

INTRODUCTION
Mobile medical clinics (MMCs) are non-traditional healthcare strategies that increase access to care by removing geographic and social barriers associated with traditional, fixed healthcare settings. As such, they are frequently regarded as venues of convenience, delivering healthcare at the doorstep of communities that are otherwise limited by location (Leese et al. 1993, Sarnquist et al. 2011), cost (Edgerley et al. 2007), insurance status (Edgerley et al. 2007, Heller and Goldwater 2004), diverse language (Guruge et al. 2010), stigma (Whelan C 2010, Daiski 2005), or other structural barriers such as proximity and access to transportation (Hastings et al. 2007, Shannon et al. 2008, Collinson and Ward 2010).
According to the Mobile Health Map Project, there are approximately 1,500 MMCs across North America providing a variety of prevention and treatment services to 6.5 million people (Vavasis 2013). MMCs have been especially successful in addressing the geographical extremes of both rural (Peritogiannis et al. 2011, Sarnquist et al. 2011) and urban poor (Daiski 2005), where accessibility to fixed healthcare is limited due to the dearth of facilities and meager financial resources. They are also advantageous in meeting the needs of medically vulnerable populations that often experience erratic or limited healthcare in traditional settings due to underlying mental illness (Chiu and Primeau 1991), unstable housing (Collinson and Ward 2010, Amarasingham et al. 2001, Whelan C 2010), poverty, migration status (Collinson and Ward 2010, Guruge et al. 2010, Simsek et al. 2012), substance use (Thompson et al. 1998), or other stigmatized behaviors such as sex work (Shannon et al. 2008). MMCs therefore innovatively increase healthcare accessibility and reduce health disparities for communities marginalized by geographic, social, and structural barriers through delivering essential services for preventative (Jit et al. 2011, Collinson and Ward 2010, Morano et al. 2013b, Schwarz et al. 2009, Vyas et al. 2011), primary care (Leese et al. 1993, Daiski 2005, Simsek et al. 2012, Hastings et al. 2007, Pollack et al. 2002), and disease-specific care (Sarnquist et al. 2011, Maheswaran et al. 2012, Ruiz and Briones-Chavez 2010, Liebman et al. 2002, Ruiz et al. 1973, Massie 1972).
Numerous studies have analyzed healthcare utilization patterns and barriers to accessing fixed healthcare settings (e.g. emergency department, primary care, hospitals, STI clinics). These studies have focused primarily on geographic accessibility to these facilities (Acury 2005, Pilkington et al. 2012), affordability of receiving healthcare (Wang and Luo 2005, Guagliardo 2004), and the range of health services provided at these facilities (Wang and Luo 2005, Guagliardo 2004). Little research, however, has explored factors influencing access to MMCs specifically, and to our knowledge there are no prior studies that analyze the spatial distribution of MMC clients, healthcare service utilization, and frequency of MMC usage. This is particularly relevant as the Affordable Care Act (ACA) seeks to improve healthcare access for millions of Americans and will address a priori several policy-related decisions for providing services to medically marginalized populations, specifically with regard to: 1) accessibility for the optimal number and capacity of MMC sites; 2) geographic optimization for the ideal in situ location based on client demographics; 3) selection of health services offered to meet community needs and complement traditional healthcare setting services; and 4) client accommodation factors that are inclusive to those with no health insurance, uncertain immigration status, non-English speaking backgrounds, and need for walk-in appointments (Penchansky and Thomas 1981). Thus, this study is not only novel but also important in identifying populations (target location, demographic characteristics, and treatment needs) that rely upon non-traditional healthcare within a community where both MMC and fixed healthcare settings co-exist.
CONCEPTUAL FRAMEWORK
Prior work based on the Community Health Care Van (CHCV), a longstanding MMC in New Haven, Connecticut (Morano et al. 2013a, Maru et al. 2008, Altice et al. 2003, Altice et al. 2004, Morano et al. 2013b, Pollack et al. 2002) provides insight into the factors such as demographic characteristics and health conditions of clients accessing MMC services. Specifically, HIV-infected drug-using clients living more than four blocks from a MMC site were two-fold more likely to adhere to directly administered antiretroviral therapy (DAART) (Maru et al. 2008), which is now an evidence-based antiretroviral therapy (ART) adherence intervention (Thompson et al. 2012). In examining correlates of client visitation, we found a significant minority (predominantly substance users) who traveled considerably from distant towns and cities, suggesting two plausible scenarios: 1) the MMC provided services that might not have been provided in other settings; or 2) MMC clients might not have been satisfied with the services and accommodations provided at more geographically proximal, fixed healthcare settings. To address these hypotheses, a conceptual framework was developed to understand the interaction between health seeking behaviors, distance effects, and dimensions of accessing care. Thus, this study integrates concepts from the Health Behavior Model (HBM) that has been adapted for vulnerable populations (Andersen 1995, Acury 2005, Aday and Awe 1997, Gelberg et al. 2000), theories of health geography (Cummins et al. 2007, Duncan and Jones 1995, Duncan et al. 1995, Jones and Moon 1993, Joseph and Philips 1984, Kearns and Joseph 1993), and healthcare access (Penchansky and Thomas 1981, Nemet and Bailey 2000, Sherman et al. 2005) in order to identify plausible factors that motivate clients to travel long distances repeatedly in order to utilize healthcare at a MMC.
The HBM was initially developed to understand the correlates of health service utilization as a function of three types of factors: predisposing factors (e.g. demographics, social status, substance abuse), enabling resources (e.g. income, health insurance, or availability of healthcare services), and need factors (e.g. health status, severity or health beliefs) (Aday and Andersen 1974, Andersen 1995). Over time, the HBM has undergone parameterization and refinement to improve our understanding of health-seeking behaviors. For instance, Aday and Awe proposed that ‘less-discretionary’ utilization, or behaviors in response to disease and disorders (e.g. HIV/AIDS and substance use disorders [SUDs]) are primarily influenced by need factors. In contrast, ‘more-discretionary’ utilization, or behaviors that are preventive in nature, are influenced by predisposing and enabling resources (Aday and Awe 1997). To understand healthcare utilization by vulnerable populations, an additional set of factors, called vulnerable domains, were later added to the traditional HBM as predisposing (i.e. social structure such as immigration status, literacy, and social support, homelessness, SUDs, mental illness, HIV/AIDS), enabling resources (i.e. health insurance, income, competing needs, information about accessible local healthcare resources, available physicians, clinical, and treatment services), and need factors (i.e. perceived needs, medical comorbidities, and severity of illness for vulnerable population with STIs, SUDs, mental illness, and HIV/AIDS) (Gelberg et al. 2000, Stein et al. 2007).
Measures of geographic access and spatial behavior (e.g. distance, transportation availability, and activity space) have also been used to adapt the HBM based on the concepts of distance decay and space/place interactions (Acury 2005). The distance decay effect, typically observed in consumer travel behavior, has significant influence in healthcare utilization, with the most pronounced impact in rural areas, as is widely demonstrated globally in places such as Great Britain (Hine and Kamruzzaman 2012), Ireland (Teljeur et al. 2010), Ethiopia (Okwaraji et al. 2012), Mozambique (Yao et al. 2013), Vietnam (Malqvist et al. 2010), and throughout the United States (Acury 2005, Nemet and Bailey 2000, Winters et al. 2006). These studies highlight how travel distance to health services and the related costs affect an individual’s healthcare decisions and utilization patterns. Similar distance-related effects are seen in utilization of specific health services, such as hospitalization rates for cardiovascular disease (Harris et al. 2008), insulin use (Littenberg et al. 2006), methadone maintenance (Wong et al. 2010), and hepatitis C diagnosis (Monnet 2006). Despite geographic diversity and a variety of health-related outcomes, the distance decay effect seems to be largely universal with some exception in urban settings where other enabling resources, such as health insurance, and specific need factors for vulnerable population may be more important (Comber et al. 2011, Bissonnette et al. 2012).
This study further expands on the HBM by incorporating broader dimensions of accessibility to the existing enabling resources based upon Penchansky’s and Thomas’ five domains of healthcare access: availability, accessibility, accommodation, affordability, and acceptability (Penchansky and Thomas 1981). These five domains represent the degree of ‘fit’ between the client and the healthcare system, where: accessibility is client’s location versus healthcare facility location, taking into account distance, transportation, travel time, and cost; affordability is client’s ability to pay versus the cost of the healthcare service; availability is client’s healthcare need versus clinical services available; acceptability is client’s perception of health care delivery versus actual health care provider practices; and accommodation is client’s cooperation with facility site operations (appointment systems, hours of operation, walk-in-facilities, disability services, and language availability) versus the reality of how the healthcare facilities are managed. The ‘accessibility’ dimension is similar to Acury’s (2005) contribution to the HBM but the incorporation of other four dimensions makes the adapted HBM more robust.
The resulting conceptual framework (Figure 1) was then used to address the following objectives: 1) to examine the spatial distribution of clients’ self-reported residence and healthcare utilization patterns of MMC services, 2) to analyze the spatial distribution of clients with high MMC utilization (>20 visits) and their less-discretionary utilization pattern (Aday and Awe 1997); and 3) to explain plausibility for high frequency client visitation from distant areas based upon the five domains of access to healthcare (Penchansky and Thomas 1981).
Figure 1.

METHODS
Study Setting
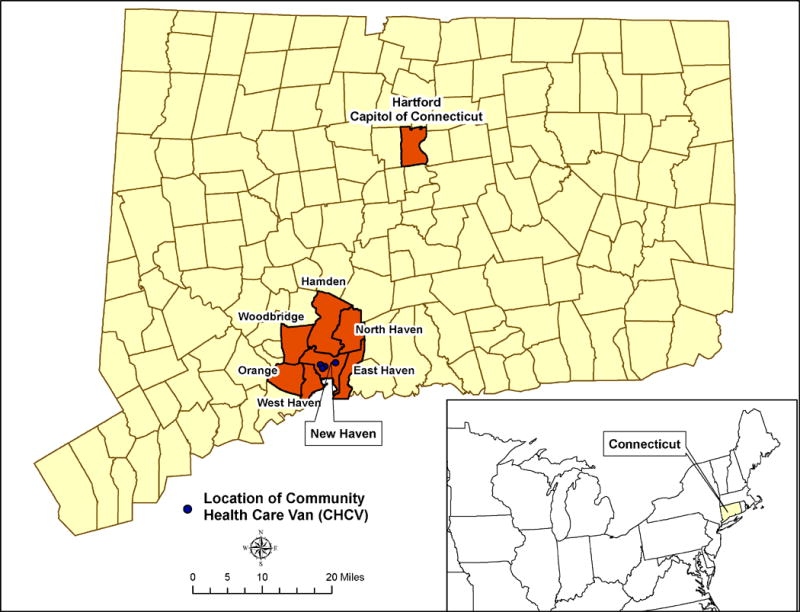
Despite Connecticut (CT) having the country’s highest per capita income for over two decades (Bureau of Business and Economic Research University of New Mexico 2013), the state faces one of the greatest income disparities (Noss 2012) and has three of the ten poorest U.S. cities for its size, including New Haven. New Haven is CT’s second largest city with 130,000 residents, and similar to other Northeast urban centers, is disproportionately impacted by substance abuse, violence, and disease-related morbidity and mortality. New Haven’s HIV prevalence is highest in the state, with 383 HIV-infected persons per 100,000 population (Centers for Disease Control and Prevention 2013), and is largely concentrated among people who inject drugs (PWID) (Connecticut Department of Public Health 2013). Needle and syringe exchange programs (NSEP) have markedly curbed HIV transmission (Heimer et al. 1993), yet they have been coupled with expansion of medication-assisted therapy (MAT), such as methadone and buprenorphine, to treat opioid dependence and reduce drug injection (Schwarz et al. 2012, Schwarz et al. 2009). There are at least 7 MMCs serving CT’s communities (Danbury, Hartford, New Haven, Norwalk, Norwich, and Stamford). In this study we focus on the Community Health Care Van (CHCV), the longest operating MMC in the state, serving the New Haven community.
