

Abstract
Background:
Adolescent idiopathic scoliosis (AIS) may lead to physical and mental problems. It also can adversely affect patient satisfaction and the quality of life. In this study, we assessed the outcomes and satisfaction rate after surgical treatment of AIS using scoliosis research society-30 questionnaire (SRS-30).
Methods:
We enrolled 135 patients with AIS undergoing corrective surgery. Patients were followed for at least 2 years. We compared pre- and post-operative x-rays in terms of Cobb’s angles and coronal balance. At the last visit, patients completed the SRS-30 questionnaire. We then assessed the correlation between radiographic measures, SRS-30 total score, and patient satisfaction.
Results:
Cobb’s angle and coronal balance improved significantly after surgery (P<0.001). The scores of functional activity, pain, self-image/cosmesis, mental health, and satisfaction were 27±4.3, 26±2.5, 33±5.2, 23±3.5, and 13±1.8, respectively. The total SRS-30 score was 127±13. Radiographic measures showed significant positive correlation with satisfaction and SRS-30 total scores. There was also a positive correlation between satisfaction and self-image/cosmesis domain scores.
Conclusions:
The greater the radiographic angles were corrected the higher the SRS-30 total score and patient satisfaction were. It is intuitive that the appearance and cosmesis is of most important factor associated with patient satisfaction.
Key words: Adolescent idiopathic scoliosis, Satisfaction, Scoliosis research society-30 questionnaire, Spinal deformity
Introduction
Idiopathic scoliosis (IS) is a complex three-dimensional deformity of the spinal column being the most common type of spinal curvature (1). Adolescent idiopathic scoliosis (AIS) is the most common type accounting for about 80% of idiopathic scoliosis involving healthy individuals during puberty (2, 3). The prevalence of AIS has been reported to be 0.47-5.2% of adolescent population and schoolchildren (4).
The prognosis depends on several factors including curve morphology, magnitude of curvature, age of onset, stage of bone growth, and rate of progression that varies from curve progression to stabilization or disappearance with growth (1, 5). Progression of the curves may result in several pronounced body deformities, uneven shoulders, and asymmetric waist line that subsequently leads to damaged body self image and mental health, pain, spinal degenerative changes, several limitations in activities of daily living, and in severe cases disturbed pulmonary function (5-7).
Surgical reduction of deformity may be required to improve cosmesis and self-image while improving pulmonary function, relieving pain, and preventing curve progression (8). The rate of correction utilizing new instruments is reported between 60-80% while postoperative bracing is not necessary (9-11).
It is shown that scoliosis causes mental dysfunction and psychological problems involving both the patient and the family in that the severity is not in accordance with the severity of the disease based on physical and radiographic findings (12-16). Also, several studies reported that objective success in correction is not correlated with subjective satisfaction of the patient and the family because their perception of appearance differs from that of surgeons (17, 18).
Currently, there is a trend toward evaluating subjective outcomes and quality of life reported by patients (6, 19-21). Questionnaires are self reported measures developed to demonstrate the outcomes and effects of treatment on the quality of life and satisfaction (19, 22). The scoliosis Research Society instrument (SRS 24) was a simple practical tool developed to measure the effects of surgical treatment in AIS (23). SRS-22, a modification of this tool, was presented afterwards (24). Recently, SRS-30 was introduced as a new skillful combination of SRS-24 and SRS-22 (25). In the current study, we aimed to assess the outcome of surgical treatment of AIS and to assess its correlation with patient satisfaction.
Methods
In this study, 142 patients with spinal fusion for the adolescent idiopathic scoliosis (AIS) were included between 2002 and 2008. Ethical committee approval was obtained prior to initiation of the present study. Orthotic treatment was done before surgery for all patients. Seven patients were excluded because they had a history of previous spinal surgery. We measured the magnitude of the curves and the coronal balance on preoperative anteroposterior and lateral spinal x-rays utilizing the Cobb’s method. Patients were classified based on King’s classification. Also, patients were classified using preoperative Cobb’s angle as follows:
group I: Cobb’s angle < 50 degrees (51 patients)
group II: Cobb’s angle between 50-70 degrees (39 patients)
group III: Cobb’s angle between 70-90 degrees (29)
group IV: Cobb’s angle > 90 degrees (16 patients)
Using the pre- and post-operative radiographs, we measured the percentage of change in Cobb’s angle and coronal balance. After surgery, patients were followed for at least 2 years. At the last visit, spinal radiographs were repeated to measure the curvature magnitude and coronal balance. Patients were also asked to complete the SRS-30 questionnaire that is comprised of 5 domains including function/activity (7-35 points), pain (6-30 points), self-image/cosmesis (9-45 points), mental health (5-25 points), and satisfaction with management (3-15). Maximum total score of the questionnaire is 150 with higher scores indicating better outcomes.
