

Abstract
Background:
Childhood obesity is a worldwide major public health problem in both developed and developing countries. The purpose of this study was to determine the prevalence of obesity and overweight in 12-14-year-old students in the city of Isfahan.
Methods:
This study was conducted among 10,531 girls and 2415 boys aged 12–14 years in the city of Isfahan. Percentage of children in the corresponding body mass index (BMI) categories for overweight and obesity (specified by the Centers for Disease Control and Prevention criteria percentiles) were assessed, based on preventive plan of inactivity in children and youth of Isfahan province.
Results:
Findings revealed that prevalence of overweight in children varied by age from 15.3% to 26.9% in boys and 12.9% to 29.9% in girls, and prevalence of obesity varied from 14.8% to 33.7% and 15% to 29.9% in boys and girls, respectively. Percentile norms for BMI of subjects were computed based on sex categories.
Conclusions:
To conclude, results of the study revealed that subjects have approximately the same percentage of overweight/obesity compared to other children have been studied; however, in comparison to previous studies, a higher rate was witnessed in grade 8 boy students. These situations indicate that there are needs to implement some intervention programs, as well as management policies.
Keywords: Children, Isfahan, obesity, overweight, prevalence
INTRODUCTION
The prevalence of childhood obesity is increasing at an alarming rate, and many local governments have enacted policies to increase physical activity in schools as a way to fight childhood obesity.[1] Determining the prevalence of overweight and obesity in children is of obvious importance, because it has been reported that more than 60% of obese children have one or more cardiovascular risk factors such as hyperinsulinemia, glucose intolerance, dyslipidemia, or hypertension that are directly or indirectly related to obesity.[1,2]
Overweight children are reported to have higher fasting glucose levels,[3] and they produce more insulin after a glucose challenge.[3] An increased body mass index (BMI) in adolescence predicts elevated adult mortality and cardiovascular disease rates, even if the excessive body weight is lost.[3,4] Childhood obesity is reported to be an important predictor of adult obesity,[5] as more than 60% of children who are overweight before puberty will be overweight in early adulthood as well. This issue is of particular concern as it will probably reduce the average age at which noncommunicable diseases become apparent, thus greatly increasing the burden on health services which will have to provide treatment during most of their adult life.[6,7] Unfortunately, children are now more frequently subject to many obesity-related health conditions than before, because of automated and inactive lifestyle.
Most studies in this regard indicate that one in four children aged 6–14 years is overweight in developed and developing countries,[8] which ranges from 11% to 39%.[3] Although the prevalence of overweight and obesity was reported significantly different between genders, as some studies reported higher prevalence in girls,[8] and some in boys,[3,9,10] some studies have reported similar prevalence in both genders.[8]
Based on published data in a health survey conducted in 1999, prevalence rates of overweight and obesity for school-aged Iranian children was 13.6%.[11] Low levels of physical activity and health-related physical fitness represented by cardio-respiratory endurance have been reported in some studies, but little data have been recorded regarding the middle school students in the city of Isfahan.
There are only a few data available about the prevalence of overweight and obesity among children in the city of Isfahan, the second large city in Iran. As we need solid base to implement preventive and treatment strategies of heath care organizations, the purpose of this study was to determine the prevalence of obesity and overweight in 12–14 years old students in city of Isfahan.
METHODS
Subjects
This descriptive survey was performed among 12,946 students aged 12–14 years in Isfahan county, from whom 2415 were boys and 10,531 girls, respectively. Evaluations were performed during February to May 2010. Stratified random sampling was used in this study. A number of 30 schools were identified and randomly selected from Isfahan city on a proportional basis. Principals of the schools were contacted with the aims of the study explained to both physical education teachers and school administrators. Agreement forms for parents were distributed, and once schools and parents had agreed to let their children participate in the study, they completed a testing participation and medical history questionnaire and were informed that they could withdraw from the study at any time. Participants were in good health, free from musculoskeletal dysfunctions, metabolic disorders, and heart diseases. None of the subjects were on medication at the time of the study.
