

Abstract
Cardiac myxomas are rare primary cardiac tumors that usually present with dyspnea or manifestations of systemic embolization. Coronary steal is a rare phenomenon of unbalanced blood flow that is seen primarily in patients who have undergone coronary artery bypass grafting and have subclavian artery stenosis.
We report the case of a 72-year-old woman who presented with fatigue, weakness, and exertional chest heaviness and had abnormal results on a cardiac stress test. The results of coronary angiography showed no obstructive coronary artery disease but revealed a large intracardiac left atrial mass that was supplied by 2 anomalous coronary arteries. The patient underwent successful ligation of the anomalous coronary arteries and resection of the mass, which was histologically an atrial myxoma. The patient's symptoms resolved, and results of a repeat cardiac stress test were normal.
To our knowledge, this is the first report of a highly vascularized atrial myxoma that caused coronary steal with objective evidence of ischemia, and with subsequent resolution after resection of the mass and ligation of the anomalous coronary arteries.
Keywords: Diagnosis, differential; heart atria/pathology; heart neoplasms/complications/diagnosis/surgery; myxoma/complications/diagnosis; subclavian steal syndrome/etiology; treatment outcome
Atrial cardiac myxoma, a primary cardiac tumor, has a reported prevalence of 0.0017% to 0.19% at autopsy.1 Most atrial myxomas are benign and are found incidentally. If symptoms develop, they typically manifest themselves as dyspnea or as sequelae of systemic embolization. We present a case in which a cardiac myxoma caused angina that was thought to be due to coronary steal.
Case Report
In May 2013, a 72-year-old woman with psychological depression and a remote history of stroke was evaluated by her primary care physician for worsening fatigue, weakness, and exertional chest heaviness. A transthoracic echocardiogram (TTE) showed no clear abnormalities. A regadenoson nuclear stress test revealed a moderate reversible perfusion defect in the mid and distal inferior segments that suggested coronary ischemia in the apical inferior wall. At our hospital, coronary angiography was performed. The results revealed no obstructive coronary artery disease but showed a large intracardiac mass that instantly opacified upon the administration of contrast medium. The mass was supplied by 2 anomalous arteries, one arising from the proximal left coronary artery and one from the distal right coronary artery (Fig. 1). A transesophageal echocardiogram and cardiac magnetic resonance images (MRI) confirmed the presence of a left atrial mass (Fig. 2). The initial differential diagnosis was angiosarcoma, hemangioma, or myxoma.
Fig. 1.
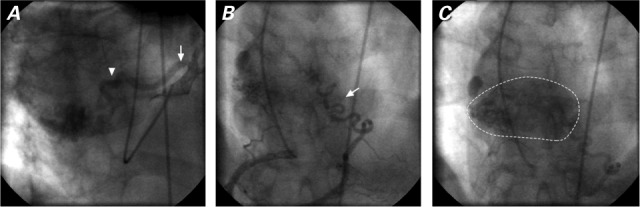
Coronary angiograms. A) The anomalous coronary artery arises from the proximal left coronary artery (arrow) that supplies the left atrial mass (arrowhead). B) Another anomalous coronary artery arises from the distal right coronary artery (arrow) that C) fully supplies the left atrial mass.
Fig. 2.
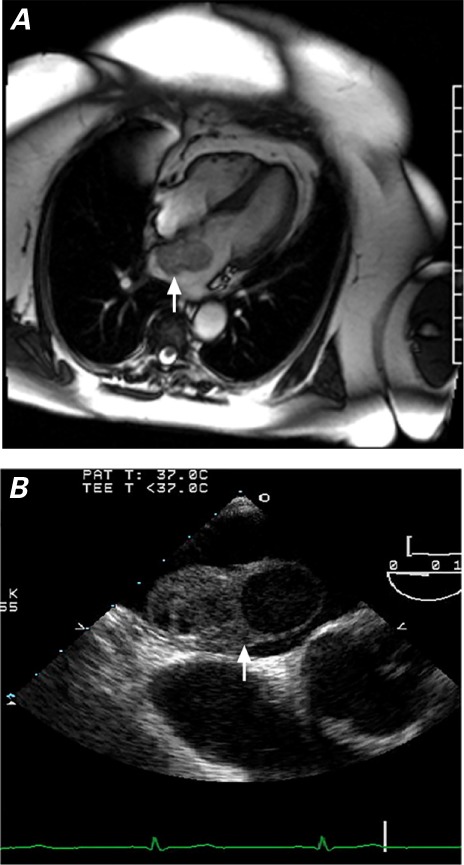
A) Cardiac magnetic resonance image (4-chamber view) and B) transesophageal echocardiogram show the left atrial mass (arrows).
The patient was scheduled for surgery. Standard aortic and bicaval cannulation was performed. Myocardial protection was provided by means of antegrade and retrograde administration of cardioplegic solution with topical and mild systemic cooling. The left atrium was approached though the intra-atrial groove. The anomalous feeder arteries were ligated and transected. The broad-based mass, which arose from the interatrial septum onto the right superior pulmonary vein orifice, was completely resected (Fig. 3A). The right superior pulmonary vein was augmented with bovine pericardium, and the atriotomy was closed with use of 2 layers of running monofilament suture. Histologically, the tumor was an atrial myxoma (Fig. 3B).
Fig. 3.
