

Abstract
Background and Purpose
Clinical administration of the wrist stability, wrist mobility, and hand items of the upper extremity Fugl-Meyer (W/H UE FM) may prove a rigorous, easily administered, bedside measure of motor impairment in mildly impaired stroke survivors. The purpose of this study was to evaluate the item-structure of the W/H UE FM using Rasch analysis.
Methods
Secondary analysis of W/H UE FM data arising from clinical trials of mildly impaired stroke survivors using latent parallel analysis, ordinal factor analysis, and partial credit model Rasch analyses.
Results
Latent parallel analysis and ordinal factor analysis indicated that all W/H UE FM items represent a single unidimensional construct, wrist and hand motor ability. Rasch analysis of data from 150 mildly impaired stroke survivors (94 men; mean age, 57.1 ± 11.4y; mean time since stroke, 19.5 months) revealed that the W/H UE FM operated as a reliable, valid, and effective measure of wrist and hand motor ability. These data were compatible with Rasch model assumptions and are consistent with previous W/H UE FM research. Mass flexion and extension movements were the least difficult W/H UE FM items.
Discussion and Conclusion
The W/H UE FM is well suited to mildly impaired stroke survivors who exhibit the ability perform mass flexion and mass extension movements. The full scale UE FM may be preferable for stroke survivors with lower levels of ability.
Upper extremity (UE) hemiparesis remains one of the most common impairments exhibited among the expanding stroke survivor population,1 and frequently undermines performance of valued activities. Indeed, despite weeks of rehabilitation, 50% of stroke survivors retain some degree of UE weakness 2 and up to seventy percent remain unable to functionally use their paretic UEs 3 in the months after stroke.
Developed in 1975, the UE section of the Fugl-Meyer (UE FM) 4 remains one of the most established and widely-used 5 assessment of UE impairment in stroke. Moreover, the UE FM is recommended for use in stroke rehabilitative trials 6 and, unlike other measures of paretic UE dysfunction 7-9 only requires a few household items to administer, making it especially conducive for clinical use. Using classical test theory techniques, the psychometric reliability 10-13 and validity 14-18 of the UE FM have been shown, and support its integrated, clinical use for assessing UE impairment after stroke. Recent investigations that employ Rasch analysis also demonstrate the strength of the UE FM items themselves. For example, it is now well established that the majority of UE FM items represent the unidimensional construct of UE motor ability 19 and that the UE FM constitutes a useful tool for classifying post-stroke UE motor impairment as mild, moderate, or severe. 5
The proliferation of UE therapies targeting stroke survivors exhibiting minimal UE impairment 20-23 has necessitated the continued development and evaluation of assessment tools providing high reliability, validity, and clinical utility. Such tools are necessary because (a) clinical time is valuable and (b) recent evidence19,24 demonstrates that the traditional understanding of UE motor recovery (i.e., proximal to distal, reflexive then synergistic then isolated) is not absolute. Further, existing measures of wrist and hand motor impairment25-27 may require specialized materials, training, and may take an excessive amount of time. To address the need for a quickly administered, rigorous, bedside measure of active UE motor ability the wrist stability, wrist mobility, and hand items of the UE FM (W/H UE FM) were administered in a standardized manner to subjects with minimal28 and moderate29 UE impairment. This 12-item subset of the UE FM was recently shown to have high intrarater reliability (ICCs = 0.95), internal consistency (Cronbach α > 0.80; ordinal α > 0.80), and concurrent validity (Action Research Arm Test correlation > 0.70) in samples of mildly impaired28 and moderately impaired29 stroke survivors. These findings provide strong evidence that the W/H UE FM may prove a viable tool for efficient, reliable, and valid assessment of UE motor ability in persons with stroke who have mild and moderate impairment. Despite these promising results, it remains unclear how individual W/H UE FM items function in the population of stroke survivors exhibiting minimal UE impairment. Because individuals experiencing mild, and even moderate, UE impairment may be at risk for early supported discharge from rehabilitative services30-32 it is critical that the psychometric properties of these items be ascertained. Our overall goal was to examine the item-level psychometrics of W/H UE FM items in a population of mildly impaired stroke survivors using Rasch analysis. To accomplish this goal, the specific aims of this study were to: (a) determine whether W/H UE FM items represent a unidimensional construct, wrist and hand motor ability and (b) determine the Rasch modeled item-structure of the W/H UE FM.
Rasch analysis provides a measurement model for evaluation of categorical data based on the tenet that a total score results from the interaction of (1) person ability and (2) item difficulty.33 The first step in a Rasch analysis is to construct a scalogram. The scalogram is an ordered table of data resulting from measurement of any single attribute (e.g. wrist and hand motor ability). People are ordered from least able to most able based on their ability. Thus, person ability is given by the number of items answered correctly or points earned out of the total possible. Similarly, test items are ordered from least difficult to most difficult, with item difficulty given as the number of items endorsed out of the total possible. These data are transformed from the ordinal (i.e., categorical) level of measurement to an interval scale by means of a log-odds transformation. The resulting logits enable direct, linear, comparison of person abilities and item difficulties, a primary advantage of the Rasch model. Applied to wrist and hand motor ability, as is the case here, the probability of a person's “success for any given item depends on the difference between the ability of the person and the difficulty of the item.”33 Rasch analysis also enables evaluation of individual items using fit statistics, which reflect the alignment of each item to the construct being measured.34 Researchers use these statistics to refine new and existing instruments, examine reliability and validity, and optimize clinical utility for specific populations.
