

Abstract
Background:
Holding educational sessions in a clinical environment is a major concern for faculty members because of its special difficulties and restrictions. This study attempts to recognize the challenges of the ward round teaching through investigating the experiences of clinical teachers in 2011.
Materials and Methods:
This qualitative research is carried out through purposive sampling with maximum variation from among the clinical teachers of major departments in Isfahan University of Medical Sciences (9 persons). The sampling continued until data saturation. Data were collected through semi-structured interview and analyzed through Collaizzi method. Data reliability and validity was confirmed through the four aspects of Lincoln and Guba method (credibility, conformability, transferability, and dependability).
Results:
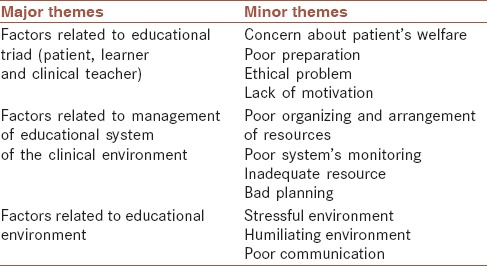
Three major themes and their related sub-themes (minor themes) were found out including the factors related to the triad of clinical teaching (patient, learner, and clinical teacher) (concern about patient's welfare, poor preparation, lack of motivation, ethical problems), factors related to the educational environment (stressful environment, humiliating environment and poor communication) and the factors related to the educational system of the clinical environment (poor organizing and arrangement of resources, poor system's monitoring, bad planning and inadequate resource).
Conclusion:
Ward round teaching has many concerns for teachers, and this should be recognized and resolved by authorities and teachers. If these problems are not resolved, it would affect the quality of clinical teaching.
Keywords: Challenge, clinical teacher, clinical teaching, qualitative study, ward round teaching
INTRODUCTION
Teaching in a clinical environment includes interactions between clinical teacher, learner, and patient, and it must be focused on patient's problems.[1] The purpose of clinical teaching is to learn clinical skills and integrate the basic knowledge with essential mental and psychokinetic skills to render acceptable patient care. In order to learn physical examination, history taking, communicational skills and professional ethics, it is necessary to communicate with the patient and to run teaching sessions on patient's bedside.[1,2,3] It is impossible to effectively teach diverse clinical skills specially related to the human interactions and communication in class, in such cases there should be a real patient or a standard patient.[4,5]
Clinical environment includes outpatient and in-patient wards and social environment. Traditionally, medical instruction happens in in-patient wards where the teacher and his disciples gather at the patient's bedside to investigate his/her problems (disease) and to set up an educational session concurrently.[6,7]
In spite of the ward round importance, nowadays to run educational sessions at bedside is one of the most challenging scientific duties of the medical teachers because of its difficulties and restrictions.[8] A clinical teacher has crucial roles as facilitator, medical specialist, director, and manager.[9] In addition, heavy workload, lack of a suitable and feedback system for instructional activities and distrust decreases her/his motivation to run appropriate bedside sessions.[7,10,11,12]
On the other hand, some other factors make the clinical environment more chaotic, like: Learners’ different educational background that need more energy to engage them, lack of motivation in ward staff, and unpredictable conditions in hospital, leads to decreased teachers’ interest and motivation to teach.[8]
Because of the above-mentioned restrictions, some of the medical teachers prefer to run the educational rounds in conference rooms, or on patient's bedside without any effective effort to teach them; however, most of the times, instructional sessions take place in conference rooms.[7]
We could found only a few studies about challenges and restrictions of holding educational sessions in a clinical environment considering teacher's experiences.[1,8,12] Various researches were carried out in Iran about medical teachers and the condition of educational round environment; for example, they investigated characteristics of effective teaching, stressful factors affecting clinical instruction, effects of ward round teaching, teaching techniques, characteristics of a good medical teacher and an educational round environment according to learners, patients and teachers.[13,14,15,16,17] However, in all these quantitative studies we could find a few researches that had investigated problems of teaching in a clinical environment through recognizing medical teacher's experiences. Therefore, this study attempts to investigate ward round teaching challenges by probing clinical experiences of medical teachers in major departments of the Isfahan University of Medical Sciences.