Community Health Care Van Program Description
The CHCV, which began in 1993, address the healthcare needs of New Haven’s impoverished neighborhoods and has spent the last two decades providing medical and substance use prevention and treatment services at the doorstep of these vulnerable and medically marginalized communities. It offers care in four distinct neighborhoods and may change exact locations within these neighborhoods due to logistical or convenience needs (Figure 2). CHCV clients enrolled in research studies can also receive supplemental counseling support provided at one nearby fixed location, primarily those with SUDs receiving buprenorphine or methadone. Biweekly outreach at a day program for homeless individuals is also provided. Services are free and include community outreach, acute and episodic primary care, health education, harm reduction services (condom and syringe distribution), and screening for a variety of conditions, such as hypertension, diabetes, tuberculosis, HIV, viral hepatitis, and STIs (Morano et al. 2013a). The CHCV also pioneered DAART among PWIDs (Altice et al. 2003, Copenhaver et al. 2007, Altice et al. 2004, Ing et al. 2011, Maru et al. 2008, Smith-Rohrberg et al. 2006) and was the first MMC to provide buprenorphine (Schwarz et al. 2012, Schwarz et al. 2009) and directly observed therapy (DOT) for latent tuberculosis (Morano et al. 2013b). In addition, MAT for opioid dependence is coupled with counseling and treatment (Copenhaver et al. 2007). Dedicated staff members are bilingual, culturally sensitive, and provide non-judgmental care that overcomes barriers of language, finances, non-insurance status, and stigma. Clients are seen without appointments, allowing them to obtain care on their own schedule. It should be noted that the CHCV is not meant to be a stand-alone source of continuous healthcare but rather serves to stabilize clients with more chaotic lives and ultimately link them to other clinical and social services. While the CHCV is better suited for acute and episodic preventative care, it often serves as a primary source of healthcare for clients who are reluctant to access services elsewhere or who are otherwise ineligible to do so.
Figure 2.
Data Collection
An electronic health record database maintains all relevant clinical information. All CHCV clients undergo a structured intake interview at their first visit, which assesses in-depth information including their residence address, demographics, sexual behaviors, substance use, medical history, and clinical information. Client files are updated with this information for any visits encountered after one month of an in-depth intake. Visits within one month of an in-depth intake are recorded in a briefer assessment that records only clinically relevant information. From January 2004 until December 2012, 9,716 unique clients made a total of 30,041 CHCV visits. All clients (n=8,404) who provided a street address, including that of a homeless shelter, were included in the spatial analysis; those clients reporting no street address were excluded from analysis (n=1,417).
Recognizing the high prevalence of HIV, SUDs, or psychiatric disorders in our sample (n=6,367; 64.8%), we wanted to test the hypotheses that within the broader framework of HBM adapted for vulnerable populations, the five factors of access to healthcare (accessibility, affordability, acceptability, availability, and accommodation) and/or need factors were driving clients frequently to travel large distances to the MMC despite the existence of fixed mental health and substance use treatment facilities in the local area. We therefore accessed the Substance Abuse and Mental Health Services Agency (SAMHSA) Behavioral Health Treatment Services Locator to identify and map the locations of all substance abuse and mental health treatment facilities throughout CT. Service options varied between locations but included any one of the following: substance abuse treatment, detoxification, methadone maintenance therapy, halfway houses, psychiatric services, and onsite general health services (SAMHSA 2013).
Definitions
Study variables were defined as the following. “Undocumented migrant” included any client who was a non-US citizen living in the United States with expired residence or work permit or without any documentation for legal residence. “Unstably housed” was defined as living in a hotel, boarding house, halfway house, shelter, public place, or street. “Homelessness” is included in the unstably housed population and is considered a subset that reported residing in a shelter, public place, or on the street. “Committed relationship” was defined as being married or living with a partner. MSM was defined as any male client who reported having sex with another male. WSW was defined as any female client who reported having sex with another female. Recent “incarceration” was defined as anyone who reported being incarcerated within six months prior to a CHCV visit. “Sex solicitation” was defined as those reporting paying for sex. “Sex work” was defined as providing sex in exchange for shelter, drugs, protection, or money. “Illicit drug use” was defined as ever using marijuana, cocaine, crack, heroin, “wooly/illy”, “speedball” (mixture of injected heroin and cocaine), “ecstasy” (MDMA, 3,4-methylenedioxy-methamphetamine), methamphetamine, and/or ketamine. “Wooly/Illy” refers to use of marijuana mixed with other substances, such as crack or formaldehyde. “Street methadone” or “street buprenorphine” was defined as having been obtained illicitly without a prescription. Medical conditions were coded using ICD-9 diagnostic codes from: 1) questionnaire self-reported past medical history; or 2) CHCV examination or testing results. “Mental illness” included anxiety, bipolar disorder, depression, post-traumatic stress disorder (PTSD), schizophrenia, or a general report of ever having a mental health diagnosis. “TST-related services” were defined as visits for tuberculosis screening that included the tuberculin skin test (TST) placement or TST reading. “Mental health services” included both on-site and off-site consultation for psychiatric counseling services.
Data Analysis
Data were analyzed primarily using two software packages: STATA 12 IC (College Station, TX, USA) (StataCorp 2011) for statistical analysis and ArcGIS 10.1 (Redlands, CA, USA) (ESRI 2011) for mapping and spatial analysis. Polygon shapefile of Census Tract boundary for the state of Connecticut (University of Connecticut Libraries Map and Geographic Information Center 2010) and point shapefile of SAMHSA treatment facilities (SAMHSA 2013) were used to assist with spatial analysis.
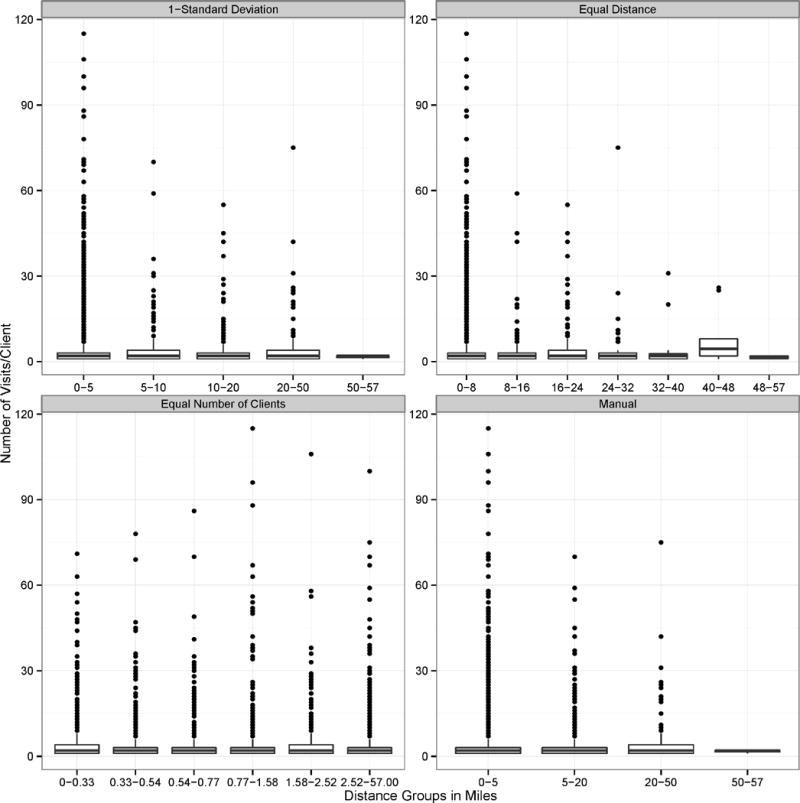
First, client self-reported addresses were geocoded (Chang 2011) to points determined by latitude and longitude in ArcGIS 10.1. Second, distances on road network were calculated from client’s location to all of the four MMC community sites, the linked main ‘storefront’ fixed facility, as well as the nearest of the four MMC sites using ArcGIS 10.1 Network Analyst functions. Scatter plots were then created and “Loess” fit, a combination of linear least squares and nonlinear regression (Cleveland 1979), was overlaid to show the relationship between distance and frequency of visits per client (Figure 3). To further understand the bivariate relationship between distance and frequency of visits, box plots were drawn (Figure 4). For a robust analysis, we conducted four distinct approaches of binning distances: 1) 1-standard deviation from the mean, 2) equal distance bands, 3) equal number of clients in distance bands, and 4) manual distance bands based upon researchers’ domain knowledge. In comparing the results of client characteristics stratified by each type of distance bins, we found that the results were similar, robust, and independent of these approaches. We therefore chose to represent our data using distance bands derived from the 1-standard deviation from the mean classification approach. Buffer zones were then placed around the MMC sites based on the selected distance bands and client data were spatially joined to each of the buffer zones and exported for statistical analysis using STATA 12 IC.
Figure 3.
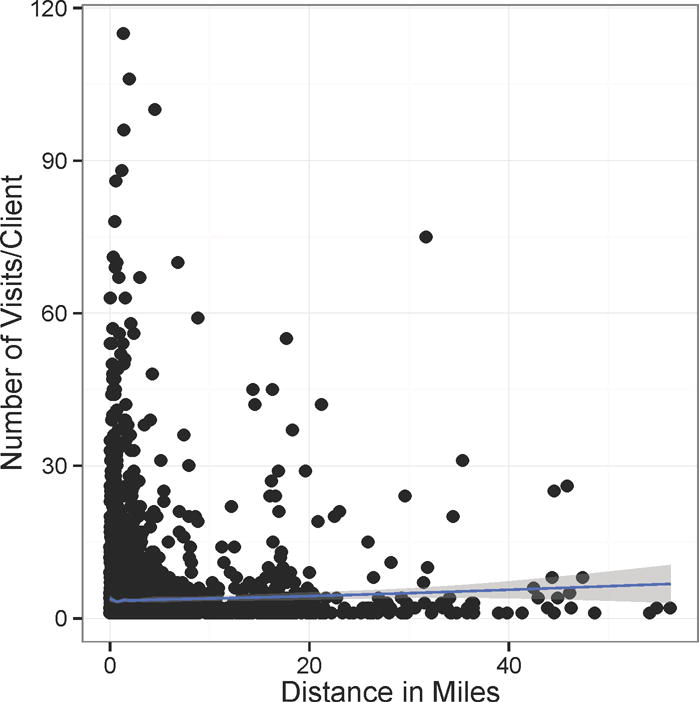
Figure 4.