Method
Study Design
This study was a secondary analysis of data obtained during outpatient, randomized controlled trials approved by the Human Research Protection Program at The Ohio State University. The UE FM was administered on multiple occasions as part of a larger battery of outcome measures. The current study focused solely on pretest data, collected prior to randomization and to any interventions taking place.
Instruments
The battery of measures included frequently used, established, instruments administered to assess both UE impairment (i.e., active movement in each UE joint) and function (i.e., intersegmental movements put together in sequential fashion to accomplish a functional goal). Licensed therapists, acting as blinded raters at participating rehabilitation centers, administered all outcome measures. All raters were certified and re-certified on the outcome measures every three months using standardized, live, and video-based interrater reliability checks at the main study center.
The full-scale UE FM4 served as the primary outcome measure for the trials that contributed data to this study. The UE FM is a, 33-item, proximal (e.g., shoulder flexion) to distal (e.g., hook grasp) assessment of upper extremity motor impairment. Data arises from a 3-point ordinal scale (0 = cannot perform; 1 = can partially perform; 2 = can perform fully) and is often summed to yield a maximum total score of 66.
The W/H UE FM28 is a 12-item assessment (Table 1) of wrist and hand motor impairment derived from the larger, full-scale, UE FM. Items are scored using the same 3-point ordinal scale as the UE FM. Preliminary evidence supports the intrarater reliability, internal consistency, and concurrent validity of the W/H UE FM28 when used with mildly impaired stroke survivors. Standardized directions for administration of the W/H UE FM are available for scholarly and clinical use.28
Table 1.
Ordinal Exploratory Factor Analysis - Factor Pattern
| Item Number and Description | Factor Loading |
|---|---|
| Item 11: Cylindrical grasp | 0.861 |
| Item 5: Circumduction | 0.846 |
| Item 2: Wrist mobility, elbow at 90° | 0.843 |
| Item 1: Wrist stability, elbow at 90° | 0.839 |
| Item 7: Mass extension | 0.824 |
| Item 3: Wrist stability, elbow at 0° | 0.784 |
| Item 12: Spherical grasp | 0.783 |
| Item 6: Mass flexion | 0.777 |
| Item 4: Wrist mobility, elbow at 0° | 0.743 |
| Item 10: Pincer grasp | 0.637 |
| Item 9: Radial grasp | 0.624 |
| Item 8: Hook grasp | 0.477 |
Psychometric Evaluation
For the current study, the psychometric validity of the W/H UE FM was assessed using Rasch analysis.33,35 Prior to conducting any analyses employing the Rasch model, the prerequisite unidimensionality of the W/H UE FM was examined using latent parallel analysis36 and ordinal exploratory factor analysis (EFA).37 Latent parallel analysis provides a rigorous method for examining the dimensionality of measures composed of polytomous items38 and is preferred for its accuracy relative to other methods of factor extraction (i.e., Kaiser criterion, scree plot).39,40 Likewise, ordinal EFA offers advantages including utilization of all response data and robustness when data are missing.37,41 The working hypotheses were: (a) the W/H UE FM represented a unidimensional construct, wrist and hand motor ability and (b) all W/H UE FM items would load onto this single factor.
Rasch analysis conducted on the W/H UE FM used an established methodology.33,35 Specifically, examination of infit and outfit statistics enabled identification of misfitting items and persons. Fit statistics are reported as mean-square residual summary statistics (MNSQ) and reflect the degree to which data fit the Rasch model.33,35 Applied here, fit statistics reveal the extent to which the data (e.g., person abilities and item difficulties) contribute to a single construct, such as wrist and hand motor ability. As the W/H UE FM is a clinical tool, MNSQ values between 0.5 and 1.7 (i.e., standardized Z values < 2) were considered acceptable.42 Next, using these criteria to direct a process of iterative model-building and comparison, misfitting items and people were temporarily removed from the dataset.35,43 When the removal of misfitting items (or persons) improves fit to the Rasch model, a cross-plot of the person measures resulting from each model should show a poor correlation. When the removal of misfitting items (or persons) fails to improve the model, the cross-plot should reveal a strong correlation (e.g., Figure 2). In this way, misfitting items and/ or persons are systematically removed from the dataset until doing so fails to improve model fit.35,43
Figure 2.
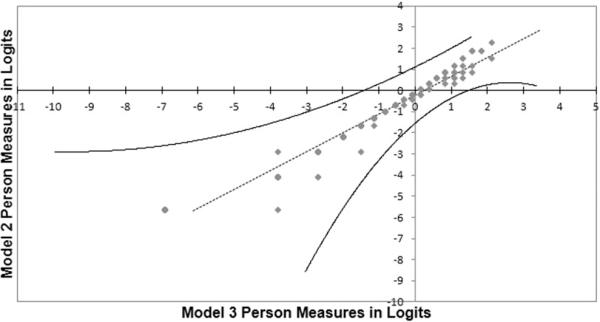
Cross-plot comparison of person measures resulting from the Rasch analysis of model 2 (140 people; 12 items) and model 3 (140 people; 10 items). The strong linear relationship depicted in the figure indicates that the removal of Items 6 and 8 did not significantly affect measurement precision.
Participants
Participants were recruited for the trials from across the Midwestern United States using active and passive recruitment strategies,44 including print advertisements placed in clinics near enrolling sites, in-services to local clinicians, and communications to local stroke support groups. As potential participants came forward, the following screening criteria were applied to determine study eligibility. Inclusion criteria were: (a) at least 10° of active flexion in the more affected wrist, and at least 2 fingers of the paretic hand; (b) experienced stroke ≥ 12 months prior to study enrollment; (c) Modified Mini-Mental Status Exam score ≥ 70;45 (d) between age 18 and 75; (e) first stroke experienced; and (f) not receiving any form of physical rehabilitation. Exclusion criteria were: (a) excessive spasticity in the more affected UE (Modified Ashworth Scale46 score ≥ 3); (b) significant pain in the more affected UE (score ≥ 5 on visual analog scale); and (c) enrollment in any rehabilitative trials.
