

Background
In breast cancer patients with apical axillary involvement, level III clearance is necessary.1,2 Access and visualisation is important if injury to neurovascular structures in the area is to be avoided. Exposure can be suboptimal in obese patients, those with extensive tumour involvement and those undergoing reoperation for level III recurrence. We report a surgical approach that facilitates safe clearance of level III lymph nodes.
Technique
Access to level III is achieved through a muscle splitting transverse incision on the pectoralis major, centred on the point where the axillary vein crosses the first rib. This is located 5cm lateral and 1cm superior to the suprasternal notch. The pectoralis minor can be retracted laterally and the neurovascular bundle to the pectoralis major can be dissected out of the surrounding fat and retracted in a silastic sling (Fig 1). This alternative approach provides excellent visualisation of level III with the corresponding portion of the axillary vein, its tributaries and the descending brachial plexus branches, allowing safe dissection of the apical axillary fat pad from the surrounding structures (Fig 1).
Figure 1.
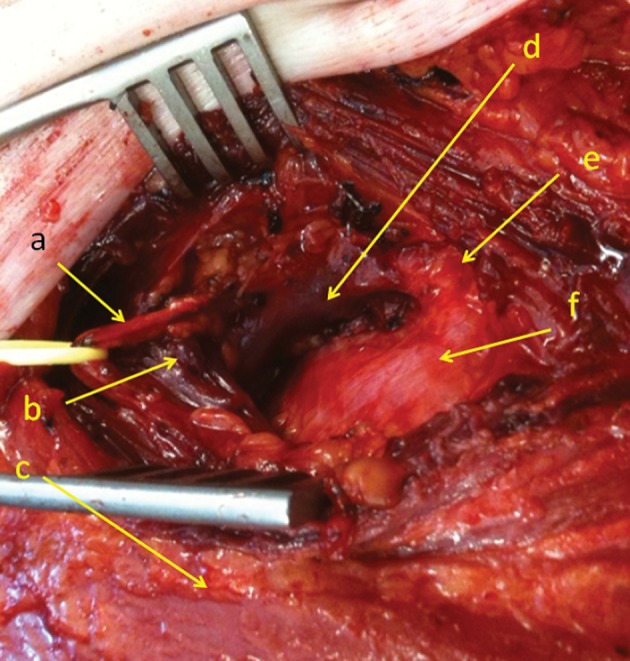
Direct transpectoral approach for level III axillary lymph node clearance. a = thoracoacromial vein + artery (pectoral branch); b = medial edge of pectoralis minor; c = pectoralis major; d = axillary vein; e = Halsted’s ligament; f = first rib
Discussion
We recommend this approach for patients undergoing a mastectomy since the muscle splitting incision can be performed without the need for a separate skin incision. We believe it is ideal for patients with level III recurrence as it allows the surgeon to access level III without having to go through previously operated levels I and II, thereby minimising the risk of nerve or vessel injury during dissection.
References
- 1.Surgical guidelines for the management of breast cancer. Eur J Surg Oncol 2009; 35 Suppl 1: 1–22. [DOI] [PubMed] [Google Scholar]
- 2.Glynn RW, Williams L, Dixon JM. A further survey of surgical management of the axilla in UK breast cancer patients. Ann R Coll Surg Engl 2010; 92: 506–511. [DOI] [PMC free article] [PubMed] [Google Scholar]