

Abstract
Background:
BRCA1/2 genes mutation prevalence varies among ethnic groups and may be influenced by founder mutations. Understanding BRCA1/2 genes mutations is important for reducing breast cancer (BC) incidence, accurate risk assessment and counseling. This systematic review of the literature was conducted to addressing BRCA1/2 mutations in Iranian BC patients.
Materials and Methods:
A search for relevant articles was run on before January 2014 using MedLine, PubMed, Science Iranian Database, Google, and Web sites related to the study topic. The key words included: BC and Iran with Genes, BRCA Genes, BRCA1 and BRCA2; “Cancer Genes,” and “Iran.”
Results:
Thirteen articles retrieved from this search strategy were eligible for this review. The overall BRCA1 mutation rate for Iranian female BC patients was detected 31.8% (377/1183). Although this gene mutation rate for male patients is <0.01%. Eight BRCA1 mutations (c. 4837A > G, c. 3419G > A, c. 3119G > A, c. 2612C > T, c. 3113A > G, c. 2311T > C, c. 4301T > C and c. 4308T > C in BRCA1, and one BRCA2 mutation (c. 6494G > C) were found in multiple case subjects and represent candidate founder mutations.
Conclusion:
According to these studies, there is heterogeneity in BRCA mutations in Iranian BC patients.
Keywords: BRCA1, BRCA2, breast cancer, familial, Iran
INTRODUCTION
Breast cancer (BC) continues to remain the commonest cause of cancer death in women worldwide. BC is increasing in regions that until recently had low rates of the disease.[1] In Asia, BC incidence peaks among women in their forties, whereas in the United States and Europe, it peaks among women in their 60's. Similarly, in Iran, BC is most common cancer among females, which comprising 24.4% of all neoplasms. The mortality rate of BC was 5.8/100,000 women in Tehran in 1998, 2.5/100,000 for a female population, and 7762 years life lost in the 18 provinces of Iran in 2001.[2] The latest data on age-specific incidence rate of BC showed that its crude incidence rate and ASR are 17.4 and 23.1/100,000, respectively. Data from the Cancer Institute show that BC highest rate is occurring in those aged between 35 and 44 years in Iran.[3] It is suggested that BC incidence among Iranian females is rising and affects at least one decade earlier than their western counterparts, with a mean age ranging from 47.1 to 48.8 years.[4] Furthermore, in Iran BC affects the majority of patients in the premenopausal age.[5]
Various risk factors for BC have identified, but a positive family history remains among the most important ones established for BC, with first-degree relatives of patients having an approximately two-fold elevated risk. It is estimated that approximately 20-25% of this risk is explained by known BC susceptibility genes, mostly those conferring high risks, such as BRCA1 and BRCA2. Germline mutations in the BRCA1 (BC 1, early onset) and BRCA2 (BC 2, early onset) genes are the most important cause of hereditary breast and ovarian cancer. There is not a direct procedure to estimate the prevalence of BRCA1/2 mutations in the general population. In the absence of such measurement procedure, it can be assumed that nearly 50% of the mutations would be in BRCA1 and 50% in BRCA2.[6]
Since the isolation of these two genes, more than 2000 different mutations have been identified. The most common types of mutation are attributed to small insertion/deletion frameshift, non-synonymous truncation, and disruption of splice site leading to entire nonfunctional BRCA proteins.
Early works of the BC Linkage Consortium have shown that respectively 52% and 32% of families with at least four cases of BC diagnosed <60 are caused by BRCA1 and BRCA2. When selecting families with BC and one or more cases with ovarian cancer 81% of the families are explained by BRCA1 and 14% by BRCA2. However, when selecting families with four or more cases of BC diagnosed <60 and no cases of ovarian cancer or male BC only 33% could be explained by BRCA1 and BRCA2 together.[7] Moreover, based on one report of clinical referral populations that considered both BRCA1 and BRCA2 mutations together, the prevalence among those with a strong family history of cancer is estimated to be 8.7%. Additional prevalence estimates for individuals from referral populations with various levels of family history range from 3.4% (no BC diagnosed in relatives younger than age 50, no ovarian cancer) to 15.5% (BC diagnosed in a relative younger than age 50 and ovarian cancer diagnosed at any age).[8,9]
Since the overall BRCA mutation rate in Iranian BC patients has not been estimated to date, the present review was conducted to evaluate the frequency of BRCA1/2 mutations in Iranian BC patients.
MATERIALS AND METHODS
Selection of publications
The following inclusion criteria developed and applied to identify and select eligible studies: Published in English; case-control, and cross-sectional studies. Titles and abstracts were reviewed to identify studies that potentially detailed the frequency of BRCA1/2 genes mutations testing in Iranian BC patients. After the titles and abstracts had been screened, and the relevant articles identified the specific information including type of study, number of exons evaluated, number, type and classification of mutations were retrieved.
Eligible studies were excluded if: They did focus in BRCA1/2 genes mutation in another condition. Molecular biology studies, in vivo studies, comments, opinions, abstracts and unpublished studies were excluded.