RESULTS
Participant Demographics
Using the aforementioned study criteria, 150 subjects were determined to be eligible and included in the current analyses (94 males; mean age, 57.1 ± 11.4y; mean time since stroke, 19.5 months; 121 ischemic strokes; 78 with right hemiparesis; 105 Caucasian participants, 40 African-American, 2 Hispanic/ Latino, 2 Asian-Pacific Islander, and 1 participant of more than 1 race; UE FM mean score, 28.3 ± 12.0; mean W/H UE FM score 7.34 ± 5.44).
Dimensionality
Latent parallel analysis was conducted on W/H UE FM data for 150 mildly impaired stroke survivors. First, SAS 9.3 software (SAS Version 9.3., SAS Institute Inc.; Cary, NC) was used to create a polychoric correlation matrix of the data. The polychoric correlation is appropriate when polytomous data arises from a latent normal distribution, as is the case with the W/H UE FM. Next, the polychoric correlation matrix was used as the input for latent parallel analysis. Ten thousand random datasets that parallel the actual W/H UE FM data (i.e., 150 cases; 12 variables; 3-point scale) were created using Monte Carlo simulations in SAS. The latent parallel analysis program then computed eigenvalues for the real dataset and for each of the 10,000 randomly generated datasets. SAS then compared the real eigenvalues to those derived from the random data (Figure 1). Factors were only retained when the real eigenvalues exceeded the randomly generated values. Latent parallel analysis of the W/H UE FM data suggested extracting only 1 factor.
Figure 1.
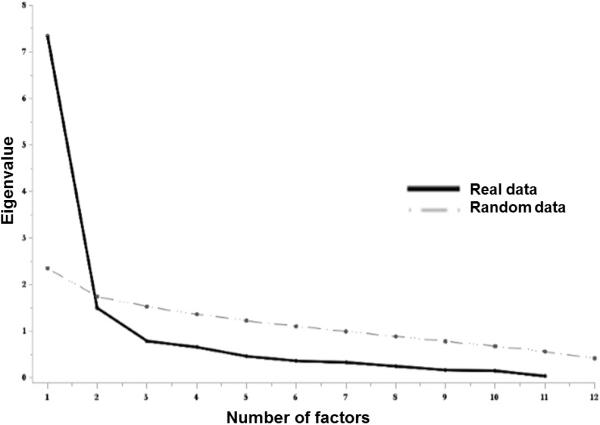
Plot of actual versus randomly generated eigenvalues. Data indicates that W/H UE FM data contribute to a single-construct, wrist and hand motor ability.
Based on the results of latent parallel analysis, the decision was made to proceed to ordinal EFA with a single factor solution. That is, only one factor was retained and EFA was performed without rotation. The SAS generated factor pattern (Table 1) indicated that all 12 W/H UE FM items had large positive loadings with the single factor retained. Items 8 and 9 (i.e., radial grasp, hook grasp) had the smallest factor loadings (0.477 and 0.624 respectively; Table 1). These findings (i.e., latent factor analysis, ordinal EFA) illustrate that the W/H UE FM is unidimensional.
Rasch Analysis
Having established the prerequisite unidimensionality, WINSTEPS 3.80.1 software (Winsteps; Version 3.80.1; JM Linacre; Beaverton, OR:) was used to conduct a Partial Credit Model (PCM)33 Rasch analysis of W/H UE FM items in a sample of mildly impaired stroke survivors. Rasch analysis conducted using the PCM allows for different Rasch-Andrich thresholds for each item. The Rasch-Andrich threshold is the boundary between two points on a scale, say 1 and 2, where the probability of selecting either option is 50%. By employing the PCM, this analysis allows for these boundaries to vary item-to-item (i.e., each item has it's own rating scale). This iterative, model- building, process35,43 (Table 2) was used to develop the final item-difficulty hierarchy that conforms to the Rasch model.33 That is, items had acceptable fit statistics and are presented from least difficult to most difficult.
Table 2.
Audit Trail for Iterative Development of Final Rasch Item Difficulty Hierarchy
| Model | Items Included | People Included | Did Model Fit Improve? | Findings |
|---|---|---|---|---|
| 1 | 1-12 | 150 | - | - |
| 2 | 1-12 | 140 | Yes | Item 6 outfit MNSQ = 2.40 |
| Item 8 outfit MNSQ = 3.88 | ||||
| 3 | 1-5, 7, 9-12 | 140 | No | Determined that items 6 & 8 did not substantially influence person measures |
| 4 | 1-12* |
Persons and items that attain the minimum measure on an instrument (i.e., in the case of persons a score of zero (0) on all items and in the case of items a score of 0 for all persons) do not contribute to measurement of the construct. Here, a total of ten (n=10) stroke survivors received scores of zero on the W/H UE FM and were temporarily removed from the analysis (model 2; 140 people, 12 items).35,43 Model 2 item-statistics identified Items 6 and 8 as misfitting (outfit MNSQ > 1.7;42 Table 2). These misfitting items were temporarily removed from the analysis, yielding model 3 (140 people; 10 items). Analysis of the cross-plot (Figure 2; strong correlation) of person measures for models 2 and 3 indicated that the removal of items 6 and 8 was unnecessary. That is, removal of items 6 and 8 did not influence person measures. Accordingly, these items were returned to the analysis.35,43 Finally, item-difficulty values were anchored43 using model 2 values and the analysis was rerun using all 150 people (model 4; includes the 10 people previously, temporarily removed). This iterative process allowed for estimation of “clean” item-difficulty and error values (e.g., values not influenced by the misfitting items; Table 3).
