

Abstract
A closed loop audit of the ear nose and throat (ENT) urgent referral clinic at a London hospital was conducted assessing the number of patients reviewed, referral source, appropriateness of referral, presenting complaint and assigned follow-up appointments. Data was sourced from clinic letters and the patient appointment system over a 3-mo period. The initial cycle analysed 490 patients and the subsequent cycle 396. The initial audit yielded clinically relevant and cost effective recommendations which were implemented, and the audit cycle was subsequently repeated. The re-audit demonstrated decreased clinic numbers from an average 9.8 to 7.2 patients per clinic, in keeping with ENT United Kingdom guidelines. A 21% decrease in patient follow-up and 13% decrease in inappropriate referrals was achieved. Direct bookings into outpatient clinics decreased by 8%, due to correct referral pathway utilisation. Comparisons of all data sets were found to show statistical significance P < 0.05. We reported a total financial saving of £32490 in a period of 3 mo (£590 per clinic). We demonstrated that simple guidelines, supervision and consultant-led education which are non-labour intensive can have a significant impact on service provision and cost.
Keywords: Otorhinolaryngologic diseases, Quality of health care, Clinical audit, Practice guideline, Total quality management, Ambulatory care facilities
Core tip: The implementation of simple clinical guidelines, a transparent referral pathway to the ear nose and throat urgent referral clinic, and consultant led education to both juniors and referring specialties has demonstrated an improved service provision whilst being more cost effective and efficient.
INTRODUCTION
The ear nose and throat (ENT) urgent referral clinic is a fundamental and well established service provided by otolaryngology department. This service is heavily depended upon by primary care providers and emergency departments to avoid unnecessary admissions and inpatient reviews[1]. With Accident and Emergency presentations rising to 21.7 million in 2012/13, a fifty percent increase in the last decade, urgent referral clinics such as that provided by the ENT department are increasingly pressurised[2]. Improving the efficiency of these clinics whilst ensuring that standards are maintained is a necessary adaptation. The services provided in ENT urgent referral clinics can vary significantly from one trust to another with no gold standard or national guidelines[3]. However, historically, these clinics are booked beyond their capacity due to high service demand. This can lead to erroneous direct bookings into consultant led two week wait clinics. This has an evident threat to patient safety but also a significant financial implication. The inevitable result of this high demand is non-adherence to clinic appointments and to time, resulting in poor patient satisfaction which is a key indicator of quality of care[4]. The source of this extra demand cannot be attributed to the increasing pressures on the accident and emergency department alone. The ENT urgent referral clinic itself can generate unnecessary patient follow-up which is a well-recognised source of financial pressure as funding is typically only available for a limited number of follow up appointments.
AUDIT CYCLE
A closed loop audit was performed with implementation of new guidelines after the initial cycle, highlighting key areas of improvement. Local guidelines were constructed on the basis of our findings.
Data for each audit cycle was sourced from clinic letters, each over a period of 3 mo, conducted at Northwick Park Hospital. The initial audit analysed 490 patients and the subsequent re-audit 396 patients. The primary outcome measure of this study was the number of patients reviewed in each urgent referral clinic and whether these were in line with the standards set by ENT United Kingdom[5].
Data pertaining to the following was also evaluated: (1) the source of the original referral; (2) the presenting feature; (3) the number of follow up appointments for each patient; and (4) the appropriateness of the referrals and whether patients were diverted towards main outpatient clinics, ultimately causing a loss of funding.
Data was analysed using GraphPad prism v5.0 (San Diego, California, United States) with a P value of < 0.05 considered statistically significant.
SUMMARY OF DATA FROM INITIAL AUDIT CYCLE
All patients reviewed in the urgent referral clinic in a 3-mo period were analysed both in the initial and subsequent re-audit.
The initial audit analysed 490 patients during a 3-mo period from the urgent referral ENT clinic at Northwick Park Hospital. An average of 9.8 patients were reviewed in each clinic. Thirty-two percent (158 patients) were listed for follow up appointments after assessment in the urgent referral clinic. Twelve percent (59 patients) were direct outpatient bookings rather than registration through the “choose and book” service and therefore bypassed the appropriate referral and funding pathway. Re-referrals via the GP only consisted of 0.2% (1 patient) which is a source of income generation for the trust. Eighteen percent (89 patients) of referrals were deemed to be inappropriate for urgent referral review by a designated senior clinician and were suitable for either GP review or non-urgent ENT review. The most common presentation to the ENT urgent referral clinic was otitis externa consisting of 26% of patient reviews. The others included 16% nasal trauma, 15% removal of a foreign object and 11% with epistaxis which are consistent with similar audits conducted[3].
