

Abstract
Background
The physical work demands of construction work can be reduced using ergonomic measures. The aim of this study was to evaluate the use of ergonomic measures related to musculoskeletal disorders (MSDs) among construction workers.
Methods
A questionnaire was sent at baseline and 2 years later to 1,130 construction workers. We established (1) the proportion of workers reporting an increase in their use of ergonomic measures, (2) the proportion of workers reporting a decrease in MSDs, (3) the relative risk for an increase in the use of ergonomic measures and a decrease in MSDs, and (4) workers' knowledge and opinions about the use of ergonomic measures.
Results
At follow-up, response rate was 63% (713/1,130). The proportion of workers using ergonomic measures for vertical transport increased (34%, 144/419, p < 0.01); for measures regarding horizontal transport and the positioning of materials, no change was reported. The proportion of workers reporting shoulder complaints decreased (28%, 176/638, p = 0.02). A relationship between the use of ergonomic measures and MSDs was not found; 83% (581/704) of the workers indicated having sufficient knowledge about ergonomic measures. Lightening the physical load was reported to be the main reason for using them.
Conclusion
Only the use of ergonomic measures for vertical transport increased over a 2-year period. No relationship between the use of ergonomic measures and MSDs was found. Strategies aimed at improving the availability of ergonomic equipment complemented with individualized advice and training in using them might be the required next steps to increase the use of ergonomic measures.
Keywords: construction industry, ergonomics, longitudinal study, musculoskeletal pain
1. Introduction
Work-related musculoskeletal disorders (MSDs) are one of the most prevalent occupational health problems [1], affecting millions of workers every year. Specifically, construction workers face higher rates of work-related MSDs [2]: approximately 16% higher than workers in other industries [3]. Major causes of MSDs among construction workers are high physical demands [4], such as heavy lifting, repetitive motions, and awkward working postures (e.g., bending and twisting, kneeling, working with the arms above shoulder height) [3,5]. Ergonomic solutions may therefore help to reduce the risk of MSDs among construction workers [3,6].
In general, ergonomists agree that the use of ergonomic measures to reduce the physical work load of construction workers should be facilitated [7,8]. However, ergonomic measures do not find their way automatically to the workers. Therefore, the Dutch sectors' Health and Safety Institute (Arbouw, Dutch Health and Safety Institute in the Construction Industry, Harderwijk, The Netherlands) implemented the national campaign “Lighter Work(s),” whose goal was to inform both workers and employers about ergonomic measures that are aimed at decreasing adverse physical exposures. The goal of the campaign was to increase awareness and induce a change regarding ergonomic working methods and the use of mechanical ergonomic measures. The campaign was an opportunity for evaluating the use of ergonomic measures related to musculoskeletal complaints among construction workers over a 2-year period. We assumed that the physical work demands related to physically demanding construction trades would be reduced by ergonomic measures and consequently MSDs would be reduced. Therefore, we hypothesized that when the use of ergonomic measures would increase by means of a national campaign, eventually MSDs would decrease (Fig. 1). Furthermore, we wanted to gain more knowledge on barriers and facilitators for using ergonomic measures.
Fig. 1.
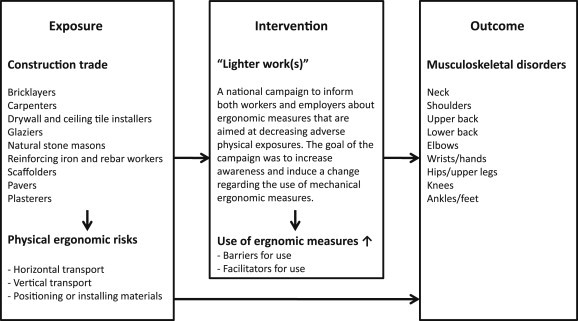
Hypothesis on the relation between exposure, ergonomic measures, and MSDs. MSDs, musculoskeletal disorders.
Physical demands vary widely across different construction occupations. Bricklayers and drywall installers, for example, spent most of their working time in a bent and twisted position while performing repetitive hand-arm movements, whereas tile workers spent most of their working time in a kneeled, crouched, or stooped position [3]. Nowadays, a wide variety of ergonomic solutions for a range of occupations can reduce the time spent by the workers in these adverse activities and improve working postures, thus potentially reducing MSDs.
The following types of ergonomic measures were highlighted in the campaign: measures for horizontal/vertical transport and for the positioning or installing of materials. Measures for horizontal transport aimed at decreasing pushing, pulling, and carrying. Measures for vertical transport aimed at decreasing heavy lifting, and measures for the positioning or installing of materials were aimed at optimizing the working height and thereby decreasing kneeling, working with a bent back, or with the arms above shoulder height.