Literature search
The comprehensive data on BRCA1 and BRCA2 mutation in BC in Iranian patients was undertaken via a literature search. A search for relevant articles was run on or before January 2014 using Medline, PubMed, Science Iranian Database, Google, and Web sites-related to the study topic. The key words included: BC and Iran with Genes, BRCA Genes, BRCA1 and BRCA2. In order for a comprehensive search, different combinations of the terms were used. In all instances, searches were limited to studies published in English. The reference lists of articles selected for the review were also manually checked for additional literature. Studies combining and/or comparing Iranian in or outside Iran with other ethnic groups were included but only the data of the Iranian analyzed were included in this review.
RESULTS
A flow chart showing the study selection process is presented in Figure 1. In total, 13 studies have been carried out about BRCA1/2 gene mutation in Iranian BC yet. These studies are summarized in the following:
Figure 1.
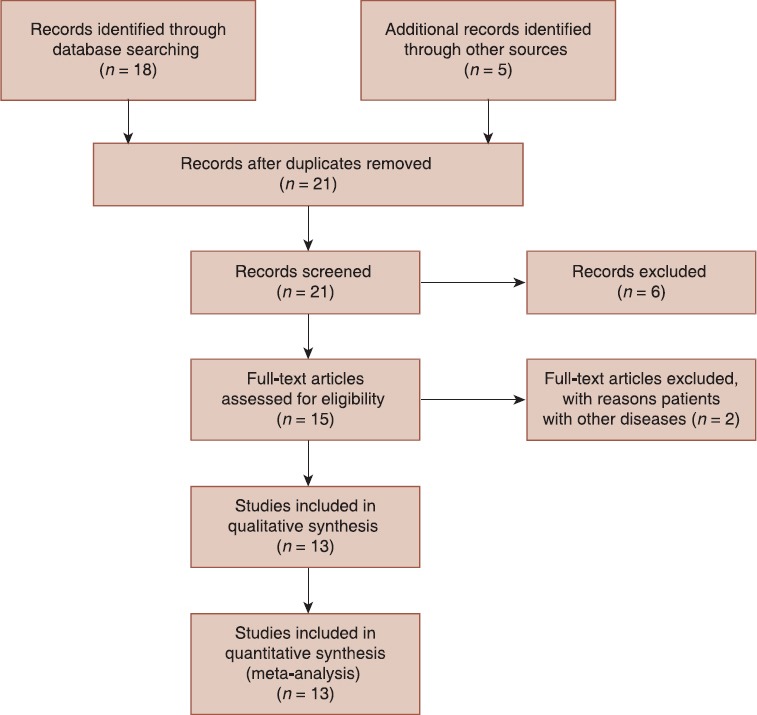
Study flow diagram for previous included studies
Bar-Sade et al. have screened a population consist of 150 Iranian Jews, 354 of Moroccan origin, and 200 Yemenites to determine the prevalence of BRCA1 185delAG founder mutation. They found that four of Moroccan origin (1.1%) and none of the Yemenites or Iranians was a carrier of the 185delAG mutation.[10]
Ghaderi et al. carried out the first mutation detection in BRCA1 gene among Iranian BC patients. A cohort of 80 patients that 22 of those had at least one first-degree relative with any kind of cancer was screened. Their analysis was initially limited to exon 2 of BRCA1 for 185delAG in 80 Iranian BC patients by direct sequencing. None of the cohort showed the 185delAG mutation or any changes in the sequences of exon 2. They also performed a complete analysis of the entire 5.6 kb BRCA1 gene coding region in a 22 DNA sample which were selected out of 80 samples according to the patients’ family history of breast or ovarian cancer, or any other cancers in their first-degree relatives. There were nine mutations (six missense and three unknown variants) in BRCA1, which three of those were placed in the intronic part of the gene. Four missense mutations were identified in exon 11. The remaining mutations were in exon 13, 16, and 18. With the exception of a point mutation in exon-16, which has not been reported previously, the remaining polymorphic sites in the BRCA1 exons have frequently been reported by others studies.[11]
Yassaee et al. with the collaboration of two main centers for cancer evaluated peripheral bloods of 83 women with early-onset BC under 45 years old to determine germline mutations in the BRCA1 and BRCA2 genes. BRCA1 exons 2, 3, 5, 13 and 20 and BRCA2 exons 9, 17, 18, and 23 with the single-strand conformation polymorphism assay on genomic DNA amplified by polymerase chain reaction (SSCP-PCR), and BRCA1 exons 11 and BRCA2 exons 10 and 11 by the protein truncation test (PTT) were analyzed. Ten germline mutations in the cohort were found (4 in BRCA1 and 6 in BRCA2). There were 5 frameshifts (3 in BRCA1 and 2 in BRCA2), 4 of which were novel (3 in BRCA1 and 1 in BRCA2), 3 missense changes of unknown significance (all in BRCA2) and 2 polymorphisms. One case of the cohort had 2 mutation, the first mutation in BRCA1 (12bp dup GTATTCCACTCC IVS20 + 48) and second mutation in BRCA2 (6261-6262insGT). The mutations were: 185-186delAG and 181-182insT in exon 2, 2335-2336delAA in exon 11, and 12bp dup GTATTCCACTCC IVS20 + 48 in exon 20 mutations in BRCA1, and 3979-3980insA, 6261-6262insGT and 5972C > TT1915M in exon 11, IVS16-14T > C IVS16-6T > G in exon 17, 8345A > G N2706S in exon 18 and 9266C > TT3013I in exon 23 mutations in BRCA2.[12]
Moslehi et al. (2002) studied a family with four cases of ovarian cancer and one case of BC in close relatives for common mutations in the BRCA1 and BRCA2 genes using SSCP of exons 2 and 20 of the BRCA1 gene and PTT on exon 11 of the BRCA1 gene and exons 10 and 11 of the BRCA2 gene. PTT demonstrated an abnormal result in exon 11 of the BRCA1 gene in the three sisters. Upon sequencing a novel c. 2031T >G mutation was found at codon 638 (BIC accession no. 6432). It was a nonsense mutation which leads to a truncated protein by replace Glutamic acid with a stop codon.[13]
For the first time, Pietschmannl et al. have performed a study that screened complete coding sequences and 3’ and 5’ UTR regions of BRCA1 and BRCA2 genes in Iranian BC patients. In addition, they used semi-quantitative fluorescent multiplex PCR to detect large rearrangements of the genes. The patient population was selection account of individuals from 10 unrelated high-risk families, which had at least three breast, breast and ovarian cancer cases as first-degree relatives, multiple cases as first, second and other relatives, bilateral BC, and early onset of breast and/or ovarian cancer (<50 years). They found one intronic variation and a deletion/insertion insertion in the 3’ untranslated region of BRCA1 in cases of 2 investigated families and 2 pathogenic mutations in the BRCA2 gene, which one of them was a novel deletion (c. 4415_4418delAGAA).[14]