Measurements
Each child underwent a 1-day testing session in which anthropometric assessment tests were carried out. Heights were measured using a stadiometer (Novin Company, Tehran, Iran) to the nearest 0.5 cm while body weights were obtained to the nearest 0.2 kg using a calibrated balance beam scale (Novin, Iran). BMI was calculated as weight (kg)/height (m2). Children were considered overweight or obese based on age-specific BMI reference guidelines.[12,13]
Statistical analysis
Descriptive statistics was conducted on all the measured variables, and percentile ranks for BMI of subjects were computed based on sex categories. Data were analyzed by the SPSS-PC software (version 20.0) IBM SPSS inc. USA.
RESULTS
The descriptive data of the measured variables such as the mean of weight, height, and BMI of subjects are shown in Table 1. In Tables 2 and 3, we can find the normative data for BMI of male and female children. Table 4 shows the prevalence of overweight and obesity in children specified according to the 85th and 95th percentile from Centers for Disease Control and Prevention (CDC) criteria. Prevalence of overweight based on CDC criteria varied by age from 15.3% to 26.9% in boys and 12.9–29.9% in girls, and prevalence of obesity varied from 14.8% to 33.7% and 15–29.9% in boys and girls, respectively. The older group (14 years) in both sex had the higher prevalence.
Table 1.
Descriptive data related to measured variables in students (n=12,946)

Table 2.
BMI percentiles of girl students aged 12–14 years in the city of Isfahan
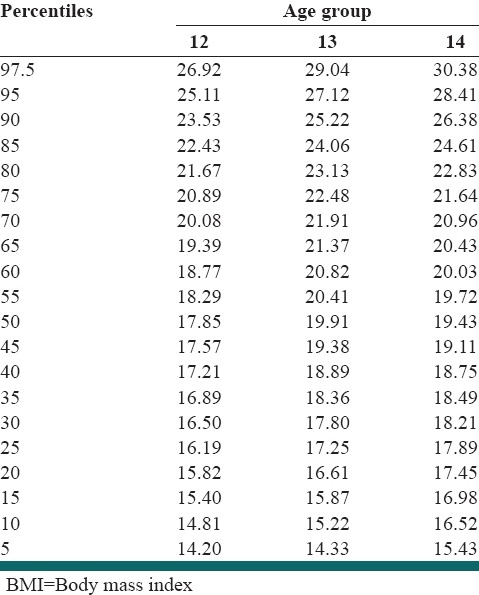
Table 3.
BMI percentiles in boy students aged 12-14 years in the city of Isfahan
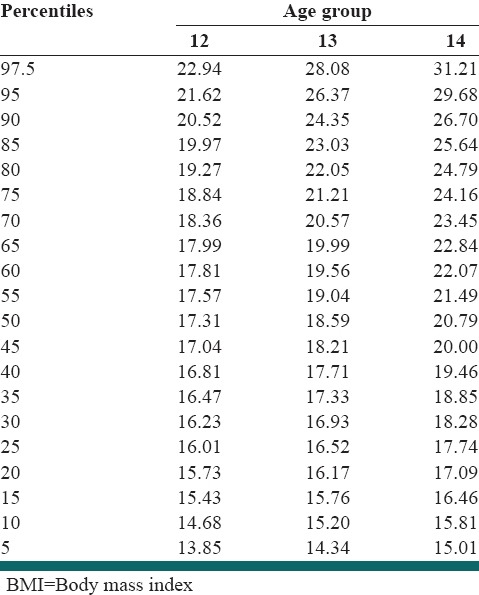
Table 4.
Distribution of body composition based on CDC criteria in 12-14 years students

The data obtained from the present study demonstrated that the prevalence of overweight was not similar among boys and girls; as girls had higher BMI levels compared to their male counterparts in all age categories. Since, we did not assess the stage of puberty of subjects, and there are probably gender differences in sexual maturation of them, it is necessary to consider some cautions for interpretation of results.
