

Abstract
Mindless eating, or eating while distracted by surrounding stimuli, leads to overeating. The present study explored whether “mindless feeding,” or maternal distraction during bottle-feeding, is associated with greater infant formula/milk intakes and lower maternal sensitivity to infant cues. Mothers and their ≤24-week-old bottle-feeding infants (N=28) visited our laboratory for a video-recorded feeding observation. Infant intake was assessed by weighing bottles before and after the feedings. Maternal sensitivity to infant cues was objectively assessed by behavioral coding of video-records using the Nursing Child Assessment Feeding Scale. Maternal distraction was defined as looking away from the infant >75% of the feeding; using a mobile device; conversing with another adult; or sleeping. Twenty-nine percent (n=8) of mothers were distracted. While differences in intakes for infants of distracted vs. not distracted mothers did not reach significance (p=0.24), the association between distraction and infant intake was modified by two dimensions of temperament: orienting/regulation capacity (p=0.03) and surgency/extraversion (p=0.04). For infants with low orienting/regulation capacity, infants of distracted mothers consumed more (177.1 ± 33.8 ml) than those of not distracted mothers (92.4 ± 13.8 ml). Similar findings were noted for infants with low surgency/extraversion (distracted: 140.6 ± 22.5 ml; not distracted: 78.4 ± 14.3 ml). No association between distraction and intake was seen for infants with high orienting/regulation capacity or surgency/extraversion. A significantly greater proportion of distracted mothers showed low sensitivity to infant cues compared to not distracted mothers (p=0.04). In sum, mindless feeding may interact with infant characteristics to influence feeding outcomes; further experimental and longitudinal studies are needed.
Keywords: mindless feeding, bottle-feeding, infant feeding practices, overfeeding, mother-infant interactions, mindless eating, obesity prevention
INTRODUCTION
Rates of childhood overweight and obesity have stabilized and even declined for certain age groups over the past decade (Ogden, Carroll, Kit, & Flegal, 2014). Despite these promising trends, the prevalence of overweight and obesity remains well above national health targets (U.S. Department of Health and Human Services: Office of Disease Prevention and Health Promotion; U.S. Department of Health and Human Services: Office of Disease Prevention and Health Promotion) as 32% of youth are either overweight or obese, and 17% are obese (Ogden et al., 2014). Additionally, over 7% of infants are classified as having a high weight-for-recumbent length (Ogden et al., 2014). Overweight and obesity track across the life-course (Baird et al., 2005), and infancy, in particular, has been highlighted as a critical period for determining later chronic disease risk (Institute of Medicine, 2011). These data suggest that evidence-based obesity prevention strategies are still relevant and should be focused on during the first few years of life.
One of the earliest postnatal risk factors is rapid weight gain during infancy (Druet et al., 2012), which is a strong predictor of later obesity (Dennison, Edmunds, Stratton, & Pruzek, 2006); higher blood pressure, fasting glucose levels, and fasting triglyceride concentrations and lower high density lipoprotein (HDL) cholesterol levels (Ekelund et al., 2007); higher waist circumference (Sacco, de Castro, Euclydes, Souza, & Rondo, 2013), and non-alcoholic fatty liver disease (Breij, Kerkhof, & Hokken-Koelega, 2014). Given that infants are primarily dependent on their caregivers, and most often their mothers (Demaris, Mahoney, & Pargament, 2013; Nystrom & Ohrling, 2004), to determine when, where, what, and sometimes even how much, will be consumed, consideration of mother-infant interactions and the impact of mothers’ feeding practices on infant feeding and weight status outcomes, is a logical starting point for understanding predictors of rapid weight gain during infancy.
A recent Institute of Medicine (IOM) report outlines several recommendations for reducing risk for rapid weight gain during infancy, one of which encourages measures to help caregivers recognize and feed in response to infant hunger and fullness cues, especially during bottle-feeding (Institute of Medicine, 2011). Indeed, previous studies have suggested that mothers with lower responsiveness to infant cues have infants with greater weight gain across infancy (Blissett & Farrow, 2007; C. Farrow & Blissett, 2006; C. V. Farrow & Blissett, 2008; Worobey, Lopez, & Hoffman, 2009), but few studies have examined predictors of low maternal responsiveness (Brown & Lee, 2011) or have directly assessed the impact of mothers’ lack of responsiveness on infant intake and weight gain trajectories (DiSantis, Hodges, Johnson, & Fisher, 2011). Thus, our current understanding of how to promote responsive feeding practices during infant-feeding interactions is limited.
Although there may be many reasons for why a mother would feed in a way that is not responsive to an infant’s cues (Brown & Lee, 2013; Brown, Raynor, & Lee, 2011; Stifter, Anzman-Frasca, Birch, & Voegtline, 2011), one reason that, to our knowledge, has not been explored is the possibility that maternal distraction, or the tendency of the mother to pay attention to stimuli other than her infant during feeding interactions, impairs mothers’ abilities to recognize and feed in response to infants’ hunger and fullness cues. A substantial body of research illustrates that older children and adults who engage in “mindless eating,” or eating while distracted, tend to consume more food than those who concentrate solely on their food (Wansink, 2006). Individuals who are distracted by other tasks, computers, television, work, or driving (Wansink, 2006), tend to rely on external cues to dictate when they should stop eating (e.g., when the episode of a TV show they are watching ends), rather than on their internal cues of hunger and fullness (Wansink, Payne, & Chandon, 2007). They also tend to report feeling less satiated than non-distracted individuals after eating the same amount of food (Brunstrom & Mitchell, 2006), and thus continue to eat in the absence of hunger (McKetta & Rich, 2011; Wansink et al., 2007). As follows, it is possible that caregivers who engage in “mindless feeding,” or who are distracted while feeding their infants, would be less sensitive to their infants’ cues and at higher risk for overfeeding.
It is also possible, however, that certain infants would be more impacted by a lack of maternal attention during feeding than others, as previous research has highlighted several factors that increase risk for overfeeding. For example, satiety responsiveness declines with age, which may be due to learned tendencies to overeat (Birch, Fisher, & Davison, 2003; Jansen, 1998). Furthermore, infants with certain temperament characteristics, such as higher negativity (Anzman-Frasca, Stifter, & Birch, 2012; Slining, Adair, Goldman, Borja, & Bentley, 2009), surgency/extraversion [a precursor to later impulsivity (Burton et al., 2011; Rothbart, Ahadi, Hershey, & Fisher, 2001)], or lower orienting/regulation capacity [an early manifestation of poor self-regulation skills (Francis & Susman, 2009; Graziano, Calkins, & Keane, 2010; Tan & Holub, 2011; Wells et al., 1997)] are at higher risk for rapid weight gain and later obesity, which may be due, in part, to poor self-regulatory abilities. Thus, it is possible that caregiver attention to infant feeding behaviors may be especially critical to ensure these infants do not over-feed.