Quintana-Murci et al. have conducted a study to assess the prevalence of Tyr978X BRCA1 germline mutation in the general population of Iranian non-Jewish individuals and compare the BRCA1-linked haplotype of Jewish and non-Jewish mutation carriers. The population was 442 men who were unselected for personal or familial history of cancer. They were originated from different Iranian regions, including Zagros Mountains (Kordestan, Lorestan, Elam and Khuzestan), West Caspian (Gilan), East Caspian (Mazandaran), Central-North (Zanjan, Markazi, Hamadan and Semnan), Central-South (Fars, Esfahan, Hormozgan), and Eastern provinces (Khorasan, Baluchestan and Kerman). The RFLP-PCR evaluations results have shown that Tyr978X BRCA1 germline mutation not exists in any of the total 442 non-Jewish Iranian men.[15]
Mehdipour et al. have conducted a study of 400 case subjects with primary BC (396 women and 4 men with the mean age of 48.8 ± 11.3 year, age range 15-95 year) to explore the contribution three Ashkenazi founder mutations (185delAG and 5382insC in BRCA1 and 6174delT in BRCA2). There was a positive family background of BC and other malignancies in 27.5% and 52% of patient pedigrees, respectively. The most frequent occurrence of BC across four generations revealed to be 50% in the 1st degree in the 3rd generation, 68.8% in the 2nd degree in the 2nd generation, and 59.5% in the 3rd degree in the 3rd generation. They have found only two patients with 185delAG mutation in the BRCA1 gene (2/400), which they were two sisters of the one family. However, they did not found the other two mutations, that is, 5382insC in BRCA1 gene and 6174delT in BRCA2 gene.[16]
Rassi et al. (2008) performed a study to determine the prevalence three Ashkenazi founder mutation (185delAG and 5382insC in BRCA1, and 6174delT in BRCA2), using 34 formalin fixed, paraffin embedded breast tissue from 16 patients with familial BC and 18 patients with non-familial BC. A total of three mutations of Ashkenazi 5382insC founder mutation were found in 16 familial BCs.[17]
Fattahi et al. have conducted a case–control study to detection of 5382insC and 185delAG in BRCA1 and 6174delT in BRCA2 by a multiplex PCR with allele-specific oligonucleotide primers. The study population was 250 women with sporadic BC, 55 women with a familial history of BC in their first degree-relatives and 200 healthy women. Their evaluation indicated that the mutations were detected neither in patients (250 patients with sporadic BC and 55 familial BC patients) nor in 200 healthy individuals.[18]
Saleh-gohari et al. (2012) have studied 27 females and three males with BC living in Kerman province, Iran. The exon 2 and partial regions covering 11 regions of the BRCA1 gene were screened for mutations by direct sequencing. Nine different mutations that were detected include: Deletion of one adenine (c. 1017delA) and insertion of one cytosine (c. 969InsC) have found as the most frequent (20%) mutation in this survey. A substitution of thymine for adenine (c. 999T > A) has detected as the second common BRCA1 gene defect (6.7%). The other mutations have identified as single nucleotide replacement including: c. 792A > C, c. 825G > C, c. 822T > A, c. 1068A > G, c. 969A > T and c. 966T > C.[19]
Keshavarzi et al. studied 27 patients with either early onset BC (at age ≤35 year) or personal and/or family history of breast or ovarian cancer. All of the BRCA1 and BRCA2 genes except exons 1 and 4 in BRCA1 and exon 1 in BRCA2 were analyzed. They identified a total of 13 missense mutations, 9 in BRCA1 and 4 in BRCA2. Two of these were novel (c. 3538A > G in BRCA1 and c. 4350G > A in BRCA2). In addition, c. 3232G > A and c. 3538A > G BRCA1 mutations were found in large series of breast and ovarian cancer and matched controls.[20]
In another study, Keshavarzi et al. investigated entire coding sequences and each intron/exon boundaries of BRCA1/2 genes in 85 patients from high risk Iranian families. Thirty-six patients had a family history of BC, while 49 patients had early onset BC (<35 years) and had not previous family history of the breast or ovarian cancer. They found a higher incidence of BRCA mutations (32 BRCA1 and 6 BRCA2), which 21 mutations were novel mutations (17 BRCA1 and 2 BRCA2) and have not been previously reported. The majority of the mutations are located on exon 2 (13) and 11 (7) of BRCA1. Their results cleared that 8 BRCA1 and 1 BRCA2 mutations have found in seven of the patients with early onset BC. The co-existence of two different mutations in BRCA1 (c. 550T > A) and BRCA2 (c. 2600-70T > G) were identified in one patient with early BC and one control. In addition, a missense mutation within exon 11 of the BRCA1 (c. 3419GA) was identified in 20% of patients and 8% of controls.[21]
Kooshyar et al. have studied 39 patients with BC and 29 high risk healthy women, related to the patients to find to find 185delAG and 5382insC founder mutations. In addition, a 251bp fragment of BRCA1's exon 11 was analysed to determination new mutations. They found that 185delAG and 5382insC founder mutations exist in both groups studied. Two out of 39 BC patients (5.1%) and 1 out of 29 relatives (3.4%) were carriers of 185delAG mutations, and 1 patient (2.6%) was a carrier of a 5382insC mutation. In addition, 2 patients (5.1%) and 3 (10.3%) of relatives were carriers of unclassified mutations in the BRCA1 gene 251bp fragment[22] [Tables 1 and 2].
