

Earlier, we described a late-life depression-executive dysfunction syndrome associated with disability (1). Microstructural white matter abnormalities, common in this syndrome, are principally caused by cerebrovascular changes and contribute to executive dysfunction and resistance to antidepressants (2).
We recently treated a 71 year-old woman in the third episode of early-onset (mid-thirties) major depression, hospitalized after an overdose. She had a dysexecutive behavioral syndrome, prominent hyperintensities on MRI (Figure 1), but no impairment on executive function tests. She presented with mood lability and poor monitoring of her own behavior, i.e. repetition, distractibility, and impulsivity. She performed in the average to superior range on tasks of processing speed (Trails A 73rd percentile), cognitive inhibition (Stroop 66th percentile), set-shifting (Trails B 96th percentile; Wisconsin Card Sort 61st percentile), and planning (Tower Test, 75th percentile). She was partially aware of her pathology, noting “I want to change the habit of speaking out without thinking and acting impulsively”. Her husband’s report on the Frontal System Behavior Rating Scale (3) showed major abnormalities in “disinhibition” with much milder abnormalities in the “dysexecutive” and “apathy” domains.
Figure 1.
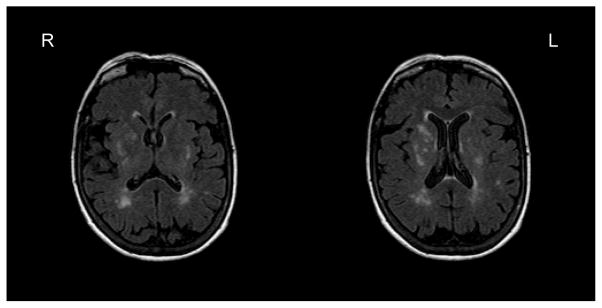
Patient’s MRI Findings
This patient’s behavior was consistent with ventromedial cortex (VMPFC) dysfunction. Lesions in this area may disconnect frontal monitoring systems from limbic output resulting in prominent mood lability, behavioral disinhibition, and inappropriate behavior and judgment (4). Patients with VMPFC dysfunction may have intact executive functioning primarily served by dorsolateral prefrontal cortex and dorsal anterior cingulate circuitry (4).
Behavioral abnormalities related to the VMPFC have seldom been investigated in late-life depression. We recently conducted a cluster analysis of 52 adults with late-life depression and identified three patient subgroups. Cluster 1 (n=20) performed poorly on a task requiring VMPFC integrity (Iowa Gambling) but performed well on cognitive control tasks (Stroop Color Word, Tower), and had no apathy. Cluster 2 (n=19) performed well on the Iowa, had impaired performance on the Stroop and Tower, and had mild apathy. Cluster 3 (n=13) performed well on the Iowa, Stroop, and Tower but had significant apathy. Impairment in risk-sensitive decision-making has been documented in older suicide attempters (5), suggesting that select patients may present with VMPFC impairment. We suggest that disinhibited behavior, dissociable from cognitive control dysfunction, characterizes a subgroup of late-life depression whose neurobiology and treatment response require investigation.
References
- 1.Alexopoulos GS. “The depression-executive dysfunction syndrome of late life”: a specific target for D3 agonists? Am J Geriatr Psychiatry. 2001;9:22–29. [PubMed] [Google Scholar]
- 2.Taylor WD, Aizenstein HJ, Alexopoulos GS. The vascular depression hypothesis: mechanisms linking vascular disease with depression. Mol Psychiatry. 2013;18:963–974. doi: 10.1038/mp.2013.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Grace J, Malloy P. Frontal Systems Behavior Scale (FrSBe): Professional Manual. Lutz, FL: Psychological Assessment Resources; 2001. [Google Scholar]
- 4.Bonelli RM, Cummings JL. Frontal-subcortical circuitry and behavior. Dialogues Clin Neurosci. 2007;9:141–151. doi: 10.31887/DCNS.2007.9.2/rbonelli. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Clark L, Dombrovski AY, Siegle GJ, et al. Impairment in risk-sensitive decision-making in older suicide attempters with depression. Psychol Aging. 2011;26:321–330. doi: 10.1037/a0021646. [DOI] [PMC free article] [PubMed] [Google Scholar]