The objective of the present study was to assess the association between maternal distraction during infant feeding interactions and feeding outcomes. The first aim of this study was to explore: 1) whether mothers who were distracted while feeding their infants would feed their infants more formula or milk than mothers who were not distracted, and 2) whether infant characteristics (e.g., age or temperament) would moderate the association between distraction and infant intake. The second aim of this study was to assess whether mothers who were distracted would show lower levels of sensitivity to their infants’ cues compared to mothers who were not distracted.
METHODS
Participants
Twenty-eight bottle-feeding mothers and their healthy, full-term infants participated in an experimental infant-feeding study [data reported elsewhere; (Ventura & Golen, 2015)]. The present study is a secondary analysis of data from the control condition, which was designed to reflect a typical bottle-feeding interaction. Twenty-five of these dyads were exclusively (n = 22) or predominantly (>80% of feeds; n = 3) formula-feeding; three fed breast milk from a bottle on a regular basis. An additional infant was tested but not included in the present study because she was ill during the visit (n=1). Infants were eligible if they were between 0 and 6 months of age, had the experience of feeding from a bottle, and had not yet been introduced to solid foods. Infants were excluded if they were preterm or if they had medical conditions that interfered with feeding. Mothers were eligible if they were between 18 and 40 years of age, and did not have gestational diabetes or any complications during pregnancy and/or birth that may have resulted in their infants having problems feeding. Participants were recruited through fliers posted in Women, Infant & Children (WIC) offices, libraries, coffee shops, and pediatric offices around Philadelphia. They were also recruited through an advertisement in a local parenting magazine. Mothers were compensated a total of $95.00 for completing the study. All study procedures were approved by the Office of Regulatory Affairs at Drexel University. The parent study was registered at clinicaltrials.gov (NCT02111694).
Procedures
Upon arrival to our laboratory, infants were changed into a standard onesie. Infants’ weight and length and mothers’ weight and height measurements were then collected and recorded in triplicate. Infant anthropometric data was later normalized to z-scores using the World Health Organization (WHO) Anthro software version 3.0.1 (http://who.int/childgrowth/en/); age- and sex-specific percentiles were calculated based on these z-scores.
When the infant began to display hunger cues (e.g., crying, fussing, or putting his or her hand to his or her mouth) and the mother indicated she was ready to begin the feeding, a trained research assistant prepared the infant’s typical formula or milk in either a 4-ounce or 8-ounce glass bottle with a low-flow nipple (Evenflo, Ohio USA). Bottle-size and amount offered were determined by the mother’s report of her infant’s typical bottle size and amount consumed.
Mothers were instructed to feed their infants exactly as they would at home, and to tell the researcher when they were ready to start the feed and end the feed by stating “I would like to start the feed now,” and “I would like to end the feed now.” The entire feeding session was video-recorded using a Canon VIXIA HF M40 Full HD Camcorder (Canon, New York, USA). The video camera was placed approximately 10 to 12 feet from the mother-infant dyads. Infant intake was assessed by weighing the bottle before and after the feeding using a top-loading balance (Mettler Toledo MS3002S NewClassic, Greifensee, Switzerland).
Mothers also completed a demographics questionnaire and the Infant Behavior Questionnaire-Revised Very Short Form [Very Short Form-IBQ-R (Gartstein & Rothbart, 2003; Putnam, Helbig, Gartstein, Rothbart, & Leerkes, 2014)]. This 37-item form is an abbreviated version of the 184-item standard IBQ-R, which assesses mothers’ perceptions of infant temperament based on the infant’s behaviors as they relate to reactivity and self-regulation in the first year postpartum (Gartstein & Rothbart, 2003). The 37 items represent 16 scales, which are further reduced into three dimensions of infant temperament: surgency/extraversion, orienting/regulation capacity, and negative affectivity. Surgency/extraversion is represented by the Approach, Vocal Reactivity, High Intensity Pleasure, Smiling and Laughter, Activity Level, and Perceptual Sensitivity scales (α = 0.92). Negative affectivity is represented by the Sadness, Distress to Limitations, Fear, and Falling Reactivity scales (α = 0.91). Orienting/regulation capacity is represented by the Low Intensity Pleasure, Cuddliness/Affiliation, Duration of Orienting, and Soothability scales (α = 0.91).
Analysis of Video Records
Videos were recorded onto Secure Digital cards (SanDisk, California, USA), and then imported into an event recorder program (Observer XT, version 10.5; Noldus Information Technology, Heerlen, the Netherlands). Later analysis of the videos allowed for classification of mothers who engaged in distracted feeding. Distracted feeding was defined as engaging in one or more of the following behaviors during the feeding observation: 1) looking somewhere other than at the infant for more than 75% of the feeding; 2) using a cell-phone or smart phone (including talking, texting or using apps); 3) engaging in full conversations with someone else in the room other than the infant; and 4) falling asleep.
Mother and infant behavior during each feeding was coded using the Nursing Child Assessment Feeding Scale [NCAFS; (Sumner & Spitz, 1994)]. There are six subscales within this scale, which include four caregiver attributes (Sensitivity to Cues, Response to Child’s Distress, Social-Emotional Growth Fostering, and Cognitive Growth Fostering) and two infant attributes (Clarity of Cues and Responsiveness to Caregiver). The present study focused on the Sensitivity to Cues subscale of NCAFS, which measures the degree to which the mother or caregiver is able to understand and respond appropriately and in a timely manner to her infant’s cues (Sumner & Spitz, 1994). A mother who displays sensitivity to her infants’ cues increases the quality of the feeding interaction between her and her infant, and teaches her infant that he or she is valued and has an impact on his or her surroundings (Sumner & Spitz, 1994).