DISCUSSION
Childhood obesity is becoming a worldwide epidemic problem. When children, who were obese and overweight by BMI criteria, were considered together, more alarming data were generated as higher values of overweight and obese children found in this study (45% for boys and 43% girls) compared to other studies.[1,14,15] Al-Nakeeb et al. indicated that over 37% of boys and girls from Birmingham fell into overweight and obese classifications, with one in 5 (22%) children having more than 30% body-fat.[16] They also reported that 71% of children had a percentage of body-fat in excess of 20%, which is recognized as the upper end of the optimal range for this age-group.[13] In a study that held on Mexican children, authors reported that based on the CDC percentiles, overweight prevalence in different age groups varied from 10.8% to 16.1% in boys and from 14.3% to 19.1% in girls, whereas obesity prevalence were from 9.2% to 14.7% in boys and 6.8% to 10.6% in girls.[5] The prevalence of obesity among children from Spain was 5–8%,[10] while it was 7.9% among boys and 4.7% among girls in Qatari adolescents.[17,18]
There is little evidence of significant age differences in overweight or obesity among Iranian middle school students, either for boys or girls, but analysis of data in current studies indicates that there is a tendency for 12-year-old girls and boys to have lower levels of overweight or obesity than those aged 14 years that is consistent with previous studies.[1,13]
Goran et al. reported that boys have a higher prevalence of overweight and obesity than girls in almost all countries involved in study at all ages, except for a few exceptions like in 11-year-olds in Denmark, France, The Netherlands and the United Kingdom and in 13-year-olds in Ireland, where girls are more frequently overweight and obese than boys. In 11-year-olds, the prevalence of overweight or obesity is 16% among boys and 12% among girls; this difference persists at 13 years of age, where the prevalence is 15% in boys and 10% in girls and continues in 15-year-olds.[2,11]
A similar worsening pattern can be seen in boys. There were no countries or areas in which the prevalence in boys in 2001 was below 5%; and it increased in all countries and areas with obesity and overweight prevalence lower than 10% in 2001 except The Netherlands.[8,9,10,11,12,13,14,15,16,17,18,19] Among twelve countries or areas where the prevalence in boys was >15% in 2001, over the period, a fall in prevalence was seen in only six. The prevalence continued to increase in two of the six countries (Greece and Italy) where the prevalence was >20% in 2001, although it did begin to fall in Malta, Portugal, Spain, and the United Kingdom.[1,10]
These trends reveal the fact that despite many international and national efforts, their positive consequences have not become apparent. Many initiatives have taken place in the last few years, including legislation, action plans, and guidelines for preventing obesity. The prevalence and temporal trends in obesity reveal the need for a greater commitment on the part of countries in order to put these recommendations and tools into practice to address the main driving forces of this health burden, including nutrition, physical activity, and lifestyle.[20]
Much effort needs to be dedicated in the next few years to make sure that the instruments available are used and implemented, as well as assessing their effectiveness through continued monitoring and assessment of their effects. Hence, it is not surprising that people who have sedentary lifestyles also have low levels of fitness and excessive body fat.[2] Therefore, it appears that the goal of optimal altering of adiposity in children should begin with increasing physical activity and fitness, which, in turn, will lead to reductions in body-fat. Moreover, children who improve their cardiovascular fitness during childhood have less overall adiposity and less abdominal adiposity than their counterparts during adolescence and adulthood.[8] Participation in vigorous physical activities has been shown to relate inversely to fat deposition in both children and adults.[13]
The primary behavioral and environmental factors causing obesity are food-consumption patterns, sedentary behavior, and socioeconomic status.[12,14,19] The gradual increase in body weight that leads to obesity is the consequence of a prolonged positive energy balance, meaning when energy intake exceeds energy loss. There are many factors that can influence energy balance and therefore be identified as contributors to the current obesity epidemic in children, with biological, behavioral, environmental, and social being most cited.[18] Although the relative contribution of energy intake versus energy loss to the obesity epidemic is a source of continuing debate, available data clearly indicate that physical activity plays an integral role in the prevention of obesity.[15,20]
Inactivity is only one of the factors interconnected with obesity, and perhaps it is one of the easiest to modify.[1] Guidelines for physical activity in children and youth recommended to participate in moderate to vigorous physical activities for at least 60 min a day for health promotion and from a weight-control perspective.[21]
Recent studies suggest that inactivity is only one of the factors interconnected with obesity; however, it is perhaps one of the easiest to modify.[1,21] Guidelines for physical activity in youths recommend involvement in moderate to vigorous physical activities for at least 60 min a day for health promotion and from a weight-control perspective.[13,22] According to the results of the present study and the fact that Iranian academic curriculum includes only 90-min physical activity for students per week, initiatives should be put forward to promote physical activity in Iranian children in both school and out-of-school environment.