Table 3.
Final Anchored Item-Difficulties, Fit Statistics, and Correlations for the w/h UE FM
| w/h UE FM item | Measure* | Error | Outfit MNSQ | Observed PMC | Expected PMC |
|---|---|---|---|---|---|
| Item 9: Radial grasp | 2.10 | 0.22 | 0.60 | 0.29 | 0.28 |
| Item 8: Hook grasp | 1.92 | 0.21 | 3.88 | 0.27 | 0.32 |
| Item 4: Wrist mobility, elbow at 0° | 0.94 | 0.19 | 0.95 | 0.56 | 0.56 |
| Item 5: Circumduction | 0.75 | 0.18 | 0.60 | 0.61 | 0.56 |
| Item 10: Pincer grasp | 0.55 | 0.15 | 1.43 | 0.46 | 0.51 |
| Item 3: Wrist mobility, elbow at 90° | 0.29 | 0.15 | 0.87 | 0.54 | 0.55 |
| Item 12: Spherical grasp | −0.11 | 0.15 | 0.85 | 0.60 | 0.61 |
| Item 2: Wrist mobility, elbow at 90° | −0.34 | 0.20 | 0.80 | 0.72 | 0.70 |
| Item 11: Cylindrical grasp | −0.46 | 0.15 | 0.86 | 0.63 | 0.63 |
| Item 1: Wrist stability, elbow at 90° | −0.72 | 0.15 | 0.85 | 0.67 | 0.66 |
| Item 7: Mass extension | −1.01 | 0.21 | 0.89 | 0.75 | 0.73 |
| Item 6: Mass flexion | −3.90 | 0.27 | 2.41 | 0.65 | 0.65 |
items anchored; PMC Point-Measure Correlation
The final analysis (model 4; Figure 3; Table 3) incorporates anchored item-difficulty values (model 2) and person ability scores for all 150-stroke survivors.33 Mass flexion (Item 6; -3.90 ± 0.27 logits) and mass extension (Item 7; -1.01 ± 0.21 logits) were easiest for this sample of mildly impaired stroke survivors to perform. The radial grasp (Item 9; 2.10 ± 0.22 logits) and hook grasp (Item 8; 1.92 ± 0.21 logits) were most difficult. As W/H UE FM item difficulties exceeded person abilities for much of the sample. Person abilities for 16% of the sample (24 people) were less than -3.90 logits, the mean item difficulty value for Item 6: mass flexion, the easiest W/H UE FM item. Person abilities for another 37% of the sample (56 people) were less than -1.01 logits, the mean item difficulty value for Item 7: mass extension, the second-easiest W/H UE FM item. The standard error associated with the person measures for this group of participants ranged from 0.58 to 2.11, in contrast to values ≤ 0.54 for participants with higher abilities. Despite these limitations, comparison of the Rasch modeled expected point-measure correlations with observed correlations (Table 3) failed to reveal any differences > 0.05. This finding indicates compatibility of the final model (model 4) with Rasch modeled expectations. Further interpretation of the variable map (Figure 3) is present in the discussion.
Figure 3.
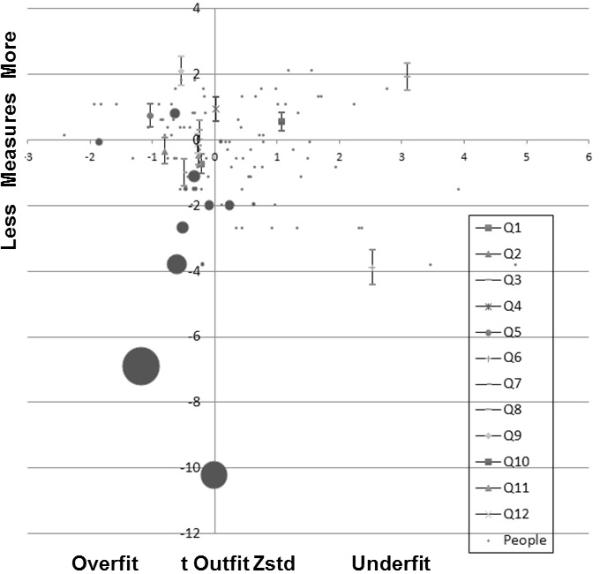
The Modified Wright Map depicts the Rasch measure value (in logits) for both persons (n=150) and items (n=12) on the vertical axis. Harder items/ more able persons appear at the top of the graph and easier items/ less able persons fall at the bottom. The horizontal axis reflects the outfit t values (μ = 0, σ = 0) for each person and item. Larger circles reflect multiple persons. For example the large circle at the bottom of the figure represents the 10 people, with zero scores, who were temporarily removed from the analysis.
Values for the person separation index, number of person strata, and test reliability of person separation of the W/H UE FM (i.e., short form) and UE FM (i.e., long form) were calculated using Rasch modeled statistics.35 The person separation index (Gp) reflects the spread of persons within the sample in units of test error.49 Gp for the W/H UE FM was 2.41, whereas it was 3.77 for the full scale UE FM. The number of person strata (Hp) was calculated using the formula Hp = (4Gp + 1)/3.35 Strata are defined as “statistically distinct levels of person ability...with centers three measurement errors apart.”35 Hp for the W/H UE FM was 3.55 and was 5.36 for the UE FM. Finally, the test reliability of person separation (Rp) was calculated using the formula . Rp reflects the proportion of observed score variance not do to chance (i.e., measurement error) and was 0.85 for the W/H UE FM and 0.93 for the UE FM.