Evidence on the impact of the use of ergonomic measures by means of a large-scale campaign like “Lighter Work(s)” is conflicting. A longitudinal study among carpenters and pavers indicated that the use of some specific ergonomic measures was associated with a lower likelihood of lower back or shoulder complaints [9], but most ergonomic measures for these occupations were not associated with such a reduction in complaints [9,10].
This paper describes a 2-year follow-up study about the use of ergonomic measures related to musculoskeletal complaints among nine construction occupations. The research questions were as follows: (1) What is the use of ergonomic measures over a 2-year period and what are the facilitating factors and barriers for using ergonomic measures?; (2) What is the change in MSDs over the 2-year period?; (3) Is there a relationship between an increase in the use of ergonomic measures and a decrease in MSDs (in the most affected body regions, i.e., the shoulders, lower back, and knees)?; and (4) To what extent do the workers have sufficient knowledge about the use of ergonomic measures and what activities are, according to the workers, needed to facilitate the use?
2. Materials and methods
2.1. Study design and participants
A 2-year follow-up study was conducted among construction workers in nine different occupations (reinforcing iron and rebar workers, glaziers, bricklayers, natural stone masons, drywall and ceiling tile installers, scaffolders, pavers, plasterers, and carpenters). We randomly selected 4,500 Dutch construction workers, 500 in each occupation. The random selection was performed by the independent data manager of the Registry of Arbouw who frequently assisted in selecting samples for research purposes.
The survey consisted of a baseline questionnaire (October 2010) and a follow-up questionnaire (March 2013). At baseline, all participants received a sealed envelope at their home address containing an invitation to participate, a questionnaire survey, and an incentive (lottery ticket, with an iPod as the first prize). At follow-up, only those who had responded at baseline were sent a second postcard, a follow-up questionnaire, and an incentive (lottery ticket). Completing the questionnaires took approximately 15 minutes. The participants were asked to fully complete and return the questionnaire within 2 weeks. One reminder letter was sent to all participants after 1 week.
2.2. The campaign “Lighter work(s)”
The campaign “Lighter Work(s)” focused on each of the ergonomic measures (when applicable) for nine construction occupations (reinforcing iron and rebar workers, glaziers, bricklayers, natural stone masons, drywall and ceiling tile installers, scaffolders, pavers, plasterers, and carpenters). The assumed efficacy of the ergonomic measures was based on evidence when possible, or based on professional and ergonomic recommendations applied by the Dutch Health and Safety Institute for the Construction Industry when no scientific evidence was available.
The campaign was supported by an informative web site (www.lichterwerkt.nl). The web site provided both workers and employers with information about physical risks for each occupation, MSDs resulting from those physical risks, and occupation-specific ergonomic measures for reducing the physical exposure. The web site included both written information and YouTube videos. Employers were invited to use a freely available toolbox (with advice, handy hints, and examples aimed at reducing the physical work demands) and posters for their workplaces. The web site was publicized through social media, radio, the Arbouw magazine, and the Arbouw web site. The campaign lasted for 2 years, and in every trimester another occupation received more specific attention.
2.3. Questionnaire
A questionnaire was designed for each occupation. The questionnaire consisted of the following items. (1) Individual characteristics: age (year of birth), years of working experience in the occupation, height (cm), and body weight (kg). (2) The current use of ergonomic measures for horizontal/vertical transport and for the positioning or installing of materials: frequency of using different ergonomic measures [(almost) never; now and then; regularly; often; and (almost) always] [9] and the reason for not using ergonomic measures (unfamiliarity; impractical; costs too much time; too expensive; and not available). In the follow-up questionnaire, one question was added regarding the respondents' reasons for using ergonomic measures (practical; works faster; better quality; works lighter; and is compulsory). (3) MSDs: Frequency and duration (never; sometimes; regular; and sustained) of complaints per bodily region (neck; shoulders; upper back; lower back; elbows; wrists/hands; hips/upper legs; knees; and ankles/feet) during the 6 months prior to filling in the questionnaire, the work relatedness according to the respondents (no; I do not know; yes, partially; yes, completely; and not applicable), worsening of the complaints due to the work (no; I do not know; yes, partially; yes, completely; and not applicable), and work limitations due to complaints (no; I do not know; yes, partially; yes, completely; and not applicable) [9,10]. (4) Opinions of the workers on the campaign and ergonomic measures, defined by the authors: Sufficient knowledge about ergonomic measures to lighten physically demanding work (yes/no), activities needed to implement the use of ergonomic measures (no activities needed; information about ergonomic measures; training or education; support by occupational health service or manager; support by colleagues; and other, own answer).
