

Abstract
Objectives:
The success of endodontic treatment is based on cleaning and shaping of the root canals. The root canals have complex morphology and wide individual variations. The objective of this study was to analyze root canals morphology and existence of extra canals in maxillary molars in Saudi subpopulation.
Methods:
Freshly extracted maxillary first molars (n=100) were included in this study. All teeth were examined for morphology of roots, root canals and apical foramen by Cone Beam Computed Tomography (CBCT). The root canals configuration was classified using Vertucci’s classification.
Results:
The majority of maxillary first molars (94%) were having three distinctly separated roots and 6% had four roots. Palatal and distobuccal roots were observed to contain one root canal (100%) and Vertucci’s type I configuration. The mesiobuccal root had one (29.4%; type I) or two canals (70.6%; type II, III or IV).
Conclusions:
The occurrence of second canal in the mesiobuccal root of upper first molar is very much likely (>70%). The mesiobuccal roots are more likely to have Vertucci’s type I or II configuration (>76%). The palatal and distobuccal roots always have a Vertucci’s type I canal configuration.
KEY WORDS: 1st Molar, Endodontics, Vertucci’s classification
INTRODUCTION
The success of endodontic treatment is keenly correlated to the exploration of the entire root canal system, thorough cleansing (mechanical as well as chemical) followed by obturation of prepared root canal system using inert filling materials and a sealant.1 In order to achieve this goal, it is crucial to detect each and every canal inside the roots. Any existing root canals that remain undetected by the operator during the entire course of endodontic treatment are a major threat to the failure of treatment.2 Hence the detailed knowledge of root canals morphology is essential. Considering the vast individual, genetic and ethnic variations, the clinicians must look for extra canals.
The details of human tooth morphology were published by GV Black in 1902.3 Each human tooth has its unique roots anatomy and has been studied in details.1 For example, mesiobuccal root of maxillary 1st molar has been reported to have two distinct canals since 1925.4 The first molar is the earliest permanent tooth to appear in the oral cavity exposing it for decay and in need of endodontic treatment. A number of studies have been published5-7 regarding maxillary first molar root canals morphology using various ethnic groups, methods, and approaches. Frequently utilized methods to study the root canal morphology are using staining solutions,1 radiographic techniques8,9 and more recently introduced cone beam computed tomography.10 CBCT is a technique that uses a specific beam to produce three dimensional images to reveal anatomic details precisely.11 The key advantages of using CBCT are that it is non-invasive and permits 3-D reconstruction of the root canals.12 Root morphology and properties of human tooth tissues differ among various ethnic populations.13 There is little scientific literature available for root morphology of various teeth in Saudi populations. The aim of the current research was to describe the variations in the root canal anatomy of maxillary first molar in residents of Al-Madinah Al-Munuawarrah, Saudi Arabia using cone beam computed tomography (CBCT).
METHODS
Freshly extracted maxillary permanent first molars (from residents of Madinah Munawarah, Saudi Arabia; age; 20-60 years) were included in this study (n=100). The patient’s gender and reason for extraction was not recorded. All teeth were inspected carefully to ensure the presence of intact roots with mature apices. Teeth with incomplete, broken or resorbed roots or obturated canals were excluded from the study. In order to remove any debris or attached tissue remnants, all teeth were cleaned and disinfected using 5% NaOCl solution for a day and washed using vigorous amount of ultrapure water. Teeth were kept in the normal saline medium while waiting for further experimentation. The study design was approved by Taibah University, College of dentistry research ethics committee (TUCD-REC-291014).
CBCT acquisition of specimens was conducted using Kodak 9000c 3-D system. The extraoral imaging machine and 3-DKodak Dental Imaging software (KDIS) version 1.3 were used following manufacturer’s guidelines. The image capturing parameters were set at 80 kV, exposure time of 30 seconds at 5.0 mA current. A 14-bit grey scalevoxel size (76×76×76μm) was used. The whole CBCT imaging protocol was carried by a registered dental radiologist following the ALARP [As Low As Reasonably Practicable] protocol.