DISCUSSION
This study examined the dimensionality and item-level function of W/H UE FM items with stroke survivors exhibiting mild UE impairment. This is a population for whom a number of promising interventions have been developed and for whom easily-administered clinical measures are needed. This psychometric evaluation of the W/H UE FM provides new data that informs usefulness of the W/H UE FM with this important, increasingly prevalent, group.
Establishing Unidimensionality
Previous research19 had established that a modified, 30-item version of the UE FM functions as a single, unified measure of upper extremity motor ability in stroke survivors exhibiting mild, moderate, or severe impairment. This positive finding supported the construct validity, clinical, and scholarly use of the UE FM with stroke survivors. However, because mildly impaired stroke survivors can usually perform most UE FM items, administration of the full-scale UE FM may prove superfluous. Consequently, the W/H UE FM was developed to address the need for a quick, easy-to-administer screening assessment of active motor ability in stroke survivors. The rigorous implementation of latent parallel analysis and ordinal EFA performed herein confirmed the working hypotheses that: (a) W/H UE FM items represent the unidimensional construct, wrist and hand motor ability and (b) all W/H UE FM items had large positive loading with this single factor. Specifically, latent parallel analysis indicated that W/H UE FM items contributed to a single factor solution and ordinal EFA confirmed that W/H UE FM items loaded onto this single factor.
Items 8 and 9 (i.e., radial grasp, hook grasp) had the smallest factor loadings, 0.477 and 0.624 respectively (Table 1). These items each test a distinct hand skill. Item 8, the hook grasp, challenges the subject to fully extend digits two through five at the metacarpophalangeal joint while simultaneously flexing at the proximal and distal interphalangeal joints. Item 9, the radial grasp, asks the subject to flex the thumb towards the second digit in an isolated fashion. Both of these skills are known to be extraordinarily challenging for stroke survivors experiencing UE motor impairment.5,19,28 That these skills are challenging may explain why they contribute the least to the unidimensional construct, wrist and hand motor ability, especially given the motor impairment levels of subjects comprising the current sample.
Item-Difficulty
Rasch analysis of the W/H UE FM provided several, unique insights related to assessment and clinical care of mildly impaired stroke survivors. While the W/H UE FM performed adequately for the majority of the sample, analysis of the final, validated Rasch model (i.e., model 4) indicated that the W/H UE FM did not precisely measure stroke survivors with relatively lower levels of ability. This finding was unanticipated. When compared to survivors of stroke with moderate and severe impairment, mildly impaired stroke survivors represent a relatively higher functioning cohort of individuals seeking rehabilitation in the weeks and months following stroke. It was expected that these individuals would demonstrate the ability to complete all W/H UE FM items.
Under the Rasch model, a measurement instrument functions best when item difficulties are well matched to the ability levels of the people being measured (i.e., mildly impaired stroke survivors). This is not observed in the data (Figure 3). While all W/H UE FM items were found to have small error values (Table 3), and thus high precision, the measurement error for people increased for those with ability scores below -1.01 logits. That is, the W/H UE FM measured individuals with relatively lower ability levels less precisely. It is not surprising then, that the clinical implication of this finding is that the W/H UE FM is less precise in measuring stroke survivors who are on the lower end of the spectrum herein included (i.e., people who met our study criteria but are more moderately impaired). Additional items, targeted at individuals with lower ability levels would likely enhance the item-level functioning of the W/H UE FM and are recommended for future research. This could likely be accomplished by adding additional items from the UE FM if the individual being tested exhibits more motor impairment than those who were included in this study.
Separation, Strata, and Reliability
Rasch modeled statistics were used to calculate the person separation index (Gp), number of person strata (Hp), and test reliability of person separation (Rp).35 The W/H UE FM was able to separate people into 3 distinct strata (Hp = 3.55), whereas the UE FM separated people into 5 strata (Hp = 5.36). Practically, this means that the UE FM is better able to distinguish mild stroke survivors based on individual differences of UE motor ability than is the W/H UE FM. Similarly, the test reliability of person separation (Rp) was greater of the full scale UE FM (Rp = 0.93), than it was for the W/H UE FM (Rp = 0.85). These findings make sense for a couple reasons. First, the modified UE FM,5,19 has 18 more items than does the W/H UE FM, all of which measure other aspects of UE motor ability. Second, it is generally accepted that reliability can be expected to increase as the length of a test increases.50
Implications for Clinical Use and Future Research
This study is the third and most advanced evaluation of the W/H UE FM to date.28,29 The final model (model 4) revealed Items 6 and 7 (i.e., mass flexion; mass extension) as the easiest W/H UE FM items. This finding is consistent with previous Rasch analyses5,19 of the UE FM, which have identified W/H UE FM items 6 and 7 as easiest to endorse. Thus, it is particularly troubling that these easiest W/H UE FM items remained too difficult for many participants. For survivors of stroke, active finger extension is a powerful predictor of UE motor recovery 51,52 and potential to benefit from neurorehabilitation.38 To date, research has failed to examine the potential predictive power of this distal motor skill from a psychometric perspective.
The present analysis is the first, of which we are aware, to reveal that mass extension may be useful from a measurement point of view as well. For example, quick bedside screening for mass extension may provide useful information for researchers and clinicians who make decisions about the need for assessment and potential to benefit from rehabilitation. While additional studies will be required, we recommend that future psychometric evaluations of the UE FM include designed, item-level analyses of this important item. While the W/H UE FM has been evaluated for use with survivors of stroke with minimal28 and moderate29 UE impairment, additional research is needed to extend these results to other populations and settings. For example, future research should evaluate the reliability and validity of the W/H UE FM in survivors of stroke who exhibit severe impairment of UE function. Similarly, the clinical utility of measurements made using the W/H UE FM during the acute, sub-acute, and chronic phases of recovery should be evaluated. It is also important that the convergent and discriminant validity of the W/H UE FM be assessed by administering it in conjunction with other tests of wrist and hand motor ability.
