

Abstract
STUDY DESIGN
Controlled laboratory study using a cross-sectional design.
OBJECTIVES
To analyze the relationship of quadriceps-hamstrings and medial-lateral quadriceps anatomical cross-sectional area (ACSA) ratios with knee loads during walking and articular and meniscal cartilage composition in young, healthy subjects.
BACKGROUND
Muscle forces affect knee loading during walking, but it is not known if muscle morphology is associated with walking mechanics and cartilage composition in young subjects.
METHODS
Forty-two knees from 27 young, healthy, active volunteers (age, 20-35 years; body mass index, <28 kg/m2) underwent 3-T magnetic resonance imaging (MRI) and 3-D motion capture. Standard MRI sequences were used for articular and meniscal cartilage T1rho and T2 relaxation times and for quadriceps and hamstrings muscle ACSA. Frontal plane kinetics during the stance phase of walking was calculated. Generalized estimating equation models were used to identify muscle variables that predicted MRI and gait parameters.
RESULTS
Quadriceps-hamstrings and medial-lateral quadriceps ACSA ratios were positively related to frontal plane loading (β = .27-.54, P≤.006), global articular cartilage relaxation times (β = .22-.28, P≤.041), and the medial-lateral ratio of meniscus T1rho relaxation time (β = .26-.36, P≤.049). The medial-lateral quadriceps ACSA ratio was positively related to global meniscus T1rho relaxation times (β = .30, P = .046).
CONCLUSION
Higher quadriceps-hamstrings and medial-lateral quadriceps ACSA ratios were associated with higher frontal plane loading during walking and with articular and meniscal cartilage T1rho and T2 relaxation times. These findings highlight the relationships between different knee tissues and knee mechanics in young, healthy individuals.
Keywords: cartilage, gait, knee adduction moment, meniscus, quantitative MRI
Quadriceps and hamstrings muscles, along with the gastrocnemii, are the largest contributors to articular loading at the knee during walking and impact the distribution of loads across the knee.19,38,47,58,59 The external knee adduction moment (KAM)4,19 and impulse54 are common indirect measures of frontal plane knee loading. They are associated with greater load over the medial knee compartment19,32 and an increased risk of medial cartilage and meniscus damage, and may lead to medial knee osteoarthritis (OA).29,46,55 Although radiographic OA severity and varus malalignment partly explain the variability in KAM across individuals,12 biomechanical properties of the quadriceps and hamstrings may also be related to the magnitude of frontal plane loads.13,25,34 For instance, greater quadriceps strength has been shown to be related to faster walking speed,9,36,57 which leads to higher KAM.33 In people with knee OA and obesity, maximal hamstring strength was found to be positively correlated with KAM.1 These findings suggest that quadriceps and hamstrings strength may be related to KAM during walking.
Muscle strength tests are affected by multiple factors, including motivation, pain, fatigue, etc.44 Because the force-generating ability of a muscle closely depends on the muscle mass, anatomical cross-sectional area (ACSA) measured with magnetic resonance imaging (MRI) offers a valid and easy alternative that has been shown to strongly correlate with strength measures.14,35,49 Earlier work has shown that healthy individuals with varus alignment have a greater vastus medialis-vastus lateralis ACSA ratio.50 It is also known that healthy individuals with varus alignment walk with higher KAM compared to those with neutral alignment, which may predispose them to knee OA.6 Hence, there may be an association between measures of muscle ACSA ratios and those of knee loading.
Because quadriceps and hamstrings muscles influence loading patterns at the knee during walking, presumably, they would be related to knee cartilage health. People with knee OA or patellofemoral joint pain syndrome exhibit a reduction of quadriceps ACSA.18,41 In young, healthy people, thigh muscle ACSA is positively associated with knee cartilage thickness and volume.15 Early cartilage changes in knee OA consist of proteoglycan loss and an increase in water content, along with loosening, disorganization, and loss of collagen matrix (FIGURE 1).26,39 These early changes can be detected as an increase in MRI T1rho and T2 relaxation-time parameters.2,22,23,42,43 A positive association between higher medial-lateral quadriceps ACSA ratio and greater cartilage degeneration has been shown in older adults with preclinical knee OA, using quantitative T2 relaxation-time mapping and clinical whole-organ MRI scores.37
FIGURE 1.