Client-level data were then compared by the selected distance bands from MMC sites. Frequencies were calculated for sociodemographic, behavioral, medical history, and service utilization within each group and compared using Kruskal-Wallis test, as our data were right-skewed and non-parametric (Table 1). Client data were also compared by visitation frequency by specifically examining clients making only one visit (low-frequency) versus those clients visiting >20 times (high-frequency). Visitation frequencies were reported for sociodemographic, behavioral, medical history, and service utilization within these groups, and Kruskal-Wallis test was used for comparison between low-frequency and high-frequency users (Table 2).
Table 1.
Client characteristics of mobile medical clinic, stratified by distance from points of care, New Haven, Connecticut.
| Variable | ≤ 5 Miles n (%) |
>5 – 10 Miles n (%) |
>10 – 20 Miles n (%) |
>21 – 50 Miles n (%) |
>50 Miles n (%) |
p-value* |
|---|---|---|---|---|---|---|
| Total Sample (N=8404) | 7,579 (90.2) | 234 (2.8) | 360 (4.3) | 107 (1.3) | 124 (1.5) | |
| Mean number of CHCV Visits/Client | 3.58 ± 6.8 | 4.26 ± 7.9 | 5.28 ± 9.8 | 2.22 ± 3.6 | 2.56 ± 3.6 | 0.033 |
| Gender | ||||||
| Male | 4,204 (55.5) | 130 (55.6) | 215 (59.7) | 63 (58.9) | 77 (62.1) | 0.060 |
| Female | 3,374 (44.5) | 104 (44.4) | 145 (40.3) | 44 (41.1) | 47 (37.9) | 0.058 |
| Race/Ethnicity | ||||||
| White, non-Hispanic | 1,733 (22.9) | 141 (60.3) | 166 (46.1) | 55 (51.4) | 36 (29.0) | <0.001 |
| Black, non-Hispanic | 3,176 (41.9) | 39 (16.7) | 75 (20.8) | 26 (24.3) | 45 (36.2) | <0.001 |
| Hispanic | 2,655 (35.0) | 55 (23.5) | 117 (32.5) | 26 (24.3) | 40 (32.3) | 0.001 |
| Median Age (IQR), years | 35 (27, 46) | 35.5 (27, 46) | 34 (27, 43) | 35.5 (26, 47) | 35 (28, 45) | 0.965 |
| Foreign Born | 2,962 (39.1) | 81 (34.6) | 122 (33.9) | 40 (37.4) | 41 (33.1) | 0.009 |
| Undocumented | 891 (11.8) | 13 (5.6) | 16 (4.4) | 2 (1.9) | 11 (8.9) | <0.001 |
| Less than high school | 2,143 (28.3) | 39 (16.7) | 83 (23.1) | 28 (26.2) | 40 (32.3) | 0.003 |
| Housing Status | ||||||
| Unstably Housed | 2,538 (33.5) | 41 (17.5) | 82 (22.8) | 36 (33.6) | 63 (50.8) | 0.001 |
| Homeless | 701 (0.09) | 11 (4.7) | 28 (7.8) | 3 (2.8) | 50 (40.3) | 0.027 |
| Relationship Status | ||||||
| Committed | 1,519 (20.0) | 54 (23.1) | 55 (15.3) | 12 (11.2) | 19 (15.3) | 0.232 |
| Non-Committed | 6,034 (79.6) | 180 (76.9) | 304 (84.4) | 95 (88.8) | 105 (84.7) | 0.232 |
| Unemployed | 5,150 (68.0) | 154 I65.8) | 249 (69.2) | 81 (75.7) | 94 (75.8) | 0.174 |
| Lack of Health Insurance | 4,191 (55.3) | 125 (53.4) | 160 (44.4) | 50 (46.7) | 66 (53.2) | <0.001 |
| MSM | 177 (2.3) | 14 (6.0) | 15 (4.2) | 6 (5.6) | 1 (0.8) | 0.001 |
| WSW | 213 (2,8) | 7 (3.0) | 9 (2.5) | 4 (3.7) | 1 (0.8) | 0.631 |
| Injection Drug Use | 1,888 (24.9) | 70 (29.9) | 144 (40.0) | 38 (35.5) | 28 (22.6) | <0.001 |
| Incarceration History | 1,549 (20.4) | 28 (12.0) | 73 (20.3) | 25 (23.4) | 21 (16.9) | 0.095 |
| Sex Solicitation | 748 (9.9) | 16 (6.8) | 25 (6.9) | 8 (7.5) | 10 (8.1) | 0.013 |
| Sex Work | 591 (7.8) | 14 (6.0) | 33 (9.2) | 10 (9.3) | 7 (5.6) | 0.949 |
| Drug Use | ||||||
| Any illicit drug use | 4,963 (65.5) | 163 (70.0) | 283 (78.6) | 89 (83.2) | 73 (58.9) | <0.001 |
| Marijuana | 4,626 (61.0) | 150 (64.1) | 259 (71.9) | 81 (75.7) | 69 (55.6) | <0.001 |
| Cocaine | 2,215 (29.2) | 94 (40.2) | 149 (41.4.) | 50 (46.7) | 37 (29.8) | <0.001 |
| Crack | 2,107 (27.8) | 80 (34.2) | 142 (39.4) | 44 (41.1) | 36 (29.0) | <0.001 |
| Heroin | 1,646 (21.7) | 68 (29.1) | 146 (40.6) | 42 (39.3) | 28 (22.6) | <0.001 |
| Wooly/Illy | 996 (13.1) | 30 (12.8) | 54 (15.0) | 17 (15.9) | 10 (8.1) | 0.836 |
| Speedball | 858 (11.3) | 33 (14.1) | 70 (19.4) | 17 (15.9) | 12 (9.7) | <0.001 |
| MDMA (“Ecstasy”) | 770 (10.2) | 39 (16.7) | 63 (17.5) | 24 (22.4) | 9 (7.3) | <0.001 |
| Methamphetamine | 268 (3.5) | 8 (3.4) | 19 (5.3) | 3 (2.8) | 1 (0.8) | 0.801 |
| Ketamine | 220 (2.9) | 14 (6.0) | 24 (6.7) | 5 (4.7) | 1 (0.8) | <0.001 |
| Medication-Assisted Therapy | 587 (7.7) | 41 (17.5) | 67 (18.6) | 22 (20.6) | 12 (9.7) | <0.001 |
| Methadone Program | 406 (5.4) | 28 (12.0) | 39 (10.8) | 10 (9.3) | 10 (8.1) | <0.001 |
| Buprenorphine Program | 111 (1.5) | 9 (3.8) | 15 (4.2) | 5 (4.7) | 1 (0.8) | <0.001 |
| Street Methadone | 103 (1.4) | 6 (2.6) | 8 (2.2) | 2 (1.9) | 1 (0.8) | 0.124 |
| Street Buprenorphine | 64 (0.8) | 6 (2.6) | 8 (2.2) | 0 (0.0) | 0 (0.0) | 0.024 |
| Domestic Violence Victim | 1,120 (14.8) | 29 (12.4) | 56 (15.6) | 18 (16.8) | 16 (12.9) | 0.703 |
| Sexual Assault Victim | 732 (9.7) | 26 (11.1) | 48 (13.3) | 17 (15.9) | 10 (8.1) | 0.025 |
| Reported Medical Conditions | ||||||
| STI | 1,936 (25.5) | 47 (20.1) | 78 (21.7) | 23 (21.5) | 27 (21.8) | 0.007 |
| Mental Illness | 1,828 (24.1) | 74 (31.6) | 114 (31.7) | 40 (37.3) | 29 (23.4) | <0.001 |
| Hypertension | 1,482 (19.6) | 38 (16.2) | 49 (13.6) | 21 (19.6) | 17 (13.7) | 0.002 |
| Hepatitis C | 717 (9.5) | 26 (11.1) | 55 (15.3) | 8 (7.5) | 10 (8.1) | 0.023 |
| Diabetes | 651 (8.6) | 21 (9.0) | 28 (7.8) | 2 (1.9) | 12 (9.7) | 0.327 |
| HIV | 621 (8.2) | 22 (9.4) | 35 (9.7) | 19 (17.8) | 8 (6.5) | 0.048 |
| Hepatitis B | 160 (2.1) | 4 (1.7) | 10 (2.8) | 1 (0.9) | 3 (2.4) | 0.857 |
| CHCV Services Received | ||||||
| TST-Related Service | 2,961 (39.1) | 83 (35.5) | 126 (35.0) | 44 (41.1) | 50 (16.1) | 0.214 |
| STI Screen | 1,415 (18.7) | 35 (15.0) | 56 (15.6) | 19 (17.8) | 12 (9.7) | 0.006 |
| HIV Testing | 1,357 (17.9) | 34 (14.5) | 69 (19.2) | 20 (18.7) | 14 (11.3) | 0.351 |
| Urinalysis | 469 (6.2) | 9 (3.8) | 10 (2.8) | 6 (5.6) | 2 (1.6) | 0.007 |
| Hepatitis B Screening | 428 (5.6) | 10 (4.3) | 25 (6.9) | 8 (7.5) | 3 (2.4) | 0.914 |
| Mental Health Service | 223 (2.9) | 18 (7.7) | 23 (6.4) | 12 (11.1) | 3 (2.5) | <0.001 |
| Buprenorphine Maintenance Therapy | 140 (1.8) | 14 (6.0) | 18 (5.0) | 7 (6.5) | 0 (0.0) | <0.001 |
| Drug Treatment Advocacy | 97 (1.3) | 11 (4.7) | 9 (2.5) | 4 (3.7) | 1 (0.8) | <0.001 |
Legend: MSM= men who have sex with men; WSW= women who have sex with women; STI = sexually transmitted infections, including chlamydia, gonorrhea, syphilis, herpes simplex virus (HSV), Trichamonas vaginalis, and human papilloma virus (HPV). TST = tuberculin skin testing to screen for latent or active tuberculosis infection.
Table 2.
