMed] [Google Scholar]
- 62.Poulin C, Alary M, Lambert G et al. Prevalence of HIV and hepatitis C virus infections among inmates of Quebec provincial prisons. CMAJ. 2007;177(3):252–256. doi: 10.1503/cmaj.060760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Rosen DL, Schoenbach VJ, Wohl DA, White BL, Stewart PW, Golin CE. Characteristics and behaviors associated with HIV infection among inmates in the North Carolina prison system. Am J Public Health. 2009;99(6):1123–1130. doi: 10.2105/AJPH.2007.133389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Sabin KM, Frey RL, Jr, Horsley R, Greby SM. Characteristics and trends of newly identified HIV infections among incarcerated populations: CDC HIV voluntary counseling, testing, and referral system, 1992–1998. J Urban Health. 2001;78(2):241–255. doi: 10.1093/jurban/78.2.241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Tartaro C, Levy MP. HIV Testing in Jail. AmericanJails. 2013:32–36. [Google Scholar]
- 66.White MC, Mehrotra A, Menendez E, Estes M, Goldenson J, Tulsky JP. Jail inmates and HIV care: provision of antiretroviral therapy and Pneumocystis carinii pneumonia prophylaxis. Int J STD AIDS. 2001;12(6):380–385. doi: 10.1258/0956462011923327. [DOI] [PubMed] [Google Scholar]
- 67.Harzke AJ, Ross MW, Scott DP. Predictors of post-release primary care utilization among HIV-positive prison inmates: a pilot study. AIDS Care. 2006;18(4):290–301. doi: 10.1080/09540120500161892. [DOI] [PubMed] [Google Scholar]
- 68.Althoff AL, Zelenev A, Meyer JP et al. Correlates of retention in HIV care after release from jail: results from a multi-site study. AIDS Behav. 2013;17(suppl 2):S156–S170. doi: 10.1007/s10461-012-0372-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Khawcharoenporn T, Zawitz C, Young JD, Kessler HA. Continuity of care in a cohort of HIV-infected former jail detainees. J Correct Health Care. 2013;19(1):36–42. doi: 10.1177/1078345812458246. [DOI] [PubMed] [Google Scholar]
- 70.Farley JL, Mitty JA, Lally MA et al. Comprehensive medical care among HIV-positive incarcerated women: the Rhode Island experience. J Womens Health Gend Based Med. 2000;9(1):51–56. doi: 10.1089/152460900318966. [DOI] [PubMed] [Google Scholar]
- 71.Zaller ND, Holmes L, Dyl AC et al. Linkage to treatment and supportive services among HIV-positive ex-offenders in Project Bridge. J Health Care Poor Underserved. 2008;19(2):522–531. doi: 10.1353/hpu.0.0030. [DOI] [PubMed] [Google Scholar]
- 72.Warren N, Bellin E, Zoloth S, Safyer S. Human immunodeficiency virus infection care is unavailable to inmates on release from jail. Arch Fam Med. 1994;3(10):894–898. doi: 10.1001/archfami.3.10.894. [DOI] [PubMed] [Google Scholar]
- 73.Rich JD, Holmes L, Salas C et al. Successful linkage of medical care and community services for HIV-positive offenders being released from prison. J Urban Health. 2001;78(2):279–289. doi: 10.1093/jurban/78.2.279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Fontana L, Beckerman A. Recently released with HIV/AIDS: primary care treatment needs and experiences. J Health Care Poor Underserved. 2007;18(3):699–714. doi: 10.1353/hpu.2007.0058. [DOI] [PubMed] [Google Scholar]
- 75.Baillargeon JG, Giordano TP, Harzke AJ, Baillargeon G, Rich JD, Paar DP. Enrollment in outpatient care among newly released prison inmates with HIV infection. Public Health Rep. 2010;125(suppl 1):64–71. doi: 10.1177/00333549101250S109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Westergaard RP, Kirk GD, Richesson DR, Galai N, Mehta SH. Incarceration predicts virologic failure for HIV-infected injection drug users receiving antiretroviral therapy. Clin Infect Dis. 2011;53(7):725–731. doi: 10.1093/cid/cir491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Wohl DA, Scheyett A, Golin CE et al. Intensive case management before and after prison release is no more effective than comprehensive pre-release discharge planning in linking HIV-infected prisoners to care: a randomized trial. AIDS Behav. 2011;15(2):356–364. doi: 10.1007/s10461-010-9843-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Beckwith C, Bazerman L, Gillani F et al. The feasibility of implementing the HIV seek, test, and treat strategy in jails. AIDS Patient Care STDS. 2014;28(4):183–187. doi: 10.1089/apc.2013.0357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Clements-Nolle K, Marx R, Pendo M, Loughran E, Estes M, Katz M. Highly active antiretroviral therapy use and HIV transmission risk behaviors among individuals who are HIV infected and were recently released from jail. Am J Public Health. 