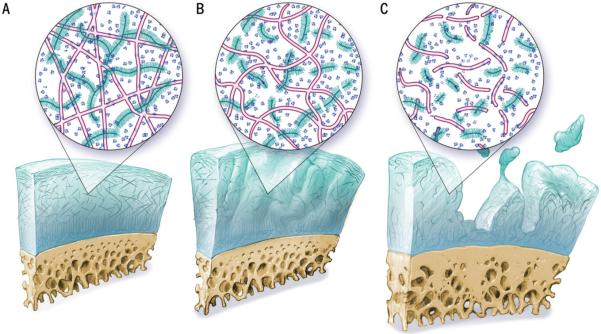
Schematic showing changes in articular cartilage with osteoarthritis. Cartilage layer is shown in blue and subchondral bone in yellow. The zoomed area shows cartilage composition with pink collagen network and blue proteoglycan molecules. (A) Healthy cartilage, (B) early degeneration with intact cartilage but loss of proteoglycans and disruption of collagen network, and (C) advanced degeneration with cartilage fissuring, further loss of proteoglycans, and collagen degradation. ©Andrew Swift. Reproduced with permission.
Quantitative evaluation of thigh muscle, knee cartilage, and gait mechanics in asymptomatic young populations has not been performed. As such, the aims of this study were (1) to analyze the relationship of the quadriceps-hamstrings (QH) ACSA ratio and the medial-lateral quadriceps (QuadML) ACSA ratio with walking mechanics, and (2) to analyze the relationship of the QH ACSA ratio and the QuadML ACSA ratio with articular and meniscal cartilage T1rho and T2 relaxation times in young, healthy people. The study hypotheses were that (1) higher muscle ACSA ratios would be related to higher frontal plane loading during walking, and (2) higher muscle ACSA ratios would be related to higher articular and meniscal cartilage T1rho and T2 relaxation times.
METHODS
Subjects
Twenty-seven healthy volunteers (mean ± SD age, 27.6 ± 3.7 years; body mass index [BMI], 22.7 ± 2.1 kg/m2; 18 men, 9 women) between the ages of 20 and 35 years were recruited from the community. The University of California San Francisco Institutional Review Board approved the study protocol, and all subjects signed an approved informed-consent form. The subjects were physically active (at least 150 min/ wk of moderate to vigorous physical activity) and had no history of knee pain or any other lower extremity injuries that would confound the evaluation of walking patterns. Though MRI images from both knees were collected where available, not all subjects completed an MRI in both knees, thus the total sample was of 42 knees.
MRI Image Acquisition
All imaging was performed with a 3-T Signa HDx MRI scanner (GE Healthcare, Waukesha, WI), using an 8-channel phased-array transmit/receive knee coil (Invivo, Gainesville, FL). The total acquisition time for 1 knee was approximately 25 minutes. For thigh muscle ACSA, the subjects were repositioned in the scanner without the knee coil. The body coil was used to acquire axial slices from the middle 50% of the total length of the bilateral thighs in the same field of view. The mid thigh was selected, because earlier work has shown that image acquisition at 50% of the femur length is the best compromise for evaluating quadriceps and hamstrings ACSA in a single slice, and ACSA estimates at this level correlate well with muscle volume.11 It also helped standardize image acquisition. The length of the thighs was calculated using the distance between the center of the femoral head and the center of the knee joint from a scout view. The imaging parameters for all sequences are shown in TABLE 1.
TABLE 1.
