

Abstract
Early adolescence (ages 10–14 years) is among the most neglected stages of development, yet there are few stages during the life course where changes are as dramatic. The present conceptual framework proposes four central goals to be achieved by early adolescence: engagement with learning, emotional and physical safety, positive sense of self/self-efficacy, acquisition of life/decision-making skills. The framework proposes an ecological model where the macro level factors (economic forces, historical events, national priorities, laws/policies/norms and values, national events, and political realities) all set the contexts that influence community, family, school and peer factors that all in turn influence the adolescent. Existing indicators for points of development are noted as are future areas of research priority.
Keywords: adolescence, conceptual framework, early adolescence, very young adolescence
Introduction
Adolescence is frequently divided into three stages: early, middle, and late. The ages from 10 to 14 years – referred to here as early adolescence – are marked by dramatic physical, cognitive, and social changes; however, researchers view it as among the most neglected periods of life (1). Across these 5 years, a young person physically develops, progressing from a prepubescent youngster with childlike features to someone with an adult appearance. So too, this period is marked by social and cognitive shifts that set the stage for lifelong capacities and aspirations. Social relationships often expand beyond the family unit to include more peer group influences; and young people begin to acquire behaviors that have a profound impact on later life. In many societies, these years encompass a major educational shift from primary to secondary school or, conversely, to early school leaving, employment in the formal or informal sectors, and perhaps early marriage. In this paper, we propose a conceptual framework that is intended to guide future research, policy, and programming for young people as they make the transition into adolescence.
There is a set of premises that guide our work. First, while human development occurs from birth to death, there are key transition points when development is progressing at such a fast pace that development itself becomes a central component of health. Early adolescence is one such transition. Second, although less visible than pubertal maturation, this age period is marked by equally profound brain development that fundamentally alters how young people think and engage the world (2–5). Third, this work rests on the assumption that healthy development has as one component empowerment rather than acquiescence and decision-making capacity rather than compliance. Fourth and finally, it rests on the assumption that equity is a component of a healthy society and that the formation of gender norms among early adolescents is important to understand because gender differentiation is a central component of adolescent development that will enhance or subvert equity. Thus, fundamentally, what we are proposing is a rights framework for healthy development of the early adolescent.
Why focus on early adolescence?
The present paper responds to a call for a conceptual framework for early adolescence by the World Health Organization (WHO). Specifically, a technical working group convened by the WHO on November 4–5, 2010 said: “Older adolescents aged 15–19 have drawn the lion’s share of attention, while the special needs and concerns of younger adolescents aged 10–14 – some of whom are already sexually active – have been relatively neglected”. The Technical Consultation was intended to identify and help fill the gaps in research, programming, and policy making for girls and boys aged 10–14 years in developing countries. The Consultation called upon the WHO to identify and assess existing conceptual frameworks empirically for researching sexual and reproductive health issues, as well as asset building factors for adolescents and suggest others, based on new evidence.
Over the past century, the age of menarche, a marker of adolescence, has declined throughout Europe and North America, and recently similar shifts have also been reported in low- and middle-income countries (LMICs) (6–9). At a national level, there is an inverse relationship between the age of menarche and the average life expectancy (10). In addition to reflecting improved health and nutritional status, however, these downward trends also present new challenges. Paralleling the decline in the age of menarche has been a younger age of sexual debut of young people in some parts of Africa (11) and Latin America (12). Early sexual initiation for girls – especially if it results in early childbearing – can undermine the accomplishment of a central development goal of many LMICs, namely, universal primary education. Today, more than half of all countries in the world mandate education through the age of 14 years (13), and since 1991, worldwide rates of secondary school enrollment for girls increased from 44% to 58% (14, 15).
In summary, the simultaneous worldwide increase in school enrollment during early adolescence and the challenge to educational attainment posed by the increasing potential for a very early sexual debut brings the early adolescent phase of life into sharp focus (6).
Early adolescent health: a brief snapshot
In 2009, Patton and colleagues analyzed worldwide mortality data by age. They found that the overall infectious disease mortality rate for males 10–14 years of age is approximately 20 per 100,000 and the rate for females was 28 per 100,000. The major etiologies include: lower respiratory tract infections, meningitis, tuberculosis, and HIV/AIDS. For chronic disease mortality the rates are lower among adolescents (approx. 15 per 100,000) for both sexes than for their younger and older peers, with the major causes of death in this age group including cancer, cardiovascular disease, epilepsy, and other neuropsychiatric conditions. For injury mortality among young adolescents, the rate is approximately 22 per 100,000 for young men and 18 per 100,000 for young women with the primary causes of death including vehicular injury, drowning, and violence (16).
With respect to morbidity, recent analysis by Gore and her colleagues (17) sheds light on the global burden of disease as well as major threats to young adolescents’ health. For 10 to 14 year olds, non-communicable diseases predominate with the major risk factors contributing to disease burden including alcohol, unsafe sex, iron deficiency, unsafe water, sanitation and hygiene, unsafe healthcare injections, and high blood glucose. Although there is little variation in total prevalence of health compromising factors across regions of the world, there is substantial variation in the causes of morbidity (see, e.g., the comparisons between Europe and Southeast Asia; Figure 1)
Figure 1.
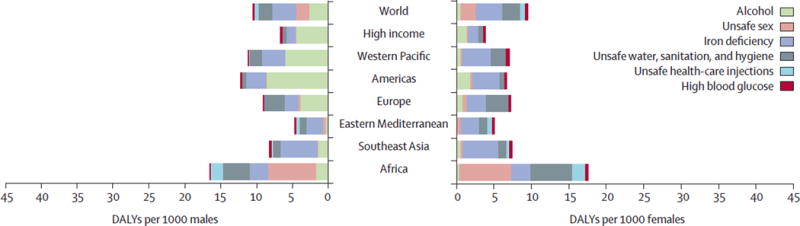
Risk factors that contribute to years of life lost (YLL) and years of life with disability (YLD) for 10 to 14 year olds measured in disability-adjusted life years (DALYs) by region and sex. Source: Gore et al. (17).