Table 1.
Descriptive characteristics of 13 studies on the BRCA1 mutations in Iranian breast cancer patients
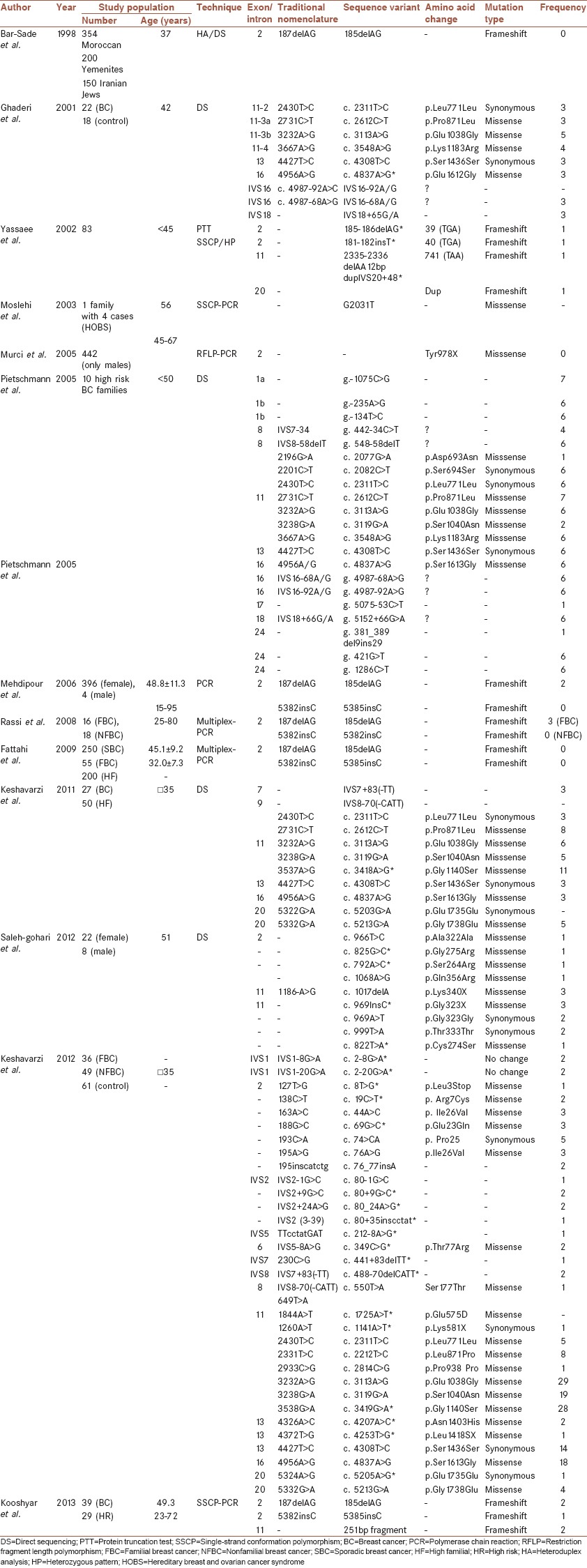
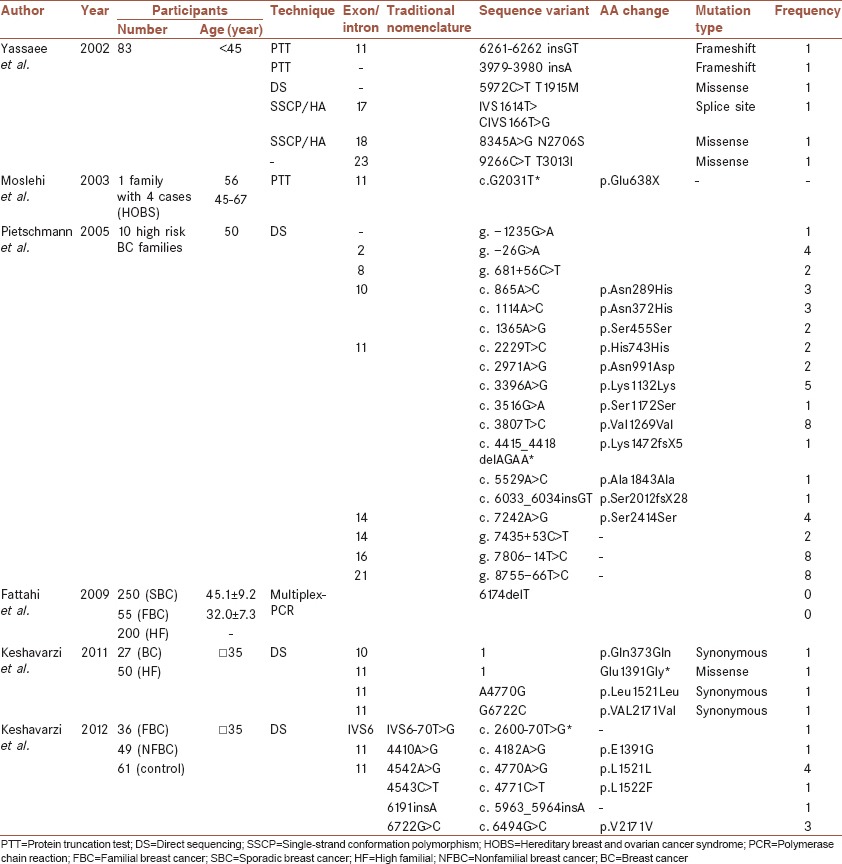
Table 2.
Descriptive characteristics of 6 studies on the BRCA2 mutations in Iranian breast cancer patients
DISCUSSION
The present review provides the identified BRCA mutations rates in Iranian BC patients to date. The 13 studies included in this study, screened a total of 1183 and 454 female and male BC patients, respectively [Tables 1 and 2].
The prevalence of BRCA mutations carriers in the general population is estimated at between 0.12% and 0.1%.[23] It is estimated that in all women, the prevalence of BRCA1 mutation is 1 in 800-1 in 1400 and the prevalence of BRCA2 mutation is slightly lower at 1 in 450-1 in 80).[24] Genetic linkage analyses have shown that the prevalence of BRCA gene mutation in familial BC and/or ovary cancer rate ranging from 45% to 90%. While, many of screening studies have shown BRCA1 mutation rate is about 6-45% and in familial BC varies from 1% to 35% worldwide.[25,26,27] Among early onset familial cases, 10-40% was found to be associated with BRCA1 and BRCA2 mutations. In contrast, among sporadic early-onset BC patients, the frequency of BRCA1/2 mutation ranges from 1% to 10%.[28]
Of the total of 1183 patients who were included in the studies 377 cases at least had a mutation in the BRCA1 gene. Therefore, based on the previous studies, the overall BRCA1 mutation rate in Iranian BC patients with various levels of family history range (with or without BC diagnosed in relatives) was estimated 31.8% (377/1183). While, this gene mutation rate for male patients is less than 0.01%. This