A total of 28 mother-infant feeding dyad videos were observed and analyzed by four individuals whom, prior to the start of coding, attended a three full-day intensive training. Throughout the training, all subscales and definitions within subscales were explained and reviewed by a certified NCAFS-trainer to ensure their understanding and proper application. In addition, coders were given several practice opportunities to code sample mother-infant dyad feeding videos using NCAFS scoring sheets. Once all coders successfully passed the final training examination, inter- and intra-rater reliability was established with an 86% and 90% consistency, respectively. Inter-rater reliability was determined by the cross-coding of three videos (11%) by all four coders, and five videos (18%) by two coders. Each rater double-coded five videos to determine intra-rater reliability. Coding occurred over the course of four months. Coders met regularly to explore and resolve questions and concerns that arose during the course of coding.
Data Collection and Management
Study data were collected and managed using REDCap electronic data capture tools hosted at Drexel University (Harris et al., 2009). REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies, providing: 1) an intuitive interface for validated data entry; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for importing data from external sources. (Harris et al., 2009)
Statistical Analyses
We used SAS v.9.4 (SAS Institute Inc. North Carolina, USA) to analyze all data. Prior to data analysis, data were thoroughly cleaned and assessed for normality. The first aim of this study was to assess: 1) whether mothers who were distracted during the feeding interaction our laboratory would feed them more formula or milk than mothers who were not distracted, and 2) whether infant characteristics (e.g., age or temperament) would moderate the association between distraction and intake. To address this aim, Analysis of Covariance (ANCOVA) was used to assess the association between distraction and the amount of formula/milk infants consumed, while controlling for infant age and hunger index (calculated as [amount consumed at last feeding / time since last feeding]). To explore whether infant characteristics moderated the associations between maternal distraction and amount of formula/milk infants consumed, infant age and temperament dimensions (negative affectivity, orienting/regulation capacity, and surgency/extraversion) were first dichotomized using median splits. We then included each of these variables into separate models testing the association between distraction and infant intake. Moderation was determined by a significant interaction between distraction and each variable. The second aim of this study was to assess whether mothers who were distracted versus those who were not distracted would show lower levels of sensitivity to their infant cues. To address this aim, we used median splits to classify mothers as high versus low on the Sensitivity to Infant Cues subscale of NCAFS. Fisher’s exact test was then used to determine whether greater proportions of distracted mothers scored lower on the Sensitivity to Cues subscale. Where applicable, effect sizes were estimated using partial eta squared [η2p; (Lakens, 2013)]. Results are presented as means or least squared means ± standard deviations or standard errors. We used p < 0.05 as a criterion for statistical significance of main and interaction effects. Additionally, because this was an exploratory study with a small sample size, we also noted statistical trends (p < 0.10).
RESULTS
Sample Characteristics
Sample characteristics are presented in Table 1. Sixty percent of infants were female. Infants had a mean age of 2.8 ± 1.7 months (11.2 ± 6.8 weeks) upon study entry, with a mean weight-for-length percentile of 75.2 ± 24.8 and weight-for-length z-score of 2.1 ± 0.7. The majority of infants consumed partial protein-hydrolysate formula (pPHF; 43%, n=12). Lesser proportions of infants consumed cow’s milk formula (CMF; 25%), soy-protein formula (SPF; 21%), and breast milk (11%). Average age of mothers was 26.9 ± 6.9 years and pre-pregnancy BMI was 31.7 ± 6.2. The majority of mothers (91.7%) received federal assistance (e.g., WIC benefits) and 60.7% had a family income of <$15,000 per year. The percentage of mothers with no college education or vocational degree was 60.7%. Seventy-six percent of mothers were non-Hispanic Black, and 75% were not married. The majority of mothers had three or fewer children (one child: 28%, two children: 28%, three children: 16%).
Table 1.
Percent (n) or Mean ± SD Values for Sample Characteristics (N=28)
| Infant Characteristics: | |
| Sex, % female | 60.0 (15) |
| Age at study entry, months | 2.8 ± 1.7 |
| Birth weight-for-length percentile | 39.0 ± 39.4 |
| Weight-for-length percentile at study entry | 75.2 ± 24.8 |
| Type of milk/formula consumed during study | |
| Breast Milk | 11 (3) |
| pPHF | 43 (12) |
| SPF | 21 (6) |
| CMF | 25 (7) |
| Maternal/Familial Characteristics: | |
| Age, years | 26.9 ± 6.9 |
| Pre-Pregnancy BMI, kg/m2 | 31.2 ± 8.3 |
| Received Federal Assistance (WIC) | 91.7 (22) |
| Family Income, % <$15,000/year | 60.7 (17) |
| Level of Education, % High School Only | 60.7 (17) |
| Racial/Ethnic Category | |
| Non-Hispanic White | 12 (3) |
| Non-Hispanic Black | 76 (19) |
| Hispanic Black | 12 (3) |
| Marital Status, % Married | 25 (7) |
| Parity, % Primiparous | 28 (7) |
Abbreviations: CMF, cow’s milk formula; pPHF, partial protein hydrolysate formula; SPF, soy-protein formula.
Association between maternal distraction and infant intake
Eight of the 28 mothers tested (28.6%) were classified as distracted. There was no association between distraction and infant formula/milk consumption (distracted: 133.4 ml ± 18.6 ml vs. not distracted: 111.2 ml ± 11.7 ml, F[1, 25] = 1.01, p = 0.24, η2p = 0.04).
Infant age and temperament dimensions were explored as possible moderators of the association between maternal distraction and infant intake. Before inclusion of these variables as possible moderators, the association of each variable with infant intake was assessed. There was no association between formula type and the amount consumed (CMF: 139.1 ± 19.4 ml; pPHF: 113.0 ± 15.4 ml; SPF: 126.8 ± 24.7 ml, F[3, 23] = 1.47, p = 0.25, η2p = 0.16). There was, however, a trend towards infants consuming significantly less when breast-milk was in the bottle compared to formula (breast milk: 67.5 ± 28.9 ml vs. formula: 123.6 ± 10.0 ml; F[1, 25] = 3.37, p = 0.08, η2p = 0.12). In addition, there was a significant association between age and amount consumed in that younger infants (1.6 to 10.9 weeks of age: 93.9 ± 12.6 ml) consumed significantly less than older infants (11 to 24 weeks of age: 141.3 ± 12.6 ml; F[1, 25] = 7.01, p = 0.01, η2p = 0.22). There was no association between mothers’ perceptions of infants’ negative affectivity (F[1, 25] = 0.01, p = 0.93, η2p = 0.00) or orienting/regulation capacity (F[1, 25] = 1.77, p=0.20, η2p = 0.06) and amount consumed. Conversely, infants classified as high on surgency/extraversion consumed significantly more than infants classified as low on surgency/extraversion (138.8 ± 12.9 ml vs. 96.3 ± 12.9 ml, respectively; F[1, 25] = 5.40, p = 0.03, η2p = 0.18).