MATERIALS AND METHODS
This qualitative study tried to understand medical teachers’ experiences as phenomena influenced by values, cultures, and human communications.[18,19]
The research environment were teaching hospitals affiliated with Isfahan University of Medical Sciences, and the research community included clinical teachers of internal, Obstetrics and Gynecology, Pediatrics, and Surgery Departments of Faculty of Medicine. Participants of the study were chosen through purposive sampling with maximum variation.[20,21] Sampling continued until data saturation.[22] Data were collected through individual semi-structured interviews. Interviews started with simple general questions such as: “please, explain your experiences about ward round teaching.” And “which problems do you usually encounter while holding ward round teaching?” on the basis of the information obtained during the interview session, more questions were posed (probing questions). The interviewer was physician with some experience in clinical teaching, and all researchers were expert in medical education.
As the teachers suggested, the interviews took place in their room in the hospital. All interviews were recorded for further investigation. Interview sessions continued for 45-75 min. Informed consent was obtained from participants before the interview.
Collaizzi method was used to analyze the data.[23] Interviews were verbatim transcribed for further analysis. To understand the interviewees “experiences,” interviews were read line by line and major concepts were coded, and were categorized into groups; at last, findings were referred to the interviewees and they confirmed the validity of the results. Lincoln and Guba (1983) suggested four ways to confirm authenticity and rigor of the data, that is, credibility, dependability, conformability, and transferability. Considering these criteria in the research, the researcher tried to attain the trustworthiness of the findings by using different ways. Credibility was checked by allocating sufficient time to data collection process (long engagement) and member check procedure. The long-term experience of two of the researchers (first and last authors) in clinical teaching was useful in confirming codes. Transferability was considered by tick description procedure, and dependability was strengthened by writing memos and coding data by 2 experts in qualitative research (external audit).
Ethical considerations included: Securing informed consent, considering the right of anonymity, privacy and confidentiality and their right of withdrawal at any stage of the research.
RESULTS
Study sample consisted of nine clinical teachers (4 women and 5 men) of Isfahan University of Medical Sciences, specialized in internal medicine (2), pediatrics (2), obstetrics and gynecology (2), Cardiology (1) and surgery (2) who had more than 5 years (average of 18 years) work experience. Among them, five were associate professors, three assistant professors and one full professor. Therefore, suitable combinations of participants were invited for interview.
The overall findings of the qualitative data analysis called disrupting factors of ward round teaching included three major themes of “factors related to educational triad,” “related to educational environment,” and related to the “management of educational system of the clinical environment.” The subgroups of the themes (minor theme) are as follows [Table 1].
Table 1.
Themes and their sub-groups
Factors related to the educational triad
This theme includes the challenges that three major parts of clinical instruction, that is, patient, student and clinical teacher somehow cause them. This theme is itself parted into the miner themes of “concern about patient's welfare,” “poor preparation,” “ethical problem” and “lack of motivation.”
Concern about patient's welfare
This minor theme means teacher's concern about possible physical and mental harms to the patient and violation of his privacy during the instruction to the students. Expression of the participant number (2) is an example of this: “Since hospitalized, the patient has been examined 2 or 3 times, at the time of admission each 1st and 2nd year intern and resident has once examined him/her. A patient with prolapsed hardly accepts to go to the examination room 4-5 times.”
Poor preparation
Participants in the study believed that before ward round teaching, the teacher, and the students should be prepared. Poor preparation means the inadequate preparedness of the teachers and students. For example, students should study before round meeting and get patient's history; and teachers should make sure the physiological and safety needs are met. The statements of the participants indicated teacher's problems with their salaries and allowances and financial problems of the students. Therefore, the first level of preparation may be meeting their physiologic needs. Expression of the participant number (4) is an example of this: “Too much outside work of the intern and resident causes some problems for teaching; for instance he trades in the car, he has night shifts outside the hospital because he is going to marry. He comes sleepy to the round.”