2.4. Analysis
Answers on the questionnaire were automatically imported, manually checked for errors, and impossible values were corrected. Analyses were performed for the group as a whole and separately for the nine occupations. Descriptive statistics were presented as the percentage, mean, and standard deviation (SD). The denominator was corrected for missing values. All analyses were performed with the statistical software IBM SPSS Statistics 20 (IBM, Armonk, NY, USA).
To gain insight into the characteristics and representativeness of the respondents, we tested (1) for differences in age between responders and nonresponders at follow-up using a t test and (2) the relation between having or not having MSDs at baseline and response at follow-up using univariate logistic regression analysis. Statistical significance was set at α = 0.05. The prevalence and 95% confidence interval of the MSDs were calculated using the follow-up data. Confidence intervals were calculated using the Wald method when the sample consisted of more than 150 persons and the adjusted Wald method when the sample consisted of < 150 persons [11].
2.4.1. Use of ergonomic measures and prevalence of MSDs
The use of ergonomic measures was described at the population level by means of the percentage of workers in each category using ergonomic measures and the change in percentage from baseline to follow-up. A change in the use of ergonomic measures at the individual level was described by the percentage of respondents who reported a decrease, an increase, or no change in using or not using ergonomic measures. Statistical significance of the change from baseline to follow-up 2 years later was tested by the Wilcoxon signed-rank test for paired data.
The frequency and duration of MSDs were dichotomized into “MSD present” (regular and sustained) and “no MSD” (never and sometimes). The prevalence of MSDs was described at the population level by means of the percentage of workers reporting MSDs for each bodily region and the change in percentage from baseline to follow-up. A change in MSDs at the individual level was described by the percentage of respondents who reported a decrease, an increase, or no change in MSDs. Statistical significance of the change from baseline to follow-up 2 years later was tested by the McNemar test for paired data. The work relatedness was described by the percentage of respondents for each answer category.
2.4.2. Relationship between use of ergonomic measures and MSDs
The use of ergonomic measures was dichotomized per occupation and per type of ergonomic measure into “increase in the use” and “no increase in the use” (i.e., a decrease or no change in using or not using ergonomic measures). MSD per bodily region was dichotomized into “decrease of MSD” and “no decrease of MSD” (i.e., an increase or no change in MSD).
For each occupation and each of the ergonomic measures, relative risks (RRs) were calculated for the increase in the use of the ergonomic measures for reporting a decrease in MSDs for the three bodily regions most often affected (i.e., shoulders, lower back, and knees). An RR < 1 indicates a protective effect when at least regular use of one type of ergonomic measures is associated with a decreased risk of reporting MSDs.
2.4.3. Opinions of workers on ergonomic measures
The opinions of the workers on ergonomic measures were descriptively analyzed: the percentages of respondents who had sufficient knowledge about ergonomic measures were presented. Furthermore, the activities needed to implement the use of ergonomic measures were indicated by the percentage of respondents for each of the answers. Respondents' remarks were collected, grouped into topics by the research team, and these topics qualitatively described.
3. Results
3.1. Response and respondents' characteristics
In 2010, a total of 1,551 respondents returned a questionnaire eligible for analysis (34%; 1,551/4,500). In 2013, 421 respondents were either no longer employed in the construction industry, retired, deceased, or no longer approachable for the follow-up measurement for other reasons. A total of 1,130 workers were sent the follow-up questionnaire and 713 returned a questionnaire eligible for analysis, resulting in a net response rate of 63% (713/1,130) for the follow-up. These respondents' characteristics are presented in Table 1.
Table 1.
Mean (standard deviation) age, job experience, height, and weight of the construction workers who participated in the baseline (2010) and follow-up survey (2013)
| Age (y, SD) | Job experience (y, SD) | Height (cm, SD) | Weight (kg, SD) | |
|---|---|---|---|---|
| Bricklayers (n = 129) | 53 (7.1) | 36 (8.3) | 179 (6.3) | 83 (10.1) |
| Carpenters (n = 121) | 50 (9.2) | 33 (9.9) | 180 (6.8) | 84 (10.9) |
| Glaziers (n = 54) | 53 (8.1) | 31 (8.6) | 181 (7.2) | 87 (12.7) |
| Drywall and ceiling tile installers (n = 77) | 49 (8.1) | 23 (9.0) | 182 (7.4) | 88 (11.3) |
| Stone masons (n = 66) | 49 (7.2) | 22 (12.4) | 180 (7.5) | 84 (11.6) |
| Scaffolders (n = 59) | 46 (10.6) | 21 (10.9) | 179 (6.7) | 84 (11.4) |
| Pavers (n = 87) | 49 (9.7) | 31 (11.3) | 179 (13.1) | 86 (12.3) |
| Plasterers (n = 47) | 45 (12.7) | 24 (13.4) | 179 (7.1) | 84 (9.7) |
| Reinforcing iron and rebar workers (n = 68) | 52 (7.5) | 30 (11.3) | 176 (6.3) | 84 (12.1) |
| Total population (n = 711) | 50 (9.1) | 29 (11.6) | 180 (8.0) | 85 (11.3) |
SD, standard deviation.