In the interim, we recommend that clinicians and researchers consider using the W/H UE FM with survivors of stroke who exhibit mild and moderate UE impairment. In cases where limited mass flexion and mass extension are observed, we recommend that professionals access the full scale UE FM to gather a more comprehensive picture of UE function.
Limitations
This study is limited by the following factors. The W/H UE FM data analyzed herein was collected as part of larger trials that used the UE FM. Performance may have been affected by the administration of extra items. Next, these data were collected only from stroke survivors exhibiting minimal UE impairment and do not represent the full range of UE abilities in stroke survivors. As such, these findings should be viewed as preliminary.
The limitations of the UE FM are also applicable. First, proximal functions are more heavily weighted than are distal functions, such as the wrist and hand items that compose the W/H UE FM. Second, while the instrument includes hand items, finger movement and function is not specifically assessed, a limitation that is not overcome by the W/H UE FM. Finally, previous research5,19 demonstrates that the UE FM does not always function as a single unidimensional construct. These limitations should be kept in mind when considering use of the UE FM and W/H UE FM.
CONCLUSIONS
The W/H UE FM provides a reliable, valid, rigorous, and easy-to-administer bedside assessment of wrist and hand motor ability for use with mildly impaired stroke survivors. This tool performed well in a sample of mildly impaired stroke survivors exhibiting the ability to perform mass flexion and mass extension movements. Future psychometric studies of the W/H UE FM should include examinations of Item 7: mass extension as a potentially powerful predictive tool.
Supplementary Material
Acknowledgments
SOURCES OF FUNDING: This work was partially supported by grants from the National Institutes of Health (R01AT004454-04).
Footnotes
DISCLOSURE OF ANY CONFLICTS OF INTEREST: None
STATEMENT OF PREVIOUS PRESENTATION AND/ OR PUBLICATION: This work represented herein was presented at a poster at the 2015 ACRM Conference.
Clinical Trial Registration Information: Data predate the FDAAA 801 requirements.
Contributor Information
Andrew C. Persch, Division of Occupational Therapy, The Ohio State University.
P. Cristian Gugiu, Quantitative Research, Evaluation, and Measurement, College of Education and Human Ecology, The Ohio State University.
Craig A. Velozo, Division of Occupational Therapy, Medical University of South Carolina.
Stephen J. Page, Division of Occupational Therapy, The Ohio State University..
REFERENCES
- 1.Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke Statistics—2013 update: A report from the american heart association. Circulation. 2013;127:e6–e245. doi: 10.1161/CIR.0b013e31828124ad. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kelly-Hayes M, Beiser A, Kase CS, Scaramucci A, D'Agostino RB, Wolf PA. The influence of gender and age on disability following ischemic stroke: The framingham study. Journal of Stroke and Cerebrovascular Diseases. 2003;12:119–126. doi: 10.1016/S1052-3057(03)00042-9. [DOI] [PubMed] [Google Scholar]
- 3.Gresham GE, Fitzpatrick TE, Wolf PA, McNamara PM, Kannel WB, Dawber TR. Residual disability in survivors of stroke--the framingham study. N Engl J Med. 1975;293:954–6. doi: 10.1056/NEJM197511062931903. [DOI] [PubMed] [Google Scholar]
- 4.Fugl-Meyer AR, Jääskö L, Leyman I, Olsson S, Steglind S. The post-stroke hemiplegic patient: A method for evaluation of physical performance. Scand J Rehabil Med. 1975;7:13–31. [PubMed] [Google Scholar]
- 5.Woodbury ML, Velozo CA, Richards LG, Duncan PW. Rasch analysis staging methodology to classify upper extremity movement impairment after stroke. YAPMR Archives of Physical Medicine and Rehabilitation. 2013;94:1527–1533. doi: 10.1016/j.apmr.2013.03.007. [DOI] [PubMed] [Google Scholar]
- 6.Gladstone DL, Danells CJ, Black SE. The fugl-meyer assessment of motor recovery after stroke: A critical review of its measurement properties. Neurorehabilitation & Neural Repair. 2002;16:232. doi: 10.1177/154596802401105171. [DOI] [PubMed] [Google Scholar]
- 7.Lyle RC. A performance test for assessment of upper limb function in physical rehabilitation treatment and research. International Journal of Rehabilitation Research. 1981;4:483–492. doi: 10.1097/00004356-198112000-00001. [DOI] [PubMed] [Google Scholar]
- 8.Kopp B, Kunkel A, Flor H, Platz T, Rose U, Mauritz KH, et al. The arm motor ability test: Reliability, validity, and sensitivity to change of an instrument for assessing disabilities in activities of daily living. Arch Phys Med Rehabil. 1997;78:615–20. doi: 10.1016/s0003-9993(97)90427-5. [DOI] [PubMed] [Google Scholar]