Client Characteristics of Mobile Medical Clinic, stratified by healthcare utilization frequency, New Haven, Connecticut
| Variables | 1 Visit n (%) |
2–10 Visits n (%) |
11–20 Visits n (%) |
>20 Visits n (%) |
Comparison of 1 Visit and >20 Visits* p-value |
|---|---|---|---|---|---|
| Total Sample (n=8404) | 3426 (40.8) | 4541 (54.0) | 256 (3.0) | 180 (2.2) | |
| Sex | |||||
| Male | 1849 (54.0) | 2570 (56.6) | 150 (58.6) | 120 (66.7) | 0.001 |
| Female | 1577 (46.0) | 1971 (43.4) | 106 (41.4) | 60 (33.3) | 0.001 |
| Race/Ethnicity | |||||
| White | 835 (24.4) | 1154 (25.4) | 75 (29.3) | 67 (37.2) | <0.001 |
| Black | 1345 (39.3) | 1865 (41.1) | 101 (39.5) | 50 (27.8) | 0.002 |
| Hispanic | 1210 (25.3) | 1533 (33.8) | 85 (33.2) | 65 (36.1) | 0.820 |
| Median Age (IQR) | 33 (25, 44) | 36 (27, 46) | 44 (35,51) | 46 (36,53) | <0.001 |
| Foreign Born | 973 (28.4) | 1887 (41.6) | 216 (84.4) | 170 (94.4) | <0.001 |
| Undocumented | 370 (10.8) | 505 (11.1) | 40 (15.6) | 18 (10.0) | 0.739 |
| Less than high school Education | 908 (26.5) | 1309 (28.8) | 58 (22.7) | 58 (32.2) | 0.256 |
| Unstably Housed | 864 (25.2) | 1698 (37.4) | 107 (41.8) | 91 (50.6) | <0.001 |
| Homeless | 208 (6.1) | 497 (10.9) | 40 (15.6) | 48 (26.7) | <0.001 |
| Relationship Status | |||||
| Committed | 657 (19.2) | 894 (19.7) | 65 (25.4) | 43 (23.9) | 0.108 |
| Non-Committed | 2754 (80.4) | 3638 (80.1) | 191 (74.6) | 135 (75.0) | 0.108 |
| Unemployed | 2114 (61.7) | 3260 (71.8) | 201 (78.5) | 153 (85.0) | <0.001 |
| Lack of Health Insurance | 1948 (56.9) | 2422 (53.3) | 141 (55.1) | 81 (45.0) | 0.002 |
| MSM | 81 (2.4) | 114 (2.5) | 9 (3.5) | 9 (5.0) | 0.027 |
| WSW | 69 (2.0) | 149 (3.3) | 9 (3.5) | 7 (3.9) | 0.088 |
| Injection Drug Use | 809 (23.6) | 1143 (25.2) | 101 (39.5) | 115 (63.9) | <0.001 |
| Incarceration History | 547 (16.0) | 1014 (22.3) | 69 (27.0) | 66 (36.7) | <0.001 |
| Sex Solicitation | 230 (6.7) | 487 (10.7) | 47 (18.4) | 43 (23.9) | <0.001 |
| Sex Work | 175 (5.1) | 404 (8.9) | 37 (14.5) | 39 (21.7) | <0.001 |
| Drug Use | |||||
| Any illicit drug use | 2024 (59.1) | 3197 (70.4) | 193 (75.4) | 157 (87.2) | <0.001 |
| Marijuana | 1883 (55.0) | 2976 (65.5) | 182 (71.1) | 144 (80.0) | <0.001 |
| Cocaine | 683 (19.9) | 1619 (35.7) | 125 (48.8) | 118 (65.6) | <0.001 |
| Crack | 677 (19.8) | 1494 (32.9) | 123 (48.0) | 115 (63.9) | <0.001 |
| Heroin | 569 (16.9) | 1135 (25.0) | 101 (39.5) | 125 (69.4) | <0.001 |
| Wooly/Illy | 304 (8.9) | 716 (15.8) | 47 (18.4) | 40 (22.2) | <0.001 |
| Speedball | 241 (7.0) | 600 (13.2) | 68 (26.6) | 81 (45.0) | <0.001 |
| MDMA (“Ecstasy”) | 271 (7.9) | 576 (12.7) | 29 (11.3) | 29 (16.1) | <0.001 |
| Methamphetamine | 76 (2.2) | 185 (4.1) | 19 (7.4) | 19 (10.6) | <0.001 |
| Ketamine | 69 (2.0) | 172 (3.8) | 9 (3.5) | 14 (7.8) | <0.001 |
| Medication-Assisted Therapy | 159 (4.6) | 405 (8.9) | 68 (26.6) | 97 (53.9) | <0.001 |
| Methadone | 130 (3.8) | 291 (6.4) | 31 (12.1) | 41 (22.8) | <0.001 |
| Buprenorphine | 25 (0.7) | 58 (1.3) | 19 (7.4) | 39 (21.7) | <0.001 |
| Street Methadone | 23 (0.7) | 75 (1.7) | 12 (4.7) | 10 (5.6) | <0.001 |
| Street Buprenorphine | 16 (0.5) | 47 (1.0) | 3 (1.2) | 12 (6.7) | <0.001 |
| Domestic Violence Victim | 376 (11.0) | 756 (16.6) | 56 (21.9) | 51 (28.3) | <0.001 |
| Sexual Assault Victim | 260 (7.6) | 492 (10.8) | 38 (14.8) | 43 (23.9) | <0.001 |
| Reported Medical Conditions | |||||
| STI | 702 (20.5) | 1241 (27.3) | 93 (36.3) | 75 (41.7) | <0.001 |
| Mental Illness | 669 (19.5) | 1183 (26.1) | 109 (42.6) | 124 (68.9) | <0.001 |
| Hypertension | 547 (16.0) | 910 (20.0) | 86 (33.6) | 64 (35.6) | <0.001 |
| HCV infection | 198 (5.8) | 477 (10.5) | 65 (25.4) | 76 (42.2) | <0.001 |
| Diabetes | 242 (7.1) | 398 (8.8) | 43 (16.8) | 31 (17.2) | <0.001 |
| HIV infection | 119 (3.5) | 357 (7.9) | 94 (36.7) | 135 (75.0) | <0.001 |
| HBV infection | 46 (1.3) | 97 (2.1) | 20 (7.8) | 15 (8.3) | <0.001 |
| CHCV Services Received | |||||
| TST-Related Service | 410 (12.0) | 2584 (56.9) | 165 (64.5) | 105 (58.3) | <0.001 |
| STI Screening | 474 (13.8) | 954 (21.0) | 67 (26.2) | 42 (23.3) | <0.001 |
| HIV Testing | 487 (14.2) | 881 (19.4) | 79 (30.9) | 47 (26.1) | <0.001 |
| Urinalysis | 144 (4.2) | 291 (6.4) | 42 (16.4) | 19 (10.6) | <0.001 |
| Pregnancy Test | 221 (6.5) | 246 (5.4) | 16 (6.3) | 15 (8.3) | 0.319 |
| Hepatitis B Screening | 91 (2.7) | 320 (7.0) | 36 (14.1) | 27 (15.0) | <0.001 |
| Mental Health Service | 7 (0.2) | 104 (2.3) | 57 (22.3) | 111 (61.7) | <0.001 |
| Buprenorphine Treatment | 7 (0.2) | 82 (1.8) | 29 (11.3) | 61 (33.9) | <0.001 |
| Drug Treatment Advocacy | 11 (0.3) | 71 (1.6) | 17 (6.6) | 23 (12.8) | <0.001 |
Legend: MSM= men who have sex with men; WSW= women who have sex with women; STI = sexually transmitted infections, including chlamydia, gonorrhea, syphilis, herpes simplex virus (HSV), Trichamonas vaginalis, and human papilloma virus (HPV). TST indicates tuberculin skin testing to screen for latent or active tuberculosis infection.
To preserve confidentiality of personal health information and individual anonymity, we aggregated the data at the US census tract, block-group, and block levels. Next, we aggregated client data to these geographies of scale to further explore the relationship between distance and average frequency of visit in scatter plots overlaid with Loess fit (Figure 5), which showed that there is little to no significant difference by different geographies of scale. Thus, we chose to represent our data by census tracts, as it generated a distribution of fewer zeroes, i.e. tracts with no CHCV clients. The spatial distributions of client’s place of reported residence and visitation frequency are represented using choropleth maps (Figures 6 and 7).
Figure 5.
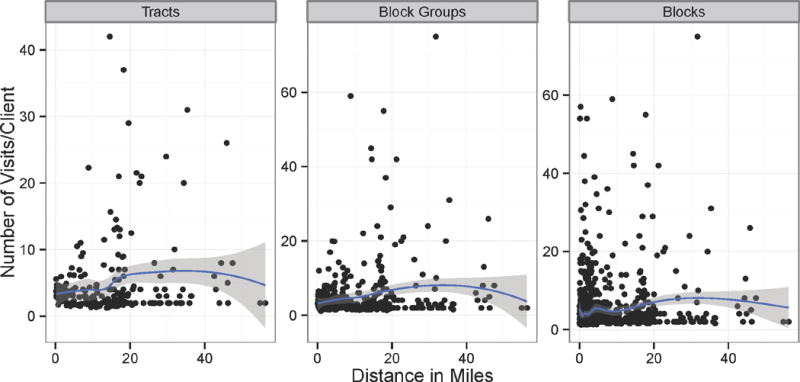
Figure 6.
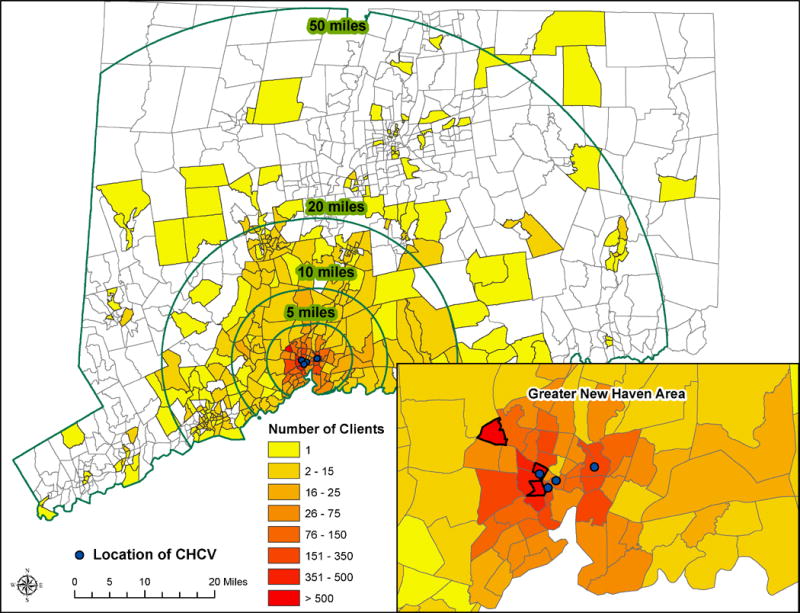
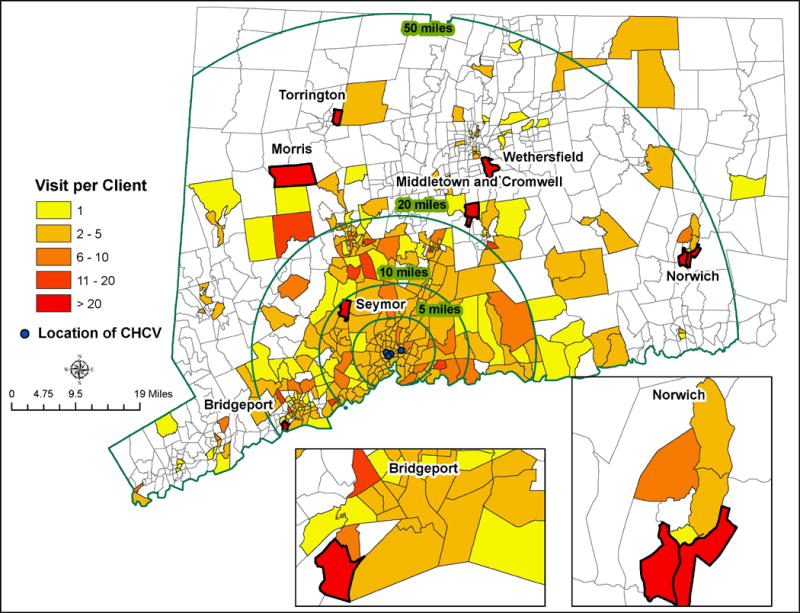
Figure 7.