Participants believed that to have enough equipment, to be cognitively and emotionally prepared and also to be skilled enough are the other essential conditions to attend at ward round teachings. Expression of the participant (7) indicates that some learners do not have enough equipment: “One of our ward round problems is that the resident does not have a stethoscope, the student does not bring stethoscope and says i will bring from the ward.”
Expression of the participant number (5) indicates lack of enough skill: “You can never imagine that the student of month 3 and 4 do not know how to use thermometer; or the intern does not know how to see the patient's throat. He does not take the tongue blade and the flashlight correctly.”
Ethical problems
Participants expected the respect to professional ethics and existence of some problems in medical ethics caused tension for them. They mentioned “not having appropriate I clothing of the learners, not observing professional disciplinary rules and using unsuitable ornaments as some of these problems. Expression of the participant number (5) is an example of this: “We start the round for example with 10 persons, but at the end of the round there are only 5. The others went away one by one.”
Lack of motivation
Lack of motivation in this study means lack of interest of the students in progress. Teachers frequently complained about that and knew it as the main challenge of instruction. Concepts such as “frequent distraction,” “not paying due attention to learning” and “not learning deeply” indicate lack of motivation of the students and are categorized in this sub-theme (minor theme). Expression of the participant number (7) is an example of this: “If I see the learner has hope and inquiries into the matter, I really love him/her so that i want to worship him/her. If I see an intern asks about a patient, I wonder because most of the students are hopeless and dull.”
Factors related to the management of educational system in clinical environment
The purpose of this theme is the process during which a meaningful layout forms between the elements, in addition, through scientific planning, targets and activities are determined and facilities are prepared, also people's activities and the plan are evaluated. This theme is categorized into four sub-theme of: “poor organizing and arrangement of resources,” “lack of system's monitoring,” “inadequate resource” and “bad planning.”
Poor organizing and arrangement of resources
This means unsuitable allocating of educational activities among the members and inappropriate spatial environment of the wards. Expression such as “different ward round teachers during the week,” “inappropriate shift time,” “not simultaneous shifting of the interns” and “inappropriate sharing of learners among the teachers” are examples of poor organizing and arrangement of resources. Expression of the participant number (2) is an example of this: “They don’t tell me you should teach these four interns from the beginning to the end of the month, if it were so, i would know him, give him an assignment, and ask him the next day. But we are not coordinated. 1-day I am in round, another day another teacher.”
Also “several educational groups in one room” and “diverse educational programs in different hospitals” refer to this sub-theme.
Expression of the participant number (2) is an example of this: “There are too many people in a small room and another group is going to have round, we usually wait until the round of the previous group finishes and then we start.”
Other cases that are categorized in this group and the participants emphasized on are “their several duties,” “excessive expectations of teachers and insufficient capacity to manage them.” and “their lack of time due to that. Expression of the participant number (3) is an example of this: “To have work and teaching rounds together makes so many problems for me, if i just want to have work round, teaching will be sacrificed. And if i had only educational round, my patient treatment tasks would remain unfinished.”
Poor educational system's monitoring
This sub-theme means inappropriate teacher's and program evaluation. Expressions such as “not having justly evaluation system,” “instruction quality not influencing teacher's evaluation,” “not receiving in-time positive or negative feedback” and “not evaluating the rounds” show this problem. Expression of the participant number (3) is an example of this: “Instruction is not tangible, if you taught 3 h a day and the intern complimented you, it would not useful for you. But if you had three articles, you would become associate professor and you can have an office.”
Inadequate resources
This concept means unavailable physical and human resources so that teaching in clinical environment encounters some problems.” Shortage of equipment such as sonography, impossible internet connection, incomplete patient's files, shortage of bed and ventilation and small rooms, are examples of this concept. Shortage of human resources was declared in. Like “shortage of personnel and faculty members.” Expression of the participant number (5) is an example of this: “I have repeatedly said nurse supervisor should be present at rounds but because of their numerous duties and few of them this is not always possible.”