Statistical analysis
After checking for normality of the data, pre- and post-operative Cobb’s angles and coronal balance were compared using paired t-test and Wilcoxon test. In order to assess the correlation between changes in curve magnitude and coronal balance and SRS-30 scores, Pearson’s correlation coefficient (r) and Spearman’s rank correlation coefficient (rho) were used. Also, the correlation between satisfaction domain and other domains of SRS-30 was evaluated using Pearson’s correlation coefficient (r). The mean SRS-30 score was compared among various King’s classification using one-way ANOVA. P value < 0.05 was considered significant.
Results
One hundred and thirty five patients were available at the last follow up. Of 135 patients, 27 were male (20%) and 108 were female (80%) with a mean age of 16±4.7 years (range:11-23 years) at the time of surgery. Patients were followed for a mean of 42±33 months (range: 18 to 120 months). Postoperatively, Cobb’s angle and coronal balance improved significantly compared to the preoperative values [Table 1]. The maximum score of the SRS domains was for satisfaction followed by self-image/cosmesis [Table 2].
Table 1.
Comparison the pre- and post-operative Cobb’s angles and coronal balance
| Preoperation | Postoperation | P value | |
|---|---|---|---|
| Cobb’s angle (degree) | 61.96±45.9 | 26.54±37.2 | < 0.001 |
| Coronal balance (cm) | 1.86±1.69 | 0.88±0.55 | < 0.001 |
Table 2.
Mean of total postoperative SRS 30 score and its domains
| Domain | Score |
|---|---|
| Functional activity | 26.7±4.3 (16-35) |
| Pain | 25.9±2.5 (21-30) |
| Self-image/cosmesis | 33.3±5.2 (26-42) |
| Mental health | 22.7±3.5 (14-25) |
| Satisfaction | 13.1±1.8 (9-15) |
| Total | 126.8±12.7 (110-146) |
There was no significant difference in mean total SRS score between males and females (126±6.9 for males versus 127±8.5 for females; P=0.38). There were 16 (12%), 34 (25%), 37 (27%), 23 (17%), and 19 (14%) patients in grades I, II, III, IV, and V of King’s classification, respectively although six patients (4.4%) could not be assigned to any of these groups. There was no significant difference in total SRS score among different types of King’s classification (P=0.15) [Figure 1]. There was no correlation between the total SRS 30 score and the type of King’s classification and preoperative Cobb’s angle (P=0.42 and 0.34, respectively). However, there was a positive correlation between the percentage of curve correction and total SRS score (r=0.52, P<0.001). Although preoperative coronal balance was not correlated with the total SRS score, the rate of coronal balance correction and total SRS score showed significant positive correlation (rho=0.37; P=0.042). The mean total SRS score was significantly higher in patients with greater than 2 cm coronal balance correction compared to those with less than 2 cm correction (131±12 versus 112±7.3; P=0.031). Between SRS domains, only self-image/cosmesis was positively correlated with satisfaction (r=0.528, P<0.001). Also, the satisfaction score was positively correlated with the rate of coronal balance correction (rho=0.211, P=0.038) and percentage of curve correction (r=0.386, P=0.026).
Figure 1.
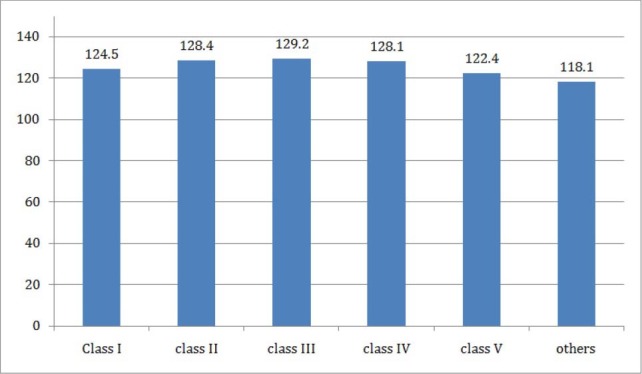
Comparing the mean of SRS 30 between different groups of King’s classification.
Discussion
AIS is a challenging and bothersome deformity that can adversely affect various aspects of the patient’s life. This deformity significantly deteriorates the ability of independently performing activities of daily living and contribution in social activities. In addition to physical health problems which can be life threatening in severe cases, the appearance of the patient especially in females, affects the mental health, self confidence, and self-image making them avoid participation in groups of family, school, university, and other public societies. The negative effects of AIS on psychological conditions and quality of life have been shown in several studies (12-16).