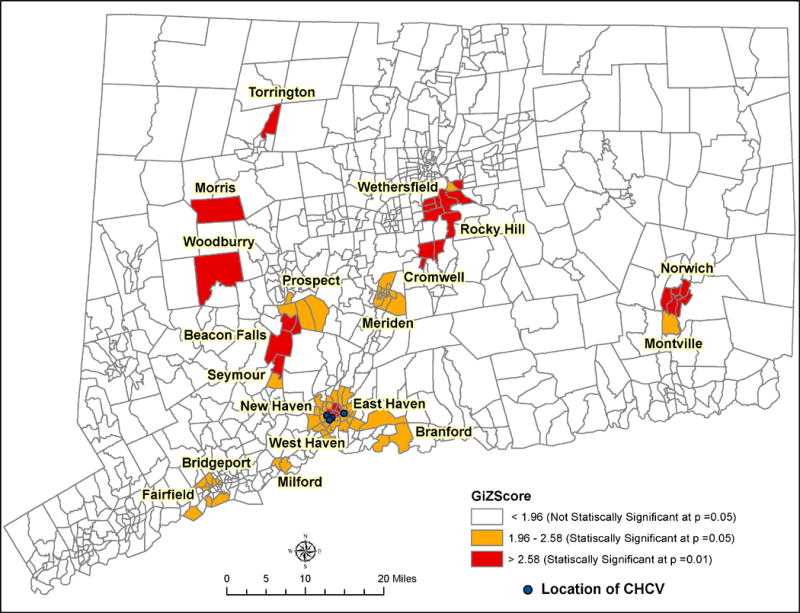
Spatial cluster analysis was conducted to identify census tracts with a higher (or lower) than expected proportion of frequency of visits per client using the Hot-Spot function in ArcGIS 10.1 (Getis and Ord 1992, Ord and Getis 1995). The Hot-Spot function, based upon the Getis-Ord Gi* statistic, identifies clusters of census tracts with statistically significant high (“hot-spot”) or low (“cold-spot”) values of average frequency of visit per client (Getis and Ord 1992, Ord and Getis 1995). To be a statistically significant hot spot, a census tract will have a high value (i.e., high visit frequency) and would be surrounded by other tracts with high values such that the local sum for that particular tract and its neighbors should be very different than the expected sum resulting in a high Z-score. Similarly, this tool also delineates clusters of lower than expected values, or “cold spots”, of census tracts with significantly low frequency of client visits (Getis and Ord 1992, Ord and Getis 1995). In our study we did not identify any cold spots. The results of the hot spot analysis are summarized in Figure 8.
Figure 8.
Statistically significant clusters of census tracts from the hot-spot analysis were analyzed in respect to nearby SAMHSA substance abuse treatment facilities. The SAMHSA facilities that were located within the buffer of 3, 5, and 10 miles from the population centroid of these census tracts (Table 3) were summarized using the Penchansky and Thomas’s robust definition of access, incorporating the five dimensions (Penchansky and Thomas 1981).
Table 3.
Comparison of 5 Dimensions of Access between Drug Treatment Facilities and the Mobile Medical Clinic
| Dimensions of Accessibility | SAMHSA Facilities | Mobile Medical Clinic | ||
|---|---|---|---|---|
|
| ||||
| 3 Miles | 5 Miles | 10 Miles | 20 to 50 Miles | |
| Accessibility | Accessibility | |||
|
| ||||
| Number of SAMHSA facilities | 56 (100) | 80 (100) | 112 (100) | Locations of Community Health Care Van |
|
| ||||
| Affordability | Affordability | |||
|
| ||||
| Requires Health Insurance | 56 (100) | 80 (100) | 112 (100) | Does not require health insurance |
|
| ||||
| Availability | Availability (also has Outpatient services) | |||
|
| ||||
| Substance Abuse | 56 (100) | 80 (100) | 112 (100) | Drug Treatment Advocacy |
| Detoxification | 13 (23.2) | 18 (22.5) | 26 (23.2) | Buprenorphine Induction |
| Methadone Maintenance | 16 (28.6) | 19 (23.8) | 23 (20.5) | Mental Health Service |
| Buprenorphine Maintenance | 13 (23.2) | 19 (23.8) | 26 (23.2) | HIV Testing |
| Mental Health and Substance Abuse | 23 (41.1) | 30 (37.5) | 40 (35.7) | Directly Administered Antiretroviral Therapy |
| Outpatient Services | 46 (82.1) | 58 (72.5) | 81 (72.3) | Urinalysis |
| STI Screening | ||||
| Hepatitis A, B, C Screening | ||||
| Hepatitis B Vaccine | ||||
| Diabetes Screening | ||||
| TST Related Service Tuberculosis Screening (TST-Related) | ||||
| Pregnancy Tests | ||||
|
| ||||
| Acceptability | Acceptability | |||
|
| ||||
| Criminal Justice | 12 (21.4) | 16 (20.0) | 16 (14.3) | History of Incarceration |
| HIV/AIDS | 15 (26.8) | 17 (21.3) | 23 (20.5) | HIV infected |
| Pregnant Women | 13 (23.2) | 15 (18.8) | 23 (20.5) | Sex Workers |
| Women | 27 (48.2) | 39 (48.8) | 54 (48.2) | Domestic Violence Victim |
| Adolescents | 8 (14.3) | 10 (12.5) | 14 (12.5) | Sexual Assault Victim |
| Senior Citizens | 8 (14.3) | 12 (15.0) | 16 (14.3) | Mental Illness |
| LGBT | 5 (8.9) | 5 (6.3) | 7 (6.25) | Drug Users |
| MSM/WSW | ||||
|
| ||||
| Accommodation | Accommodation | |||
|
| ||||
| Disability | 42 (75.0) | 53 (66.3) | 77 (68.8) | Bilingual Staff Members, |
| Foreign Language | 44 (78.6) | 53 (66.3) | 70 (62.5) | Culturally sensitive staff members |
| Offers walk-in services | ||||
Legend: SAMHSA=Substance Abuse and Mental Health Services Agency; STI=sexually transmitted infection; HIV=human immunodeficiency virus; TST = tuberculin skin testing; LGBT = lesbian, gay, bisexual, transgendered community; MSM = men who have sex with men; WSW = women who have sex with women
RESULTS
Table 1 describes the client characteristics and stratifies them by 1-standard deviation from the mean distance groups. The client visitation rates were significantly different and most frequent visitation occurred between 11–20 miles (5.28 visits per client). Significant client level characteristics between distance-based subgroups were race, foreign-born, undocumented immigration status, less than high school education, unstable housing, lack of health insurance, sex solicitation, drug use, receipt of MAT, and self-reported mental illness. Two-group comparisons identified higher rates of unstable housing (p<0.001) and homelessness (p<0.001) in those >50 miles from a MMC site compared to those <5 miles away. Clients traveling between 21–50 miles had significantly higher rates of unstable housing (p=0.001) than those traveling 5–20 miles. In terms of health status differences, HIV prevalence was highest among those living in the 21–50 mile band at 17.8%, and significant differences between distances bands existed for reported history of STIs, mental illness, hypertension, hepatitis C, and HIV infection. Figure 6 further describes the spatial variation of client origin based upon self-reported residential location and distance from the MMC sites aggregated by census tracts. Most clients (300 to 500 per census tract) lived within the Greater New Haven area including nearby cities of New Haven, Hamden, Woodbridge, Orange, West Haven, East Haven and North Haven. These cities are all within 8 to 10 miles from MMC locations. In addition, a high proportion of clients (>500 per census tracts), who are typically low-frequency users, lived in a concentrated area of less than 5 miles from MMC sites. Therefore as expected and consistent with the concept of distance decay, the number of clients visiting the MMC decreases with increasing distance from the CHCV locations with <20 clients per census tracts living between 21 to 50 miles, with the fewest clients living 50 miles from a MMC site.
Table 2 stratifies clients based on their frequency of CHCV utilization, including those that used services once (low-frequency users), 2–10 times, 11–20 times, and >20 times (high-frequency users). Between the four groups, statistically significant differences were found for sex, race/ethnicity, age, foreign-born status, housing, employment, health insurance, drug use, incarceration, transactional sex, medication-assisted therapy, violence victim, reported medical conditions and services utilized. Comparison of low-frequency to high frequency users (>20 visits) shows that, in addition to having higher rates of health insurance (p=0.002), the high-frequency users had significantly higher rates of being foreign-born (p<0.001), unstably housed (p<0.001), homeless (p<0.001), unemployed (p<0.001), drug users (p<0.001), recently incarcerated (p<0.001), commercial sex workers (p<0.001), domestically (p<0.001) and sexually victimized (p<0.001), medication-assisted therapy clients (p<0.001), and also had significantly higher rates of all reported health conditions (p<0.001), including 75% with HIV infection (p<0.001). These results indicate that for our study population with vulnerable health conditions, their utilization is likely “less-discretionary” and thus influenced primarily by the need factors of the adapted HBM.
In Figure 7, the pattern of client visit per census tract shows several census tract clusters with clients visiting >20 times who resided between 21 to 50 miles from the van locations. Conversely, tracts within <5 miles from the CHCV have relatively lower frequency of client visits. The census tract clusters with higher visit frequency are in the towns of Bridgeport, Norwich, Morris, Torrington, Wethersfield, and Cromwell. Seymour is the only town within 10–15 miles from a MMC site with a frequency of more than 20 visits per clients. Since this finding is unique and contrary to most of the studies on access to healthcare services, we decided to further explore this spatial pattern using a hot-spot analysis in a Geographic Information Science (GIS) environment.
The hot-spot analysis divided all of the census tracts into 3 groups (Figure 8): 1) census tracts that have significantly high frequency of client visits with respect to the surrounding local area at p<0.05 (labeled Hot-Spot 1); 2) census tracts that have an even higher significant frequency of client visits with respect to the surrounding local area at p<0.01 (labeled Hot-Spot 2); and 3) census tracts with frequency of client visit but not statistically significant. Of the 19 census tracts in Hot-Spot 2, 90% of the tracts are located >20 miles from the MMC. There is only one cluster with high frequency of client visits significant at p<0.01 located in Greater New Haven, i.e. very close to the CHCV sites. Most of the census tracts in Hot-Spot 1 are also not located near the MMC but rather are as far as 40 miles away (e.g., Norwich and Montville). Thus, the hot-spot analysis statistically confirms our finding that although a large number of clients living <5 miles are utilizing MMC services for up to 10 visits, a small but significant proportion of clients traveling longer distances (between 21 to 50 miles) have higher frequency of visits. There are 56 SAMHSA facilities within a buffer of 3 miles from all the 76 census tracts combined (Hot-Spots 1 and 2), 80 facilities within a buffer of <5 miles, and 112 treatment facilities within a buffer <10 miles (Figure 9). Despite state and federally-funded SAMSHA treatment facilities providing substance abuse treatment resources in their local areas, clients traveled between 20–50 miles and visited the CHCV frequently (>20 visits) for substance abuse treatment, HIV testing and treatment, HBV vaccination and other health-related services. This clearly emphasizes the importance of ‘need’ factors over predisposing and geography-related enabling resources in explaining the higher frequency of visits from the clients located over 20 miles from the MMC sites.
Figure 9.