is comparable to that of Algerian and Tunisian families BRCA1 mutation frequency, which were reported 36.4% and 37.5%, respectively. The prevalence of BRCA1 mutations reported in a study conducted on French hereditary BC and/or OC families (10.3%) is approximately 3 times less than that estimated for our community.[29] This high prevalence may be due to limited particular region of the genes, and the techniques were used.
Identification of BRCA mutations in a substantial proportion of Iranian patients indicates that these genes play a role in the incidence of BC in the Iranian population. In addition, According to these studies, there is heterogeneity in BRCA mutations in Iranian BC patients like other population.
Results shown that a total of 104 BRCA1/2 distinct mutations were identified in the interim 13 articles analysis among 377 females BC patients with or without family history, which 71 (68.8%) mutations were in BRCA1, and 33 (31.2%) were in BRCA2. Thirty-two mutations were putatively novel mutations that previously not reported. Of these, 28 of 71 in BRCA1 (39.4%) and 4 of 33 in BRCA2 (12.2%) were putatively novel mutations which previously not reported. Most of the novel mutations were missense and identified in exon 11.
As shown in Tables 3 and 4, the most common recurrent mutations in Iranian BC patients, which were repeatedly reported twice or more in different articles included: c. 4837A > G, c. 3419G > A, c. 3119G > A, c. 2612C > T, c. 3113A > G, c. 2311T > C, c. 4301T > C and c. 4308T > C in BRCA1, c. 4771C > T and c. 6494G > C in BRCA2. However, BRCA1 c. 3419G > A mutation was identified as a novel mutation, but its prevalence was higher than expected (28/377).
Table 3.