2008;98(4):661–666. doi: 10.2105/AJPH.2007.112656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Springer SA, Pesanti E, Hodges J, Macura T, Doros G, Altice FL. Effectiveness of antiretroviral therapy among HIV-infected prisoners: reincarceration and the lack of sustained benefit after release to the community. Clin Infect Dis. 2004;38(12):1754–1760. doi: 10.1086/421392. [DOI] [PubMed] [Google Scholar]
- 81.Meyer JP, Zelenev A, Wickersham JA, Williams CT, Teixeira PA, Altice FL. Gender disparities in HIV treatment outcomes following release from jail: results from a multicenter study. Am J Public Health. 2014;104(3):434–441. doi: 10.2105/AJPH.2013.301553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Arriola KR, Braithwaite RL, Kennedy S et al. A collaborative effort to enhance HIV/STI screening in five county jails. Public Health Rep. 2001;116(6):520–529. doi: 10.1016/S0033-3549(04)50084-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Baillargeon J, Borucki MJ, Zepeda S, Jenson HB, Leach CT. Antiretroviral prescribing patterns in the Texas prison system. Clin Infect Dis. 2000;31(6):1476–1481. doi: 10.1086/317478. [DOI] [PubMed] [Google Scholar]
- 84.Menezes P, Rosen D, Wohl DA et al. Low prevalence of antiretroviral resistance among HIV type 1-positive prisoners in the Southeast United States. AIDS Res Hum Retroviruses. 2013;29(1):136–141. doi: 10.1089/aid.2012.0102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Mostashari F, Riley E, Selwyn PA, Altice FL. Acceptance and adherence with antiretroviral therapy among HIV-infected women in a correctional facility. J Acquir Immune Defic Syndr Hum Retrovirol. 1998;18(4):341–348. doi: 10.1097/00042560-199808010-00005. [DOI] [PubMed] [Google Scholar]
- 86.Bingham JT. Federal Bureau of Prisons HIV consultant pharmacist monitoring and advisory program. J Am Pharm Assoc (2003) 2012;52(6):798–801. doi: 10.1331/JAPhA.2012.10208. [DOI] [PubMed] [Google Scholar]
- 87.Wohl DA, Stephenson BL, Golin CE et al. Adherence to directly observed antiretroviral therapy among human immunodeficiency virus–infected prison inmates. Clin Infect Dis. 2003;36(12):1572–1576. doi: 10.1086/375076. [DOI] [PubMed] [Google Scholar]
- 88.Pai NP, Estes M, Moodie EE, Reingold AL, Tulsky JP. The impact of antiretroviral therapy in a cohort of HIV-infected patients going in and out of the San Francisco county jail. PLoS ONE. 2009;4(9):e7115. doi: 10.1371/journal.pone.0007115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Altice FL, Mostashari F, Friedland GH. Trust and the acceptance of and adherence to antiretroviral therapy. J Acquir Immune Defic Syndr. 2001;28(1):47–58. doi: 10.1097/00042560-200109010-00008. [DOI] [PubMed] [Google Scholar]
- 90.Griffin MM, Ryan JG, Briscoe VS, Shadle KM. Effects of incarceration on HIV-infected individuals. J Natl Med Assoc. 1996;88(10):639–644. [PMC free article] [PubMed] [Google Scholar]
- 91.Kirkland LR, Fischl MA, Tashima KT et al. Response to lamivudine-zidovudine plus abacavir twice daily in antiretroviral-naive, incarcerated patients with HIV infection taking directly observed treatment. Clin Infect Dis. 2002;34(4):511–518. doi: 10.1086/338400. [DOI] [PubMed] [Google Scholar]
- 92.Stephenson BL, Wohl DA, Golin CE, Tien HC, Stewart P, Kaplan AH. Effect of release from prison and re-incarceration on the viral loads of HIV-infected individuals. Public Health Rep. 2005;120(1):84–88. doi: 10.1177/003335490512000114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Meyer JP, Qiu J, Chen NE, Larkin GL, Altice FL. Emergency department use by released prisoners with HIV: an observational longitudinal study. PLoS ONE. 2012;7(8):e42416. doi: 10.1371/journal.pone.0042416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Springer SA, Chen S, Altice FL. Improved HIV and substance abuse treatment outcomes for released HIV-infected prisoners: the impact of buprenorphine treatment. J Urban Health. 