In tests examining whether any of the above characteristics modified the association between maternal distraction and infant intake, the possible interaction between breast milk versus formula and distraction could not be tested because none of the mothers feeding breast-from a bottle were classified as distracted. When analyses were limited to mothers who fed their infants formula, there was no interaction between formula type and distraction (F[2, 20] = 0.75, p = 0.49, η2p = 0.07). There was a trend toward an interaction between distraction and infant age (F[1, 23]=3.93, p = 0.06, η2p = 0.15; Figure 1). Post-hoc comparisons revealed that when infants were younger (1.6–10.9 weeks of age) there was no association between maternal distraction and infant intake (distracted: 94.5 ± 23.0 ml, not distracted: 95.0 ± 14.5 ml, p = 0.99). In contrast, older infants (11–24 weeks of age) of distracted mothers trended toward consuming more than older infants of mothers who were not distracted (distracted: 174.4 ± 23.0 ml, not distracted: 126.7 ± 14.5 ml, p = 0.09).
Figure 1. Infant age trended towards moderating the association between maternal distraction and infant intake.
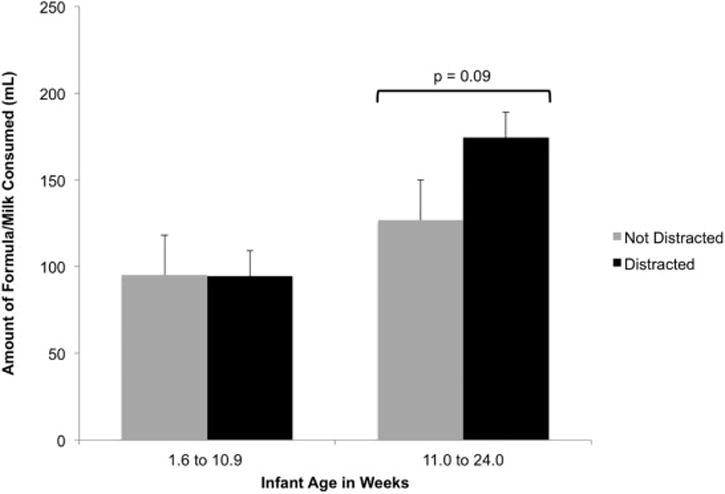
When infants were older (11–24 weeks of age), there was a trend towards infants of distracted mothers consuming more than infants whose mothers were not distracted (p = 0.09). Maternal distractedness was not associated with amount consumed for younger infants (1.6–10.9 weeks of age; p = 0.99).
The association between maternal distraction and infant intake was also modified by two dimensions of mothers’ perceptions of infant temperament: orienting/regulation capacity (F[1, 23] = 5.53, p = 0.03 for the interaction, η2p = 0.19; Figure 2) and surgency/extraversion (F[1, 23]=4.59, p = 0.04 for the interaction, η2p = 0.17; Figure 3). With respect to orienting/regulation capacity, when infants had low levels of orienting/regulation capacity, those whose mothers were distracted consumed significantly more formula than those whose mothers were not distracted (177.1 ml ± 33.8 ml vs. 92.4 ml ± 13.8 ml, p = 0.03). In contrast, when infants had high levels of orienting/regulation capacity, the association between maternal distraction and infant intake was not significant (p = 0.44). In addition, when mothers were not distracted, infants who were low in orienting/regulation capacity consumed significantly less than infants who were high in orienting/regulation capacity (92.4 ml ± 13.8 ml vs. 139.3 ml ± 16.9 ml, p = 0.04). With respect to surgency/extraversion, for infants with low levels of surgency/extraversion, those whose mothers were distracted consumed significantly more than those whose mothers were not distracted (140.6 ml ± 22.5 ml vs. 78.4 ml ± 14.3 ml p = 0.03, respectively). In addition there was no association between maternal distraction and infant intake when infants had high levels of surgency/extraversion (p = 0.54).
Figure 2. Mothers’ perception of infants’ orienting/regulation capacity moderates the association between maternal distraction and infant intake.
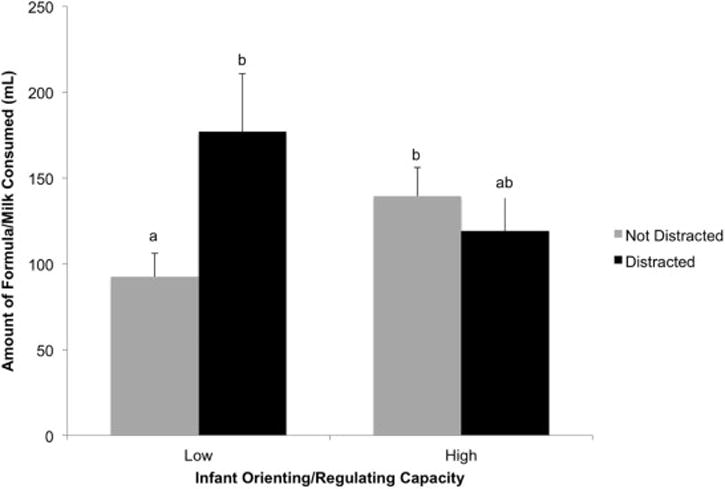
For infants low in orienting/regulation capacity (self-regulation skills), those whose mothers were distracted consumed significantly more formula/milk than infants whose mothers were not distracted (p = 0.03). However, when mothers were not distracted, infants who were low in orienting/regulation capacity consumed significantly less than infants who were high in orienting/regulation capacity (p = 0.04). Different letters between and among groups indicate significant differences in amounts consumed (p < 0.05).
Figure 3. Mothers’ perception of infants’ surgency/extraversion moderates the association between maternal distraction and infant intake.