Behavior is a central aspect of adolescent health. Many behaviors that are known to cause non-communicable disease later in life begin in adolescence, and thus adolescence appears to be a window of opportunity for prevention of these diseases (17). The quality of the data on health behavior in early adolescence is highly variable. From the Global Youth Tobacco Survey, which has been conducted in over 100 countries since 1999, we can reliably estimate that approximately 10% of young people aged 13 to 15 years smoke cigarettes with the gender gap narrowing in many regions of the world (18). Data on sexual initiation are less reliable. The estimates of sexual debut before the age of 15 years for both sexes are: East/Southern Africa, 14%; West/Middle Africa, 17%; Caribbean/Central America, 31%; South America, 31% (19). Although there is little difference between male and female sexual behavior before the age of 15 years in Africa, there is a significantly higher proportion of young male adolescents in the Caribbean and Central and South America who are engaged in early sexual intercourse (19).
The health risks associated with early sexual initiation and pregnancy are heightened if they occur in early adolescence. The maternal mortality risk for mothers under 15 years is double that of older women, and in addition they face significantly higher rates of obstetrical fistulae than their older peers (19). Unintended pregnancies are also associated with early age of sexual initiation, as Lule and her colleagues (19) note: “about 1 in 7 young women in West and Middle Africa and about 7% to 9% in Central America and the Caribbean, as well as South East Asia, have a child before the age of 16”.
Although there is a growing body of data that indicate the behavioral factors that compromise early adolescent health, significantly less is known about the risk and protective factors that contribute to or impede healthy development. Such is the focus of the present conceptual framework.
A conceptual framework for early adolescence
The following is both a multilevel and life course framework for early adolescent health and development. The factors shown are highly interrelated but do not completely coincide. So for example, we know that a caring and committed adult can buffer a young person who grows up in a violent and abusive environment from its consequences. Conversely, those who grow up with many of the protective advantages of education and financial resources can be derailed by peer or neighborhood influences. The model first identifies the major domains wherein young adolescents develop, then it delineates aspects of those domains that are protective and those that can leave adolescents vulnerable. Although we propose these factors as risk or protective, we are fully aware that what is protective in one cultural context or environment (e.g., behavioral monitoring) may be impeding of healthy development in another.
We propose four central goals for young people to reach at the completion of early adolescence. Based on an extensive review of the international literature coupled with soliciting the input of nearly 50 global experts in adolescent health and development, these are the building blocks of healthy development (20–22), and when in place each is associated with later onset of sexual debut, improved contraceptive utilization, diminished risk of sexual infections, and improved social, educational, and behavioral outcomes:
engagement with learning,
emotional and physical safety,
positive sense of self/self-efficacy,
acquisition of life/decision-making skills.
There are many factors that facilitate the attainment of these goals including: intrinsic factors (physical and mental health, the ability to self-regulate) and extrinsic factors (gender equity, academic or apprenticeship opportunities, access to human and institutional resources, security, high expectations for achievement from teachers and care providers, and behavioral monitoring) (Figure 2).
Figure 2.
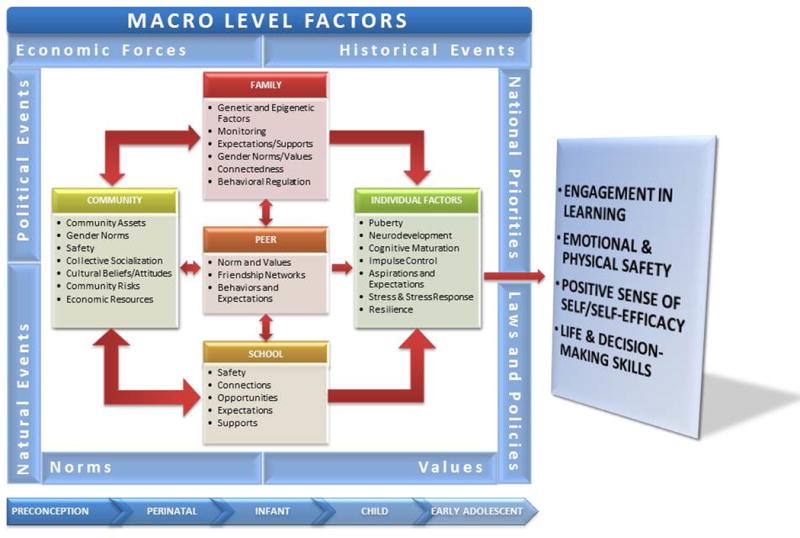
A conceptual framework for healthy early adolescence.
Macro-level factors that impact early adolescent health and development
National and global forces shape adolescent health both directly and indirectly. Historical events such as the tsunami in Japan in 2011 or Hurricane Katrina in New Orleans in 2005 indirectly affect adolescent health through impacting the other contextual domains of neighborhood, school, and family. So too, macro-level factors may directly impact youth. For example, laws in one country (e.g., US protectionist tariffs on imported catfish) may impact the livelihoods of young workers halfway across the globe in Vietnam (23).
Political and civil societies
Through economic, agricultural, and educational policies, national governments distribute available resources, and allocation distribution has a profound impact on young people. When the national political context is unstable, the impact on families, schools, and communities is direct and profound. The most extreme example is civil strife and war. The conscription of early adolescents into civil conflicts has been well described in Mozambique (24), Uganda (25), Sierra Leone (26), and Somalia (27). But even when civil strife does not result in war, the disruptions to the social fabric interrupt healthy development.
Conversely, national policies and laws may also have effects that promote adolescent development and health. A minimum age for marriage, child labor laws, compulsory schooling, laws promoting young people’s access to reproductive health services, restrictions on tobacco and alcohol, graduated drivers’ licenses are all examples of such protective macro-level factors.