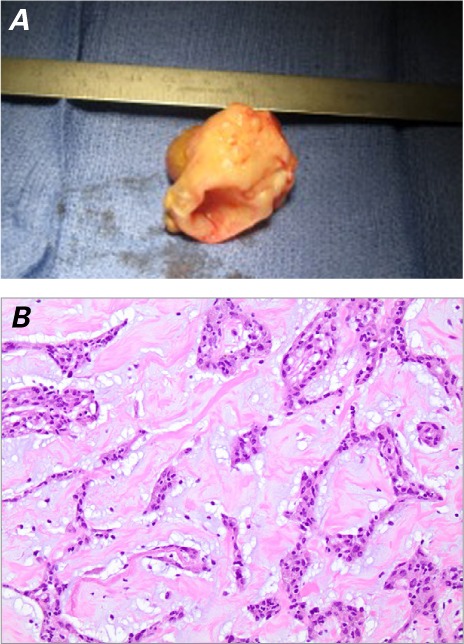
A) Photograph shows the resected left atrial mass. B) Photomicrograph shows cords and nests of bland cells in a myxoid ground substance, consistent with a myxoma (H & E, orig. × 40).
The patient recovered uneventfully and was discharged from the hospital on postoperative day 6. Upon follow-up examination 6 months later, her fatigue, weakness, and chest heaviness had completely resolved. Results of a cardiac stress test showed resolution of the inferoapical ischemia.
Discussion
The most frequently reported presentations of atrial myxoma are dyspnea and systemic embolization.1 Dyspnea is thought to occur when the tumor mass intermittently obstructs flow across the atrioventricular valves. In severe cases, the obstruction can lead to pulmonary edema and heart failure. Most myxomas arise in the left atrium, and the tumor or thrombus can embolize systemically. In one series, 30% of cases were diagnosed because of peripheral embolization.2 Rarely, patients present with myocardial infarction caused by coronary embolization.3
When atrial myxomas are seen incidentally during coronary angiography, they can appear as a blush from an anomalous artery that arises from a coronary artery. However, in our patient, the mass was easily seen as a highly vascularized structure that was fed by 2 anomalous arteries. Because of the high vascular content, the initial differential diagnosis on cardiac MRI included angiosarcoma or hemangioma. We identified, ligated, and transected the feeder vessels.
Transthoracic echocardiography is an important initial diagnostic tool and has a reported sensitivity as high as 95%.4 However, TTE did not clearly show our patient's mass, perhaps because of the myxoma's highly vascular nature.
The abnormal results of the stress test probably occurred because of unbalanced coronary blood flow during stress from the coronary-supplied myxoma. The coronary steal phenomenon classically occurs when blood is diverted from the coronary territory by traveling retrograde through an internal mammary artery bypass graft to the upper limb, as a result of substantial stenosis in or occlusion of the proximal subclavian artery.5 The concept of coronary steal caused by atrial myxoma has been reported; however, those instances were diagnosed on the basis of patients' symptoms and the flow to the myxoma upon cardiac catheterization, without evidence of ischemia on stress testing.6,7 To our knowledge, ours is the first report of a highly vascularized atrial myxoma that caused coronary steal with objective evidence of ischemia and subsequent resolution after resection of the mass and ligation of the anomalous coronary arteries.
Footnotes
From: Divisions of Cardiology, Department of Medicine (Drs. Bittenbender, Bush, and Stiver) and Cardiac Surgery (Dr. Whitson), Wexner Medical Center Department of Surgery, The Ohio State University, Columbus, Ohio 43210
References
- 1.Reynen K. Cardiac myxomas. N Engl J Med. 1995;333(24):1610–7. doi: 10.1056/NEJM199512143332407. [DOI] [PubMed] [Google Scholar]
- 2.Blondeau P. Primary cardiac tumors--French studies of 533 cases. Thorac Cardiovasc Surg. 1990;38(Suppl 2):192–5. doi: 10.1055/s-2007-1014065. [DOI] [PubMed] [Google Scholar]
- 3.Pano A., Kalangos A., Sztajzel J. Left atrial myxoma presenting with myocardial infarction. Case report and review of the literature. Int J Cardiol. 1997;62(1):73–5. doi: 10.1016/s0167-5273(97)00178-2. [DOI] [PubMed] [Google Scholar]
- 4.Percell R. L., Jr, Henning R. J., Siddique Patel M. Atrial myxoma: case report and a review of the literature. Heart Dis. 2003;5(3):224–30. doi: 10.1097/01.hdx.0000074515.95567.92. [DOI] [PubMed] [Google Scholar]
- 5.McIvor M. E., Williams G. M., Brinker J. Subclavian-coronary steal through a LIMA-to LAD bypass graft. Cathet Cardiovasc Diagn. 1998;14(2):100–4. doi: 10.1002/ccd.1810140208. [DOI] [PubMed] [Google Scholar]
- 6.Alvarez J. R., Quiroga J. S., Cereijo J. M., Lopez L. R. Coronary steal by left atrial myxoma: a case report. Cases J. 2009;2:6741. doi: 10.4076/1757-1626-2-6741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sogabe O., Inokawa H., Tanaka S., Yamamoto H., Hashimoto K. Left atrial myxoma with a coronary artery steal syndrome due to the coronary artery to left atrial fistula; report of a case [in Japanese] Kyobu Geka. 2013;66(4):341–4. [PubMed] [Google Scholar]