Bad planning
Some of the expressions of the participants showed planning deficiency, for example: “Not paying enough attention to the educational requirements in academic planning,” “holding the educational rounds and the classes at the same time” and “holding rounds at the same time as work shifts” are in this category. On the other hand, problems such as “inappropriate references determined by ministry of health, care and medical education,” “inappropriate arena for medical education,” and “the priority of postgraduate instruction” are the most important problems mentioned by some of the teachers who participate in medical education. Expression of the participant number (7) is an example of this: “Since postgraduate has come, all our energy is spent on it, that while this students leaves here, he is good, he will be the best … it means we just focus on this.” Expression of the participant number (2) is an example of this: “Students (interns) want to leave at 11, then they leave at 10:30 and say we should go to Beheshti Hospital, we have another class there.”
Deficiency in students’ evaluation including “evaluation of the students at low levels of bloom's taxonomy” and “lack of evaluation of the students according to their function” are the cases mentioned by most of the participants. Expression of the participant number (3) is an example of this: “Their assessments are according to the knowledge not based on the performance and approach to the patient. Therefore, they mostly prefer to study theories than to stay in rounds and gain experience.”
Another instance of planning deficiency is lack of rules or a system of informing the beneficiary persons so that the participants mentioned related cases such as “no rules with executive force, e.g., clothing related rules” and “no nurse at rounds.”
Factors related to the educational environment
In this study, harmful factors of educational environment included the conditions that according to the participants’ ideas would impair teaching and learning in clinical environment. Its sub-concepts are “stressful environment,”“humiliating environment” and “poor communication.”
Stressful environment
Stressful environment means there are some conditions in educational environment that cause stress or threaten the participants. Codes like “different levels of the learners,” “too many nurses and patient's companions in the room,” “noisy environment,” “very crowded rooms,” “unpredictable conditions of clinical environment,” “deterioration of the patient's disease during the round,” “frequent phone calls during the round” are categorized in this sub-theme. Expression of the participant number (5) is an example of this: “During the round the nurse comes and says doctor for example Hosein (intern) you have a phone call and he (intern) goes away.”
Humiliating environment
Participants believed interactions are so that they cause humiliation of the learners. Cases such as “not paying due attention to the students,” “feeling disdain to teach the students” are mentioned in this regard.
Expression of the participant number (3) is an example of this: “By the extra work that we assign interns and residents to do, we have converted them to the servers who bring the laboratory test results, Doctor! go to the lower floor and bring the test results, Doctor! Call and bring the graph.”
Poor communication
This means lack of suitable communication among all groups in educational system or clinical environment including students, interns, residents and personnel. Expression of the participant number (6) is an example of this: “Our students learn nothing from interns, our interns do not try to teach them, resident says i have learned myself, attend physician has not taught me why should i teach intern?”
Lack of influential relationship between physician and patient categorized in codes such as “not having patient's permission,” “not justifying the patient” and “using scientific words by the patient's bedside” are in this sub-concept. “patient's anger” and “lack of cooperation of the patient with the students” are because of inappropriate communication with the patient. Expression of the participant number (5) is an example of this: “Some times during the round i see the patient has frowned. I ask her” why are you upset? “She pours her heart out. You have kept me here without doing anything useful for me. Whomever i speak to, doesn’t answer me clearly i don’t know what to do…”
DISCUSSION
The results of this study are generally called disrupting factors for teaching in clinical environment. In ward round teaching the teacher, students, patient and the personnel come together. The purpose is to train competent physicians to take care of the patients. To meet this goal interaction and accurate function of these parts are needed.
Members of this system have interactions with their environment. It means that they are influenced by the environment conditions and their relationship affects the present environment. Inappropriate relationship of the students with each other and with their teacher creates a stressful (tense) environment which can itself prevent the teacher and the learners to act correctly. Management of this system together with establishing rules and regulations, instructions and frameworks regulate the system and causes its survival. Therefore, to imagine such a system helps to realize and recognize disrupting factors obtained from this study, that is, factors related to the elements of teaching in clinical environment, factors and conditions related to the environment in which these elements exist and factors related to the system monitoring (management) [Shape 1].