Economy
Education and economic opportunity are closely intertwined, and the returns on education are a key factor in motivating young people for educational achievement. In addition, when domestic economic opportunities are limited it is not uncommon for one parent to immigrate for employment providing financial resources to her or his family, but denying children the supports of a nurturing parent (28). Likewise, in a number of African communities where schools may not exist beyond the sixth grade, young adolescents may be sent to larger communities for more schooling, which has educational benefits while concurrently increasing her or his vulnerability and depriving the young person of parental support (29, 30).
Systemic inequity, including gender inequality
In addition to the larger political and economic context, many nations are characterized by systemic inequality of social class, ethnicity, sexual orientation, immigration status, and/or gender. Early adolescent girls experience increased vulnerabilities in many settings due to restricted access to community resources, such as healthcare (31), education (32), increased physical and sexual vulnerability, which can include holding them accountable for sexual assaults they may experience (33–35), subservient social status, and early marriage (36). Systematic inequalities are most pernicious when they become internalized and the group discriminated against perceive themselves as unworthy (6).
Neighborhood/community
The empirical evidence for the association between neighborhood poverty and juvenile violence goes back at least to the 1940s (37). So too, Crane et al. (38) demonstrated that there were relationships between the percent of people in a neighborhood employed and both early school leaving and teen pregnancy. Additionally, there have been a host of US based surveys (and few from elsewhere) that have consistently found relationships between adolescent sexual behavior and neighborhoods in which young people live (39–41). This may be particularly true for infectious disease. Jennings and colleagues (42) recently demonstrated that neighborhood is an independent risk factor for sexually transmitted infections controlling for behavior. Others have shown similar relationships between neighborhood and adolescent mental health (43), substance use (42), and school achievement (44–46).
In addition, the interaction between neighborhoods and families are particularly important to note. For example, Browning et al. (47) found that collective efficacy – defined as the ability of a community to “mobilize on behalf of shared goals” – delayed sexual initiation, particularly among individuals who experienced low levels of parental monitoring. This suggests that young adolescents need a certain amount of monitoring, and when parents will not or cannot provide it, other adults can step forward in their place. Therefore, individuals with low levels of parental monitoring and community supervision are at a particularly greater risk of early sexual initiation as well as violence. Addressing both the community and family levels, and understanding the interaction of the two, is necessary in implementing effective policies and programs.
The family
The family is the central context in which most human development occurs. In the early part of the life course, the family in question is usually one’s parents (or caretakers) and siblings. As it relates to early adolescence, Barber et al. (48) identified three core parental behaviors: connection, encouraging autonomy (e.g., respect for the individual), and behavioral regulation. They went on to show that in 12 countries where it was studied psychological regulation or control (often manifested as abusive/manipulative behavior on the part of parents) exacerbated behavior problems of young people as did lack of respect for individuality.
In Ecuador, low family cohesion and exclusion from family decision making were associated with significantly higher adolescent pregnancy risk (49). So too, among young adolescents in Brazil, early sexual initiation was much lower among both male and female adolescents with positive family relationships, as was smoking, drug use, and suicidal thoughts and attempts (50). Similar findings have been seen in the Caribbean among adolescents of both sexes with regard to early sexual debut, violence, regular alcohol use, and cigarette smoking (51). Most recently, the protective role of the family has been seen once again in Hanoi, Shanghai, and Taipei (52) with findings suggesting that parental support and closeness are protective against suicidal ideation and attempts.
The centrality of parental connectedness was further underscored in a four-country (USA, China, Korea, and Czech Republic) study by Dmitrieva et al. (53) where they found parental connectedness and involvement to be key mediators between family life events and adolescent depression; and likewise, they found little cultural variation across countries. In Sub-Saharan Africa, Crichton and Theobald (54) reported that parent-child communication, especially about sexual and reproductive issues, is uncommon. The same researchers found that young adolescent girls wanted parental communication to begin early and to be continuous.
Finally, using a national US sample, Roche and colleagues explored the cause and effects of parental closeness and behavioral regulation during early adolescence on educational attainment and sexual behavior among young adults 7 years later (55). Specifically, using a cohort of 12 to 14 year olds from the National Longitudinal Study of Adolescent Health (Add Health Study), the authors examined family closeness and parental behavioral control at the ages of 12 to 14 years and then explored school leaving and multiple sexual partners 7 years later (at the ages of 18 to 22 years). For early school leaving, parental monitoring at the age of 12 to 14 years had little impact; however, parental closeness impacted skipping school in middle adolescence, which in turn impacted early school leaving over the subsequent 7 years for both males and females. For having reported multiple sexual partners by the ages of 18 to 22 years, parental monitoring of young adolescent males had a significant behavioral impact over the next 7 years but for females it was parental closeness that was the key influence on age of sexual debut and whether they reported having had multiple sexual partners 7 years later. Parental closeness had no similar effect for males.
In summary, parenting behaviors during early adolescence have different consequences for different behaviors and the impact varies by gender. The evidence, however, is clear that for early adolescents, parental connectedness and behavioral regulation with its concomitant communication of expectations are critical elements for healthy transitions to middle adolescence and beyond.
It is not clear how the effects of parental connectedness, behavioral regulation, and monitoring vary by characteristics of families or social context. These are critical areas for future research because families are changing dramatically. Specifically, family size is shrinking globally and the effects of smaller size on family functioning and supports have yet to be fully understood. Likewise, increasingly families are leaving their rural roots for urban residence (56). This has profound effects on young adolescents because family members living apart often accompanies urban relocation. Although the majority (66%) live with two biological parents, 27% of 12–14 year old girls in two informal settlements of Nairobi lived with one or no parents (57, 58). Additionally, traditional parenting practices and strategies for dealing with the transition to adolescence that worked well in rural contexts, where young people were embedded in close knit networks of relatives and neighbors may not be optimal for parents who live in cities. The close knit nature of many rural communities may allow parents to depend on neighbors to watch out for their young adolescents. Parents who move to the city may need to be much more proactive in supervising their adolescents and devise monitoring strategies that will be compatible with urban work realities and less safe neighborhoods.