Because of severe impacts scoliosis has on satisfaction and quality of life, several studies tried to determine the effects of treatment on these parameters. To achieve this goal, SRS questionnaire became a useful tool, which was validated in several previous studies (22, 26-29). In a study by Bridwell et al, SRS was more responsive to changes at 1 and 2 years after surgery compared to Oswestry disability index (ODI) and short form-12 (SF-12) (30).
In the current study, we found that the rates of curve correction and coronal balance correction can significantly affect the total SRS-30 score. Also, we found that the rate of correction was positively correlated with satisfaction. In other words, the greater correction results in more satisfaction and better quality of life. Between SRS domains, we found that only self-image was positively correlated with satisfaction. Based on this finding, we think that cosmesis and appearance is the most important factor affecting patient’s satisfaction and quality of life. Although patients with AIS travail from the pain and functional limitations, it seems that the most important obsession of these patients is the appearance which should be considered in treatment planning.
Recently, Omidi Kashani et al investigated the clinical outcomes of surgical treatment of spinal deformities (congenital scoliosis, idiopathic scoliosis and Scheuerman’s kyphosis). They found that surgery was associated with improved patient’s self-image, psychology, and satisfaction while pain and function remained unchanged. In their study, the total SRS score improved significantly after surgery (31). In a study by Carreon et al, the surgical treatment of AIS was associated with significant improvement in all domains of SRS. Moreover, each domain showed mild to moderate positive correlation with SRS satisfaction score. They explained that this finding might be attributable to poor responsiveness of SRS tool or substantial effect of satisfaction domain (32). Gorzkowicz et al evaluated the quality of life after surgical treatment of idiopathic scoliosis and concluded that operative correction improves self-image substantially and enhances the satisfaction of the patient. They also found that physical and mental problems and pain intensity were related to location of the patient and socioeconimic status (33).
There are several factors regarding dissatisfaction or neutrality about the outcomes of treatment including preoperative physical characteristics, psychological problems, impractical assumption regarding the postoperative cosmesis, type of the curve, and high thoracic apical translation (6, 17, 19). Ameri et al found that only half of the patients with severe AIS were satisfied with the postoperative cosmesis. They showed that King II or King IV curves are associated with less correction and displeasure of the outcomes (6). In a study by Sanders et al, patients with less spinal appearance issues were less satisfied with the outcomes (34). However, in our study we found no significant difference between different types of AIS based on King’s classification.
Like other studies, our study has its own limitations. We did not have the preoperative SRS score to demonstrate the improvement after surgery. We used the Persian SRS 30 which was comprised of the SRS 22 that was already validated plus 8 more items that were added only after simple translation (27).
In conclusion, greater radiographic correction of the AIS through surgery is associated with higher satisfaction and SRS-30 scores. Satisfaction was correlated positively with self-image/cosmesis score as well. It seems that cosmesis is the most important factor affecting patient’s satisfaction after surgical treatment.
References
- 1.Gorman KF, Julien C, Moreau A. The genetic epidemiology of idiopathic scoliosis. Eur Spine J. 2012;21(10):1905–19. doi: 10.1007/s00586-012-2389-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Weiss HR, Goodall D. The treatment of adolescent idiopathic scoliosis (AIS) according to present evidence. A systematic review. Eur J Phys Rehabil Med. 2008;44(2):177–93. [PubMed] [Google Scholar]