Incidence of more frequent BRC1 mutations in the Iranian BC patients
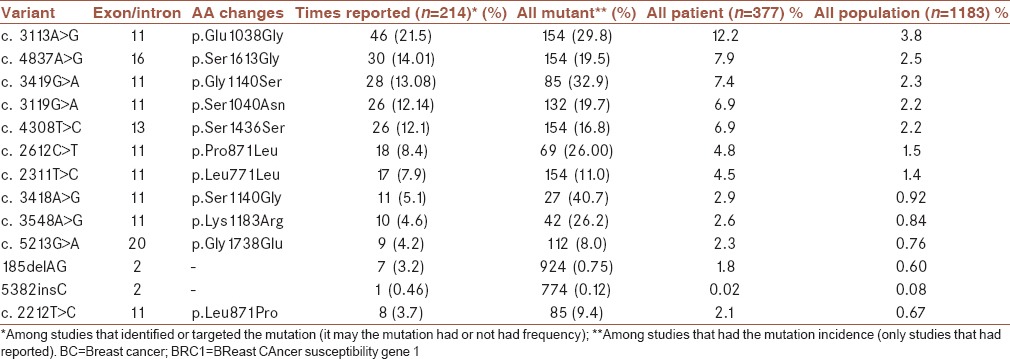
Table 4.
Incidence of recurrent BRC1 mutations in the Iranian Breast Cancer patients
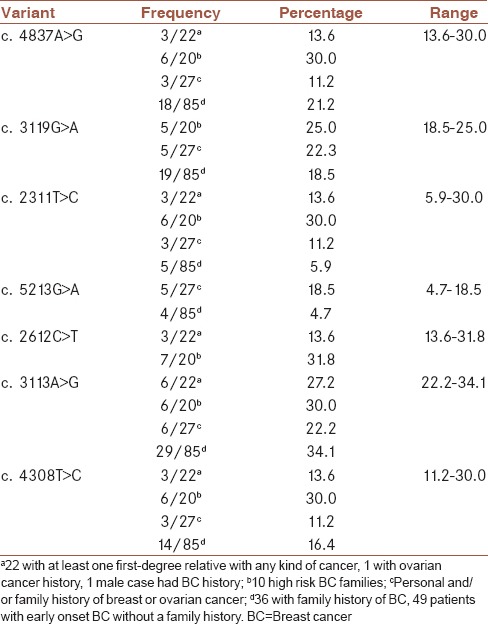
The frequency range of seven common mutations is shown in Table 4. The frequency range for c. 4837A > G was between 13.6 and 30.0, for c. 3119G > A was between 18.5 and 25.0, for c. 2311T > C was between 5.9 and 30.0, for c. 5213G > A was between 4.7 and 18.5, for c. 2612C > T was between 13.6 and 31.8, for c. 3113A > G was between 22.2 and 34.1, and for c. 4308T > C was between 11.2 and 30.0.
To the best of our knowledge, it has not introduced a founder mutation in Iranian breast and ovarian patients yet. Therefore, these mutations could represent candidate founder mutations and support testing these mutations at least for those with a family history of BC.
The effect of most of the BRCA mutations on protein is unknown and making it difficult to predict the consequences on risks of breast and ovarian cancers. Thus, many individuals undergoing genetic testing for BRCA mutations receive test results reporting a variant of uncertain clinical significance, leading to issues in risk assessment, counseling, and preventive care.[30] Based on the virtual analyses of functional compatibility for amino acid changes using SIFT and GVGD programs, 4 of the 8 most frequent variants in BRCA1 (i.e. p.Ser1613Gly, p.Ser1040Asn, p.Pro871Leu, and p.Glu1038Gly) were predicted to have an impact on protein structure (Align-GVGD, http: www.//agvgd.iarc.fr/) and SIFT (http://www.sift.bii.a-star.edu.sg/).[31]
In well-defined populations based on ethnicity, founder mutations in the BRCA1 and BRCA2 genes have been found to account for a higher proportion of breast and ovarian cancer than in the general population. Three specific mutations (185delAG, 5382insC in BRCA1, and 6174delT in BRCA2 occur in 36% of breast/ovarian cancer families. Interestingly, it is reported that 185delAG mutation occurs at a very high frequency of 18.0% in families of Ashkenazi Jews with breast/ovarian cancer. This mutation also occurs at a frequency of 1% among the Ashkenazi general population.[32] Based on the previous studies results, Ashkenazi Jewish founder mutations 185delAG and 5382insC (BRCA1) rates among Iranian BC patients were estimated approximately 0.75% (7/924) and 0.13% (1/774), respectively. However, some studies have supported that Ashkenazi Jewish founder mutations is not restricted to this particular ethnic subgroup and occurs in non-Ashkenazi Jewish ethnic groups at rates similar to the Ashkenazi population, with a similar genetic background for all Jewish mutation carriers. These mutations are not frequent mutation in Iranian BC patients.[10]
According to the Pietschmann et al. (2009) and Keshavarzi et al. (2012) studies, which have sequenced most coding regions of BRCA1 and BRCA2, Exons 2 and 11 in BRCA1 harbor 13.2% (7/53) and 28.3% (15/53) of the BRCA mutations, respectively.[14,21] For the BRCA2, the overall frequency of 4075delGT was 0.02 (95% CI: 0.00–0.03, P = 0.51 for heterogeneity test).
CONCLUSION
Until date, no other such analysis study on BC in Iran has been published. The major advantage of this review is help to determining the spectrum of BRCA mutations in Iranian BC patients and must be strengthened with further studies with a larger cohort in order to determine the rate of the BRCA mutations in the Iranian general population and to determine the existence of founder mutations. Although, these studies were limited by some reasons, they are useable to provide appropriate cancer prevention, screening, and counseling strategies based on the mutation data. Therefore, a new BC risk assessment based BRCA mutations data were created for the Iranian population.