Schools
Second only to family, schools have been repeatedly shown to be the most significant context in the lives of young people. The World Bank, for example, has shown that for every year a young woman remains in school after age 11 years the risk of unplanned pregnancy declines by 7% for women with at least a primary education, and 6% for women with a secondary degree (59). School enrollment is associated with a later age of marriage, better contraceptive utilization, and greater access to health information. In the 2009 Survey Assessment of Vietnamese Youth (SAVY 2), Loi (60) found higher education to be associated with lower levels of every health risk behavior studied. So too, in the US Add Health Study, Resnick et al. (61) found that young people who reported being connected to school were less likely to smoke cigarettes, use alcohol or marijuana, report depression or suicidal thoughts, engage in violent behavior or report ever having become pregnant. In many LMICs, however, young female adolescents are up to ten times less likely than their male counterparts to be enrolled in school (62).
In a study on enhancing school engagement, the US National Academy of Sciences (63) identified a triad of key factors: (i) interpersonal connection with school staff and peers; (ii) an engaging environment that is physically, environmentally, and academically safe; and (iii) an environment that couples high academic expectations with high support and relevant instruction.
Although there have yet to be extensive studies on the links between school connectedness and health behaviors, research from the USA is suggestive of a strong relationship. Specifically, exploring the transitions into health compromising behaviors over a year-long period of time, McNeely and Falci (64) studied the relationship of perceived teacher support to the onset of a range of behaviors. They found for cigarette smoking 5.3% of the national sample transitioned from being non-smokers to regular smokers over that year when teacher support was seen as low, compared with 2.8% when it was high. For transitioning from no to regular heavy drinking, it was 6.3% when teacher connection was low compared with 3.2% when it was high. The researchers found that 4.2% of the national sample reported transitioning from no to regular marijuana use when teacher support was low, compared with 2.6% when it was high. And thus for all behaviors where teacher support was seen as high, young people were between 50% and 100% less likely to engage in any of the risk behaviors studied. If these US data are generalizable, teacher and presumably other adult support in school is one of the keys to enhancing school engagement.
In LMIC settings, schools have also demonstrated protective effects on young people’s health provided that they have adequate support. For example, a randomized controlled trial conducted in Kenya implemented an intervention for comprehensive educational support (i.e., school fees, uniforms, community visitor to monitor attendance, etc.) among orphans, and monitored their school attendance and health behaviors over time (65). The researchers found that providing comprehensive educational support not only lowered school absenteeism and dropout but it also had promise to delay sexual initiation and other risk factors associated with HIV. Similar findings by Lloyd (66) have reinforced the value of educating adolescent girls with a priority to focus on those in the early adolescent years.
Synthesizing the literature we see four core school factors as key to early adolescent development and health:
physical, emotional, and academic safety;
high academic expectations coupled with supports;
connectedness with adults in the school;
opportunities for social engagement.
Academic safety is the safety in school to be right or wrong in response to teacher questions without fear of peer or educator humiliation or recrimination (Figure 3).
Figure 3.
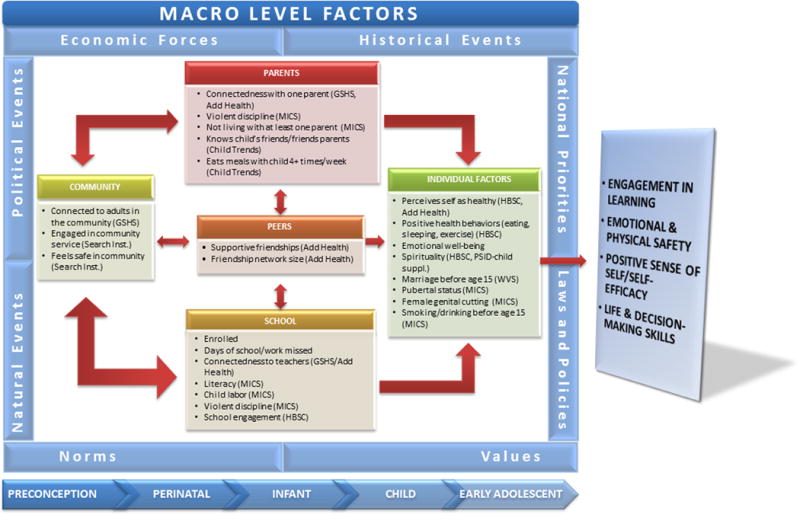
Potential indicators of early adolescent healthy development. Abbreviations: GSHS, Global School Health Survey; Search Inst., Assets Assessment of Search Institute, Minneapolis, MN.; Add Health, National Longitudinal Study of Adolescent Health; MICS, Multiple Indicator Cluster Survey (UNICEF); HBSC, Health Behavior of School-age Children; PSSID, ; WVS, World Values Survey.
Indicators of achieving healthy early adolescence
The indicators below are keyed to the primary domains of influence in the lives of young adolescents described above. They are derived from existing national and global surveys. They are not indicators of the four core outcomes of healthy early adolescent development; rather, they measure the factors that are the preconditions for healthy development. As will be seen subsequently there are a number of limitations in these measures and additionally there are a number of elements in the conceptual framework that are not captured here. Implementing these measures for the 10–14 year olds would allow for a richer understanding of the health and healthy development of early adolescents than currently exists.
Limitations of existing measures for early adolescents
The problems with the indicators available from existing systems are several. Globally, much of what is known about health on a population level is derived from national systems such as the Demographic and Health Survey (DHS) and Multiple Indicator Cluster Survey (MICS). These large-scale, nationally representative systems always sample women, but survey men more sporadically, and sometimes the male respondents are fewer in number and abbreviated instruments are used. Another problem is a tendency towards a focus on a narrow set of health issues, most notably reproductive health. This is a limitation when applied to early adolescents.