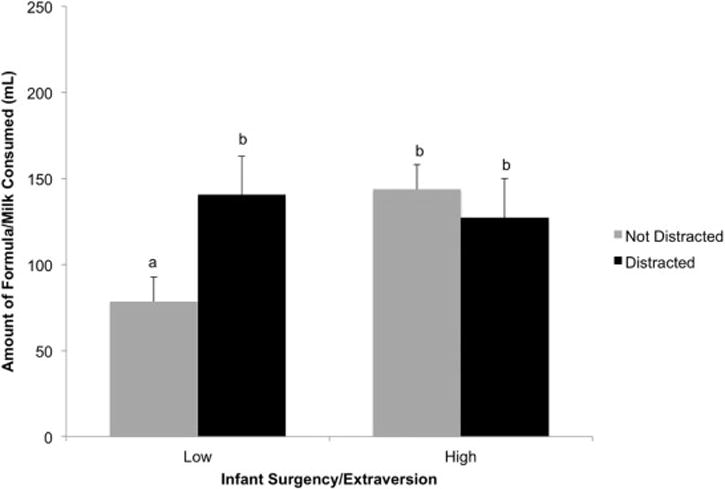
Among infants low in surgency/extraversion, formula/milk intake was significantly higher when mothers were distracted compared to when mothers were not distracted (p = 0.03). When infants were high in surgency/extraversion, there was no significant difference in formula/milk intake between infants of distracted versus not-distracted mothers (p = 0.54). Different letters between and among groups indicate significant differences in amounts consumed (p < 0.05).
Association Between Maternal Distraction and Maternal Sensitivity to Infant Cues
A significantly larger proportion of distracted mothers scored low on the Sensitivity to Cues subscale of NCAFS compared to mothers who were not distracted. Specifically, whereas 75% of distracted mothers scored low on the Sensitivity to Cues subscale, only 30% of mothers who were not distracted scored low on this subscale (p = 0.04, Fisher’s Exact Test).
DISCUSSION
The present study illustrates that mothers’ engagement in mindless feeding, or attention to environmental distractors during bottle-feeding, may interact with infant characteristics to influence feeding outcomes. These findings add to the existing body of research that attempts to identify which infants are at risk for rapid weight gain during infancy, a significant predictor of obesity later in life (Dennison et al., 2006; Druet et al., 2012), and highlight potential targets for prevention efforts. Whereas maternal distraction alone was not associated with greater formula/milk intake, infant characteristics including age, orienting/regulation capacity, and surgency/extraversion moderated the associations between distraction and formula/milk consumption.
In this study, older infants (11 to 24 weeks of age) whose mothers were distracted during bottle-feeding tended to consume more formula/milk than older infants whose mothers were not distracted. Conversely, maternal distraction was not associated with intakes for younger infants (1.6 to 10.9 weeks of age). One possible interpretation of this finding is that younger infants are better able to regulate their intake, regardless of their mothers’ attentiveness and sensitivity to their feeding cues. Conversely, older infants whose mothers are more distracted, and therefore, more disconnected and less responsive to their satiation cues during the feeding interaction, may learn to disregard their feelings of satiation and continue to eat when they are no longer hungry. This interpretation is supported by Worobey and colleagues (2009), who found that lower maternal sensitivity to infant feeding cues was associated with increased infant weight gain in older infants (24 to 48 weeks of age), but not in younger infants (12 to 24 weeks of age). Similarly, Birch and colleagues explored the development of eating in the absence of hunger in a longitudinal study of young girls and found that tendencies to eat in the absence of hunger significantly increased between ages 5 and 9 years for all girls, and that this change was significantly greater for girls whose mothers used restrictive feeding practices (Birch et al., 2003). The present study was cross-sectional and observational, thus cannot inform as to whether distracted feeding directly caused the development of poorer regulatory abilities for older infants. Further research using experimental and longitudinal designs, as well as infants with a wider range of ages, would provide insight into whether habitual maternal distraction during bottle-feeding leads to the development of poorer self-regulatory abilities and greater tendencies to eat in the absence of hunger for infants.
Another notable finding from this study was related to mothers’ perceptions of their infants’ orienting/regulation capacity, which is predictive of later effortful control, or the ability to maintain attentional focus and employ cognitive, behavioral, and emotional self-control (Rothbart, Ellis, Rueda, & Posner, 2003). Previous research suggests that young children with poorer global self-regulation or inhibition capacities (as reported by their mothers) tend to have poorer abilities to self regulate their energy intake and to have higher weight statuses than young children who are higher in global self-regulation or inhibition skills (Francis & Susman, 2009; Graziano et al., 2010; Tan & Holub, 2011). We did not find a main effect of infants’ orienting/regulation capacity on infant intake, however, when infants were low in orienting/regulation capacity, those whose mothers were distracted consumed significantly more formula/milk than those whose mothers were not distracted. One possible explanation for this finding is that distracted mothers of infants with low self-regulatory abilities were less aware than their not-distracted counterparts of their infants’ satiation signals and propensities to eat beyond fullness, leading them to overfeed. However, this interpretation does not take into account our findings that: 1) intakes of infants with low regulation/orienting capacity and distracted mothers were not statistically different from those of infants with higher regulation/orienting capacity, and 2) among mothers who were not distracted, infants with low regulation/orienting capacity consumed significantly less than infants with high regulation/orienting capacity. Given these findings, it is possible that, among mothers who were not distracted, those who perceived their infants to have low self-regulatory capacity were overly cautious with regard to how much they fed their infants, leading to underfeeding, whereas those who perceived their infants to have high orienting/regulation capacity were more trusting of their infants, and in effect exerted less control over the feed. This interpretation is consistent with previous studies showing that mothers who believe their infants are at risk for overeating and rapid weight gain are inclined to use more controlling and restrictive feeding practices (Brown & Lee, 2011; Francis, Hofer, & Birch, 2001). While the present study suggests that maternal distraction, or lack thereof, may interact with infants’ self-regulatory abilities to influence feeding outcomes, future experimental and longitudinal studies are needed to better understand this relationship.