AUTHOR'S CONTRIBUTION
All authors equally contributed in the conception of the work, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work. HN contributed in the conception of the work, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work. SMS contributed in the conception of the work, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work. SMK contributed in the conception of the work, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Abdulrahman GO, Jr, Rahman GA. Epidemiology of breast cancer in Europe and Africa. J Cancer Epidemiol 2012. 2012:915610. doi: 10.1155/2012/915610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mousavi SM, Gouya MM, Ramazani R, Davanlou M, Hajsadeghi N, Seddighi Z. Cancer incidence and mortality in Iran. Ann Oncol. 2009;20:556–63. doi: 10.1093/annonc/mdn642. [DOI] [PubMed] [Google Scholar]
- 3.Heidari Z, Mahmoudzadeh-Sagheb HR, Sakhavar N. Breast cancer screening knowledge and practice among women in southwest of Iran. Acta Med Iran. 2008;46:321–8. [Google Scholar]
- 4.Kolahdoozan S, Sadjadi A, Radmard AR, Khademi H. Five common cancers in Iran. Arch Iran Med. 2010;13:143–6. [PubMed] [Google Scholar]
- 5.Harirchi I, Kolahdoozan S, Karbakhsh M, Chegini N, Mohseni SM, Montazeri A, et al. Twenty years of breast cancer in Iran: Downstaging without a formal screening program. Ann Oncol. 2011;22:93–7. doi: 10.1093/annonc/mdq303. [DOI] [PubMed] [Google Scholar]
- 6.Antoniou AC, Gayther SA, Stratton JF, Ponder BA, Easton DF. Risk models for familial ovarian and breast cancer. Genet Epidemiol. 2000;18:173–90. doi: 10.1002/(SICI)1098-2272(200002)18:2<173::AID-GEPI6>3.0.CO;2-R. [DOI] [PubMed] [Google Scholar]
- 7.Ford D, Easton DF, Stratton M, Narod S, Goldgar D, Devilee P, et al. Genetic heterogeneity and penetrance analysis of the BRCA1 and BRCA2 genes in breast cancer families. The Breast Cancer Linkage Consortium. Am J Hum Genet. 1998;62:676–89. doi: 10.1086/301749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Karami F, Mehdipour P. A comprehensive focus on global spectrum of BRCA1 and BRCA2 mutations in breast cancer. Biomed Res Int 2013. 2013:928562. doi: 10.1155/2013/928562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nelson HD, Huffman LH, Fu R, Harris EL. U.S. Preventive Services Task Force. Genetic risk assessment and BRCA mutation testing for breast and ovarian cancer susceptibility: Systematic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med. 2005;143:362–79. doi: 10.7326/0003-4819-143-5-200509060-00012. [DOI] [PubMed] [Google Scholar]
- 10.Bar-Sade RB, Kruglikova A, Modan B, Gak E, Hirsh-Yechezkel G, Theodor L, et al. The 185delAG BRCA1 mutation originated before the dispersion of Jews in the diaspora and is not limited to Ashkenazim. Hum Mol Genet. 1998;7:801–5. doi: 10.1093/hmg/7.5.801. [DOI] [PubMed] [Google Scholar]
- 11.Ghaderi A, Talei A, Farjadian S, Mosalaei A, Doroudchi M, Kimura H. Germline BRCA1 mutations in Iranian women with breast cancer. Cancer Lett. 2001;165:87–94. doi: 10.1016/s0304-3835(01)00394-9. [DOI] [PubMed] [Google Scholar]
- 12.Yassaee VR, Zeinali S, Harirchi I, Jarvandi S, Mohagheghi MA, Hornby DP, et al. Novel mutations in the BRCA1 and BRCA2 genes in Iranian women with early-onset breast cancer. Breast Cancer Res. 2002;4:R6. doi: 10.1186/bcr443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Moslehi R, Kariminejad MH, Ghafari V, Narod S. Analysis of BRCA1 and BRCA2 mutations in an Iranian family with hereditary breast and ovarian cancer syndrome. Am J Med Genet A. 2003;117A:304–5. doi: 10.1002/ajmg.a.10031. [DOI] [PubMed] [Google Scholar]
- 14.Pietschmann A, Mehdipour P, Mehdipour P, Atri M, Hofmann W, Hosseini-Asl SS, et al. Mutation analysis of BRCA1 and BRCA2 genes in Iranian high risk breast cancer families. J Cancer Res Clin Oncol. 2005;131:552–8. doi: 10.1007/s00432-005-0678-8. [DOI] [PubMed] [Google Scholar]
- 15.Quintana-Murci L, Gal I, Bakhan T, Quach H, Sayar SH, Shiri-Sverdlov R, et al. The Tyr978X BRCA1 mutation: Occurrence in non-Jewish Iranians and haplotype in French-Canadian and non-Ashkenazi Jews. Fam Cancer. 2005;4:85–8. doi: 10.1007/s10689-004-2101-z. [DOI] [PubMed] [Google Scholar]