Magnetic Resonance Imaging Acquisition Parameters
| Sequence | Parameters | Variables |
|---|---|---|
| Sagittal, T2-weighted, fat-saturated FSE | TR/TE, 4300/51 ms; FOV, 14 cm; matrix, 512 × 256; slice thickness, 2.5 mm; gap, 0.5 mm; ETL, 9; bandwidth, 31.25 kHz; NEX, 2 | Semi-quantitative clinical WORMS grades |
| Sagittal, 3-D, fat-saturated high-resolution SPGR | TR/TE, 15/6.7 ms; flip angle, 18; FOV, 14 cm; matrix, 512 × 512; slice thickness, 1 mm; bandwidth, 31.25 kHz; NEX, 1 | Articular cartilage thickness |
| T1rho/T2 quantification sequence | TSL, 0/10/40/80 ms; prep TE, 0/13.7/27.3/54.7 ms; FOV, 14 cm; matrix, 256 × 128; VPS, 64; time of recovery, 1.2 s; slice thickness, 4 mm; number of slices, 26; acquisition time, 9 min and 30 s | Articular and meniscal cartilage T1rho/T2 relaxation times |
| Axial, FSE T1-weighted sequence of thigh muscles | TE/TR, 6.41/800; slice thickness, 10 mm; matrix, 384 × 1932; ETL, 2; bandwidth, 150 kHz; NEX, 4 | Thigh muscle ACSA |
Abbreviations: ACSA, anatomical cross-sectional area; ETL, echo train length; FOV, field of view; FSE, fast spin-echo; NEX, number of excitations; SPGR, spoiled gradient-echo; TE, echo time; TR, relaxation time; TSL, spin lock time; VPS, views per segment; WORMS, whole-organ magnetic resonance imaging score.
Semi-quantitative Morphological MRI Grading
The modified whole-organ MRI score40,61 was used to assess cartilage and meniscus abnormalities on sagittal, T2-weighted, fast spin echo, fat-saturated images (TABLE 1) by a musculoskeletal radiologist with 20 years of experience (T.M.L.).
MRI Image Analysis
MRI images were transferred to a workstation (Hewlett-Packard Company, Palo Alto, CA) for offline quantification of MRI relaxation times (T1rho and T2). Cartilage surface and meniscus were segmented in sagittal spoiled gradient-echo images using a software program developed in-house, based on a spline-based, semi-automated (automated edge detection and manual correction) segmentation algorithm in MATLAB (The MathWorks, Inc, Natick, MA). This algorithm was used to identify the boundary of the cartilage regions of interest.
Cartilage segmentation was divided into 6 regions: medial and lateral femoral condyle, medial and lateral tibial plateau, patella, and trochlea. For the purpose of this paper, all the regions of interest were merged to form the global knee region. Also, the medial femur and tibia were combined to form the medial knee region, and the lateral femur and tibia combined to form the lateral knee region. Relaxation times were then calculated for the merged regions of interest. Medial-lateral ratios were taken by dividing medial-region by lateral-region variables.
Six regions of the meniscus (medial and lateral posterior horns, medial and lateral anterior horns, and medial and lateral body) were also segmented. For the purpose of this paper, all subregions of the medial meniscus were combined to form the medial meniscus region and, similarly, all subregions of the lateral meniscus were combined to form the lateral meniscus region. Medial and lateral regions were combined to form the global meniscus region. Medial-lateral ratios for the meniscus were taken by dividing medial by lateral values.