The respondents who participated in both the baseline and follow-up survey were statistically significantly older (mean age, 47.9 years; SD, 9.2) than those who participated only in the baseline survey (mean age, 44.4 years; SD, 12.2). No statistically significant relationship was found between having MSDs in any bodily region at baseline and responding at follow-up [odds ratio 1.11 (0.89–1.39)].
3.2. The use of ergonomic measures and facilitating factors and barriers for their use
At baseline, 21 respondents (3%) reported that they (almost) never used any of the ergonomic measures. At follow-up, this number was 26 respondents (4%). According to 59–65% of the respondents, depending on the type of ergonomic measure, the unavailability of the ergonomic equipment is the main barrier for using them. The other reasons are less often mentioned (18–23%, unfamiliarity; 11–17%, impractical; 10–18%, costs too much time; 14–16%, too expensive).
At follow-up, 19–24% of the respondents, depending on the type of ergonomic measure, reported using them (almost) always. Measures for horizontal and vertical transport were used by 69% and 71% of the workers, respectively. Measures for positioning or installing of materials are regularly or more often used by about half of the workers (54%). More than half of the respondents (55–73%) who use ergonomic measures reported that lightening the physical load is the most important reason for using ergonomic measures, irrespective of the type of measure. Working more practically (33–37%) and faster (24–38%) are other reasons for the respondents to use ergonomic measures. Fewer respondents indicated that they perceived the quality of the work to be better when using the ergonomic measures (5–8%) or that the use of the measures was compulsory (16–21%).
At the individual level, we found that a quarter of the total population decreased their use of ergonomic measures, irrespective of the type of measure. In total, 29–34% of the respondents increased their use of ergonomic measures. For the ergonomic measures used during vertical transport, the difference was statistically significant: 34% of the respondents increased their use of measures, compared with 25% of the respondents who decreased their use of measures for vertical transport (Table 2).
Table 2.
Change in the use of ergonomic measures over a period of 2 years among construction workers, percentage (95% CI) and relative frequency
| Type of ergonomic measure | Decrease in use % (95% CI) (relative frequency) |
No change (no use) % (95% CI) (relative frequency) |
No change (using) % (95% CI) (relative frequency) |
Increase in use % (95% CI) (relative frequency) |
p |
|---|---|---|---|---|---|
| For horizontal transport (n = 656) | 27 (23–30) (174/656) |
15 (12–18) (98/656) |
29 (26–33) (193/656) |
29 (26–33) (191/656) |
0.14 |
| For vertical transport* (n = 419) | 25 (21–29) (104/419) |
12 (9–15) (48/419) |
29 (25–34) (123/419) |
34 (30–39) (144/419) |
0.00 |
| For the positioning or installing of materials (n = 649) | 24 (21–27) (157/649) |
24 (21–28) (158/649) |
23 (19–26) (147/649) |
29 (25–32) (187/649) |
0.18 |
*p < 0.05
CI, confidence interval.
Regarding the specific occupations, the following statistically significant positive changes in the use of ergonomic measures were observed: 37–41% of bricklayers reported an increase in their use of measures to position their materials (bricks, blocks, mortar, glue) at working height (raised). Among the bricklayers who decreased their use of the measures (16%), the main barrier was the unavailability: 63% of these bricklayers indicated this as the reason for not using the measures. The majority of the bricklayers (81%) who increased their use of the measures indicated “work lighter” as the main reason.
Half of the reinforcing iron and rebar workers reported that they increased their use of measures to position their materials (mats and bars). As with the bricklayers, most of the iron and rebar workers reported that they experienced that the work was lighter when using the ergonomic measures. Barriers for using the measures were the expensiveness and unavailability of related ergonomic equipment.
Among the drywall and ceiling tile installers at follow-up, 43% reported using measures for horizontal transport more often compared with baseline. Those drywall and ceiling tile installers indicated that working with the measures was both faster and lighter. Unfamiliarity with the measures (20%) and unavailability (80%) were the main barriers mentioned by workers using the measures less.