Additionally, the samples are often limited to older adolescents. There are also other limitations of these data. Even among women of reproductive age and within the field of reproductive health, the data generated through these systems focus on health outcomes with fewer measures of risk and protective factors across levels. Although public health has shifted from a focus on identifying negative outcomes to a broader conceptualization of health that is influenced by both risk and protective factors, the inclusion of indicators of protective factors on these surveillance systems lags behind.
An exception is the Health Behavior in School-Aged Children (HBSC), which is an international, school-based survey conducted in over 40 countries around the world, and samples youth ages 11–15 years. Similar to DHS and MICS, the HBSC is heavily focused on health outcomes (e.g., including substance use, sexual risk, nutrition, sedentary behavior, and bullying), enabling much-needed surveillance. Although not the focus of this paper, it also provides a starting point for understanding risk and protective factors spanning individual, family, and school-level protective factors, however, including assessments of individual academic achievement, life satisfaction, family poverty, parent connectedness, parental monitoring, presence of close male and female friends, and school connectedness.
Another global surveillance system that can inform early adolescent health is the Global School Health Survey (GSHS). The GSHS is also an international, school-based survey that samples youth primarily ages 13–15 years of age. The GSHS is similarly outcomes-oriented, although it includes risk and protective factors spanning individual, family, and school-level protective factors, including assessments of anger management education, stress management, mental health, parental alcohol use, parental closeness, parental monitoring, school connectedness, and school hygiene and safety. Although both the HBSC and the GSHS are valuable, it should be noted that the existing surveillance systems for early adolescence (HBSC and GSHS) are school-based, limiting our understanding of health and development among the most vulnerable youth.
In summary, advancing the global knowledge base of early adolescent health and development requires not only including this age population within existing surveillance systems but also adopting and evaluating measures that assess risk and protective factors. That said, interventions targeted to early adolescents may benefit from including existing measures for many of the risk and protective factors described in the model within ongoing program evaluation as well as local surveillance and needs assessment efforts.
Future research areas
To continue to build on the advances offered by the currently proposed model, a number of additional research steps are required in the years ahead (67). An important next step in the study of early adolescence is the development and refinement of a set of valid indicators and a monitoring system to evaluate and assess the health of this population. Specifically, cross-nationally and cross-culturally valid indicators are needed. Based on the conceptual model, priorities should be given to academic engagement, perceived emotional and physical safety, self-efficacy, life and decision-making skills, and physical/mental health. So too, priority should be given to identifying those protective factors which when in place moderate or mitigate social and environmental risks. There is a need to understand cultural and geographical variations of such factors, as well as the ways in which they vary by gender. Because the early adolescent period is an under-researched age group, there is a lack of a set of tools to comprehensively assess and monitor this population (68).
Second, the conceptual framework presented identifies a key set of outcomes for early adolescence: engagement in learning, emotional and physical safety, positive sense of self/self-efficacy, and life and decision-making skills. If in place by the age of 15 years, these four early adolescent outcomes will shape the life-long developmental trajectory and health of individuals including their decision-making capacity, academic achievement, life skills, civic engagement, social skills, opportunities for exploration, and resilience, as well as physical and emotional health. Although there are certainly other domains and outcomes of interest, these serve as a starting point to begin to conceptualize and monitor the health of young adolescents.
Third, life course principles suggest that it is an imperative to continue assessing individuals over time; therefore, indicators should be malleable to changing contexts and experiences. Scales to monitor certain childhood behaviors, such as social competence, have been validated in the USA and Western settings (69), but the extent to which indicators may be used across settings and countries need to be further explored, with particular needs in developing settings. Similarly, the Child Trends DataBank provides indicators on six main categories across childhood to early adulthood including health, social and emotional well-being, assets, work, education, and skills, demographics, and family and community (68). These domains are generalizable across settings, and there is a need for population level indicators that can be applied to multiple contexts and populations. In addition, pubertal maturation is grounded in biological underpinnings, yet the social consequences have been poorly researched. The issue is all the more compelling as the age of puberty is declining in many LMICs.
Fourth, although still highly prevalent in many countries, it appears that child marriage is declining (70) and education attainment is increasing, especially among adolescent females (13), the changing cultural norms, gender expectations, and power dynamics will directly influence early adolescent females and there is a need to understand the processes of social change and how they impact young adolescents.
Lastly, although adolescence has primarily been conceptualized as a risk-prone time period, there is growing recognition that positive development and protective factors should also be emphasized (71–73). The conceptual framework presented here specifically highlights the balance between vulnerability and protection in a young person’s life and, consequently, indicators should span both measures of risk and protective factors.
The value of focusing on early adolescence is clear. The proposed conceptual model should provide meaningful direction for programmatic and policy approaches that seek to bolster positive youth development. In doing so, we will not only achieve health among early adolescents but we will also protect adolescents against subsequent threats to health and well-being in late adolescence, early adulthood, and beyond.
Conclusion
Despite the significance of early adolescence in shaping later adolescent and early adulthood outcomes and behaviors, there currently exists a dearth of research and focus on early adolescence. Using the existing evidence base, this paper presents a working conceptual framework to guide future research as well as programmatic and policy efforts for this critical population. Although the specific content of many of the domains our framework will exhibit regional and contextual variation, the overwhelming consistency of findings regarding the general dimensions of the model, as well as the mechanisms that underpin it strongly suggests its utility for application across a wide range of settings. This empirically and theoretically informed conceptual model should therefore serve as a tool for individual policymakers and interventionists, as well as those setting regional and global priorities and agendas. By harnessing consistent evidence from a variety of settings, it provides a starting point for policy and programmatic guidance, even in settings where very little is known.
The advantages and applications of a shared understanding of the early adolescent underpinnings of physical, mental, and sexual/reproductive health are many. As the programmatic and policy infrastructure advances in the area of early adolescence, conceptual consistency across geographical settings will provide a basis for collection of comparable data so as to support cross-regional comparisons. Harnessing this comparability will, in turn, allow the research base to advance synergistically.
The framework should play a vital role in guiding priorities for intervention. Applying the schema to existing conditions can allow for easy identification in gaps in services, missing links, and high-risk groups most in need of assistance. Where time and resources allow, the framework can guide the development of rapid surveillance efforts to quantify missing links and unmet needs in a given setting or population.