2010;87(4):592–602. doi: 10.1007/s11524-010-9438-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Reznick OG, McCartney K, Gregorich SE, Zack B, Feaster DJ. An ecosystem-based intervention to reduce HIV transmission risk and increase medication adherence among inmates being released to the community. J Correct Health Care. 2013;19(3):178–193. doi: 10.1177/1078345813486442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Baillargeon J, Giordano TP, Rich JD et al. Accessing antiretroviral therapy following release from prison. JAMA. 2009;301(8):848–857. doi: 10.1001/jama.2009.202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Devereux PG, Whitley R, Ragavan A. Discharge planning for inmates with HIV/AIDS: can it help increase adherence to medical treatment and lower recidivism? Corrections Today. 2002;64(6):127–129. [Google Scholar]
- 98.Meyer JP, Cepeda J, Wu J, Trestman RL, Altice FL, Springer SA. Optimization of human immunodeficiency virus treatment during incarceration: viral suppression at the prison gate. JAMA Intern Med. 2014;174(5):721–729. doi: 10.1001/jamainternmed.2014.601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Spaulding AC, Messina LC, Kim BI et al. Planning for success predicts virus suppressed: results of a non-controlled, observational study of factors associated with viral suppression among HIV-positive persons following jail release. AIDS Behav. 2013;17(suppl 2):S203–S211. doi: 10.1007/s10461-012-0341-8. [DOI] [PubMed] [Google Scholar]
- 100. Costa M, Montague B. Linkage to HIV care on release from incarceration: data from the LINCS Project 2010–2012 in RI and NC. Oral presentation at: 7th Academic and Health Policy Conference on Correctional Health; March 21, 2014; Houston, TX.
- 101. Bina C. Bureau of Prisons national HIV clinical pharmacist consultant program. Poster presented at: American Conference for the Treatment of HIV; September 16, 2005; Atlanta, GA.
- 102.Hammett TM. HIV/AIDS and other infectious diseases among correctional inmates: transmission, burden, and an appropriate response. Am J Public Health. 2006;96(6):974–978. doi: 10.2105/AJPH.2005.066993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Atlanta, GA: Centers for Disease Control and Prevention; 2009. HIV testing implementation guidance for correctional settings; pp. 1–38. [Google Scholar]
- 104.Solomon L, Montague BT, Beckwith CG et al. Survey finds that many prisons and jails have room to improve HIV testing and coordination of postrelease treatment. Health Aff (Millwood) 2014;33(3):434–442. doi: 10.1377/hlthaff.2013.1115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Varghese B, Peterman TA. Cost-effectiveness of HIV counseling and testing in US prisons. J Urban Health. 2001;78(2):304–312. doi: 10.1093/jurban/78.2.304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Wong MT. HIV care in correctional settings is cost-effective and improves medical outcomes. Infect Dis Clin Pract. 2001;10(suppl 1):S9–S15. [Google Scholar]
- 107.Hall HI, Gray KM, Tang T, Li J, Shouse L, Mermin J. Retention in care of adults and adolescents living with HIV in 13 US areas. J Acquir Immune Defic Syndr. 2012;60(1):77–82. doi: 10.1097/QAI.0b013e318249fe90. [DOI] [PubMed] [Google Scholar]
- 108.Booker CA, Flygare CT, Solomon L et al. Linkage to HIV care for jail detainees: findings from detention to the first 30 days after release. AIDS Behav. 2013;17(suppl 2):S128–S136. doi: 10.1007/s10461-012-0354-3. [DOI] [PubMed] [Google Scholar]
- 109.Chitsaz E, Meyer JP, Krishnan A et al. Contribution of substance use disorders on HIV treatment outcomes and antiretroviral medication adherence among HIV-infected persons entering jail. AIDS Behav. 2013;17(suppl 2):S118–S127. doi: 10.1007/s10461-013-0506-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Brinkley-Rubinstein L, Turner WL. Health impact of incarceration on HIV-positive African American males: a qualitative exploration. AIDS Patient Care STDS. 2013;27(8):450–458. doi: 10.1089/apc.2012.0457. [DOI] [PubMed] [Google Scholar]
- 111.Rich JD, McKenzie M, Shield DC et al. Linkage with methadone treatment upon release from incarceration: a promising opportunity. J Addict Dis. 2005;24(3):49–59. doi: 10.1300/J069v24n03_04. [DOI] [PubMed] [Google Scholar]