Shape 1.
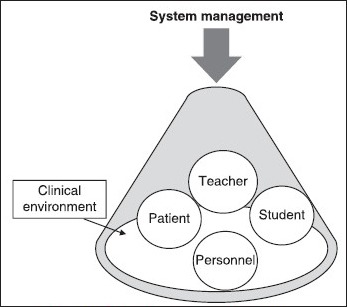
Relationship among major parts
The etiology of this event is unknown. In fact, a canalicular UDT ascends during the interval which is expected for its descend.
This issue requires larger studies. This experience facilitates the detection of secondary nonpalpable testis and makes a good guide for surgical intervention.
Elements (members) of this system should be prepared before starting instruction in clinical environment, for instance physiologic needs of the students should be provided. Tiredness, drowsiness and financial problems of the learners are obstacles for educational sessions; therefore, the first duty of teachers is to consider these needs. Learners should bring equipments such as stethoscope, sphygmomanometer and flashlight in order to have involvement in educational process. Moreover, suitable professional clothing of the learners indicates their readiness to have psychological and emotional communication with the patient. Another duty of the teacher in the next stage is to consider learner's input behaviors which are behaviors that the learner should have obtained before learning a new subject. These behaviors have cognitive, emotional and psychosomatic aspects. In this study and also other studies teachers emphasized on learners’ failure at learning primary clinical skills.[24] Lack of due attention to these needs decreases the effect of educational process.[25] Therefore work-hour of the interns and residents should be so that it does not result in physical tiredness. In addition, there should be some changes in educational planning before starting the internship period so that the students get ready to learn the experiences of internship period. Also, some instructions should be determined about students’ way of clothing and having essential equipment.
But the most important concern of the participants was lack of motivation of the students to make academic progress which is also one of the major challenges in other studies.[26] On the other hand, in some studies the researchers mentioned low level of variables like optimism, self-esteem, educational factors’ quality and family revenue as the major factor responsible for decreasing educational motivation.[27]
Active involvement of the teachers as one of the inputs of teaching in clinical environment is essential to reach the goal. In this study time limitation, various grueling duties in clinical environment and large amount of services are inhibitive factors that have close relationship with each other. Seabrook, has noted time limitation and large amount of treatment as concerns of the teachers in ward round teaching.[28] Although large number and variety of the patients facilitates the process of teaching and learning, if this increase were so that residents and teachers had to spend much of their time to give service to these patients, teaching would be limited to the times of caring the patients or to their free times; consequently, there would be no time for discussion and deep learning.
Spenser and Romany mentioned lack of encouragement by the teachers and more important than all, concern of promotion and necessity of research works as obstacles forward round teaching.[1,12] Their results correspond with the results of this study. Hendry et al. in their research noted lack of financial support and more important than that, worthlessness of education and lack of attention to the teacher as prohibitive factors for teachers’ motivation.[29]
Teaching in clinical environment is together with real patient's involvement.[30] The current system of caring the patients in educational hospitals, offered by the learners under the supervision of the teachers, not only causes the patient to feel that he has turned to a tool for instruction and consequently results in psychic damage.[31] Therefore, considering their ethical responsibilities, clinical teachers are usually worried to maintain patient's safety. One of the concerns of the participant was about the protection of the patient's privacy. In a research by Ramani 2008, concern about patient's welfare is one of the factors which makes the teacher avoid teaching on patient's bedside and teach in conference room or in class instead.[11] This is while some studies with the purpose of investigating the patient's perspective about ward round show that they are not upset of holding educational sessions on their bedside, in addition they prefer it to education in conference room, far from themselves.[31,32,33,34,35]
The results of this study indicate that some teachers’ concern is to respect the patient's rights, while some other members of medical team do not pay enough attention to the patient's dignity. Lack of an effective communication between the patient and physician and inappropriate attention to the professionalism may prevent cooperation of the patient with the learners and decrease his readiness as another input of teaching in clinical environment; this is also emphasized in other studies.[1,12,36,37]
A humiliating environments categorized in disruptive factors related to the environment, threatens the process of learning and teaching. Humiliating experiences are the most stressful factors for the learners.[13] In addition, in other studies “being passive students, not to let them to speak and to humiliate them" are prevalent problems of ward round teaching.[1,38] Such research confirms the results of this study.