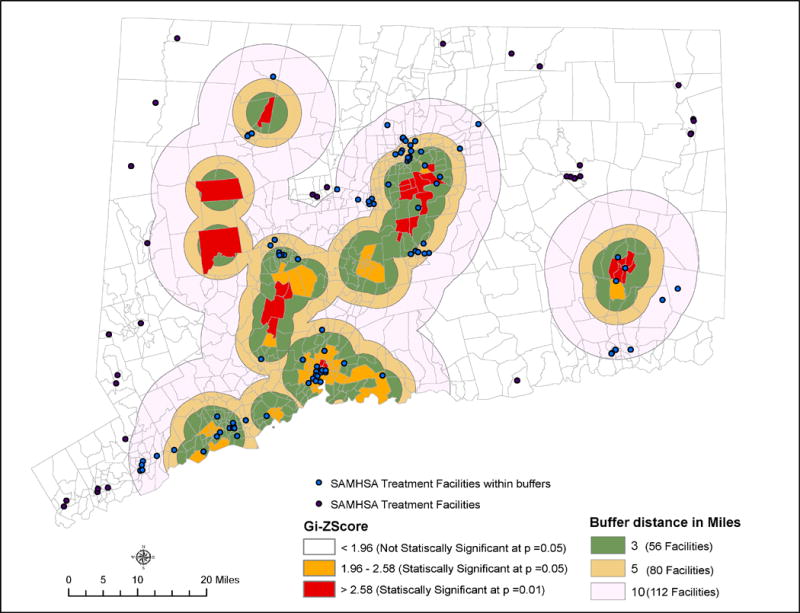
Table 3 first defines Penchansky and Thomas’ five dimensions of access with respect to our study (column 1), summarizes the SAMHSA facilities in the 3-, 5-, and 10-mile buffer zones from the census tracts with client visiting >20 times on the basis of the five dimensions (columns 2–4), and then lists the services provided at the MMC for comparison (column 5). SAMHSA facility locations and buffer zones are shown in Figure 9. For all census tracts where the clients are not only traveling long distances but also very frequently, 56 SAMHSA treatment centers are accessible within 3 miles of their population centroids. All of these 56 facilities require that the clients have health insurance, 41% provide treatment for comorbid conditions (i.e., mental health and substance abuse), and fewer than 25% provide MAT. Although 48% of these facilities have specialized services for female clients, only about one-quarter or less provide specialty services for other high-risk and medically vulnerable populations, such as people living with HIV/AIDS (27%), pregnant women (23%), clients who were recently incarcerated (21%), adolescents and senior citizens (14%), and lesbian and gay clients (9%). Almost 75% of facilities accommodate support for disabled clients and non-English speaking clients; however, we do not have detailed information on other accommodating factors, such as hours of operation and walk-in-services at these facilities. SAMHSA treatment facilities within the 5-mile (80 centers) and 10-mile (112 centers) buffers from census tracts with distance traveling, high-frequency MMC clients have similar characteristics with little variation. In comparison, the MMC (CHCV located only in New Haven) is more conducive to access, despite being 21–50 miles from the population centroids of census tracts with high frequency of client visits.
DISCUSSION
Among the predisposing, enabling resource, and need factors explaining the variation in MMC utilization according to the adapted HBM, the enabling factors related to geographic proximity did not have any significant influence. This result of minimal to non-existent relationship between distance and frequency of visits per client was consistent both at the client-level and at the aggregated census tract scale.
In comparing predisposing and non-geographic enabling resources of CHCV clients, however, we find several statistically significant differences. Based on the location of self-reported residence, clients living <5 miles and >50 miles of a MMC have significantly higher rates of racial/ethnic minorities and undocumented migrants while those between five and fifty miles are predominately Caucasian and born domestically. This is likely due to the higher distribution of racial/ethnic minorities in inner cities (e.g., New Haven) compared to surrounding suburban and ex-urban areas, which have higher Caucasian populations.
A similar distribution is also seen among those with unstable housing and health insurance, with those residing within five miles and greater than fifty miles tending to be less stably housed and lack health insurance, and notably those traveling greater than fifty miles are significantly more likely to be homeless (40.3%, p=0.03) than those within a fifty-mile radius. These are important enabling resources that could influence a client’s decision to seek services at the MMC.
People who use and/or inject drugs are significantly more likely to reside between 5 to 10, 11 to 20, and 21 to 50 miles from a MMC site and clients from these proximity bands are significantly more likely to report mental illness and use of medication-assisted therapy to treat opioid dependence. This suggests willingness, perceived need, or possibly severity of illness (specifically SUDs severity) to travel to settings where they receive care and specific medications in an affordable and acceptable way. With this in mind, we observed that two distinct populations who are traveling to receive care at the MMC: The first group are those traveling between five and fifty miles and tend to be substance users who, despite having health insurance, prefer to travel to receive care at the MMC where services are easily accessible and accommodate their needs. These individuals appear to have transportation and may choose to travel either because the services they use are not available to them in their own community, they do not perceive the available services near them to be user friendly or they do not want to be recognized and treated near their homes. The second group is racial/ethnic minorities who reside greater than fifty miles away that travel due to lack of other options, as they are often undocumented immigrants or lack health insurance. The MMC, which is free, is the only setting that they can access services they need.
When stratifying by visit frequency, we see that ‘high frequency’ users are significantly more likely to be men (66.7%, p=<0.01) and are nearly all are foreign-born (94.4%, p<0.01). About 15% of these individuals are traveling more than 5 miles to receive care at the MMC. Just over half are unstably housed, 85% are unemployed, and are significantly more likely to report a history of drug use, injecting drugs, recent incarceration, sex solicitation, sex work, domestic violence, and sexual assault. Therefore, high-frequency users show typical indicators of extremely vulnerable populations. Furthermore, over half receive substance abuse treatment in the form of medication-assisted therapy (either MMT or BMT) and 75% of them are HIV-infected. This constellation of findings are wholly consistent with the “SAVA” (Substance Abuse, Violence, and AIDS) Syndemic (Meyer et al. 2011, Singer 1996) and its impact on access to health services, as we observe that despite the majority of these individuals having health insurance, they seek continued, frequent care at a MMC operating a substantial distance from their residence. This suggests that the MMC provided an array of services specific to the need of our client population (predominantly with SUDs, HIV, and mental illness) that may not be offered in the fixed healthcare venues, such as primary care settings or SAMHSA treatment facilities or that the clients are using both the facilities in tandem. More importantly, this may also indicate that the clients preferred to seek healthcare services from the MMC that was seen as user-friendly and provided services at their own convenience.
This MMC provides opportunities for clients on other dimensions of access to healthcare, which offsets the long distances to the van locations (Table 3). For example, the majority of clients are unstably housed, unemployed, and lack health insurance so offering free services may be important for access. Second, the MMC provides a wide range of services, such as HIV testing and treatment, assistance with HIV treatment adherence (i.e., DAART), treatment for SUDs, and screening and treatment for tuberculosis, hepatitis, hypertension, and diabetes. Third, the clients utilizing the MMC are challenging to reach in other venues and represent a vulnerable population, who might otherwise want to seek care from distant clinics to avoid stigma and discrimination, and maintain confidentiality from local community members. This is particularly relevant for community healthcare centers that provide local and affordable care, but employ members of the same communities, resulting in patient concerns about confidentiality for socially stigmatizing conditions (Wright et al. 2013).
Though CHCV clients are highly vulnerable (e.g. have unstable housing, use drugs, experience violence, and often have overlapping medical comorbidities, such as mental health, SUDs and HIV), MMC staff members have a longstanding presence in the New Haven community, have documented their dedication over many years, and are bi-lingual, culturally sensitive, and provide non-judgmental care. They also offer walk-in services that allow the client to obtain care when they want. This suggests that even when the physical accessibility to a MMC is not convenient, the opportunities provided in terms of availability, affordability, acceptability, and accommodation in comparison to the nearby SAMHSA facilities, are nonetheless attracting clients to the MMC. The lack of support and resources at nearby traditional healthcare setting and the ease of seeking treatment at the MMC also led to higher retention in care for a significant minority of clients.
This analysis has identified characteristics and health-seeking behaviors for a proportion of clients frequently traveling sizeable distances to receive healthcare at a non-traditional healthcare venue. Our findings suggest that factors beyond the enabling (geographic proximity or a lack of health insurance) influence clients to travel and seek continuous care at a MMC designed for acute and episodic care and linkage to other services. From these results, we hypothesize that multidimensional factors of accessibility and the less discretionary needs of the medically vulnerable clients make the CHCV (a MMC) an attractive healthcare option for individuals, as it provides free care, harm reduction services, and requires no appointment. This allows clients with chaotic lifestyles to receive care when they are ready to seek it and provides an environment that addresses the social and medical needs of vulnerable clients, many of who suffer from the ‘SAVA’ syndemic. With the implementation of the ACA, it is important to develop healthcare delivery models that consider factors outside of health insurance to promote access to healthcare and to treat medically marginalized populations. This study demonstrates how an MMC can be more than a geographically convenient venue, but also can offer services that are acceptable and accommodating to vulnerable populations.
LIMITATIONS
While we are able to present a thorough description of the geographic distribution, socio-demographics, reported health conditions, and health services sought by MMC clients, our data is from a clinical database that is comprised of a series of cross-sectional interviews that only assesses when client choose to utilize care. Thus, our study is limited in its ability to describe other sources of healthcare utilization before, simultaneous with, or after MMC visitation. It also does not describe linkages to care for clients that are effectively linked by MMC staff – one of the missions of the program. We are also unable to track and report client mobility, as our database only includes the addresses that were recorded at the time of the client visit. Homeless clients that remain on the street or in public places were not able to be accurately geocoded, even though closest street corner to where they last slept was used for address, and so this analysis underestimates MMC utilization by homeless patients that are mobile but who remain highly vulnerable and marginalized from traditional healthcare settings. Last, MMC clients that solely use harm reduction services (e.g., condom or clean syringe distribution) are not included in our clinical database and thus, making our analysis conservative since previous studies have shown that individuals who use harm reduction services are unlikely to travel more than 4 blocks (Cooper et al. 2011).
CONCLUSIONS
The aim of the Affordable Care Act (ACA) includes increasing the number of insured individuals in the United States and overcoming health disparities. The ACA, however, has no provisions for MMCs, which appear to serve as an important component of healthcare delivery, especially to vulnerable populations. Such populations that derive increased benefit, despite lack of geographic proximity, include those that have highly stigmatized conditions, including HIV, SUDs, mental illness, homeless populations, racial and ethnic minorities and foreign-born persons. As patients are enrolled in care and expected to receive care in nearby federally qualified community healthcare centers, subsets of patients with socially or medically stigmatizing conditions may still not utilize them. The added use of geographic assessments is a move towards expansion of patient-centered medical homes, which have as their underlying premise to improve accessible, comprehensive, coordinated, high quality, and cost-effective care for patients (Peikes et al. 2012).
Acknowledgments
This research involves analyzing clinical data from the Yale University School of Medicine’s Community Health Care Van (CHCV) mobile medical clinic and was approved by the Yale School of Medicine Institutional Review Board. We would like to thank all of the clients of the CHCV and staff, including Mary Walton, M.H.S., PA-C; R. Douglas Bruce, M.D., M.A., M.Sc.; Sharon Joslin, APRN., Billy Hipp, NPC; Natalie Lourenco, PA-C; Elizabeth Roessler, PA-C; Angel P. Ojeda; Rolo Lopez; Lisandra Estremera; and David P. Hunt, PA-C.