- 112.Copenhaver MM, Tunku N, Ezeabogu I et al. Adapting an evidence-based intervention targeting HIV-infected prisoners in Malaysia. AIDS Res Treat. 2011;2011:131045. doi: 10.1155/2011/131045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Jordan AO, Cohen LR, Harriman G, Teixeira PA, Cruzado-Quinones J, Venters H. Transitional care coordination in New York City jails: facilitating linkages to care for people with HIV returning home from Rikers Island. AIDS Behav. 2013;17(suppl 2):S212–S219. doi: 10.1007/s10461-012-0352-5. [DOI] [PubMed] [Google Scholar]
- 114.Koester KA, Morewitz M, Pearson C et al. Patient navigation facilitates medical and social services engagement among HIV-infected individuals leaving jail and returning to the community. AIDS Patient Care STDS. 2014;28(2):82–90. doi: 10.1089/apc.2013.0279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Patel K, Boutwell A, Brockmann BW, Rich JD. Integrating correctional and community health care for formerly incarcerated people who are eligible for Medicaid. Health Aff (Millwood) 2014;33(3):468–473. doi: 10.1377/hlthaff.2013.1164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Palepu A, Tyndall MW, Chan K, Wood E, Montaner JS, Hogg RS. Initiating highly active antiretroviral therapy and continuity of HIV care: the impact of incarceration and prison release on adherence and HIV treatment outcomes. Antivir Ther. 2004;9(5):713–719. [PubMed] [Google Scholar]
- 117.Gardner EM, McLees MP, Steiner JF, Del Rio C, Burman WJ. The spectrum of engagement in HIV care and its relevance to test-and-treat strategies for prevention of HIV infection. Clin Infect Dis. 2011;52(6):793–800. doi: 10.1093/cid/ciq243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Hall HI, Frazier EL, Rhodes P et al. Differences in human immunodeficiency virus care and treatment among subpopulations in the United States. JAMA Intern Med. 2013;173(14):1337–1344. doi: 10.1001/jamainternmed.2013.6841. [DOI] [PubMed] [Google Scholar]
- 119.Meyer JP, Cepeda J, Springer SA, Wu J, Trestman RL, Altice FL. HIV in people reincarcerated in Connecticut prisons and jails: an observational cohort study. Lancet HIV. 2014;1(2):e77–e84. doi: 10.1016/S2352-3018(14)70022-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Milloy MJ, Kerr T, Buxton J et al. Dose–response effect of incarceration events on nonadherence to HIV antiretroviral therapy among injection drug users. J Infect Dis. 2011;203(9):1215–1221. doi: 10.1093/infdis/jir032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121. National Institute on Drug Abuse. Seek, test, treat and retain: addressing HIV in the criminal justice system. National Institutes of Health, Research Portfolio Online Reporting Tools, RePORTER; 2013. Available at: http://www.drugabuse.gov/researchers/research-resources/data-harmonization-projects/seek-test-treat-retain/addressing-hiv-in-criminal-justice-system. Accessed April 2, 2015.
- 122.Khan MR, Behrend L, Adimora AA, Weir SS, Tisdale C, Wohl DA. Dissolution of primary intimate relationships during incarceration and associations with post-release STI/HIV risk behavior in a Southeastern city. Sex Transm Dis. 2011;38(1):43–47. doi: 10.1097/OLQ.0b013e3181e969d0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Milloy MJ, Buxton J, Wood E, Li K, Montaner JS, Kerr T. Elevated HIV risk behaviour among recently incarcerated injection drug users in a Canadian setting: a longitudinal analysis. BMC Public Health. 2009;9:156. doi: 10.1186/1471-2458-9-156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Morrow KM, Project SSG. HIV, STD, and hepatitis risk behaviors of young men before and after incarceration. AIDS Care. 2009;21(2):235–243. doi: 10.1080/09540120802017586. [DOI] [PubMed] [Google Scholar]
- 125.Wood E, Li K, Small W, Montaner JS, Schechter MT, Kerr T. Recent incarceration independently associated with syringe sharing by injection drug users. Public Health Rep. 2005;120(2):150–156. doi: 10.1177/003335490512000208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Stein MS, Spaulding AC, Cunningham M et al. HIV-positive and in jail: race, risk factors, and prior access to care. AIDS Behav. 2013;17(suppl 2):S108–S117. doi: 10.1007/s10461-012-0340-9. [DOI] [PubMed] [Google Scholar]
- 127.Kerr T, Marshall A, Walsh J et al. Determinants of HAART discontinuation among injection drug users. AIDS Care. 2005;17(5):539–549. doi: 10.1080/09540120412331319778. [DOI] [PubMed] [Google Scholar]