The CBCT data was analyzed using an Imaging software (CS 3D; Care stream Health, Inc., 2011) and a 21 inches flat screen computer monitor with a resolution of 1440 × 900 pixels (Samsung Seoul, Korea). The contrast function was regulated and the magnifying device was activated when required. The X and Y cursors were used for horizontal and vertical orientation of CBCT images of teeth. In order to survey the anatomy of the roots and canals of maxillary molars from the axial plane, the Z cursor was moved slowly (1 mm interval) in cervico-apex direction. All of the images were assessed separately by two operators and any disagreement was discussed until a consensus was reached.
All maxillary molar images were analyzed carefully for roots (number), configuration and number of canals and apical foramina per root. In order to classify the root canal morphology, Vertucci’s1 classification (Fig.1) was used as a reference. Data interpretation was performed using SPSS software (version 20) and appropriate statistical tests were performed (p<0.05).
Fig.1.

Vertucci’s (1984) criteria for the classification of root canal morphology.
RESULTS
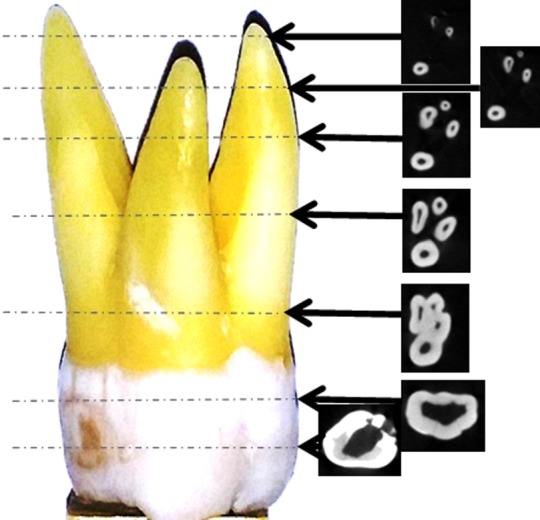
The physical and radiological examination showed that all teeth included in this study were multi-rooted containing at least three separated roots. The external morphology of typical maxillary first molar roots has been shown in Fig.2. The CBCT images of the same maxillary first molar tooth at various cervico-apical levels have been represented in Fig.3. The majority of teeth were having three distinctly separated roots (94%) followed by four (two palatal) roots (6%). The representative CBCT images of the four rooted maxillary first molar at various cervico-apical levels have been shown in Fig.4.
Fig.2.
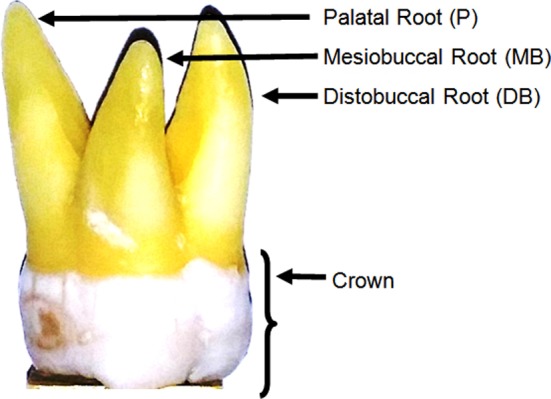
External anatomy of a typical maxillary molar with three diverging roots (mesiobuccal view).
Fig.3.

Internal anatomy of a typical maxillary 1st molar (three roots) using CBCT at various anatomical levels.
Fig.4.
Series of CBCT images of a rare (four rooted) maxillary 1st molar representing the internal anatomy and anatomical variations at various levels.
All roots (palatal and distobuccal) were observed to contain one root canal (100%) except the mesiobuccal root where single root canal was observed in 29.6% of maxillary molars (Table-I). The occurrence of two canals (mesiobuccal and mesiopalatal) in the mesiobuccal root was observed in 70.6% in the selected population.