Limitations
The clear understanding of the prevalence of overweight and obesity of children in the present study may not be possible due to several limitations. It seems that more accurate measures of body composition are required to determine the levels of overweight and obesity. Furthermore, we faced some limitations in selection and participation of male students compared to their female counterparts; hence more girl students were participated in this study. Last but not least, for establishing a more relevant standards for childhood overweight and obesity it can be said that although measurement of skinfold is more time-consuming, it is a relatively strong substitute for BMI for measuring the percentage of body-fat.
CONCLUSIONS
Our results suggest that aerobic fitness as an indicator of physical activity is linked to the increased level of adiposity in children. According to the results of the present study and the fact that Iranian academic curriculum includes only 90-min physical activity per week, initiatives should be put forward to promote physical activity in Iranian children in both school and out-of-school environments.
ACKNOWLEDGMENTS
The authors would like to thank the study participants for their cooperation and dedication. We wish to thank the Isfahan Provincial Health Office's administrators and personnel that helped and supported us in this study. This study was financially supported by the Provincial Health Office, Isfahan University of Medical Sciences, Isfahan-Iran.
Footnotes
Source of Support: This study was financially supported by the Provincial Health Office, Isfahan University of Medical Sciences, Isfahan-Iran
Conflict of Interest: None declared.
REFERENCES
- 1.del Río-Navarro BE, Velázquez-Monroy O, Sánchez-Castillo CP, Lara-Esqueda A, Berber A, Fanghänel G, et al. The high prevalence of overweight and obesity in Mexican children. Obes Res. 2004;12:215–23. doi: 10.1038/oby.2004.28. [DOI] [PubMed] [Google Scholar]
- 2.Krassas GE, Tzotzas T, Tsametis C, Konstantinidis T. Prevalence and trends in overweight and obesity among children and adolescents in Thessaloniki, Greece. J Pediatr Endocrinol Metab. 2001;14(Suppl 5):1319–26. [PubMed] [Google Scholar]
- 3.Brunet M, Chaput JP, Tremblay A. The association between low physical fitness and high body mass index or waist circumference is increasing with age in children: The ‘Québec en Forme’ Project. Int J Obes (Lond) 2007;31:637–43. doi: 10.1038/sj.ijo.0803448. [DOI] [PubMed] [Google Scholar]
- 4.Al-Nakeeb Y, Lyons M, Collins P, Al-Nuaim A, Al-Hazzaa H, Duncan M, et al. Obesity, Physical Activity and Sedentary Behavior Amongst British and Saudi Youth: A Cross-Cultural Study, Int. J. Environ. Res. Public Health. 2012;9:1490–1506. doi: 10.3390/ijerph9041490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kimm SY, Glynn NW, Obarzanek E, Kriska AM, Daniels SR, Barton BA, et al. Relation between the changes in physical activity and body-mass index during adolescence: A multicentre longitudinal study. Lancet. 2005;366:301–7. doi: 10.1016/S0140-6736(05)66837-7. [DOI] [PubMed] [Google Scholar]
- 6.Wang Y, Monteiro C, Popkin BM. Trends of obesity and underweight in older children and adolescents in the United States, Brazil, China, and Russia. Am J Clin Nutr. 2002;75:971–7. doi: 10.1093/ajcn/75.6.971. [DOI] [PubMed] [Google Scholar]
- 7.Meigs JB, Muller DC, Nathan DM, Blake DR, Andres R. Baltimore Longitudinal Study of Aging. The natural history of progression from normal glucose tolerance to type 2 diabetes in the Baltimore Longitudinal Study of Aging. Diabetes. 2003;52:1475–84. doi: 10.2337/diabetes.52.6.1475. [DOI] [PubMed] [Google Scholar]