3.3. Prevalence of MSDs
At follow-up, the respondents reported regular or long-lasting complaints of the lower back (43%), knees (31%), and shoulders (31%) most often. At the individual level, a statistically significant decrease in shoulder complaints was seen (28% reported a decrease, compared with 17% who reported an increase in shoulder complaints), but not for the other bodily regions (Table 3).
Table 3.
Change in percentage of workers with MSDs over a period of 2 years per bodily region among construction workers, percentage (95% CI) and frequency
| Bodily region | Decrease in complaints % (95% CI) (relative frequency) |
No change (no complaints) % (95% CI) (relative frequency) |
No change in complaints % (95% CI) (relative frequency) |
Increase in complaints % (95% CI) (relative frequency) |
p |
|---|---|---|---|---|---|
| Neck (n = 633) | 21 (18–24) (132/633) |
52 (48–56) (330/633) |
10 (8–12) (64/633) |
17 (14–20) (107/633) |
0.10 |
| Shoulders (n = 638)* | 28 (24–31) (176/638) |
43 (39–47) (274/638) |
12 (10–15) (79/638) |
17 (14–20) (109/638) |
0.02 |
| Upper back (n = 573) | 17 (14–20) (99/573) |
61 (57–65) (348/573) |
2 (1–4) (14/573) |
20 (16–23) (112/573) |
0.91 |
| Lower back (n = 664) | 24 (21–27) (160/664) |
30 (27–34) (201/664) |
21 (18–24) (140/664) |
25 (21–28) (163/664) |
0.37 |
| Elbows (n = 613) | 17 (14–19) (101/613) |
60 (56–64) (368/613) |
6 (4–8) (35/613) |
18 (15–21) (109/613) |
0.92 |
| Wrists/hands (n = 627) | 24 (20–27) (148/627) |
50 (46–54) (314/627) |
7 (5–9) (44/627) |
19 (16–22) (121/627) |
0.69 |
| Hips/upper legs(n = 613) | 21 (18–24) (129/613) |
57 (53–61) (350/613) |
6 (4–7) (36/613) |
16 (13–19) (98/613) |
0.60 |
| Knees (n = 649) | 25 (21–28) (159/649) |
41 (37–45) (266/649) |
14 (11–16) (89/649) |
21 (18–24) (135/649) |
0.12 |
| Ankles/feet (n = 619) | 18 (15–21) (113/619) |
57 (53–61) (353/619) |
5 (3–6) (28/619) |
20 (17–23) (125/619) |
1.00 |
*p < 0.05.
CI, confidence interval; MSD, musculoskeletal disorder.
At follow-up, 69% of the respondents with MSDs reported that their complaints resulted partially or completely from their work. About half of the respondents indicated that their complaints worsened because of their work and that they experienced limitations in their work due to their MSDs.
3.4. The relationship between an increase in the use of ergonomic measures and a decrease in MSDs
For all ergonomic measures it was found that the proportion of workers reporting an increase in the use of ergonomic measures and a decrease in MSDs is approximately the same (about 30%) as the proportion of workers not reporting an increase in the use of ergonomic measures and a decrease in MSDs. No relationship was found between the increase in use of ergonomic measures and a decrease in MSDs for any of the selected bodily regions, that is, lower back, knees, and shoulders (Table 4).
Table 4.
Relative risks and 95% confidence interval for increased use of ergonomic measures and decreased MSDs of lower back, shoulders, and knees over a 2-year period among construction workers*
| Increase in use of ergonomic measures for | Decrease in complaints per bodily region |
||
|---|---|---|---|
| Shoulder RR (95% CI) |
Lower back RR (95% CI) |
Knees RR (95% CI) |
|
| horizontal transport (n = 593–613) | 0.9 (0.69–1.20) | 1.4 (0.98–1.97) | 1.4 (0.96–1.90) |
| vertical transport (n = 379–390) | 0.9 (0.63–1.24) | 1.3 (0.90–2.02) | 1.1 (0.75–1.68) |
| the positioning or installing of materials (n = 586–599) | 0.9 (0.65–1.14) | 0.9 (0.67–1.25) | 1.2 (0.85–1.61) |
* RR for an “increase in the use of ergonomic measures” versus “no increase in the use” (i.e., a decrease or no change in using or not using ergonomic measures) and a “decrease of MSD” versus “no decrease of MSD” (i.e., an increase or no change in MSD).
CI, confidence interval; MSD, musculoskeletal disorder; RR, relative risk.
3.5. Opinions of workers on ergonomic measures
Four of every five respondents indicated having sufficient knowledge about ergonomic measures. Nearly all (90%) of the drywall and ceiling tile installers indicated having sufficient knowledge, whereas this percentage was the lowest among the carpenters and reinforcing iron and rebar workers (75%).