Table-I.
Analysis of maxillary first molar root canal morphology.
| Number of roots | ||||
| One | Two | Three | Four | |
| 0 % | 0% | 94% | 6% | |
| Number of canals | ||||
| One | Two | |||
| Palatal root | 100% | 0 % | ||
| Distobuccal root | 100% | 0% | ||
| Mesiobuccal Root | 29.4% | 70.6% | ||
The classification and canal configurations of the maxillary first molar roots according to Vertucci’s criteria (Fig.1) have been given in Table-II. The root canal configuration for palatal roots and distobuccal roots was very straight forward. Vertucci’s class I configuration was observed in all (100%) of palatal and distobuccal roots (Table-II).
Table-II.
Classification of root canal morphology in maxillary first molar using Vertucci’s criteria.
| TYPE | ||||||||
|---|---|---|---|---|---|---|---|---|
| I | II | III | IV | V | VI | VII | VIII | |
| Palatal root | 100% | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Distobuccal root | 100% | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Mesiobuccal root | 29.4% | 47% | 11.8% | 11.8% | 0 | 0 | 0 | 0 |
The morphology of mesiobuccal roots remains relatively complex and various types of Vertucci’s root canal configuration types were observed. Vertucci’s type II was found most frequently (47%) followed by type 1 (29.4%) and type III and IV (11.8% each). Other types of Vertucci’s classification (types V, VI, VII and VIII) were not observed at all in any root of maxillary first molars (Table-II).
DISCUSSION
The significance of knowledge about the anatomic morphology of the maxillary molars and possible variations is vital for successful endodontic therapy and cannot be denied. The current study provides a detailed report on the morphology of root canals of maxillary 1st molars in Saudi Arabian population using CBCT. It is largely recognized that the most frequent pattern of the permanent maxillary 1st molar is comprised of three separated roots.14 This study has reported similar results as 94% of cases with three separate roots and only 6% with four separate roots. These finding are in a very close agreement with other studies; Barrett15 used the sectioning method to study the anatomy and reported three roots of maxillary first molar in more than 90% teeth. Thomas et al.16 examined maxillary molars radiographically using radiopaque gels as canal filler and reported three roots in 94.40% molars. A higher percentage (97.60%) was reported by Al-Shalabi et al.17 In the current study, we found 6% of maxillary first molars having four roots. It is obvious that root morphological anomalies are rare however exists in most populations. For example certain studies18 have reported four roots (2 palatal), or five roots,18 two root canals in a single palatal root19 or even three canals.20 In addition, incidence of C-shaped canals and root fusion have also been reported.21
The main concern for endodontists remains the number of canals inside each root. This study has reported palatal and distobuccal roots contain single canal (100% of cases). The incidence of two palatal canals is very rare.22 Cleghorn et al.5 has conducted a comprehensive review on the anatomy of the permanent maxillary 1st molar. All inclusive studies in this review analyzed more than 8400 teeth collectively and reported very rare incidence of two palatal roots/canal.5 Similar findings have been reported for the distal root, one canal in (100%) of cases in the current study and many other studies1,19 as well as in Kuwaiti population.23 However, a very low incidence (0.1-4%) of two or more canals has been reported.16,17
The mesiobuccal root is the main focus of morphological studies as the incidence of more than one canal is significantly high and a wide range of variations has been reported.24 In our study the mesiobuccal root contained single canal in 29.4% and two canals in 70.6% of cases. The incidence of once canal in mesiobuccal root is comparatively high in Saudi subpopulation. The highest incidence of one canal (75%) has been reported by Woelfel et al.25 The reported incidence of two or more canals varies widely; 25%25, 55%1, 58%8, 73.6%16 and 78%.17 There is not even a single study denying the existence of second canal maxillary first molars.5 This is very clear from the above discussion that the internal anatomy of maxillary 1st molar particularly the mesiobuccal root has never been straight forward. There is a high frequency of two or more canals system in the mesiobuccal root and diverges broadly based on factors such as racial ethnicity, population and configuration. The configuration of root canals make it further complicated as six different types of configuration has been classified by Vertucci’s.1 In the current study, three configuration types (Vertucci’s type II, III and III) were observed for two canals and only type I was observed for single canal roots.