Quantification of T1rho and T2
The T1rho and T2 maps (FIGURES 2A and 2B) were reconstructed by fitting the image intensity (voxel by voxel) using a Levenberg-Marquardt monoexponential fitting algorithm developed in-house: S(TSL) = S0 exp(–TSL/T1rho) for T1rho fitting, where TSL is the spin lock time and S0 is the signal intensity when TSL equals 0 milliseconds; and S(TE) = S0 exp(–TE/T2) for T2 fitting, where TE is the echo time and S0 is the signal intensity when TE equals zero. All 4 T1rho- or T2-weighted images were used to reconstruct the cartilage maps. However, for the meniscus (FIGURES 2C and 2D), only the first 3 T1rho- and T2-weighted images were used.42 T1rho-weighted images with TSL equal to 80 milliseconds and T2-weighted images with TE equal to 44.8 milliseconds had a very low signal-to-noise ratio (less than 5) for the meniscus due to short T1rho and T2 in the meniscus, and therefore were not used during map reconstruction. To minimize the error due to knee motion between the scans, T1rho- and T2-weighted images with the shortest TSL or TE (and, therefore, the highest signal-to-noise ratio) were rigidly registered to high-resolution, spoiled gradient-echo images (TABLE 1) acquired in the same examination with the Visualization Toolkit by the Computational Imaging Sciences Group (Kitware, Inc, Clifton Park, NY).51,53 The transformation matrix was applied to the reconstructed T1rho and T2 maps. The original splines of segmented cartilage and meniscus contours from the high-resolution spoiled gradient-echo images were superimposed on the corresponding reconstructed T1rho and T2 maps to define the regions of interest for T1rho and T2 assessment.21,53,61 To reduce artifacts caused by partial-volume effects with synovial fluid, regions with relaxation time greater than 150 milliseconds in T1rho or 100 milliseconds in T2 maps were removed from the data used for quantification.53
FIGURE 2.

Color maps of medial femur and medial tibia articular cartilage for T1rho (A), T2 (B), and meniscal cartilage T1rho (C) and T2 (D).
Quantification of Muscle Cross-sectional Area
One researcher (W.L.) manually segmented vastus medialis, vastus lateralis, vastus intermedius, rectus femoris, medial hamstrings (semitendinosus and semi-membranosus), and lateral hamstrings (biceps femoris long head) regions of interest on 4 slices at the middle of the scanned volume (FIGURE 3A). Because the scanned volume was the middle 50% of the thigh for every subject, the segmented slices corresponded to the midsection of the thigh. Intramuscular fat, which would be minimal in these young, healthy, active subjects (Goutallier grade 0, indicating less than 5% fat fraction),3 was not excluded for the purpose of calculating muscle ACSA. After segmentation, ACSA for each muscle was calculated for each slice, using a routine developed in-house in MATLAB. The area over the 4 slices was averaged for each muscle. The 4 quadriceps were added to form the quadriceps area (FIGURE 3B). The 2 hamstrings were added to form the hamstrings area (FIGURE 3B). For the statistical analyses, ratios were taken (FIGURE 3C) for QH ACSA and QuadML ACSA.
FIGURE 3.

(A) Bilateral thigh muscle regions of interest for RF, VM, VL, VI, MH, and LH; (B) grouping of muscle regions as quadriceps (red) and hamstrings (green); and (C) grouping of the quadriceps muscle regions as medial (yellow) and lateral (pink) regions. Abbreviations: LH, lateral hamstrings; MH, medial hamstrings; RF, rectus femoris; VI, vastus intermedius; VL, vastus lateralis; VM, vastus medialis.
Motion Analysis
All subjects walked at their self-selected speed, while 3-D kinematic data were collected at 250 Hz using a passive 10-camera system (Vicon; OMG plc, Oxford, UK) and kinetic data were collected at 1000 Hz from 2 embedded force platforms (Advanced Mechanical Technology, Inc, Watertown, MA). Spherical retroreflective markers (14 mm) were placed on bony landmarks of bilateral lower extremities for identification of joint centers, and rigid clusters were placed bilaterally on the lateral surface of the subject's thighs, legs, and heel shoe counters to track segment motions.52 A trial was considered acceptable when there was a clean foot strike on any of the force platforms and the speed was within 5% of the first good trial. Five good trials were collected from both lower extremities.
Motion Analysis Data Processing
Kinematics and kinetics were calculated using Visual3D (C-Motion, Inc, Germantown, MD). All net joint moments are expressed as external moments and normalized to body weight and height (Nm/ BW·Ht). Variables were calculated for the stance phase when the foot was in contact with the ground and included peak external knee flexion moment, KAM, and KAM impulse. The average of 5 trials was calculated for each subject.