Findings from the present study also illustrated that infants whose mothers rated them as high in surgency/extraversion consumed significantly more than those rated lower in this dimension of temperament. The surgency/extraversion subscale of the IBQ-R is comprised of measures of the infants’ level of approach, vocal reactivity, high intensity pleasure, smiling and laughter, activity level, and perceptual sensitivity. This subscale was adapted for infants from the Child Behavior Questionnaire’s (CBQ) impulsivity subscale (Gartstein & Rothbart, 2003), which defined impulsivity as the quickness of reactivity, or not thinking before taking action (Francis, Granger, & Susman, 2013). Thus, the items that comprise the surgency/extraversion subscale of the IBQ-R are intended to represent aspects of impulsivity that are developmentally appropriate to infants. For example, approach, which refers to positive excitement and quick movement towards enjoyable activities (Gartstein & Rothbart, 2003), indicates a lack of thought before action. Similarly, high intensity pleasure is indicative of seeking stimulation (Gartstein & Rothbart, 2003), another key element of impulsivity. Such indicators of impulsivity have been linked to overweight and obesity in samples of children between the ages of 3 and 15 years (Francis et al., 2013; Nederkoorn, Braet, Van Eijs, Tanghe, & Jansen, 2006). With respect to infancy, Burton et al. (2011) found that higher maternal perceived levels of infant surgency predicted accelerated rates of weight gain between birth to 3 months of age, but not beyond 3 to 12 months (Burton et al., 2011). These findings may indicate that impulsive tendencies in early life lead to greater difficulty refraining from the temptation to overeat energy dense foods when they are available (Nederkoorn et al., 2006). As such, infants and children who are impulsive may be at higher risk for over-consumption and eating in the absence of hunger, and therefore less able to self-regulate their energy intake (Burton et al., 2011).
In the present study, maternal distraction was associated with intakes for infants who were lower in surgency/extraversion, but not for infants who were higher in surgency/extraversion. When infants were lower in surgency/extraversion, those whose mothers were not distracted consumed significantly less formula/milk than infants whose mothers were distracted, as well as compared to infants who were high in surgency/extraversion with distracted and not-distracted mothers. Taken together, these findings may suggest that impulsive tendencies override physiological signals of fullness for surgent/extraverted infants, given their propensity toward enjoyable activities and stimulation from eating, making it challenging for even the most attentive mothers to feed in response to these infants’ satiation cues. Furthermore, when mothers of infants who are low in surgency are distracted, the intakes for these infants look more like those of infants who are high in surgency. Thus, reducing mothers’ level of distraction while feeding may be important for ensuring that infants who have lower levels of surgency/extraversion are not over-fed, whereas, interventions other than reducing mothers’ tendencies toward distracted feeding may be necessary to prevent overfeeding in surgent/extraverted infants. Alternatively, it is also possible that mothers of infants low in surgency/extraversion who were not distracted under-fed their infants relative to other infants; further research using experimental methods is necessary to understand mechanisms and causal associations between maternal distraction and infant intake in more versus less surgent/extraverted infants.
Findings from the present study also revealed that a significantly higher percentage of distracted mothers scored lower on the Sensitivity to Cues subscale of NCAFS than non-distracted mothers. This finding, while intuitive, is critical in understanding connections between distracted and responsive feeding. The finding that distracted feeders were more likely to be less sensitive to their infants’ hunger and satiation cues than non-distracted feeders is consistent with previous literature linking distracted eating to decreased awareness of, and hence less sensitivity, to internal cues of hunger and satiation, resulting in overeating [for a review see (Robinson et al., 2013)].
This study presents a novel and valuable exploration of maternal distraction during bottle-feeding interactions. However, this study is not without limitations, each of which could pave the way for additional studies exploring this topic. First, our sample was small in size and the majority was black, low-income women, with pre-pregnancy weight statuses that were higher than national averages [but similar to averages for low-income, Black populations; (May, Freedman, Sherry, & Blanck, 2013; Ogden et al., 2014)]. These sample characteristics may hinder our ability to generalize our findings to other populations. Second, we used a standardized nipple for all infants because it was required within the experimental design of our parent study (Ventura & Golen, 2015). It is possible, however, that not all infants were accustomed to this type of nipple, and instead would have been more comfortable using a fast-flow nipple, which perhaps created an unnatural circumstance for certain infants. Third, a large number of analyses were reported and this repeated testing might have increased our chance of finding significant effects. Fourth, it is also important to note that we do not have a clear definition of over- versus under-feeding upon which to base our conclusions. Thus, our conclusions and interpretations are limited to the comparison of amounts consumed among subgroups of infants and it remains unclear whether infant groups who consumed significantly less versus more were under or overfed, respectively. Finally, although we made every effort to make our laboratory as comfortable as possible, the novelty of the setting may have influenced mothers’ and infants’ behaviors during the feeding interaction.
CONCLUSIONS AND FUTURE DIRECTIONS
Rapid infant weight gain is a strong predictor of later obesity risk; (Druet et al., 2012; Ekelund et al., 2007) thus, effective targets for prevention efforts are needed to reverse the continued high prevalence of overweight and obesity in childhood (Ogden et al., 2014). Given the potential for mothers or caregivers to influence their infant’s eating behaviors through their feeding practices and styles, more insight into mothers’ feeding practices, and how to optimize them, is essential. The current study sought to evaluate the association between maternal distraction during feeding interactions and feeding outcomes, as well as to reveal potential predictors of which infants may be more affected by distracted feeding.
To our knowledge, this is the first study to explore maternal distraction during mother-infant feeding interactions, and has opened a new avenue for further research. Future studies evaluating distraction and infant feeding outcomes should, first and foremost, include larger sample sizes as well as more diverse samples to improve the generalizability of findings. Furthermore, future studies might benefit from utilizing a home-based setting, as opposed to the laboratory-based setting used in the present study, as well as allowing infants to feed from their own bottles to elicit more natural participant behaviors. Re-examining the hypotheses posed in the present study within an experimental design is essential in better understanding the direction of causation for associations between mothers’ distracted feeding and sensitivity to infants’ cues, and infants’ formula/milk intake, and could lead to novel education efforts targeting mothers most vulnerable to mindless feeding.
HIGHLIGHTS.
We examined maternal distraction during bottle-feeding and infant feeding outcomes.
Infant temperament moderated the association between distraction and infant intake.
Distraction was associated with intake when infants had lower regulatory capacity.
Distraction was also associated with intake when infants had lower surgency.
Distracted mothers were less sensitive to infant cues than not distracted mothers.
Acknowledgments
The project described was supported by a Drexel University College of Nursing and Health Professions Research Grant and by the Eunice Kennedy Shriver National Institute Of Child Health & Human Development of the National Institutes of Health under Award Number R03HD080730. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. We thank Linda Kilby PhD, RD, LDN and the staff at the Philadelphia WIC Program for their assistance with subject recruitment and the mothers and infants who participated in this study. We also thank Sean Banks, PhD for his technical assistance with REDCap, and Stella Volpe, PhD, RD, LDN, FACSM and Beth Leonberg, MS, MA, RD, CSP, LDN, FADA for their valuable feedback on a previous version of this manuscript.