The framework should also provide concrete direction for intervention and evaluation efforts. By illustrating the interrelationships among components, the model provides a basis for understanding the long-term impact of interventions designed to modify early stage influences. Thus, early adolescent interventions designed to buffer against specific risks illustrated in the model may be considered to have an impact on more distal outcomes, such as late adolescent sexual and reproductive health, even if the follow-up time for a given intervention is not sufficiently long so as to actually witness changes in these outcomes. For example, the work of Roche and colleagues (55) found that parental closeness and behavioral monitoring at ages 12–14 years were associated with fewer sexual partners and later age of sexual debut at ages 19–21 years. The time lag between early adolescent experiences and later adolescent or early adulthood outcomes and behaviors may be very lengthy, thus a conceptual model should serve as a powerful tool in articulating the steps on the pathway to success in promoting youth health.
Acknowledgments
The authors wish to acknowledge the work of May Sudhinaraset PhD and Farah Qureshi MHS in assisting with background research, Deenah Darom for assistance with manuscript preparation, Shyam Thapa PhD for his encouragement, and the numerous colleagues from around the world who have read multiple drafts of the manuscript and have provided invaluable feedback and numerous suggestions. This work was supported in part through a contract with The World Health Organization.
References
- 1.Richter L, Norris S, De Wet T. Transition from birth to ten to birth to twenty: the South African cohort reaches 13 years of age. Paediatr Perinat Epidemiol. 2004;18(4):290–301. doi: 10.1111/j.1365-3016.2004.00572.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Spear LP. The behavioral neuroscience of adolescence. New York: Norton; 2010. [Google Scholar]
- 3.Casey BJ, Giedd JN, Thomas KM. Structural and functional brain development and its relation to cognitive development. Biol Psychol. 2000;54(1–3):241–57. doi: 10.1016/s0301-0511(00)00058-2. [DOI] [PubMed] [Google Scholar]
- 4.Giedd JN, Blumenthal J, Jeffries NO, et al. Brain development during childhood and adolescence: a longitudinal MRI study. Nat Neurosci. 1999;2(10):861–3. doi: 10.1038/13158. [DOI] [PubMed] [Google Scholar]
- 5.Compas BE, Connor-Smith JK, Saltzman H, Thomsen AH, Wadsworth ME. Coping with stress during childhood and adolescence: problems, progress, and potential in theory and research. Psychol Bull. 2001;127(1):87–127. [PubMed] [Google Scholar]
- 6.Jones L, Griffiths P, Norris S, Pettifor J, Cameron N. Age at menarche and the evidence for a positive secular trend in urban South Africa. Am J Hum Biol. 2009;21(1):130–2. doi: 10.1002/ajhb.20836. [DOI] [PubMed] [Google Scholar]
- 7.Prentice S, Fulford AJ, Jarjou LM, Goldberg GR, Prentice A. Evidence for a downward secular trend in age of menarche in a rural Gambian population. Ann Hum Biol. 2010;37(5):717–21. doi: 10.3109/03014461003727606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Opare-Addo PM, Stowe M, Ankobea-Kokroe F, Zheng T. Menarcheal and pubertal development and determining factors among schoolgirls in Kumasi, Ghana. J Obstet Gynaecol. 2012;32(2):159–65. doi: 10.3109/01443615.2011.638092. [DOI] [PubMed] [Google Scholar]
- 9.Singh S, Darroch JE. Adding it up: costs and benefits of contraceptive services – estimates for 2012. New York: Guttmacher Institute and United Nations Population Fund (UNFPA); 2012. Available at: http://www.gurrmacher.org/pubs/AIU-2012-estimates.pdf. [Google Scholar]
- 10.Thomas F, Renaud F, Benefice E, de Meeüs T, Guegan JF. International variability of ages at menarche and menopause: patterns and main determinants. Hum Biol. 2001;73(2):271–90. doi: 10.1353/hub.2001.0029. [DOI] [PubMed] [Google Scholar]
- 11.Mensch B, Grant M, Blanc A. The changing context of sexual initiation in Sub-Saharan Africa. Popul Dev Rev. 2006;32(4):699–727. [Google Scholar]
- 12.Samandari G, Speizer I. Adolescent sexual behavior and reproductive outcomes in Central America: trends over the past two decades. Int Perspect Sex Reprod Health. 2010;36(1):26–35. doi: 10.1363/ipsrh.36.026.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.UNESCO Institute for Statistics. Global education digest 2010: comparing education statistics across the world. Montreal: UNESCO Institute for Statistics; 2010. Available at: http://www.uis.unesco.org/Library/Documents/GED2010EN.pdf. [Google Scholar]
- 14.The World Bank. World data bank: gender statistics 2011. Cited July 1, 2011. Available at: http://databank.worldbank.org/
- 15.United Nations Children’s Fund. Progress for children: a report card on adolescents. New York: United Nations Children’s Fund (UNICEF); 2012. Available at: http://www.unicef.org/media/files/PFC2012Areportcardonadolescents.pdf. [Google Scholar]
- 16.Patton G, Coffey C, Sawyer S, et al. Global patterns of mortality in young people: a systematic analysis of population health data. Lancet. 2009;374(9693):881–92. doi: 10.1016/S0140-6736(09)60741-8. [DOI] [PubMed] [Google Scholar]
- 17.Gore F, Bloem P, Patton G, et al. Global burden of disease in young people aged 10–24 years: a systematic analysis. Lancet. 2011;377(9783):2093–102. doi: 10.1016/S0140-6736(11)60512-6. [DOI] [PubMed] [Google Scholar]