- 3.Riseborough EJ, Wynne-Davies R. A genetic survey of idiopathic scoliosis in Boston, Massachusetts. J Bone Joint Surg Am. 1973;55(5):974–82. [PubMed] [Google Scholar]
- 4.Konieczny MR, Senyurt H, Krauspe R. Epidemiology of adolescent idiopathic scoliosis. J Child Orthop. 2013;7(1):3–9. doi: 10.1007/s11832-012-0457-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Trobisch P, Suess O, Schwab F. Idiopathic scoliosis. Dtsch Arztebl Int. 2010;107(49):875–84. doi: 10.3238/arztebl.2010.0875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ameri E, Behtash H, Mobini B, Bouzari B, Tari V. Patient satisfaction after scoliosis surgery. Med J Islam Repub Iran. 2008;21(4):177–84. [Google Scholar]
- 7.Schwab F, Dubey A, Gamez L, El Fegoun AB, Hwang K, Pagala M, et al. Adult scoliosis: prevalence, SF-36, and nutritional parameters in an elderly volunteer population. Spine (Phila Pa 1976) 2005;30(9):1082–5. doi: 10.1097/01.brs.0000160842.43482.cd. [DOI] [PubMed] [Google Scholar]
- 8.El-Hawary R, Chukwunyerenwa C. Update on Evaluation and Treatment of Scoliosis. Pediatr Clin North Am. 2014;61(6):1223–41. doi: 10.1016/j.pcl.2014.08.007. [DOI] [PubMed] [Google Scholar]
- 9.Suk SI, Kim JH, Kim SS, Lee JJ, Han YT. Thoracoplasty in thoracic adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 2008;33(10):1061–7. doi: 10.1097/BRS.0b013e31816f2888. [DOI] [PubMed] [Google Scholar]
- 10.Bullmann V, Halm HF, Niemeyer T, Hackenberg L, Liljenqvist U. Dual-rod correction and instrumentation of idiopathic scoliosis with the Halm-Zielke instrumentation. Spine (Phila Pa 1976) 2003;28(12):1306–13. doi: 10.1097/01.BRS.0000065571.58058.68. [DOI] [PubMed] [Google Scholar]
- 11.Lonner BS, Auerbach JD, Estreicher M, Milby AH, Kean KE. Video-assisted thoracoscopic spinal fusion compared with posterior spinal fusion with thoracic pedicle screws for thoracic adolescent idiopathic scoliosis. J Bone Joint Surg Am. 2009;91(2):398–408. doi: 10.2106/JBJS.G.01044. [DOI] [PubMed] [Google Scholar]
- 12.Misterska E, Glowacki M, Harasymczuk J. Personality characteristics of females with adolescent idiopathic scoliosis after brace or surgical treatment compared to healthy controls. Med Sci Monit. 2010;16(12):CR606–15. [PubMed] [Google Scholar]
- 13.Weinstein SL, Dolan LA, Cheng JC, Danielsson A, Morcuende JA. Adolescent idiopathic scoliosis. Lancet. 2008;371(9623):1527–37. doi: 10.1016/S0140-6736(08)60658-3. [DOI] [PubMed] [Google Scholar]
- 14.Danielsson AJ, Wiklund I, Pehrsson K, Nachemson AL. Health-related quality of life in patients with adolescent idiopathic scoliosis: a matched follow-up at least 20 years after treatment with brace or surgery. Eur Spine J. 2001;10(4):278–88. doi: 10.1007/s005860100309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tones M, Moss N, Polly DW., Jr A review of quality of life and psychosocial issues in scoliosis. Spine (Phila Pa 1976) 2006;31(26):3027–38. doi: 10.1097/01.brs.0000249555.87601.fc. [DOI] [PubMed] [Google Scholar]
- 16.Matsunaga S, Hayashi K, Naruo T, Nozoe S, Komiya S. Psychologic management of brace therapy for patients with idiopathic scoliosis. Spine (Phila Pa 1976) 2005;30(5):547–50. doi: 10.1097/01.brs.0000154648.53535.52. [DOI] [PubMed] [Google Scholar]
- 17.Koch KD, Buchanan R, Birch JG, Morton AA, Gatchel RJ, Browne RH. Adolescents undergoing surgery for idiopathic scoliosis: how physical and psychological characteristics relate to patient satisfaction with the cosmetic result. Spine (Phila Pa 1976) 2001;26(19):2119–24. doi: 10.1097/00007632-200110010-00015. [DOI] [PubMed] [Google Scholar]
- 18.Merola AA, Haher TR, Brkaric M, Panagopoulos G, Mathur S, Kohani O, et al. A multicenter study of the outcomes of the surgical treatment of adolescent idiopathic scoliosis using theScoliosis Research Society (SRS) outcome instrument. Spine (Phila Pa 1976) 2002;27(18):2046–51. doi: 10.1097/00007632-200209150-00015. [DOI] [PubMed] [Google Scholar]