Statistics
Group means and standard deviations were calculated for all variables. Because there were data from both knees of some of the individuals in our cohort, we used generalized estimating equations (GEEs) to assess the relationships of muscle ACSA measures with articular and meniscal cartilage T1rho and T2 relaxation times, and with kinematic and kinetic variables. The GEE method is able to account for the interrelationship of data from bilateral knees of the same individuals.30,60 Furthermore, because muscle ACSA is known to be related to BMI and gender, the GEE models were adjusted for age, BMI, gender, and walking speed (for gait mechanics). Because the units for the muscle area, gait, and MRI variables are very different, all data were standardized (z-scores) so that the beta coefficients were in SD units. Beta coefficients range from −1 to 128 but are not equivalent to the Pearson correlation coefficient. For instance, a Pearson correlation coefficient of 0.25 would be considered a measure of a “weak” relationship (explaining 6.25% variability in the outcome), but a beta coefficient of 0.25 would indicate that a 2-SD change in the predictor is associated with a change in the outcome variable of 0.5 SD (2 × 0.25 SD), which is enough to move someone from the 50th percentile to approximately the 68th percentile. Hence, these beta coefficients should be interpreted on a case-by-case basis, considering the relative changes in SD between the predictor and the outcome variable and the associated P value.
The primary analyses were designed to evaluate the relationship of QH and QuadML ACSA ratios with peak external knee flexion moment, peak KAM, and KAM impulse during walking. Secondary analyses were used to evaluate the relationship of QH and QuadML ACSA ratios with global T1rho and T2 times, with global meniscus T1rho and T2 times, and with medial-lateral ratios of articular and meniscal cartilage T1rho and T2 times.
RESULTS
Semi-quantitative Morphological MRI Grading
Abnormalities of the menisci and cartilage were found only in 4 of 42 knees. There was 1 knee with a medial meniscus tear (posterior horn, grade 2) and 3 knees with patellofemoral cartilage lesions. These were confirmed on a repeat reading, as well as on a reading by a second experienced musculo-skeletal radiologist.
Muscle ACSA
Means and standard deviation values of the ACSA for all muscle groups are listed in TABLE 2. The ACSA of quadriceps muscle was approximately 3 times larger than that of the hamstrings, with a QH ratio of 2.85 (TABLE 2). The QuadML ACSA ratio was 0.44 (TABLE 2).
TABLE 2.
Mid-Thigh Muscle Anatomical Cross-sectional Area and Ratios*
| Compartment | Area, mm2 |
|---|---|
| Vastus medialis | 1294.30 ± 396.42 |
| Vastus lateralis | 2968.02 ± 589.40 |
| Vastus intermedius | 2416.68 ± 501.23 |
| Rectus femoris | 910.12 ± 231.41 |
| Medial hamstrings | 1580.84 ± 302.24 |
| Lateral hamstrings | 1090.41 ± 204.52 |
| Quadriceps | 7589.12 ± 1471.56 |
| Hamstrings | 2671.25 ± 453.76 |
| Anatomical cross-sectional area ratios | |
| Quadriceps-hamstrings | 2.85 ± 0.39 |
| Medial-lateral quadriceps | 0.44 ± 0.09 |
Values are mean ± SD.
Muscle ACSA and Gait Mechanics
Results are shown in TABLE 3. After accounting for age, gender, BMI, and walking speed, the QH and QuadML ACSA ratios were positively related to KAM (β = .48, P<.001; β = .27, P = .006) and KAM impulse (β = .54, P<.001; β = .32, P = .001) (FIGURES 4A and 4B). Neither of the predictors showed a significant relationship with peak external knee flexion moment (P>.05).
TABLE 3.