- 16.Mehdipour P, Hosseini-Asl S, Savabi EA, Habibi L, Ehsan Alvandi E, Atri M. Low frequency of 185delAG founder mutation of BRCA1 gene in Iranian breast cancer patients. J Cancer Mol. 2006;2:123–7. [Google Scholar]
- 17.Rassi H, Houshmand M, Hashemi M, Majidzadeh K, Akbari MH, Panahi MS. Application of multiplex PCR with histopathologic features for detection of familial breast cancer in formalin-fixed, paraffin-embedded histologic specimens. Tsitol Genet. 2008;42:55–62. [PubMed] [Google Scholar]
- 18.Fattahi MJ, Mojtahedi Z, Karimaghaee N, Talei AR, Banani SJ, Ghaderi A. Analysis of BRCA1 and BRCA2 mutations in southern Iranian breast cancer patients. Arch Iran Med. 2009;12:584–7. [PubMed] [Google Scholar]
- 19.Saleh Gohari N, Mohammadi-Anaie M, Kalantari-Khandani B. BRCA1 gene mutations in breast cancer patients from Kerman Province, Iran. Iran J Cancer Prev. 2012;5:210–5. [PMC free article] [PubMed] [Google Scholar]
- 20.Keshavarzi F, Noughani AE, Ayoubian M, Zeinali S. Sequence variants of BRCA1 and BRCA2 genes in four Iranian families with breast and ovarian cancer. Iran J Public Health. 2011;40:57–66. [PMC free article] [PubMed] [Google Scholar]
- 21.Keshavarzi F, Javadi GR, Zeinali S. BRCA1 and BRCA2 germline mutations in 85 Iranian breast cancer patients. Fam Cancer. 2012;11:57–67. doi: 10.1007/s10689-011-9477-3. [DOI] [PubMed] [Google Scholar]
- 22.Kooshyar MM, Nassiri M, Mahdavi M, Doosti M, Parizadeh A. Identification of germline BRCA1 mutations among breast cancer families in Northeastern Iran. Asian Pac J Cancer Prev. 2013;14:4339–45. doi: 10.7314/apjcp.2013.14.7.4339. [DOI] [PubMed] [Google Scholar]
- 23.Balmaña J, Díez O, Rubio IT, Cardoso F. ESMO Guidelines Working Group. BRCA in breast cancer: ESMO Clinical Practice Guidelines. Ann Oncol. 2011;22(Suppl 6):vi31–4. doi: 10.1093/annonc/mdr373. [DOI] [PubMed] [Google Scholar]
- 24.Bougie O, Weberpals JI. Clinical considerations of BRCA1- and BRCA2-mutation carriers: A review. Int J Surg Oncol 2011. 2011:374012. doi: 10.1155/2011/374012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Moatter T, Aban M, Khan S, Azam I, Pervez S. BRCA1 status in Pakistani breast cancer patients with moderate family history. J Coll Physicians Surg Pak. 2011;21:680–4. [PubMed] [Google Scholar]
- 26.Song CG, Hu Z, Yuan WT, Di GH, Shen ZZ, Huang W, et al. BRCA1 and BRCA2 gene mutations of familial breast cancer from Shanghai in China. Zhonghua Yi Xue Yi Chuan Xue Za Zhi. 2006;23:27–31. [PubMed] [Google Scholar]
- 27.De Leon Matsuda ML, Liede A, Kwan E, Mapua CA, Cutiongco EM, Tan A, et al. BRCA1 and BRCA2 mutations among breast cancer patients from the Philippines. Int J Cancer. 2002;98:596–603. doi: 10.1002/ijc.10194. [DOI] [PubMed] [Google Scholar]
- 28.Carraro DM, Koike Folgueira MA, Garcia Lisboa BC, Ribeiro Olivieri EH, Vitorino Krepischi AC, de Carvalho AF, et al. Comprehensive analysis of BRCA1, BRCA2 and TP53 germline mutation and tumor characterization: A portrait of early-onset breast cancer in Brazil. PLoS One. 2013;8:e57581. doi: 10.1371/journal.pone.0057581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Laraqui A, Uhrhammer N, Lahlou-Amine I, El Rhaffouli H, El Baghdadi J, Dehayni M, et al. Mutation screening of the BRCA1 gene in early onset and familial breast/ovarian cancer in Moroccan population. Int J Med Sci. 2013;10:60–7. doi: 10.7150/ijms.5014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Millot GA, Carvalho MA, Caputo SM, Vreeswijk MP, Brown MA, Webb M, et al. A guide for functional analysis of BRCA1 variants of uncertain significance. Hum Mutat. 2012;33:1526–37. doi: 10.1002/humu.22150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Solano AR, Aceto GM, Delettieres D, Veschi S, Neuman MI, Alonso E, et al. BRCA1 And BRCA2 analysis of Argentinean breast/ovarian cancer patients selected for age and family history highlights a role for novel mutations of putative south-American origin. Springerplus. 2012;1:20. doi: 10.1186/2193-1801-1-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Vaidyanathan K, Lakhotia S, Ravishankar HM, Tabassum U, Mukherjee G, Somasundaram K. BRCA1 and BRCA2 germline mutation analysis among Indian women from south India: Identification of four novel mutations and high-frequency occurrence of 185delAG mutation. J Biosci. 2009;34:415–22. doi: 10.1007/s12038-009-0048-9. [DOI] [PubMed] [Google Scholar]