Almost 80% of the respondents (544/704) indicated that actions are needed to implement ergonomic measures in the construction industry. Actions mentioned most often were providing information (36%) and improving the support provided by the occupational health service or manager (33%). Furthermore, respondents indicated that actions should be aimed at the employer, such as stimulating employers to buy ergonomic equipment, educating employers, and making the use of ergonomic measures legally obligatory. Respondents also mentioned that the high costs should be tackled to facilitate implementation of the measures, through discounts or by reducing retail prices of the related ergonomic equipment.
4. Discussion
4.1. Major findings
In this study with a follow-up of 2 years, we found that among nine construction occupations (1) the use of ergonomic measures for vertical transport increased statistically significantly by 9%. The use of ergonomic measures for horizontal transport and for the positioning of materials showed no differences. The lightening of the physical load was the most mentioned reason for using ergonomic measures, whereas the unavailability of ergonomic equipment was the most mentioned barrier; (2) no change in MSDs for most bodily regions was found, with the exception that statistically significantly fewer shoulder complaints were reported (11%); (3) there was no relationship between an increase in the use of ergonomic measures and a decrease in MSDs; and (4) the majority of respondents indicated that they had sufficient knowledge about ergonomic measures.
We found that a high proportion of the construction workers experienced a relief of the physical demands of their work when they use ergonomic measures, as they mentioned this most often as a facilitator for using ergonomic measures. These experiences of the workers are promising and substantiate the idea that the use of ergonomic equipment in several physically demanding construction occupations reduces the physical work demands and workload of the trade.
To stimulate the use of ergonomic measures, both researchers and practitioners should primarily focus on how to remove barriers to using ergonomic measures at the level of both the employer and the employee. The campaign was also aimed at informing employers, but the main reason for not using ergonomic measures, according to the workers, can be attributed to organizational shortcomings (unavailability of ergonomic equipment). Solving practical issues such as the availability and facilitating the purchase of ergonomic equipment by employers is needed. Furthermore, counseling and assistance in implementing ergonomic measures at the worksite can be of added value in increasing the use of ergonomic measures [12].
We found no change in MSDs, except for shoulder complaints, and no relation between an increase in the use of ergonomic measures and a decrease in MSDs of the lower back, knees, and shoulders. We explored an alternative approach—RR for using ergonomic measures [i.e., now and then; regularly; often; and (almost) always] versus not using ergonomic measures [i.e., (almost) never] and a “decrease of MSD” versus “no decrease of MSD”—but no statistically significant RRs were found for any of the MSDs. Not finding an effect of an increase in the use of ergonomic measures might be due to a lack of reduction on MSD risks (as construction work is characterized by multiple ergonomic stressors to multiple bodily regions), the relatively short time of follow-up or small attributional fraction of work exposures [13]. The fact that a substantial proportion of the workers indicated that their MSDs were not work related (31%) suggests that MSDs will not be affected by a change in the physical work load alone. In addition, half of the workers indicated that their complaints worsened because of their work and that they experienced limitations in their work, therefore the number of workers who are likely to gain most by increasing their use of ergonomic measures is limited. Finally, it should be kept in mind that workers could change their working technique (e.g., lifting technique) as a result of an ergonomic intervention and thereby reduce the potential positive effect on bodily structures [14]. As previously reported by van der Molen et al [10], other aspects should be considered when interpreting and explaining the findings: (1) the number of construction workers who use ergonomic measures (almost) always was limited and thereby the effect on MSDs is likely to be limited too; (2) the preventive effect of using ergonomic measures on MSDs in general might be limited and vary among the nine occupations and among younger and older workers; (3) owing to the episodic character of MSDs, the two time points of measurement in 2 years in combination with the 6-month recall period might be too limited to fully capture the scope of the MSD problem; and (4) limited statistical power could have masked evidence for effects or relationships, although the estimate of the risks are around 1, and the differences in MSDs between the workers using ergonomic measures and those not using ergonomic measures are therefore small.
4.2. Comparison with other studies
van der Molen et al [9] studied the use of ergonomic measures after a similar national campaign among carpenters and pavers. In several aspects their results are comparable to our results: a small proportion of construction workers increased their use of particular ergonomic measures, whereas the majority did not change their use at all and another, smaller, proportion decreased their use of ergonomic measures. The percentage of workers regularly using ergonomic measures was maximally 66% in the study by van der Molen et al [9]. In our study, this percentage was only slightly higher for measures for vertical transport at 71%, and substantially lower for measures for the positioning or installing of materials (54%). Apparently, based on two similar studies, a considerable proportion of construction workers, regardless of their occupation, cannot be reached by means of a campaign designed to increase the use of ergonomic measures. Therefore, the full use of the ergonomic measures can be regarded as fairly low. Based on the results of the present study, a biannual national information campaign aimed at increasing the use of ergonomic measures may be sufficient to raise awareness but needs to be complemented by additional strategies involving the employers to actually reduce the risks for MSDs and eventually MSDs itself.