Funding Source: The project described was supported by a Drexel University College of Nursing and Health Professions Research Grant and by the Eunice Kennedy Shriver National Institute Of Child Health & Human Development of the National Institutes of Health under Award Number R03HD080730. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Abbreviations
- IOM
Institute of Medicine
- TV
television
- WIC
Special Supplemental Nutrition Program for Women, Infants, and Children
- WHO
World Health Organization
- BMI
Body Mass Index
- IBQ-R
Infant Behavior Questionnaire-Revised Very Short Form
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflicts of Interest: The authors have no conflicts of interest to disclose.
Clinical Trial Registry: This trial was registered at clinicaltrials.gov as NCT02111694.
References
- Anzman-Frasca S, Stifter CA, Birch LL. Temperament and childhood obesity risk: a review of the literature. Journal of Developmental and Behavioral Pediatrics. 2012;33(9):732–745. doi: 10.1097/DBP.0b013e31826a119f. [DOI] [PubMed] [Google Scholar]
- Baird J, Fisher D, Lucas P, Kleijnen J, Roberts H, Law C. Being big or growing fast: systematic review of size and growth in infancy and later obesity. British Medical Journal. 2005;331(7522):929. doi: 10.1136/bmj.38586.411273.E0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Birch LL, Fisher JO, Davison KK. Learning to overeat: maternal use of restrictive feeding practices promotes girls’ eating in the absence of hunger. American Journal of Clinical Nutrition. 2003;78(2):215–220. doi: 10.1093/ajcn/78.2.215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blissett J, Farrow C. Predictors of maternal control of feeding at 1 and 2 years of age. Internaitonal Journal of Obesity (London) 2007;31(10):1520–1526. doi: 10.1038/sj.ijo.0803661. [DOI] [PubMed] [Google Scholar]
- Breij LM, Kerkhof GF, Hokken-Koelega AC. Accelerated infant weight gain and risk for nonalcoholic fatty liver disease in early adulthood. Journal of Clinical Endocrinology and Metabolism. 2014;99(4):1189–1195. doi: 10.1210/jc.2013-3199. [DOI] [PubMed] [Google Scholar]
- Brown A, Lee M. Maternal child-feeding style during the weaning period: association with infant weight and maternal eating style. Eating Behaviors. 2011;12(2):108–111. doi: 10.1016/j.eatbeh.2011.01.002. [DOI] [PubMed] [Google Scholar]
- Brown A, Lee M. Breastfeeding is associated with a maternal feeding style low in control from birth. PLoS One. 2013;8(1):e54229. doi: 10.1371/journal.pone.0054229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown A, Raynor P, Lee M. Maternal control of child-feeding during breast and formula feeding in the first 6 months post-partum. Journal of Human Nutrition and Dietetics. 2011;24(2):177–186. doi: 10.1111/j.1365-277X.2010.01145.x. [DOI] [PubMed] [Google Scholar]
- Brunstrom JM, Mitchell GL. Effects of distraction on the development of satiety. British Journal of Nutrition. 2006;96(4):761–769. [PubMed] [Google Scholar]
- Burton P, Wells JC, Kennedy K, Nicholl R, Khakoo A, Fewtrell MS. Association between infant correlates of impulsivity–surgency (extraversion)–and early infant growth. Appetite. 2011;57(2):504–509. doi: 10.1016/j.appet.2011.07.002. [DOI] [PubMed] [Google Scholar]
- Demaris A, Mahoney A, Pargament KI. Fathers’ Contributions to Housework and Childcare and Parental Aggravation Among First-Time Parents. Fathering. 2013;11(2):179–198. doi: 10.3149/fth.1102.179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dennison BA, Edmunds LS, Stratton HH, Pruzek RM. Rapid infant weight gain predicts childhood overweight. Obesity (Silver Spring) 2006;14(3):491–499. doi: 10.1038/oby.2006.64. [DOI] [PubMed] [Google Scholar]
- DiSantis KI, Hodges EA, Johnson SL, Fisher JO. The role of responsive feeding in overweight during infancy and toddlerhood: a systematic review. International Journal of Obesity (London) 2011;35(4):480–492. doi: 10.1038/ijo.2011.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Druet C, Stettler N, Sharp S, Simmons RK, Cooper C, Smith GD, Ong KK. Prediction of childhood obesity by infancy weight gain: an individual-level meta-analysis. Paediatric and Perinatal Epidemiology. 2012;26(1):19–26. doi: 10.1111/j.1365-3016.2011.01213.x. [DOI] [PubMed] [Google Scholar]
- Ekelund U, Ong KK, Linne Y, Neovius M, Brage S, Dunger DB, Rossner S. Association of weight gain in infancy and early childhood with metabolic risk in young adults. Journal of Clinical Endocrinology and Metabolism. 2007;92(1):98–103. doi: 10.1210/jc.2006-1071. [DOI] [PubMed] [Google Scholar]
- Farrow C, Blissett J. Does maternal control during feeding moderate early infant weight gain? Pediatrics. 2006;118(2):e293–298. doi: 10.1542/peds.2005-2919. [DOI] [PubMed] [Google Scholar]
- Farrow CV, Blissett J. Controlling feeding practices: cause or consequence of early child weight? Pediatrics. 2008;121(1):e164–169. doi: 10.1542/peds.2006-3437. [DOI] [PubMed] [Google Scholar]
- Francis LA, Granger DA, Susman EJ. Adrenocortical regulation, eating in the absence of hunger and BMI in young children. Appetite. 2013;64:32–38. doi: 10.1016/j.appet.2012.11.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Francis LA, Hofer SM, Birch LL. Predictors of maternal child-feeding style: maternal and child characteristics. Appetite. 2001;37(3):231–243. doi: 10.1006/appe.2001.0427. [DOI] [PubMed] [Google Scholar]
- Francis LA, Susman EJ. Self-regulation and rapid weight gain in children from age 3 to 12 years. Archives of Pediatric and Adolescent Medicine. 2009;163(4):297–302. doi: 10.1001/archpediatrics.2008.579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gartstein MA, Rothbart MK. Studying infant temperament via the Revised Infant Behavior Questionnaire. Infant Behavior and Development. 2003;26(1):64–86. [Google Scholar]