- 9.Morris DM, Uswatte G, Crago JE, Cook EW, Taub E. The reliability of the wolf motor function test for assessing upper extremity function after stroke. Archives of Physical Medicine and Rehabilitation Archives of Physical Medicine and Rehabilitation. 2001;82:750–755. doi: 10.1053/apmr.2001.23183. [DOI] [PubMed] [Google Scholar]
- 10.Duncan PW, Propst M, Nelson SG. Reliability of the fugl-meyer assessment of sensorimotor recovery following cerebrovascular accident. Phys Ther. 1983;63:1606–10. doi: 10.1093/ptj/63.10.1606. [DOI] [PubMed] [Google Scholar]
- 11.Sanford J, Moreland J, Swanson LR, Stratford PW, Gowland C. Reliability of the fugl-meyer assessment for testing motor performance in patients following stroke. Phys Ther. 1993;73:447–54. doi: 10.1093/ptj/73.7.447. [DOI] [PubMed] [Google Scholar]
- 12.Platz T, Pinkowski C, van Wijck F, Kim IH, di Bella P, Johnson G. Reliability and validity of arm function assessment with standardized guidelines for the fugl-meyer test, action research arm test and box and block test: A multicentre study. Clin Rehabil. 2005;19:404–11. doi: 10.1191/0269215505cr832oa. [DOI] [PubMed] [Google Scholar]
- 13.Wood-Dauphinee SL, Williams JI, Shapiro SH. Examining outcome measures in a clinical study of stroke. Stroke. 1990;21:731–9. doi: 10.1161/01.str.21.5.731. [DOI] [PubMed] [Google Scholar]
- 14.Poole JL, Whitney SL. Motor assessment scale for stroke patients: Concurrent validity and interrater reliability. Arch Phys Med Rehabil. 1988;69:195–7. [PubMed] [Google Scholar]
- 15.Chae J, Labatia I, Yang G. Upper limb motor function in hemiparesis: Concurrent validity of the arm motor ability test. Am J Phys Med Rehabil. 2003;82:1–8. doi: 10.1097/00002060-200301000-00001. [DOI] [PubMed] [Google Scholar]
- 16.Dettmann MA, Linder MT, Sepic SB. Relationships among walking performance, postural stability, and functional assessments of the hemiplegic patient. Am J Phys Med. 1987;66:77–90. [PubMed] [Google Scholar]
- 17.De Souza LH, Hewer RL, Miller S. Assessment of recovery of arm control in hemiplegic stroke patients. 1. arm function tests. Int Rehabil Med. 1980;2:3–9. doi: 10.3109/09638288009163947. [DOI] [PubMed] [Google Scholar]
- 18.Berglund K, Fugl-Meyer AR. Upper extremity function in hemiplegia. A cross-validation study of two assessment methods. Scand J Rehabil Med. 1986;18:155–7. [PubMed] [Google Scholar]
- 19.Woodbury ML, Velozo CA, Richards LG, Duncan PW, Studenski S, Lai S. Dimensionality and construct validity of the fugl-meyer assessment of the upper extremity. Archives of Physical Medicine and Rehabilitation. 2007;88:715–723. doi: 10.1016/j.apmr.2007.02.036. [DOI] [PubMed] [Google Scholar]
- 20.Wolf SL, Winstein CJ, Miller JP, Taub E, Uswatte G, Morris D, et al. Effect of constraint-induced movement therapy on upper extremity function 3 to 9 months after stroke: The EXCITE randomized trial. (clinical report). JAMA, The Journal of the American Medical Association. 2006;296:2095–104. doi: 10.1001/jama.296.17.2095. [DOI] [PubMed] [Google Scholar]
- 21.Page SJ, Levine P, Leonard A. Mental practice in chronic stroke: Results of a randomized, placebo-controlled trial. Stroke. 2007;38:1293–7. doi: 10.1161/01.STR.0000260205.67348.2b. [DOI] [PubMed] [Google Scholar]
- 22.Page SJ, Levine P, Leonard A, Szaflarski JP, Kissela BM. Modified constraint-induced therapy in chronic stroke: Results of a single-blinded randomized controlled trial. Phys Ther. 2008;88:333–40. doi: 10.2522/ptj.20060029. [DOI] [PubMed] [Google Scholar]
- 23.de Kroon JR, IJzerman MJ, Lankhorst GJ, Zilvold G. Electrical stimulation of the upper limb in stroke: Stimulation of the extensors of the hand vs. alternate stimulation of flexors and extensors. Am J Phys Med Rehabil. 2004;83:592–600. doi: 10.1097/01.phm.0000133435.61610.55. [DOI] [PubMed] [Google Scholar]
- 24.Crow JL, Harmeling-van der Wel BC. Hierarchical properties of the motor function sections of the fugl-meyer assessment scale for people after stroke: A retrospective study. Phys Ther. 2008;88:1554–67. doi: 10.2522/ptj.20070186. [DOI] [PubMed] [Google Scholar]
- 25.Wolf SL, Catlin PA, Ellis M, Archer AL, Morgan B, Piacentino A. Assessing Wolf motor function test as outcome measure for research in patients after stroke. Stroke. 2001;32:1635–9. doi: 10.1161/01.str.32.7.1635. [DOI] [PubMed] [Google Scholar]
- 26.Gowland C, Stratford P, Ward M, Moreland J, Torreson W, Van Hullenaar S, Barreca S, Vanspall B, Plews N. Measuring physical impairment and disability with the Chedoke-Mcmaster Stroke Assessment. Stroke. 1993;24:58–63. doi: 10.1161/01.str.24.1.58. [DOI] [PubMed] [Google Scholar]
- 27.Van der Lee JH, De Groot V, Beckerman H, Wagenaar RC, Lankhorst GJ, Bouter LM. The intra and interrater reliability of the Action Research Arm Test: A practical test of upper extremity function in patients with stroke. Archives of Physical Medicine and Rehabilitation. 2001;82:14–9. doi: 10.1053/apmr.2001.18668. [DOI] [PubMed] [Google Scholar]