As mentioned in the resources, clinical environment is an unpredictable environment[1] and in contrast with the class, there is very little control on it; this can be stressful for the teachers. However, considering the constructivism theory in which it is recommended to prepare the learning situation so that the learners can face with different viewpoints about an issue,[25] we can say unpredictable circumstances and challenging situations in clinical environment can improve learning. Since in the real world, learners often face with complicated situations, educational environments should also provide the same situations for the learners. Moreover, teachers should try to empower the learners to deal with complicated environments.
This system`s survival depends on the interaction among its parts. According to the theory of cognitive development by Vygotsky, the interaction between the learner and social environment is very important in his/her learning.[25] But in this study, the participant noted that poor communication and lack of effective relationship between multigrade learners decrease their learning. Since this threatens the system, educational planners should carefully try to solve this.
Important obstacles that the participants emphasized on, are the challenges related to the management of teaching in clinical environment. The manager is expected to plan and determine the goals based on the learners’ needs, designate necessary functions to reach the goal and evaluate them according to the determined goals. Spenser's research states cases like “lack of clear goals and expectations, concentration on the memorizations instead of focus on skills to solve the problem, different viewpoints and inappropriate level of teaching to the learners” as prevalent problems of ward round teaching.[1]
Other results of this study include poor arrangement and organizing of the human resources and facilities like inappropriate distribution of the students, uncoordinated shift of the learners, different levels of the learners and improper layout of the environment. It is expected that these problems would be solved by an accurate management. In another study to investigate the input of ward round teaching through evaluation of the students number accompanying the teacher during the visit and ratio of the beds, patients and personnel, it is concluded that the input of ward round teaching in the selected hospitals is ideal but to improve the quality of ward round teaching, accurate management and planning is needed.[38]
Positive point about this study is that it investigates the ward round teaching through the experiences of the clinical teachers and is of qualitative type through which profound and comprehensive description of the problems and restrictions is possible. Such results cannot be concluded from a quantitative study. However because these problems should also be investigated through the perspective of other parts of educational triad, that is, the patient and the student, some other studies are suggested to complement this research.
CONCLUSION
In spite of its importance, ward round teaching has caused too much concern for the teachers because of its various challenges and restrictions. Therefore; it would affect the quality of clinical teaching. Some of the important challenges are “lack of the motivation of the learners, professional stresses of the teachers, destroyed communication among the learners and lack of proper management of ward round teaching.” These problems can be widely removed through a proper management by the teachers and authorities. Consequently, we should give more importance to the ward round teaching and try to find some solutions to solve these challenges.
AUTHOR'S CONTRIBUTION
KS, FH and SB contributed in the conception of the work,conducting the study, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work. PA contributed in interpretation of data for the work, revising the work critically for important intellectual content, approval of the final version of the manuscript, and agreed for all aspects of the work. AO contributed in the conception of the work, the acquisition, analysis of data, conducting the study, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work.