CONCLUSIONS
Within the limitations of this study, the following conclusions can be drawn:
The maxillary first molar was found a three separated rooted tooth.
The incidence of two or four roots or fused roots was very rare.
The occurrence of second (mesiopalatal) canal in the maxillary 1st molar mesiobuccal root was very much likely (> 70%).
The mesiobuccal roots were more likely to have Vertucci’s type I or II canal configuration.
Footnotes
Conflict of interest: The authors declared no conflicts of interest.
Authors Contribution
Mothanna Alrahabi: Concept and research proposal, data collection and interpretation.
Muhammad Sohail Zafar: Literature review, Data analysis, drafting and revision of the manuscript.
REFERENCES
- 1.Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58(5):589–599. doi: 10.1016/0030-4220(84)90085-9. [DOI] [PubMed] [Google Scholar]
- 2.Weine FS, Healey HJ, Gerstein H, Evanson L. Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance. Oral Surg Oral Med Oral Pathol. 1969;28(3):419–425. doi: 10.1016/0030-4220(69)90237-0. [DOI] [PubMed] [Google Scholar]
- 3.Black GV. SS White manufacturing Company; 1902. Descriptive anatomy of the human teeth. [Google Scholar]
- 4.Zurcher E. New York: William Wood & Co; 1925. The anatomy of the root canals of the teeth of the deciduous dentition and of the first permanent molars. [Google Scholar]
- 5.Cleghorn BM, Christie WH, Dong CCS. Root and root canal morphology of the human permanent maxillary first molar: A literature review. J Endod. 2006;32(9):813–821. doi: 10.1016/j.joen.2006.04.014. doi:10.1016/j.joen.2006.04.014. [DOI] [PubMed] [Google Scholar]
- 6.Zheng Q, Wang Y, Zhou X, Wang Q, Zheng G, Huang D. A cone-beam computed tomography study of maxillary first permanent molar root and canal morphology in a Chinese population. J Endod. 2010;36(9):1480–1484. doi: 10.1016/j.joen.2010.06.018. doi:10.1016/j.joen.2010.06.018. [DOI] [PubMed] [Google Scholar]
- 7.Rizvi A, Zafar MS, Farid WM, Gazal G. Assessment of antimicrobial efficacy of MTAD, sodium hypochlorite, EDTA and chlorhexidine for endodontic applications: An in vitro study. Middle-East J Sci Res. 2014;21(2):353–357. [Google Scholar]
- 8.Weine F, Hayami S, Hata G, Toda T. Canal configuration of the mesiobuccal root of the maxillary first molar of a Japanese sub-population. Int Endod J. 1999;32(2):79–87. doi: 10.1046/j.1365-2591.1999.00186.x. [DOI] [PubMed] [Google Scholar]
- 9.Zafar MS, Javed E. Extraoral radiography: An alternative to intraoral radiography for endodontic (root canal system) length determination. Euro Sci J. 2013;9(15):51. [Google Scholar]
- 10.Yang H, Tian C, Li G, Yang L, Han X, Wang Y. A cone-beam computed tomography study of the root canal morphology of mandibular first premolars and the location of root canal orifices and apical foramina in a Chinese subpopulation. J Endod. 2013;39(4):435–438. doi: 10.1016/j.joen.2012.11.003. doi:10.1016/j.joen.2012.11.003. [DOI] [PubMed] [Google Scholar]
- 11.Durack C, Patel S. Cone beam computed tomography in endodontics. Braz Dent J. 2012;23(3):179–191. doi: 10.1590/s0103-64402012000300001. [DOI] [PubMed] [Google Scholar]