- 18.Warren CW, Jones N, Peruga A, et al. Global youth tobacco surveillance, 2000–2007. MMWR Surveill Summ. 2008;57(1):1–28. [PubMed] [Google Scholar]
- 19.National Research Council. Growing up global: the changing transitions to adulthood in developing countries. Washington, DC: The National Academies Press; 2005. [Google Scholar]
- 20.Konopka G. Requirements for the healthy development of adolescent youth. Adolescence. 1973;18(31):291–316. [Google Scholar]
- 21.Resnick M. Protective factors, resiliency and healthy youth development. Adolesc Med. 2000;11(1):157–65. [PubMed] [Google Scholar]
- 22.McNeely C, Blanchard J. The teen years explained: a guide to healthy adolescent development. Baltimore, MD: Johns Hopkins University; 2009. [Google Scholar]
- 23.Brambilla I, Porto G, Tarozzi A. Adjusting to trade policy: evidence from U.S. antidumping duties on Vietnamese catfish. MIT Press. 2012;94(1):304–19. [Google Scholar]
- 24.Boothby N, Crawford J, Halprin J. Mozambique child soldier life outcome study: lessons learned in rehabilitation and reintegration efforts. Glob Public Health. 2006;1(1):87–107. doi: 10.1080/17441690500324347. [DOI] [PubMed] [Google Scholar]
- 25.McDonnell F, Akallo G. Girl soldier: a story of hope for Northern Uganda’s children. 2007. [Google Scholar]
- 26.Beah I. A long way gone: memoirs of a boy soldier. 2008. [Google Scholar]
- 27.Eggers D. What is the what. Vintage. 2007 [Google Scholar]
- 28.Bakker C, Ellings-Pels M, Reis M. Impact of migration on children in the Caribbean. UNICEF Eastern Caribbean. 2009 [Google Scholar]
- 29.Min-Harris C. Topical review digest: human rights in Sub-Saharan Africa. 2010. Youth migration and poverty in Sub-Saharan Africa: empowering the rural youth; pp. 59–186. [Google Scholar]
- 30.Adepoju A. Issues and recent trends in international migration in Sub-Saharan Africa. Int Soc Sci J. 2000;52(165):383–94. [Google Scholar]
- 31.Goodman E. The role of socioeconomic status gradients in explaining differences in US adolescents’ health. Am J Public Health. 1999;89(10):1522–8. doi: 10.2105/ajph.89.10.1522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Temin M, Levine R. Start with a girl: a new agenda for global health. Washington, DC: Centre for Global Development; 2010. Available at: http://www.cgdev.org/content/publications/detail/1422899/ [Google Scholar]
- 33.Wood K, Maforah F, Jewkes R. He forced me to love him: putting violence on adolescent sexual health agendas. Soc Sci Med. 1998;47(2):233–42. doi: 10.1016/s0277-9536(98)00057-4. [DOI] [PubMed] [Google Scholar]
- 34.Davis RC, Brickman E. Supportive and unsupportive aspects of the behavior of others toward victims of sexual and nonsexual assault. J Interpers Violence. 1996;11:250–62. [Google Scholar]
- 35.Aherns C, Campbell R, Ternier-Thames N, Wasco S, Sefl T. Deciding whom to tell: expectations and outcomes of rape survivors’ first disclosures. Psychol Women Q. 2007;31(1):38–49. [Google Scholar]
- 36.Jain S, Kurz K. New insights on preventing child marriage: a global analysis of factors and programs 2007. Available at: http://www.icrw.ord/files/publications/New-Insights-on-Preventing-Child-Marriage.pdf.
- 37.Shaw C, McKay H. Juvenile delinquency and urban areas. Chicago, IL: University of Chicago Press; 1942. [Google Scholar]
- 38.Crane J, Jencks C, Peterson P, editors. The urban underclass. Washington, DC: The Brooking Institution; 1991. Effects of neighborhoods on dropping out of school and teenage childbearing; pp. 299–320. [Google Scholar]
- 39.Billy JO, Brewster KL, Grady WR. Contextual effects on the sexual behavior of adolescent women. J Marriage Fam. 1994;56:387–404. [Google Scholar]
- 40.Ku L, Sonenstein FL, Pleck JH. Neighborhood, family, and work: influences on the premarital behaviors of adolescent males. Social Forces. 1993;72:479–503. [Google Scholar]
- 41.Browning CR, Burrington LA, Leventhal T, Brooks-Gunn J. Neighborhood structural inequality, collective efficacy, and sexual risk behavior among urban youth. J Health Soc Behav. 2008;49(3):269–85. doi: 10.1177/002214650804900303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Jennings J, Taylor R, Iannacchione V, et al. The available pool of sex partners and risk for a current bacterial sexually transmitted infection. Ann Epidemiol. 2010;20(7):532–8. doi: 10.1016/j.annepidem.2010.03.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Chase-Lansdale LP, Gordon RA. Economic hardship and the development of five- and six-year-olds: neighborhood and regional perspectives. Child Dev. 1996;67:3338–68. [Google Scholar]
- 44.Entwisle B. Putting people into place. Demography. 2007;44(4):687–703. doi: 10.1353/dem.2007.0045. [DOI] [PubMed] [Google Scholar]
- 45.Brooks-Gunn J, Duncan GJ, Klebanov PK, Sealand N. Do neighborhoods influence child and adolescent development? Am J Sociol. 1993;99:353–95. [Google Scholar]
- 46.Alexander K, Entwisle D, Olson L. Lasting consequences of the summer learning gap. Am Sociol Rev. 2007;72:167–80. [Google Scholar]
- 47.Browning CR, Leventhal T, Brooks-Gunn J. Sexual initiation in early adolescence: the nexus of parental and community control. Am Sociol Rev. 2005;70:758–78. [Google Scholar]
- 48.Barber BK, Stolz HE, Olsen JA. Parental support, psychological control, and behavioral control: assessing relevance across time, culture, and method. Monogr Soc Res Child Dev. 2005;70(4):1–137. doi: 10.1111/j.1540-5834.2005.00365.x. [DOI] [PubMed] [Google Scholar]