ACKNOWLEDGMENTS
This work was supported by Iran University of Medical Sciences.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Spencer J. Learning and teaching in the clinical environment. BMJ. 2003;326:591–4. doi: 10.1136/bmj.326.7389.591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Janicik RW, Fletcher KE. Teaching at the bedside: A new model. Med Teach. 2003;25:127–30. doi: 10.1080/0142159031000092490. [DOI] [PubMed] [Google Scholar]
- 3.Haghani F, Arabshahi SK, Bigdeli S, Alavi M, Omid A. Medical academia clinical experiences of Ward Round Teaching curriculum. Adv Biomed Res. 2014;3:50. doi: 10.4103/2277-9175.125771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Nair BR, Coughlan JL, Hensley MJ. Student and patient perspectives on bedside teaching. Med Educ. 1997;31:341–6. doi: 10.1046/j.1365-2923.1997.00673.x. [DOI] [PubMed] [Google Scholar]
- 5.Ramani S. Twelve tips to improve bedside teaching. Med Teach. 2003;25:112–5. doi: 10.1080/0142159031000092463. [DOI] [PubMed] [Google Scholar]
- 6.Harden RN, Dent JA. 2nd ed. London: Churchill Livingstone; 2005. A Practical Guide for Medical Teachers. [Google Scholar]
- 7.Weinholtz D, Edwards JC. Baltimore, Maryland: Johns Hopkins University Press; 1992. Teaching During Rounds: A Handbook for Attending Physicians and Residents. [Google Scholar]
- 8.Ende J. What if Osler were one of us? Inpatient teaching today. J Gen Intern Med. 1997;12(Suppl 2):S41–8. doi: 10.1046/j.1525-1497.12.s2.6.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Crosby RM. AMEE Guide No 20: The good teacher is more than a lecturer-the twelve roles of the teacher. Med Teach. 2000;22:334–47. [Google Scholar]
- 10.Hoffman KG, Donaldson JF. Contextual tensions of the clinical environment and their influence on teaching and learning. Med Educ. 2004;38:448–54. doi: 10.1046/j.1365-2923.2004.01799.x. [DOI] [PubMed] [Google Scholar]
- 11.Lake FR. Teaching on the run tips: Doctors as teachers. Med J Aust. 2004;180:415–6. doi: 10.5694/j.1326-5377.2004.tb05997.x. [DOI] [PubMed] [Google Scholar]
- 12.Ramani S, Orlander JD, Strunin L, Barber TW. Whither bedside teaching? A focus-group study of clinical teachers. Acad Med. 2003;78:384–90. doi: 10.1097/00001888-200304000-00014. [DOI] [PubMed] [Google Scholar]
- 13.Yazdankhahfard MR, Pouladi SH, Kamali F, Mirzaei K, Akaberian SH, Yazdanpanah S, et al. The stressing factors in clinical education: The viewpoints of students. Iran J Med Educ. 2008;8:341–350. [Google Scholar]
- 14.Salehi SH, Hasanzahraie R, Ghazavi Z, Amini M, Ziai SH, Shahneh M. The Characteristics of effective clinical teachers as perceived by nursing faculty and students. Iran J Med Educ. 2004;4:37–44. [Google Scholar]
- 15.Adibi P, Anjevian M. The clinical rounds on patients bedside in internal ward from patients viewpoints. Iran J Med Educ. 2006;6:15–21. [Google Scholar]
- 16.Soltani Arabshahi K, Kouhpayezade J, Sobuti B. The educational environment of main clinical wards in educational hospitals affiliated to Iran university of medical sciences: Learners’ viewpoints based on DREEM model. Iran J Med Educ. 2008;8:43–50. [Google Scholar]
- 17.Alavi M, Abedi H. Nursing students’ experiences and perceptions of effective instructor in clinical education. Iran J Med Educ. 2008;7:325–34. [Google Scholar]
- 18.Lynch S. Qualitative Research Methods in Nursing. Columbos: Greyder Press; 1998. Using a phenomenological research method to study nursing phenomena. [Google Scholar]
- 19.Ansari M, Yamani N, Yousefi A, Yarmohammadian M. 1th ed. Isfahan: Isfahan Medical University; 2007. An Introduction to Qualitative Research. [Google Scholar]