- 12.Neelakantan P, Subbarao C, Subbarao CV. Comparative evaluation of modified canal staining and clearing technique, cone-beam computed tomography, peripheral quantitative computed tomography, spiral computed tomography, and plain and contrast Medium–enhanced digital radiography in studying root canal morphology. J Endod. 2010;36(9):1547–1551. doi: 10.1016/j.joen.2010.05.008. doi:10.1016/j.joen.2010.05.008. [DOI] [PubMed] [Google Scholar]
- 13.Kim S, Kim BS, Woo J, Kim Y. Morphology of mandibular first molars analyzed by cone-beam computed tomography in a korean population: Variations in the number of roots and canals. J Endod. 2013;39(12):1516–1521. doi: 10.1016/j.joen.2013.08.015. doi:10.1016/j.joen.2013.08.015. [DOI] [PubMed] [Google Scholar]
- 14.Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endodontic Topics. 2005;10(1):3–29. [Google Scholar]
- 15.Barrett M. The internal anatomy of the teeth with special reference to the pulp with its branches. Dent cosmos. 1925;67(6):581–598. [Google Scholar]
- 16.Thomas RP, Moule A, Bryant R. Root canal morphology of maxillary permanent first molar teeth at various ages. Int Endod J. 1993;26(5):257–267. doi: 10.1111/j.1365-2591.1993.tb00570.x. [DOI] [PubMed] [Google Scholar]
- 17.Al Shalabi R, Omer JG, Jennings M, Claffey N. Root canal anatomy of maxillary first and second permanent molars. Int Endod J. 2000;33(5):405–414. doi: 10.1046/j.1365-2591.2000.00221.x. [DOI] [PubMed] [Google Scholar]
- 18.Barbizam JVB, Ribeiro RG. Unusual anatomy of permanent maxillary molars. J Endod. 2004;30(9):668–671. doi: 10.1097/01.don.0000121618.45515.5a. [DOI] [PubMed] [Google Scholar]
- 19.Hartwell G, Bellizzi R. Clinical investigation of in vivo endodontically treated mandibular and maxillary molars. J Endod. 1982;8(12):555–557. doi: 10.1016/S0099-2399(82)80016-2. [DOI] [PubMed] [Google Scholar]
- 20.Wong M. Maxillary first molar with three palatal canals. J Endod. 1991;17(6):298–299. doi: 10.1016/S0099-2399(06)81871-6. [DOI] [PubMed] [Google Scholar]
- 21.De Moor R. C-shaped root canal configuration in maxillary first molars. Int Endod J. 2002;35(2):200–208. doi: 10.1046/j.1365-2591.2002.00461.x. [DOI] [PubMed] [Google Scholar]
- 22.Christie W, Peikoff M, Fogel H. Maxillary molars with two palatal roots: A retrospective clinical study. J Endod. 1991;17(2):80–84. doi: 10.1016/S0099-2399(06)81613-4. [DOI] [PubMed] [Google Scholar]
- 23.Zaatar EI, Al-Kandari AM, Alhomaidah S, Al Yasin IM. Frequency of endodontic treatment in Kuwait: Radiographic evaluation of 846 endodontically treated teeth. J Endod. 1997;23(7):453–456. doi: 10.1016/s0099-2399(97)80302-0. [DOI] [PubMed] [Google Scholar]
- 24.Sempira H, Hartwell G. Frequency of second mesiobuccal canals in maxillary molars as determined by use of an operating microscope: A clinical study. J Endod. 2000;26(11):673–674. doi: 10.1097/00004770-200011000-00010. [DOI] [PubMed] [Google Scholar]
- 25.Woelfel JB, Sousa NMD, Issa EP. Morphologic study of the maxillary molars part II: Internal anatomy. Braz Dent J. 1992;3:53–55. [PubMed] [Google Scholar]