- 49.Guijarro S, Naranjo J, Padilla M, Gutiérez R, Lammers C, et al. Family risk factors associated with adolescent pregnancy: study of a group of adolescent girls and their families in Ecuador. J Adolesc Health. 1999;25(2):166–72. doi: 10.1016/s1054-139x(99)00020-8. [DOI] [PubMed] [Google Scholar]
- 50.Anteghini M, Fonseca H, Ireland M, Blum RW. Health risk behaviors and associated risk and protective factors among Brazilian adolescents in Santos, Brazil. J Adolesc Health. 2001;28(4):295–302. doi: 10.1016/s1054-139x(00)00197-x. [DOI] [PubMed] [Google Scholar]
- 51.Blum RW, Ireland M. Reducing risk, increasing protective factors: findings from the Caribbean Youth Health Survey. J Adolesc Health. 2004;35(6):493–500. doi: 10.1016/j.jadohealth.2004.01.009. [DOI] [PubMed] [Google Scholar]
- 52.Blum RW, Sudhinaraset M, Emerson M. Youth at risk: suicidal thoughts and attempts in Vietnam, China and Taiwan. J Adolesc Health. 2012;50(3S):S37–44. doi: 10.1016/j.jadohealth.2011.12.006. [DOI] [PubMed] [Google Scholar]
- 53.Dmitrieva J, Chen C, Greenberger E, Gil-Rivas V. Family relationships and adolescent psychosocial outcomes: converging findings from Eastern and Western cultures. J Res Adolesc. 2004;14(4):425–47. [Google Scholar]
- 54.Crichton J, Theobald S. Strategies and tensions in communicating research on sexual and reproductive health, HIV and AIDS: a qualitative study of the experiences of researchers and communications staff. Health Res Policy Syst. 2001;16(9 Suppl 1):S4. doi: 10.1186/1478-4505-9-S1-S4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Roche K, Ahmed S, Blum RW. Enduring consequences of parenting for risky behaviors from adolescence into early adulthood. Soc Sci Med. 2008;66(9):2023–34. doi: 10.1016/j.socscimed.2008.01.009. [DOI] [PubMed] [Google Scholar]
- 56.United Nations Human Settlements Programme. State of the world’s cities 2008/2009: harmonious cities. Nairobi: UN-HABITAT; 2008. Available at: http://www.unhabitat.org/content.asp?catid=7&cid=5964&subMenuId=0&typeid=46. [Google Scholar]
- 57.Erulkar AS, Onoka CJ, Phiri A. What is youth-friendly? Adolescents’ preferences for reproductive health services in Kenya and Zimbabwe. Afr J Reprod Health. 2005;9(3):51–8. [PubMed] [Google Scholar]
- 58.Ajayi AA, Marangu LT, Miller J, Paxman JM. Adolescent sexuality and fertility in Kenya: a survey of knowledge, perceptions, and practices. Stud Fam Plann. 1991;22(4):205–16. [PubMed] [Google Scholar]
- 59.Ferre C. Age at first child: does education delay fertility timing? Washington, DC: The World Bank; 2009. (The World Bank Policy Research Working Paper). [Google Scholar]
- 60.Loi N. Survey assessment of Vietnamese youth. Hanoi, Vietnam: General Accounting Office; 2010. [Google Scholar]
- 61.Resnick M, Bearman P, Blum RW, et al. Protecting adolescents from harm. Findings from the National Longitudinal Study on Adolescent Health. JAMA. 1997;278(10):823–32. doi: 10.1001/jama.278.10.823. [DOI] [PubMed] [Google Scholar]
- 62.Mensch BS, Lloyd CB. Gender differences in the schooling experiences of adolescents in low-income countries: the case of Kenya. Stud Fam Plann. 1998;29(2):167–84. [PubMed] [Google Scholar]
- 63.National Academy of Sciences: Board on Children Youth and Families. Engaging schools: fostering high school students’ motivation to learn. Washington, DC: National Academies Press; 2003. [Google Scholar]
- 64.McNeely C, Falci C. School connectedness and the transition into and out of health-risk behavior among adolescents: a comparison of social belonging and teacher support. J Sch Health. 2004;74(7):284–92. doi: 10.1111/j.1746-1561.2004.tb08285.x. [DOI] [PubMed] [Google Scholar]
- 65.Cho H, Hallfors DD, Mbai II, et al. Keeping adolescent orphans in school to prevent human immunodeficiency virus infection: evidence from a randomized controlled trial in Kenya. J Adolesc Health. 2011;48(5):523–6. doi: 10.1016/j.jadohealth.2010.08.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Lloyd C. New lessons: the power of educating adolescent girls. New York: Population Council; 2009. Available at: www.popcouncil.org. [Google Scholar]
- 67.World Health Organization. The sexual and reproductive health of younger adolescents: research issues in developing countries. RHR/11.15. Geneva: World Health Organization; 2001. [Google Scholar]
- 68.Moore KA, Theokas C. Conceptualizing a monitoring system for indicators in middle childhood. Child Indic Res. 2008;1:109–28. [Google Scholar]
- 69.Blumberg SH, Carle AC, O’Connor KS, Moore KA, Lippman LH. Social competence: development of an indicator for children and adolescents. Child Indic Res. 2007;1(1):176–97. [Google Scholar]
- 70.United Nations Population Fund. State of the world’s population: adolescent pregnancy. New York: United Nations Population Fund (UNFPA); 2013. [Google Scholar]
- 71.Costa F, Jessor R, Turbin M. The role of social contexts in adolescence: context protection and context risk in the United States and China. Appl Dev Sci. 2005;9(2):67–85. [Google Scholar]
- 72.Blum RW. Healthy youth development as a model for youth health promotion: a review. J Adolesc Health. 1998;22(5):368–75. doi: 10.1016/s1054-139x(97)00261-9. [DOI] [PubMed] [Google Scholar]
- 73.Rutter M. Resilience: some conceptual considerations. J Adolesc Health. 1993;14(8):626–31. doi: 10.1016/1054-139x(93)90196-v. [DOI] [PubMed] [Google Scholar]