Based on the above findings from the initial cycle, the following guidelines were implemented: (1) clinical protocols were produced for ENT juniors regarding accepting, reviewing and organising subsequent follow up for patients; (2) clinical guidelines for the management of common ENT pathologies, i.e., otitis externa were produced (Figure 1); (3) a safety net system for earlier senior review of patients that had been followed up more than once and those who were immunocompromised[6]; (4) clear instructions to GPs on discharge paperwork from Accident and Emergency/wards requesting for an appropriate referral to a consultant led ENT clinic; (5) education regarding the follow up of patients more than once and deterrence from booking into main outpatient clinic appointments unless clinically indicated; and (6) education for local GPs and emergency department services regarding the referral pathway (combined contribute 95% of referrals received) by regular otolaryngology consultant led sessions.
Figure 1.
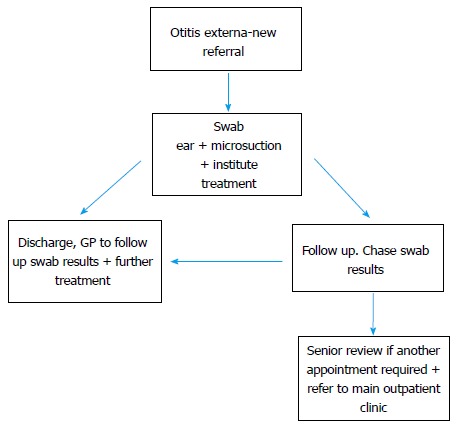
Otitis externa protocol.
SUMMARY OF DATA FROM SUBSEQUENT RE-AUDIT
The implemented guidelines overall had a significant effect on outcomes (Table 1). The number of patients per clinic decreased to 7.2. A significant decrease in the number of patient follow-ups from 32% to 11% (158 to 45 patients) was noted after the implementation of new clinical guidelines relating to common ENT presentations (Figure 2). This also led to a reduction in the number of referrals deemed to be inappropriate from 18% to 5% (89 to 21 patients). The booking of patients directly into main outpatient clinics decreased from 12% to 4% (59 to 15 patients); this was previously a significant source of financial loss. As a result of education regarding the referral system and clearer instructions to GPs, the number of re-referrals increased from 0.2% (1 patient) to 4% (15 patients).
Table 1.
Summary of data including both initial and subsequent re-audit
| Patients per clinic |
First cycle |
Re-audit |
||
|
9.8 |
7.2 |
|||
| Percentage | No. of patients | Percentage | No. of patients | |
| Follow ups | 32% | 158 | 11% | 45 |
| Direct outpatient bookings | 12% | 59 | 4% | 15 |
| Re-referrals | 0.2% | 1 | 4% | 15 |
| Inappropriate referrals | 18% | 89 | 5% | 21 |
| Total patients | 490 | 396 | ||
Figure 2.
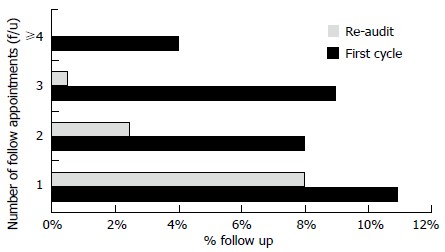
Comparison of number of follow up (f/u) appointments in first and second cycles of audit, P < 0.0001.
The above results showed statistical significance between the initial audit and the re-audit in all comparisons (P < 0.05, Table 1).
FINANCIAL IMPLICATION
The above results demonstrate a definite clinical significance, whilst simultaneously equating to a financial saving. The implemented changes described above and subsequent re-audit demonstrated a saving of £29830 over a 3-mo period. Income generated for example by re-referrals equated to £2660. Total savings amounted to £32490 over a 3-mo period, or £590 per clinic (Table 2).
Table 2.