4.3. Acknowledgment of limitations
Some limitations regarding the representativeness of the workers who participated in this study must be noted. First, the response rate was fairly low, but comparable to the response rate reported in other questionnaire surveys among construction workers [15,16]. The nonresponse bias is not measured in this study, but it seems unlikely that workers who increased or decreased their use selectively dropped out. By contrast, it cannot be ruled out that the workers who increased their use felt more involved with the study and that we overestimated the proportion of workers who increased their use.
Second, bias might have occurred by a lack of knowledge about the actual exposure. We did not study a change in physical demands through observation, and therefore got no insight into the pathway between an actual reduction of exposure and a reduction of MSDs. To obtain information on physical exposures, a self-reported physical exposure would not be robust enough to examine changes [17]. Furthermore, the potential efficacy of the chosen intervention was unknown. In our study, however, ergonomic measures were selected based on current best practices according to employers and employees regarding their potential to decrease adverse physical work demands.
Bias might also have occurred due to recall bias, but is unlikely in our opinion. Because we asked about the current use of ergonomic measures, no recall bias will affect those figures. Furthermore, we examined changes in individuals' MSDs. Recall bias is not likely to change from one measurement point to the other, and the direction of bias is probably random and unpredictable. Because the results were based on a comparison of two periods of the same recall interval, there is no reason to expect a systematic recall error in estimation of change in MSD prevalence.
Third, our results might have been affected by confounding. The higher age of the respondents might have affected the progress of MSDs, as the likelihood of having MSDs rises with increasing age [16]. In an aging population, no change in MSDs might actually be a positive effect, as an increase in MSDs is expected in an aging population. We verified whether the presence or absence of MSDs at baseline might have affected the follow-up response, but we did not find an indication for this. Our follow-up data are therefore not likely to be contaminated by a selection process. Next, various other physical, psychosocial, and individual risk factors (sex, height, medical conditions, and sports activities) for MSDs could have affected the occurrence of MSDs. All MSDs are multifactorial in origin and the relative contributions of these covariates may be specific to particular disorders. In some countries, it could be possible for different trades to have different socioeconomic identities, affecting both their likelihood for developing MSDs and their access to ergonomic interventions. In our opinion, this is not the case in The Netherlands for the trades in the present study and we decided not to include socioeconomic identity as a confounder or effect modifier in the present study.
A fourth limitation includes our study design: our study did not include a control group and we should therefore be careful in attributing changes in behavior and MSDs to the campaign. Other factors might have played a role as well. For example, in some of the occupations, a high proportion of workers (e.g., 60% of the pavers) indicated that the use of ergonomic measures was legally obliged. In addition, an increase in the availability or decrease in the selling price of ergonomic equipment is likely to have an effect on the use of the measures anyhow. Furthermore, a substantial number of workers reported having decreased their use of ergonomic measures over the 2-year period. It is likely that the main barrier mentioned by the workers, that is, the unavailability of the ergonomic equipment, possibly as a result of constraints due to varying working sites, plays an important role in this phenomenon.
Last, our study did not include the employers and it remains unknown if and to what extent they were reached by the campaign and how they facilitated the use of ergonomic measures. It is likely that due to difficult economic circumstances, the purchase of ergonomic equipment by the employer was restricted, consequently limiting the availability of the related ergonomic equipment for the workers.
4.4. Summary and recommendation
Over a 2-year period in which a national campaign was carried out, we did not find an increase in the use of ergonomic measures, except for vertical transport. Furthermore, in particular, the bricklayers, reinforcing iron and rebar workers, and drywall and ceiling tile installers increased their use of ergonomic measures. We found no relationship between an increase in the use of ergonomic measures and a decrease of complaints of the lower back, knees, or shoulders.
Because sufficient awareness of ergonomic measures is a prerequisite for using them, the national campaign added positively to the steps needed to improve physical working conditions for construction workers. Strategies aimed at improving the availability of ergonomic equipment complemented with individualized advice and training in using them might be the required next steps to increase the use of ergonomic measures.
Conflicts of interest
We have no potential conflicts of interest to disclose.
Acknowledgments
This study is financially supported by Arbouw, Dutch Health & Safety Institute, 10-008 in the Construction Industry. We thank Berry van Holland M.Sc. for collecting the baseline data. We thank the reviewers for their feedback and suggestion for improvement of this paper.