Funding was provided by the National Institutes on Drug Abuse for Career Development (FLA: K24 DA017072) and Research (FLA: R01 DA13805, R01 DA017059), the National Institutes of Allergy and Infectious Diseases (JPM: T32 A1007517), Substance Abuse and Mental Health Services Agency (TI 019806, TI 15767-01), and the National Institutes on Drug Abuse for Career Development Award (DG: K01 DA037794). Additional sources of funding for CHCV operations included the Gilead Sciences Foundation, Liberty Community Services, the Hunger and Homelessness Project at Yale School of Medicine, and the Yale-New Haven Hospital Medical Staff Fund. The authors do not declare any conflicts of interest. This study was approved by the Yale University School of Medicine Institutional Review Board (HIC # 1302011503).
Bibliography
- Acury TA, Gesler WM, Preisser JS, Sherman J, Spencer J, Perin J. The Effects of Geography and Spatial Behavior on Health Care Utilization among the Residents of a Rural Region. HSR: Health Services Research. 2005;40(1):135–156. doi: 10.1111/j.1475-6773.2005.00346.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aday L, Andersen R. Development of Indices of Access to Medical Care. Ann Arbor, MI: Health Administration Press; 1974. [Google Scholar]
- Aday L, Awe W. Health Services Utilization. In: Gochman D, editor. Handbook of Health Behavior Research:Personal and Social Determitants. New York: Plenum; 1997. pp. 153–172. [Google Scholar]
- Altice FL, Mezger JA, Hodges J, Bruce RD, Marinovich A, Walton M, Springer SA, Friedland GH. Developing a directly administered antiretroviral therapy intervention for HIV-infected drug users: implications for program replication. Clin Infect Dis. 2004;38(Suppl 5):S376–387. doi: 10.1086/421400. [DOI] [PubMed] [Google Scholar]
- Altice FL, Springer S, Buitrago M, Hunt DP, Friedland GH. Pilot study to enhance HIV care using needle exchange-based health services for out-of-treatment injecting drug users. J Urban Health. 2003;80(3):416–427. doi: 10.1093/jurban/jtg053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Amarasingham R, Spalding SH, Anderson RJ. Disease conditions most frequently evaluated among the homeless in Dallas. Journal of Health Care for the Poor and Underserved. 2001;12(2):162–176. doi: 10.1353/hpu.2010.0765. [DOI] [PubMed] [Google Scholar]
- Andersen R. Revisiting the Behavioral Model and Access to Medical Care: Does it Matter? Journal of Heath and Social behavior. 1995 Mar;36:1–10. [PubMed] [Google Scholar]
- Bissonnette L, Wilson K, Bell S, Shah TI. Neighbourhoods and potential access to health care: the role of spatial and aspatial factors. Health Place. 2012;18(4):841–53. doi: 10.1016/j.healthplace.2012.03.007. [DOI] [PubMed] [Google Scholar]
- Bureau of Business and Economic Research University of New Mexico. Per Capita Personal Income by State, 1990 to 2012. 2013 [online], available: http://bber.unm.edu/econ/us-pci.htm [accessed 08/14/2013]
- Centers for Disease Control and Prevention. HIV Surveillance Report, 2011. 2013:23. http://www.cdc.gov/hiv/topics/surveillance/resources/reports/:
- Chang KT. Introduction to Geographic Information Systems. 6. McGraw-Hill Science/Engineering/Math; 2011. [Google Scholar]
- Chiu TL, Primeau C. A psychiatric mobile crisis unit in New York City: description and assessment, with implications for mental health care in the 1990s. Int J Soc Psychiatry. 1991;37(4):251–258. doi: 10.1177/002076409103700404. [DOI] [PubMed] [Google Scholar]
- Cleveland WS. Robust Locally Weighted Regression and Smoothing Scatterplots. Journal of the American Statistical Association. 1979;74(368):829–836. [Google Scholar]
- Collinson S, Ward R. A nurse-led response to unmet needs of homeless migrants in inner London. Br J Nurs. 2010;19(1):36–41. doi: 10.12968/bjon.2010.19.1.45910. [DOI] [PubMed] [Google Scholar]
- Comber AJ, Brunsdon C, Radburn R. A spatial analysis of variations in health access: linking geography, socio-economic status and access perceptions. Int J Health Geogr. 2011;10:44. doi: 10.1186/1476-072X-10-44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Connecticut Department of Public Health. Epidemiologic Profile of HIV in Connecticut. TB, HIV, STD & Viral Hepatitis Section. 2013 [online], available: http://www.ct.gov/dph/lib/dph/aids_and_chronic/surveillance/epiprofile.pdf [accessed 8/14/2013]
- Cooper HL, Des Jarlais DC, Ross Z, Tempalski B, Bossak B, Friedman SR. Spatial access to syringe exchange programs and pharmacies selling over-the-counter syringes as predictors of drug injectors’ use of sterile syringes. Am J Public Health. 2011;101(6):1118–1125. doi: 10.2105/AJPH.2009.184580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Copenhaver MM, Bruce RD, Altice FL. Behavioral counseling content for optimizing the use of buprenorphine for treatment of opioid dependence in community-based settings: A review of the empirical evidence. American Journal of Drug and Alcohol Abuse. 2007;33(5):643–654. doi: 10.1080/00952990701522674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cummins S, Curtis S, Diez-Roux AV, Macintyre S. Understanding and representing ‘place’ in health research: a relational approach. Soc Sci Med. 2007;65(9):1825–38. doi: 10.1016/j.socscimed.2007.05.036. [DOI] [PubMed] [Google Scholar]
- Daiski I. The health bus: healthcare for marginalized populations. Policy Polit Nurs Pract. 2005;6(1):30–38. doi: 10.1177/1527154404272610. [DOI] [PubMed] [Google Scholar]
- Duncan C, Jones K. Individuals and their ecologies: analysing the geography of chronic illness within a multi-level modeling framework. Journal of Health and Place. 1995;1:27–40. [Google Scholar]
- Duncan C, Jones K, Moon G. Do places matter? A multi-level analysis of of regional variation in health related behavior in Britain. Social Science and Medicine. 1995;37:753–733. doi: 10.1016/0277-9536(93)90366-c. [DOI] [PubMed] [Google Scholar]
- Edgerley LP, El-Sayed YY, Druzin ML, Kiernan M, Daniels KI. Use of a community mobile health van to increase early access to prenatal care. Maternal and Child Health J. 2007;11(3):235–239. doi: 10.1007/s10995-006-0174-z. [DOI] [PubMed] [Google Scholar]
- ESRI. ArcGIS Desktop (Release 10) Redlands, CA: 2011. [Google Scholar]
- Gelberg L, Andersen RM, Leake BD. The Behavioral Model for Vulnerable Populations: application to medical care use and outcomes for homeless people. Health Serv Res. 2000;34(6):1273–302. [PMC free article] [PubMed] [Google Scholar]
- Getis A, Ord JK. The Analysis of Spatial Association by Use of Distance Statistics. Geographical Analysis. 1992;24(3):189–206. [Google Scholar]
- Guagliardo MF. Spatial accessibility of primary care: concepts, methods and challenges. Int J Health Geogr. 2004;3(1):3. doi: 10.1186/1476-072X-3-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guruge S, Hunter J, Barker K, McNally MJ, Magalhaes L. Immigrant women’s experiences of receiving care in a mobile health clinic. J Adv Nurs. 2010;66(2):350–359. doi: 10.1111/j.1365-2648.2009.05182.x. [DOI] [PubMed] [Google Scholar]
- Harris D, Aboueissa A, Hartley D. Myocardial Infraction and Heart Failure Hospitalization in Maine, USA - Variability among the Urban-Rural Continuum. Rural and Remote Health. 2008;8:980. [PubMed] [Google Scholar]
- Hastings J, Zulman D, Wali S. UCLA mobile clinic project. J of Health Care Poor Underserved. 2007;18(4):744–748. doi: 10.1353/hpu.2007.0097. [DOI] [PubMed] [Google Scholar]
- Heimer R, Kaplan EH, Khoshnood K, Jariwala B, Cadman EC. Needle exchange decreases the prevalence of HIV-1 proviral DNA in returned syringes in New Haven, Connecticut. Am J Med. 1993;95(2):214–220. doi: 10.1016/0002-9343(93)90263-o. [DOI] [PubMed] [Google Scholar]
- Heller BR, Goldwater MR. The Governor’s Wellmobile: Maryland’s mobile primary care clinic. J Nurs Educ. 2004;43(2):92–94. doi: 10.3928/01484834-20040201-11. [DOI] [PubMed] [Google Scholar]
- Hine J, Kamruzzaman M. Journeys to health services in Great Britain: an analysis of changing travel patterns 1985–2006. Health Place. 2012;18(2):274–85. doi: 10.1016/j.healthplace.2011.09.018. [DOI] [PubMed] [Google Scholar]
- Ing EC, Bae JW, Maru DS, Altice FL. Medication Persistence of HIV-infected Drug Users on Directly Administered Antiretroviral Therapy. AIDS Behavior. 2011;17(1):117–121. doi: 10.1007/s10461-011-0082-0. [DOI] [PubMed] [Google Scholar]
- Jit M, Stagg HR, Aldridge RW, White PJ, Abubakar I. Dedicated outreach service for hard to reach patients with tuberculosis in London: observational study and economic evaluation. BMJ. 2011;343:d5376. doi: 10.1136/bmj.d5376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones K, Moon G. Medical Geography: taking space seriously. Progress in Human Geography. 1993;17(4):515–524. [Google Scholar]
- Joseph A, Philips D. Accessibility and Utilization: Geographical Perspectives on Heathcare Delivery. New York: Harper and Row; 1984. [Google Scholar]
- Kearns R, Joseph A. Space in its place: developing the link in medical geography. Social Science and Medicine. 1993;37(6):711–717. doi: 10.1016/0277-9536(93)90364-a. [DOI] [PubMed] [Google Scholar]
- Leese GP, Ahmed S, Newton RW, Jung RT, Ellingford A, Baines P, Roxburgh S, Coleiro J. Use of mobile screening unit for diabetic-retinopathy in rural and urban areas. BMJ. 1993;306(6871):187–189. doi: 10.1136/bmj.306.6871.187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liebman J, Pat Lamberti M, Altice F. Effectiveness of a mobile medical van in providing screening services for STDs and HIV. Public Health Nurs. 2002;19(5):345–353. doi: 10.1046/j.1525-1446.2002.19504.x. [DOI] [PubMed] [Google Scholar]