Estimated savings and income
| Cost of follow up per patient | £190 | |
| Income per clinic patient reviewed | £190 + tariffs for procedures performed (discontinued after 2 follow ups) | |
| Re-audit | Savings £29830 | Income £2660 |
| Overall | £32490 over 3 mo | |
| £590 per clinic | ||
ROLE OF THE URGENT REFERRAL CLINIC
The fundamental role of the urgent referral clinic is variable and each NHS trust provides a different service with no pre-determined gold standard. There are no specific national guidelines which outline the remit of service which should be provided by urgent referral clinic, nor the manner in which referrals should be accepted. Similar audits have been conducted which show an improvement in service provision with a shift from open access to rapid access clinics and the formation of robust criteria to avoid what are deemed to be inappropriate referrals[3,7]. The overall common denominator is that these clinics are heavily depended on by primary and secondary care with a significant referral number. This can lead to abuse of the service and subsequently poor patient satisfaction.
SYNOPSIS OF KEY FINDINGS
Clinical activity decreased from 9.8 to 7.2 patients per clinic between each audit cycle with 21% decrease in patient follow up and 13% decrease in the number of referrals deemed inappropriate for review in the urgent referral clinic. Direct bookings into outpatient clinics decreased by 8% with a greater number of referrals taking the correct pathway. The implemented changes resulted in a total financial saving of £32490 in a period of 3-mo or £590 per clinic.
CLINICAL APPLICABILITY/CONLUSION
Urgent referral clinics are historically serviced by junior members of the ENT team which can lead to a greater duration of patient consultations but also a tendency towards greater clinical caution and therefore follow-up. This study demonstrates that the implementation of simple changes such as an established protocol (Figure 1) for the management of otitis externa (the commonest presentation), guidance and education to general practitioners and emergency department staff regarding the referral pathway, can all translate to an improvement in the service provided, by reducing clinical activity. This has subsequently resulted in a financial saving whilst maintaining a high standard of clinical care.
The results of this audit have a 2 fold consequence. A reduction in the overall number needed to be seen in the urgent referral clinic (primary outcome), with patients seen by the correct services. This volume reduction is in keeping with ENT United Kingdom guidelines and has resulted in clinics running to time, a higher patient satisfaction whilst permitting juniors to seek advice for complex cases[5]. Secondly, we have demonstrated that service improvements are not mutually exclusive to financial saving/income and one may run in parallel with the other through the implementation of simple guidelines, supervision, education and frameworks which are non-labour intensive. More globally we have highlighted the importance of clinical governance in driving forward service provision with an awareness of the finite resources available within our National Health Service.
Footnotes
Conflict-of-interest: The author reports no conflicts of interest in this work.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: January 7, 2015
First decision: February 7, 2015
Article in press: April 9, 2015
P- Reviewer: Sahu RP, Tsytsarev V S- Editor: Tian YL L- Editor: A E- Editor: Wu HL
References
- 1.Andrade JS, Albuquerque AM, Matos RC, Godofredo VR, Penido Nde O. Profile of otorhinolaryngology emergency unit care in a high complexity public hospital. Braz J Otorhinolaryngol. 2013;79:312–316. doi: 10.5935/1808-8694.20130056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.The King’s Fund. Are Accident and emergency attendances increasing [accepted Apr 29, 2013] Available from: http://www.kingsfund.org.uk/blog/2013/04/are-accident-and-emergency-attendances-increasing. [DOI] [PubMed]
- 3.Smyth C, Moran M, Diver C, Hampton S. Rapid access rather than open access leads to improved effectiveness of an ENT emergency clinic. BMJ Qual Improv Report. 2013;2:179–183. doi: 10.1136/bmjquality.u200524.w996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cairnes CB, Garrison HG, Hedges JR, Schriger DL, Valenzuela TD. Development of new methods to assess the outcomes of emergency care. Ann Emerg Med. 1998;31:166–171. [PubMed] [Google Scholar]
- 5.Cairnes CB ENTUK. Recommended numbers for ENT Clinics [accepted 2013] Available from: https://www.entuk.org/professionals.
- 6.Mirza A, McClelland L, Daniel M, Jones N. The ENT emergency clinic: does senior input matter? J Laryngol Otol. 2013;127:15–19. doi: 10.1017/S0022215112002538. [DOI] [PubMed] [Google Scholar]
- 7.Mylvaganam S, Patodi R, Campbell JB. The ENT emergency clinic: a prospective audit to improve effectiveness of an established service. J Laryngol Otol. 2009;123:229–233. doi: 10.1017/S0022215108003022. [DOI] [PubMed] [Google Scholar]