- 19.Misterska E, Głowacki M, Harasymczuk J. Assessment of spinal appearance in female patients with adolescent idiopathic scoliosis treated operatively. Med Sci Monit. 2011;17(7):CR404–10. doi: 10.12659/MSM.881852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kinel E, Kotwicki T, Podolska A, Białek M, Stryła W. Quality of life and stress level in adolescents with idiopathic scoliosis subjected to conservative treatment. Stud Health Technol Inform. 2012;176:419–22. [PubMed] [Google Scholar]
- 21.Spanyer JM, Crawford CH, 3rd, Canan CE, Burke LO, Heintzman SE, Carreon LY. Health-Related Quality-of-Life Scores, Spine-Related Symptoms, and Reoperations in Young Adults 7 to 17 Years After Surgical Treatment of Adolescent Idiopathic Scoliosis. Am J Orthop (Belle Mead NJ) 2015;44(1):26–31. [PubMed] [Google Scholar]
- 22.Lee JS, Lee DH, Suh KT, Kim JI, Lim JM, Goh TS. Validation of the Korean version of the Scoliosis Research Society-22 questionnaire. Eur Spine J. 2011;20(10):1751–6. doi: 10.1007/s00586-011-1872-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Haher TR, Gorup JM, Shin TM, Homel P, Merola AA, Grogan DP, et al. Results of the Scoliosis Research Society instrument for evaluation of surgical outcome in adolescent idiopathic scoliosis. A multicenter study of 244 patients. Spine (Phila Pa 1976) 1999;24(14):1435–40. doi: 10.1097/00007632-199907150-00008. [DOI] [PubMed] [Google Scholar]
- 24.Asher MA, Min Lai S, Burton DC. Further development and validation of the Scoliosis Research Society (SRS) outcomes instrument. Spine (Phila Pa 1976) 2000;25(18):2381–6. doi: 10.1097/00007632-200009150-00018. [DOI] [PubMed] [Google Scholar]
- 25.Scoliosis Research Society. Adolescent idiopathic scoliosis March 31. 2009. [Accessed June 15 2011]. Available at: http://www.srs.org/professionals/education/adolescent/idiopathic .
- 26.Carriço G, Meves R, Avanzi O. Cross-cultural adaptation and validity of an adapted Brazilian Portuguese version of Scoliosis Research Society-30 questionnaire. Spine (Phila Pa 1976) 2012;37(1):E60–3. doi: 10.1097/BRS.0b013e31823c7cd6. [DOI] [PubMed] [Google Scholar]
- 27.Mousavi SJ, Mobini B, Mehdian H, Akbarnia B, Bouzari B, Askary-Ashtiani A, et al. Reliability and validity of the persian version of the scoliosis research society-22r questionnaire. Spine (Phila Pa 1976) 2010;35(7):784–9. doi: 10.1097/BRS.0b013e3181bad0e8. [DOI] [PubMed] [Google Scholar]
- 28.Rothenfluh DA, Neubauer G, Klasen J, Min K. Analysis of internal construct validity of the SRS-24 questionnaire. Eur Spine J. 2012;21(8):1590–5. doi: 10.1007/s00586-012-2169-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sathira-Angkura V, Pithankuakul K, Sakulpipatana S, Piyaskulkaew C, Kunakornsawat S. Validity and reliability of an adapted Thai version of Scoliosis Research Society-22 questionnaire for adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 2012;37(9):783–7. doi: 10.1097/BRS.0b013e318230a92d. [DOI] [PubMed] [Google Scholar]
- 30.Bridwell KH, Berven S, Glassman S, Hamill C, Horton WC, 3rd, Lenke LG, et al. Is the SRS-22 instrument responsive to change in adult scoliosis patients having primary spinal deformity surgery? Spine (Phila Pa 1976) 2007;32(20):2220–5. doi: 10.1097/BRS.0b013e31814cf120. [DOI] [PubMed] [Google Scholar]
- 31.Omidi Kashani F, Ghayem Hasankhani E, Baradaran A, Baghban N. Clinical Outcomes of Surgery in Young Patients With Spinal Deformity. Razavi Int J Med. 2015;2(4):e23878. [Google Scholar]
- 32.Carreon LY, Sanders JO, Diab M, Sturm PF, Sucato DJ Spinal Deformity Study Group. Patient satisfaction after surgical correction of adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 2011;36(12):965–8. doi: 10.1097/BRS.0b013e3181e92b1d. [DOI] [PubMed] [Google Scholar]
- 33.Gorzkowicz B, Kołban M, Szych Z. Assessment of quality of life in patients with idiopathic scoliosis treated operatively. Ortop Traumatol Rehabil. 2009;11(6):530–41. [PubMed] [Google Scholar]
- 34.Sanders JO, Carreon LY, Sucato DJ, Sturm PF, Diab M Spinal Deformity Study Group. Preoperative and perioperative factors effect on adolescent idiopathic scoliosis surgical outcomes. Spine (Phila Pa 1976) 2010;35(20):1867–71. doi: 10.1097/BRS.0b013e3181efa6f5. [DOI] [PubMed] [Google Scholar]