- Graziano PA, Calkins SD, Keane SP. Toddler self-regulation skills predict risk for pediatric obesity. International Journal of Obesity (London) 2010;34(4):633–641. doi: 10.1038/ijo.2009.288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Information. 2009;42(2):377–381. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Institute of Medicine. Early Childhood Obesity Prevention Policies. Washington, D.C.: The National Academies Press; 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jansen A. A learning model of binge eating: cue reactivity and cue exposure. Behavioral Research and Therapy. 1998;36(3):257–272. doi: 10.1016/s0005-7967(98)00055-2. [DOI] [PubMed] [Google Scholar]
- Lakens D. Calculating and reporting effect sizes to facilitate cumulative science: a practical primer for t-tests and ANOVAs. Frontiers in Psychology. 2013;4:863. doi: 10.3389/fpsyg.2013.00863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- May AL, Freedman D, Sherry B, Blanck HM. Obesity – United States, 1999–2010. Morbidity and Mortality Weekly Report Surveillance Summaries. 2013;62(Supplement 3):120–128. [Google Scholar]
- McKetta S, Rich M. The fault, dear viewer, lies not in the screens, but in ourselves: relationships between screen media and childhood overweight/obesity. Pediatric Clinics of North America. 2011;58(6):1493–1508. xii. doi: 10.1016/j.pcl.2011.09.010. [DOI] [PubMed] [Google Scholar]
- Nederkoorn C, Braet C, Van Eijs Y, Tanghe A, Jansen A. Why obese children cannot resist food: the role of impulsivity. Eating Behaviors. 2006;7(4):315–322. doi: 10.1016/j.eatbeh.2005.11.005. [DOI] [PubMed] [Google Scholar]
- Nystrom K, Ohrling K. Parenthood experiences during the child’s first year: literature review. Journal of Advanced Nursing. 2004;46(3):319–330. doi: 10.1111/j.1365-2648.2004.02991.x. [DOI] [PubMed] [Google Scholar]
- Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011–2012. Journal of the American Medical Association. 2014;311(8):806–814. doi: 10.1001/jama.2014.732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Putnam SP, Helbig AL, Gartstein MA, Rothbart MK, Leerkes E. Development and assessment of short and very short forms of the infant behavior questionnaire-revised. Journal of Personality Assessment. 2014;96(4):445–458. doi: 10.1080/00223891.2013.841171. [DOI] [PubMed] [Google Scholar]
- Robinson E, Aveyard P, Daley A, Jolly K, Lewis A, Lycett D, Higgs S. Eating attentively: a systematic review and meta-analysis of the effect of food intake memory and awareness on eating. American Journal of Clinical Nutrition. 2013;97(4):728–742. doi: 10.3945/ajcn.112.045245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rothbart MK, Ahadi SA, Hershey KL, Fisher P. Investigations of temperament at three to seven years: the Children’s Behavior Questionnaire. Child Development. 2001;72(5):1394–1408. doi: 10.1111/1467-8624.00355. [DOI] [PubMed] [Google Scholar]
- Rothbart MK, Ellis LK, Rueda MR, Posner MI. Developing mechanisms of temperamental effortful control. Journal of Personality. 2003;71(6):1113–1143. doi: 10.1111/1467-6494.7106009. [DOI] [PubMed] [Google Scholar]
- Sacco MR, de Castro NP, Euclydes VL, Souza JM, Rondo PH. Birth weight, rapid weight gain in infancy and markers of overweight and obesity in childhood. European Journal of Clinical Nutrition. 2013;67(11):1147–1153. doi: 10.1038/ejcn.2013.183. [DOI] [PubMed] [Google Scholar]
- Slining MM, Adair L, Goldman BD, Borja J, Bentley M. Infant temperament contributes to early infant growth: A prospective cohort of African American infants. International Journal of Behavioral Nutrition and Physical Activity. 2009;6:51. doi: 10.1186/1479-5868-6-51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stifter CA, Anzman-Frasca S, Birch LL, Voegtline K. Parent use of food to soothe infant/toddler distress and child weight status. An exploratory study. Appetite. 2011;57(3):693–699. doi: 10.1016/j.appet.2011.08.013. [DOI] [PubMed] [Google Scholar]
- Sumner G, Spitz A. NCAST Caregiver/Parent-Child Interaction: Feeding Manual. Seattle, WA: NCAST Publications, University of Washington School of Nursing; 1994. [Google Scholar]
- Tan CC, Holub SC. Children’s self-regulation in eating: associations with inhibitory control and parents’ feeding behavior. Journal of Pediatric Psychology. 2011;36(3):340–345. doi: 10.1093/jpepsy/jsq089. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services: Office of Disease Prevention and Health Promotion. Healthy People 2010. Retrieved January 14, 2015, from http://www.healthypeople.gov/2010. [PubMed]
- U.S. Department of Health and Human Services: Office of Disease Prevention and Health Promotion. Healthy People 2020. Retrieved January 14, 2015, from http://www.healthypeople.gov/2020.
- Ventura AK, Golen RP. A pilot study comparing opaque, weighted bottles with conventional, clear bottles for infant feeding. Appetite. 2015;85:178–185. doi: 10.1016/j.appet.2014.11.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wansink B. Mindless eating: Why we eat more than we think. New York: Bantam-Dell; 2006. [Google Scholar]
- Wansink B, Payne CR, Chandon P. Internal and external cues of meal cessation: the French paradox redux? Obesity (Silver Spring) 2007;15(12):2920–2924. doi: 10.1038/oby.2007.348. [DOI] [PubMed] [Google Scholar]
- Wells JC, Stanley M, Laidlaw AS, Day JM, Stafford M, Davies PS. Investigation of the relationship between infant temperament and later body composition. International Journal of Obesity and Related Metabolic Disorders. 1997;21(5):400–406. doi: 10.1038/sj.ijo.0800420. [DOI] [PubMed] [Google Scholar]
- Worobey J, Lopez MI, Hoffman DJ. Maternal behavior and infant weight gain in the first year. Journal of Nutrition Education and Behavior. 2009;41(3):169–175. doi: 10.1016/j.jneb.2008.06.005. [DOI] [PMC free article] [PubMed] [Google Scholar]