- 28.Page SJ, Levine P, Hade E. Psychometric properties and administration of the wrist/hand subscales of the fugl-meyer assessment in minimally impaired upper extremity hemiparesis in stroke. Arch Phys Med Rehabil. 2012;93:2373–2376.e5. doi: 10.1016/j.apmr.2012.06.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Page SJ, Hade E, Persch A. Psychometrics of the wrist stability and hand mobility subscales of the Fugl-Meyer Assessment in moderately impaired stroke. Physical Therapy. 2015;95(1):103–8. doi: 10.2522/ptj.20130235. doi: 10.2522/ptj.20130235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Brady BK, McGahan L, Skidmore B. Systematic review of economic evidence on stroke rehabilitation services. Int J Technol Assess Health Care. 2005;21:15–21. doi: 10.1017/s0266462305050026. [DOI] [PubMed] [Google Scholar]
- 31.Fisher RJ, Gaynor C, Kerr M, Langhorne P, Anderson C, Bautz-Holter E, et al. A consensus on stroke: Early supported discharge. Stroke. 2011;42:1392–7. doi: 10.1161/STROKEAHA.110.606285. [DOI] [PubMed] [Google Scholar]
- 32.Thorsen AM, Widen Holmqvist L, von Koch L. Early supported discharge and continued rehabilitation at home after stroke: 5-year follow-up of resource use. Journal of Stroke and Cerebrovascular Diseases. 2006;15:139–143. doi: 10.1016/j.jstrokecerebrovasdis.2006.04.003. [DOI] [PubMed] [Google Scholar]
- 33.Bond TG, Fox CM. Applying the rasch model : Fundamental measurement in the human sciences. Lawrence Erlbaum Associates Publishers; Mahwah, N.J.: 2007. [Google Scholar]
- 34.Page SJ, Shawaryn MA, Cernich AN, Linacre JM. Scaling of the Revised Oswestry Low Back Pain Questionnaire. Archives of Physical Medicine and Rehabilitation. 2002;83:1579–84. doi: 10.1053/apmr.2002.34604. [DOI] [PubMed] [Google Scholar]
- 35.Wright BD, Masters GN. Rating scale analysis. Mesa Press; Chicago: 1982. [Google Scholar]
- 36.Timmerman ME, Lorenzo-Seva U. Dimensionality assessment of ordered polytomous items with parallel analysis. Psychol Methods. 2011;16:209–20. doi: 10.1037/a0023353. [DOI] [PubMed] [Google Scholar]
- 37.Muraki E, Carlson JE. Full-information factor analysis for polytomous item responses. Applied Psychological Measurement. 1995;19:73. [Google Scholar]
- 38.Fritz SL, Light KE, Patterson TS, Behrman AL, Davis SB. Active finger extension predicts outcomes after constraint-induced movement therapy for individuals with hemiparesis after stroke. Stroke. 2005;36:1172–7. doi: 10.1161/01.STR.0000165922.96430.d0. [DOI] [PubMed] [Google Scholar]
- 39.Hayton JC, James C, Allen DG, Scarpello V. Factor retention decisions in exploratory factor analysis: A tutorial on parallel analysis. Organ Res Methods. 2004;7:191–205. [Google Scholar]
- 40.O'Connor BP. SPSS and SAS programs for determining the number of components using parallel analysis and velicer's MAP test. Behavior research methods, instruments, & computers : a journal of the Psychonomic Society, Inc. 2000;32:396–402. doi: 10.3758/bf03200807. [DOI] [PubMed] [Google Scholar]
- 41.Gugiu PC, Coryn C, Clark R, Kuehn A. Development and evaluation of the short version of the patient assessment of chronic illness care instrument. Chronic Illness. 2009;5:268–76. doi: 10.1177/1742395309348072. [DOI] [PubMed] [Google Scholar]
- 42.Wright BD, Linacre JM. Reasonable mean-square fit values. Rasch Measurement Transactions. 1994;8:370. [Google Scholar]
- 43.Linacre JM. When to stop removing items and persons in rasch misfit analysis? Rasch Measurement Transactions. 2010;23:1241. [Google Scholar]
- 44.Page SJ, Persch AC. Recruitment, retention, and blinding in clinical trials. Am J Occup Ther. 2013;67:154–60. doi: 10.5014/ajot.2013.006197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Teng E, Chui HC. The modified mini-mental state (3MS) examination. J Clin Psychiatry. 1987;48:314–318. [PubMed] [Google Scholar]
- 46.Bohannon RW, Smith MB. Interrater reliability of a modified ashworth scale of muscle spasticity. Phys Ther. 1987;67:206–207. doi: 10.1093/ptj/67.2.206. [DOI] [PubMed] [Google Scholar]
- 49.Fischer WP. Reliability, separation, strata statistics. Rasch Measurement Transactions. 1992;6:238. [Google Scholar]
- 50.McDonald RP. Test Theory: A Unified Treatment. New Jersey: L. Erlbaum Associates. 1999 [Google Scholar]
- 51.Smania N, Paolucci S, Tinazzi M, Borghero A, Manganotti P, Fiaschi A, et al. Active finger extension: A simple movement predicting recovery of arm function in patients with acute stroke. Stroke. 2007;38:1088–1090. doi: 10.1161/01.STR.0000258077.88064.a3. [DOI] [PubMed] [Google Scholar]
- 52.Nijland RH, van Wegen EE, Harmeling-van der Wel BC, Kwakkel G. EPOS Investigators. Presence of finger extension and shoulder abduction within 72 hours after stroke predicts functional recovery: Early prediction of functional outcome after stroke: The EPOS cohort study. Stroke. 2010;41:745–50. doi: 10.1161/STROKEAHA.109.572065. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.