- 20.Saneei A, Nikbakht-Nasrabadi A. 1st ed. Tehran: Baraie Farda; 2004. Qualitative research methodology in medical science. [Google Scholar]
- 21.Jamshidian A, Siadat A, Norouzi R. Qum: Sama Ghalam; 2003. An Introduction to Qualitative Research. [Google Scholar]
- 22.Salsali M, Parvizi S, Adib Hajbagheri M. 1st ed. Tehran: Boshra; 2003. Qualitative Research Methodology. [Google Scholar]
- 23.Nasr A, Oreizi H, Abolghasemi M, Bagheri K, Alamatsaz M, Pakseresht M. 2nd ed. Tehran: The Organization for Researching and Composing University Textbooks in the Humanities (SAMT); 2008. Educational Research An Introduction. [Google Scholar]
- 24.Haddadgar A, Jowshan R, Changiz T, Shams B, Yousefy F. Where is here, what am I? Designing, implementation and evaluation of an introduction to clinical clerkship course for medical students. Iran J Med Educ. 2001;1:24–8. [Google Scholar]
- 25.Seif A. 43th ed. Tehran: Doran; 2012. Educational Psychology: Psychology of Learning and Instruction. [Google Scholar]
- 26.Arhami NS, Kalantari S, Atarod S. Medical students attitude towards their field of study and future. Iran J Med Educ. 2004;4:76–81. [Google Scholar]
- 27.Molavi P, Rostami K, Naeini AF, Nia HM, Zade BR. Baresi avamel moaser dar kahesh angize tahsili daneshjoian daneshgah oloom pezeshki ardebil. Journal of Medical Council of Iran. 2007;25:53–8. [Google Scholar]
- 28.Seabrook MA. Medical teachers’ concerns about the clinical teaching context. Med Educ. 2003;37:213–22. doi: 10.1046/j.1365-2923.2003.01437.x. [DOI] [PubMed] [Google Scholar]
- 29.Hendry RG, Kawai GK, Moody WE, Sheppard JE, Smith LC, Richardson M, et al. Consultant attitudes to undertaking undergraduate teaching duties: Perspectives from hospitals serving a large medical school. Med Educ. 2005;39:1129–39. doi: 10.1111/j.1365-2929.2005.02320.x. [DOI] [PubMed] [Google Scholar]
- 30.Lake FR, Ryan G. Teaching on the run tips 4: Teaching with patients. Med J Aust. 2004;181:158–9. doi: 10.5694/j.1326-5377.2004.tb06208.x. [DOI] [PubMed] [Google Scholar]
- 31.Doshi M, Brown M. Whys and hows of patient-based teahing 52. Br J Psychiatry. 2005;11:223–31. [Google Scholar]
- 32.Benson J, Quince T, Hibble A, Fanshawe T, Emery J. Impact on patients of expanded, general practice based, student teaching: Observational and qualitative study. BMJ. 2005;331:89. doi: 10.1136/bmj.38492.599606.8F. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Lynöe N, Sandlund M, Westberg K, Duchek M. Informed consent in clinical training - Patient experiences and motives for participating. Med Educ. 1998;32:465–71. doi: 10.1046/j.1365-2923.1998.00237.x. [DOI] [PubMed] [Google Scholar]
- 34.O’Flynn N, Spencer J, Jones R. Consent and confidentiality in teaching in general practice: Survey of patients’ views on presence of students. BMJ. 1997;315:1142. doi: 10.1136/bmj.315.7116.1142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Thomas E, Hafler J, Woo B. The patients experience of being interviewed by first-year medical students. Med Teach. 1999;21:311–4. [Google Scholar]
- 36.Zamani A, Shams B, Moazem E. Communication skills training for physicians as a strategy for enhancing patients satisfaction: A model for continuing education. Iran J Med Educ. 2004;4:15–22. [Google Scholar]
- 37.Farajzade S, Nohi E, Mortazavi H. Interns communication with patients during interview: The perspectives of patient and observer. Iran J Med Educ. 2006;6:79–86. [Google Scholar]
- 38.Harandi TF, Soltani Arabshahi K. Baresi darondad va faraiand amozesh balini dar daneshgah oloom pezeshki Iran. Faslnameh Paiesh. 2003;2:132. [Google Scholar]