- Littenberg B, Strauss K, MacLean C, Troy A. The Use od Insulin Declines as Patients Live Farther from their Source of Care: Results of a Survey of adults with Type 2 diabetes. BMC Public Health. 2006;6:198. doi: 10.1186/1471-2458-6-198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maheswaran H, Thulare H, Stanistreet D, Tanser F, Newell ML. Starting a home and mobile HIV testing service in a rural area of South Africa. J Acquir Immune Defic Syndr. 2012;59(3):e43–46. doi: 10.1097/QAI.0b013e3182414ed7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malqvist M, Sohel N, Do TT, Eriksson L, Persson LA. Distance decay in delivery care utilisation associated with neonatal mortality. A case referent study in northern Vietnam. BMC Public Health. 2010;10:762. doi: 10.1186/1471-2458-10-762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maru DS, Bruce RD, Walton M, Mezger JA, Springer SA, Shield D, Altice FL. Initiation, adherence, and retention in a randomized controlled trial of directly administered antiretroviral therapy. AIDS Behavior. 2008;12(2):284–293. doi: 10.1007/s10461-007-9336-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Massie HN. Neighborhood psychiatry in a mobile health unit: a report on psychiatric contact with adolescents and young adults in the Judson Mobile Health Unit in New York’s Lower East Side in 1969 and 1970. Compr Psychiatry. 1972;13(5):429–433. doi: 10.1016/0010-440x(72)90084-3. [DOI] [PubMed] [Google Scholar]
- Meyer JP, Springer SA, Altice FL. Substance abuse, violence, and HIV in women: a literature review of the syndemic. J Womens Health (Larchmt) 2011;20(7):991–1006. doi: 10.1089/jwh.2010.2328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Monnet E. Place of Residence and Distance to Medical Care Influence the Diagnosis of Hepatitis C: A Population-Based Study. Journal of Hepatology. 2006;44:499–506. doi: 10.1016/j.jhep.2005.11.044. [DOI] [PubMed] [Google Scholar]
- Morano JP, Gibson BA, Altice FL. The Burgeoning HIV/HCV Syndemic in the Urban Northeast: HCV, HIV, and HIV/HCV Coinfection in an Urban Setting. Plos One. 2013a;8(5):e64321. doi: 10.1371/journal.pone.0064321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morano JP, Walton MR, Zelenev A, Bruce RD, Altice FL. Latent Tuberculosis Infection: Screening and Treatment in an Urban Setting. J Community Health. 2013b;38(5):941–950. doi: 10.1007/s10900-013-9704-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nemet G, Bailey A. Distance and Health Care Utlization among the Rural Elderly. Social Science and Medicine. 2000;50:1197–1208. doi: 10.1016/s0277-9536(99)00365-2. [DOI] [PubMed] [Google Scholar]
- Noss A. Household Income for States: 2010 and 2011. American Community Survey Briefs. 2012 [online], available: http://www.census.gov/prod/2012pubs/acsbr11–02.pdf [accessed 6/10/13]
- Okwaraji YB, Cousens S, Berhane Y, Mulholland K, Edmond K. Effect of geographical access to health facilities on child mortality in rural Ethiopia: a community based cross sectional study. Plos One. 2012;7(3):e33564. doi: 10.1371/journal.pone.0033564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ord JK, Getis A. Local Spatial Autocorrelation Statistics - Distributional Issues and an Application. Geographical Analysis. 1995;27(4):286–306. [Google Scholar]
- Peikes D, Zutshi A, Genevro JL, Parchman ML, Meyers DS. Early evaluations of the medical home: building on a promising start. Am J Manag Care. 2012;18(2):105–16. [PubMed] [Google Scholar]
- Penchansky R, Thomas JW. The concept of access: definition and relationship to consumer satisfaction. Med Care. 1981;19(2):127–140. doi: 10.1097/00005650-198102000-00001. [DOI] [PubMed] [Google Scholar]
- Peritogiannis V, Mantas C, Alexiou D, Fotopoulou V, Mouka V, Hyphantis T. The contribution of a mobile mental health unit to the promotion of primary mental health in rural areas in Greece: A 2-year follow-up. Eur Psychiat. 2011;26(7):425–427. doi: 10.1016/j.eurpsy.2010.07.001. [DOI] [PubMed] [Google Scholar]
- Pilkington H, Blondel B, Drewniak N, Zeitlin J. Choice in maternity care: associations with unit supply, geographic accessibility and user characteristics. Int J Health Geogr. 2012;11(35) doi: 10.1186/1476-072X-11-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollack HA, Khoshnood K, Blankenship KM, Altice FL. The impact of needle exchange-based health services on emergency department use. J Gen Intern Med. 2002;17(5):341–348. doi: 10.1046/j.1525-1497.2002.10663.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruiz M, Briones-Chavez CS. How to improve the health of undocumented Latino immigrants with HIV in New Orleans: an agenda for action. Rev Panam Salud Publica. 2010;28(1):66–70. doi: 10.1590/s1020-49892010000700010. [DOI] [PubMed] [Google Scholar]
- Ruiz P, Vazquez W, Vazquez K. The mobile unit: a new approach in mental health. Community Ment Health J. 1973;9(1):18–24. doi: 10.1007/BF01441428. [DOI] [PubMed] [Google Scholar]
- SAMHSA. Behavioral Health Treatment Facilities Locator. 2013 [online], available: http://findtreatment.samhsa.gov/ [accessed 5/10/13]
- Sarnquist CC, Soni S, Hwang H, Topol BB, Mutima S, Maldonado YA. Rural HIV-infected women’s access to medical care: ongoing needs in California. AIDS Care. 2011;23(7):792–796. doi: 10.1080/09540121.2010.516345. [DOI] [PubMed] [Google Scholar]
- Schwarz R, Zelenev A, Bruce RD, Altice FL. Retention on buprenorphine treatment reduces emergency department utilization, but not hospitalization, among treatment-seeking patients with opioid dependence. J Subst Abuse Treat. 2012;43(4):451–457. doi: 10.1016/j.jsat.2012.03.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwarz RK, Bruce RD, Ball SA, Herme M, Altice FL. Comparison of tuberculin skin testing reactivity in opioid-dependent patients seeking treatment with methadone versus buprenorphine: policy implications for tuberculosis screening. Am J Drug Alcohol Abuse. 2009;35(6):439–444. doi: 10.3109/00952990903447741. [DOI] [PubMed] [Google Scholar]
- Shannon K, Rusch M, Shoveller J, Alexson D, Gibson K, Tyndall MW. Mapping violence and policing as an environmental-structural barrier to health service and syringe availability among substance-using women in street-level sex work. Int J Drug Policy. 2008;19(2):140–147. doi: 10.1016/j.drugpo.2007.11.024. [DOI] [PubMed] [Google Scholar]
- Sherman J, Spencer J, Preisser J, Gesler W, Arcury T. A Suite of Methods for Representing Activity Space in a Healthcare Accessibility Study. Int J Health Geogr. 2005;4:24. doi: 10.1186/1476-072X-4-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simsek Z, Koruk I, Doni NY. An operational study on implementation of mobile primary healthcare services for seasonal migratory farmworkers, Turkey. Matern Child Health J. 2012;16(9):1906–1912. doi: 10.1007/s10995-011-0941-3. [DOI] [PubMed] [Google Scholar]
- Singer M. Dose of drugs, a touch of violence, a case of AIDS: conceptualizing the SAVA syndemic. Free Inquiry in Creative Sociology. 1996;24(2):99–110. [Google Scholar]
- Smith-Rohrberg D, Mezger J, Walton M, Bruce RD, Altice FL. Impact of enhanced services on virologic outcomes in a directly administered antiretroviral therapy trial for HIV-infected drug users. J Acquir Immune Defic Syndr. 2006;43(Suppl 1):S48–53. doi: 10.1097/01.qai.0000248338.74943.85. [DOI] [PubMed] [Google Scholar]
- StataCorp. STATA (Release 12) College Station, TX: 2011. [Google Scholar]
- Stein JA, Andersen R, Gelberg L. Applying the Gelberg-Andersen behavioral model for vulnerable populations to health services utilization in homeless women. J Health Psychol. 2007;12(5):791–804. doi: 10.1177/1359105307080612. [DOI] [PubMed] [Google Scholar]
- Teljeur C, O’Dowd T, Thomas S, Kelly A. The distribution of GPs in Ireland in relation to deprivation. Health Place. 2010;16(6):1077–83. doi: 10.1016/j.healthplace.2010.06.011. [DOI] [PubMed] [Google Scholar]
- Thompson AS, Blankenship KM, Selwyn PA, Khoshnood K, Lopez M, Balacos K, Altice FL. Evaluation of an innovative program to address the health and social service needs of drug-using women with or at risk for HIV infection. J Community Health. 1998;23(6):419–440. doi: 10.1023/a:1018706107776. [DOI] [PubMed] [Google Scholar]
- Thompson MA, Mugavero MJ, Amico KR, Cargill VA, Chang LW, Gross R, Orrell C, Altice FL, Bangsberg DR, Bartlett JG, Beckwith CG, Dowshen N, Gordon CM, Horn T, Kumar P, Scott JD, Stirratt MJ, Remien RH, Simoni JM, Nachega JB. Guidelines for improving entry into and retention in care and antiretroviral adherence for persons with HIV: evidence-based recommendations from an International Association of Physicians in AIDS Care panel. Ann Intern Med. 2012;156(11):817–833. doi: 10.7326/0003-4819-156-11-201206050-00419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- University of Connecticut, Libraries Map and Geographic Information Center. Connecticut Tracts. 2010 [online], available: http://magic.lib.uconn.edu/connecticut_data.html#boundaries [accessed 5/10/13]
- Vavasis A, Oriol N, Bennet J, Cote P, DeLorenzo DA, Hill C. Mobile Health Clinics in the United States. Report for the U.S. Department of Health and Human Services Office of Minority Health. 2013 [online], available: www.mobilehealthmap.org [accessed 8/01/2013]
- Vyas A, Madhavan S, Lemasters T, Atkins E, Gainor S, Kennedy S, Kelly K, Vona-Davis L, Remick S. Factors Influencing Adherence to Mammography Screening Guidelines in Appalachian Women Participating in a Mobile Mammography Program. J Community Health. 2011;37(3):632–646. doi: 10.1007/s10900-011-9494-z. [DOI] [PubMed] [Google Scholar]
- Wang F, Luo W. Assessing spatial and nonspatial factors for healthcare access: towards an integrated approach to defining health professional shortage areas. Health Place. 2005;11(2):131–146. doi: 10.1016/j.healthplace.2004.02.003. [DOI] [PubMed] [Google Scholar]
- Whelan C, C C, Chan M, Thomas S, Ramos G, Hwang SW. Why do homeless people use a mobile health unit in a country with universal health care? J Primary Care Community Health. 2010;1(2):78–82. doi: 10.1177/2150131910372233. [DOI] [PubMed] [Google Scholar]
- Winters C, Cudney S, Sullivan T, Thuesen A. The Rural Context and Women’s Self-Management of Chronic Health Conditions. Chronic Illness. 2006;2:273–289. doi: 10.1177/17423953060020040801. [DOI] [PubMed] [Google Scholar]
- Wong N, Lee S, Lin H. Assessing the spatial distribution of methadone clinic clients and their access to treatment. Harm Reduction Journal. 2010;7(14) doi: 10.1186/1477-7517-7-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wright PB, Stewart KE, Curran GM, Booth BM. A Qualitative Study of Barriers to the Utilization of HIV Testing Services Among Rural African American Cocaine Users. J Drug Issues. 2013;43(3):314–334. doi: 10.1177/0022042613476260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yao J, Murray AT, Agadjanian V. A geographical perspective on access to sexual and reproductive health care for women in rural Africa. Soc Sci Med. 2013;96:60–8. doi: 10.1016/j.socscimed.2013.07.025. [DOI] [PMC free article] [PubMed] [Google Scholar]