- 8.Ara I, Moreno LA, Leiva MT, Gutin B, Casajús JA. Adiposity, physical activity, and physical fitness among children from Aragón, Spain. Obesity (Silver Spring) 2007;15:1918–24. doi: 10.1038/oby.2007.228. [DOI] [PubMed] [Google Scholar]
- 9.Shaya FT, Flores D, Gbarayor CM, Wang J. School-based obesity interventions: A literature review. J Sch Health. 2008;78:189–96. doi: 10.1111/j.1746-1561.2008.00285.x. [DOI] [PubMed] [Google Scholar]
- 10.Goran MI, Bergman RN, Avila Q, Watkins M, Ball GD, Shaibi GQ, et al. Impaired glucose tolerance and reduced beta-cell function in overweight Latino children with a positive family history for type 2 diabetes. J Clin Endocrinol Metab. 2004;89:207–12. doi: 10.1210/jc.2003-031402. [DOI] [PubMed] [Google Scholar]
- 11.Goran MI, Reynolds KD, Lindquist CH. Role of physical activity in the prevention of obesity in children. Int J Obes Relat Metab Disord. 1999;23(Suppl 3):S18–33. doi: 10.1038/sj.ijo.0800880. [DOI] [PubMed] [Google Scholar]
- 12.Wang G, Dietz WH. Economic burden of obesity in youths aged 6 to 17 years: 1979-1999. Pediatrics. 2002;109:E81–5. doi: 10.1542/peds.109.5.e81. [DOI] [PubMed] [Google Scholar]
- 13.Ogden CL, Flegal KM, Carroll MD, Johnson CL. Prevalence and trends in overweight among US children and adolescents, 1999-2000. JAMA. 2002;288:1728–32. doi: 10.1001/jama.288.14.1728. [DOI] [PubMed] [Google Scholar]
- 14.Krebs NF, Jacobson MS, American Academy of Pediatrics Committee on Nutrition. Prevention of pediatric overweight and obesity. Pediatrics. 2003;112:424–30. doi: 10.1542/peds.112.2.424. [DOI] [PubMed] [Google Scholar]
- 15.Centers for Disease Control and Prevention (CDC). Overweight among students in grades K-12 – Arkansas, 2003-04 and 2004-05 school years. MMWR Morb Mortal Wkly Rep. 2006;55:5–8. [PubMed] [Google Scholar]
- 16.Ross R, Katzmarzyk PT. Cardiorespiratory fitness is associated with diminished total and abdominal obesity independent of body mass index. Int J Obes Relat Metab. 2003;27:204–10. doi: 10.1038/sj.ijo.802222. [DOI] [PubMed] [Google Scholar]
- 17.Shultz SP, Browning RC, Schutz Y, Maffeis C, Hills AP. School-based interventions for childhood and adolescent obesity. J Int Assoc Study Obes. 2006;7:332–41. [Google Scholar]
- 18.Ostojic SM, Stojanovic MD, Stojanovic V, Maric J, Njaradi N. Correlation between fitness and fatness in 6-14-year old Serbian school children. J Health Popul Nutr. 2011;29:53–60. doi: 10.3329/jhpn.v29i1.7566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Molnár D, Livingstone B. Physical activity in relation to overweight and obesity in children and adolescents. Eur J Pediatr. 2000;159(Suppl 1):S45–55. doi: 10.1007/pl00014365. [DOI] [PubMed] [Google Scholar]
- 20.Pate RR, Saunders R, Dishman RK, Addy C, Dowda M, Ward DS. Long-term effects of a physical activity intervention in high school girls. Am J Prev Med. 2007;33:276–80. doi: 10.1016/j.amepre.2007.06.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lee SJ, Arslanian SA. Cardiorespiratory fitness and abdominal adiposity in youth. Eur J Clin Nutr. 2007;61:561–5. doi: 10.1038/sj.ejcn.1602541. [DOI] [PubMed] [Google Scholar]
- 22.King AC, Parkinson KN, Adamson AJ, Murray L, Besson H, Reilly JJ, et al. Correlates of objectively measured physical activity and sedentary behaviour in English children. Eur J Public Health. 2011;21:424–31. doi: 10.1093/eurpub/ckq104. [DOI] [PubMed] [Google Scholar]