Footnotes
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
- 1.American Academy of Orthopaedic Surgeons . 1st ed. American Academy of Orthopaedic Surgeons; Rosemont (IL): 2008. The burden of musculoskeletal diseases in the United States: prevalence, societal and economic cost. 247 p. [Google Scholar]
- 2.Stattin M., Järvholm B. Occupation, work environment, and disability pension: a prospective study of construction workers. Scand J Public Health. 2005;33:84–90. doi: 10.1080/14034940410019208. [DOI] [PubMed] [Google Scholar]
- 3.The Center for Construction Research and Training (CPWR) 5th ed. CPWR; Silver Spring (MD): 2013. The Construction Chart Book; p. 34.http://www.cpwr.com/publications/chart-book-hazards-and-exposures Available from: [Google Scholar]
- 4.Schneider S.P. Musculoskeletal injuries in construction: a review of the literature. Appl Occup Environ Hyg. 2001;16:1056–1064. doi: 10.1080/104732201753214161. [DOI] [PubMed] [Google Scholar]
- 5.Jaffar N., Abdul-Tharim A.H., Mohd-Kamar I.F., Lop N.S. A literature review of ergonomics risk factors in construction industry. Procedia Eng. 2011;20:89–97. [Google Scholar]
- 6.van der Molen H.F., Sluiter J.K., Hulshof C.T., Vink P., Frings-Dresen M.H. Effectiveness of measures and implementation strategies in reducing physical work demands due to manual handling at work. Scand J Work Environ Health. 2005;31:75–87. [PubMed] [Google Scholar]
- 7.Dale A.M., Jaegers L., Buchholz B., Welch L., Evanoff B.A. Using process evaluation to determine effectiveness of participatory ergonomics training interventions in construction. Work. 2012;41:3824–3826. doi: 10.3233/WOR-2012-0684-3824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kramer D.M., Bigelow P.L., Carlan N., Wells R.P., Garritano E., Vi P., Plawinski M. Searching for needles in a haystack: identifying innovations to prevent MSDs in the construction sector. Appl Ergon. 2010;41:577–584. doi: 10.1016/j.apergo.2009.12.003. [DOI] [PubMed] [Google Scholar]
- 9.van der Molen H.F., Sluiter J.K., Frings-Dresen M.H. The use of ergonomic measures and musculoskeletal complaints among carpenters and pavers in a 4.5-year follow-up study. Ergonomics. 2009;52:954–963. doi: 10.1080/00140130902763560. [DOI] [PubMed] [Google Scholar]
- 10.van der Molen H.F., Frings-Dresen M.H., Sluiter J.K. The longitudinal relationship between the use of ergonomic measures and the incidence of low back complaints. Am J Ind Med. 2010;53:635–640. doi: 10.1002/ajim.20830. [DOI] [PubMed] [Google Scholar]
- 11.Sauro J., Lewis J.R. Estimating completion rates from small samples using binomial confidence intervals: comparisons and recommendations. Proc Hum Fact Ergon Soc Annu Meet. 2005;49:2100–2103. [Google Scholar]
- 12.Visser S., van der Molen H.F., Sluiter J.K., Frings-Dresen M.H. Guidance strategies for a participatory ergonomic intervention to increase the use of ergonomic measures of workers in construction companies: a study design of a randomised trial. BMC Musculoskelet Disord. 2014;15:132–142. doi: 10.1186/1471-2474-15-132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Fletcher R.H., Fletcher S.W. 4th ed. Lippincott Williams & Wilkins; Baltimore (MD): 2005. Clinical epidemiology: the essentials. 288 p. [Google Scholar]
- 14.Faber G.S., Kingma I., van Dieën J.H. The effects of ergonomic interventions on low back moments are attenuated by changes in lifting behaviour. Ergonomics. 2007;50:1377–1391. doi: 10.1080/00140130701324622. [DOI] [PubMed] [Google Scholar]
- 15.Boschman J.S., van der Molen H.F., Frings-Dresen M.H.W., Sluiter J.K. Response rate of bricklayers and supervisors on an internet or a paper-and-pencil questionnaire. Int J Ind Ergon. 2012;42:178–182. [Google Scholar]
- 16.Boschman J.S., van der Molen H.F., Sluiter J.K., Frings-Dresen M.H. Musculoskeletal disorders among construction workers: a one-year follow-up study. BMC Musculoskelet Disord. 2012;13:196–205. doi: 10.1186/1471-2474-13-196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.van der Beek A.J., Frings-Dresen M.H. Assessment of mechanical exposure in ergonomic epidemiology. Occup Environ Med. 1998;55:291–299. doi: 10.1136/oem.55.5.291. [DOI] [PMC free article] [PubMed] [Google Scholar]