Results From Generalized Estimating Equations for Association Between Muscle Cross-sectional Area and Kinetic Gait Variables
| Outcome/Predictor | Beta Coefficient* | P Value |
|---|---|---|
| Peak sagittal moment | ||
| Quadriceps-hamstrings ratio | −.21 (−.49, .06) | .133 |
| Medial-lateral quadriceps ratio | .09 (−.14, .31) | .451 |
| Peak KAM | ||
| Quadriceps-hamstrings ratio | .48 (.28, .69) | <.001 |
| Medial-lateral quadriceps ratio | .27 (.01, .47) | .006 |
| KAM impulse | ||
| Quadriceps-hamstrings ratio | .54 (.35, .73) | <.001 |
| Medial-lateral quadriceps ratio | .32 (.13, .50) | .001 |
Abbreviation: KAM, knee adduction moment.
Accounting for age, gender, body mass index, and walking speed. Values in parentheses are 95% confidence interval.
FIGURE 4.

Scatter plots of key relationships. (A) Quadriceps-hamstrings ACSA ratio and peak knee adduction moment, (B) quadriceps-hamstrings ACSA ratio and knee adduction moment impulse, (C) quadriceps-hamstrings ACSA ratio and global T2, and (D) quadriceps-hamstrings ACSA ratio and medial-lateral meniscus T1rho ratio. Abbreviations: ACSA, anatomical cross-sectional area; BW, body weight; Ht, height.
Muscle ACSA and Articular Cartilage MRI Relaxation Times
Results are shown in TABLE 4. After accounting for age, gender, and BMI, the QuadML ratio was a significant predictor of global T1rho relaxation times (β = .23, P = .020), but the QH ACSA ratio did not show a similar association (β = .16, P = .199). Both the QH ratio (β = .28, P = .009) and QuadML ratio (β = .22, P = .041) had a significant positive association with global T2 relaxation times. Neither of the predictors showed a significant association with medial-lateral T1rho or T2 relaxation-time ratios (P>.05).
TABLE 4.
Results From Generalized Estimating Equations for Association Between Muscle Cross-sectional Area and Articular and Meniscal Cartilage T1rho and T2 Relaxation Times
| Outcome/Predictor | Beta Coefficient* | P Value |
|---|---|---|
| Articular cartilage T1rho and T2 relaxation times | ||
| Global T1rho | ||
| Quadriceps-hamstrings ratio | .16 (−.08, .40) | .199 |
| Medial-lateral quadriceps ratio | .23 (.02, .44) | .020 |
| Medial-lateral ratio T1rho | ||
| Quadriceps-hamstrings ratio | (−.03 (−.27, .21) | .820 |
| Medial-lateral quadriceps ratio | .19 (−.11, .49) | .207 |
| Global T2 | ||
| Quadriceps-hamstrings ratio | .28 (.07, .49) | .009 |
| Medial-lateral quadriceps ratio | .22 (.01, .44) | .041 |
| Medial-lateral ratio T2 | ||
| Quadriceps-hamstrings ratio | −.19 (−.41, .03) | .084 |
| Medial-lateral quadriceps ratio | .19 (−.07, .45) | .160 |
| Meniscal cartilage T1rho and T2 relaxation times | ||
| Global T1rho | ||
| Quadriceps-hamstrings ratio | −.09 (−.37, .20) | .563 |
| Medial-lateral quadriceps ratio | .30 (.01, .59) | .046 |
| Medial-lateral ratio T1rho | ||
| Quadriceps-hamstrings ratio | .36 (.13, .60) | .003 |
| Medial-lateral quadriceps ratio | .26 (.01, .51) | .049 |
| Global T2 | ||
| Quadriceps-hamstrings ratio | .06 (−.14, .26) | .561 |
| Medial-lateral quadriceps ratio | .15 (−.10, .39) | .234 |
| Medial-lateral ratio T2 | ||
| Quadriceps-hamstrings ratio | .08 (−.17, .32) | .537 |
| Medial-lateral quadriceps ratio | .08 (−.18, .34) | .549 |
Accounting for age, gender, and body mass index. Values in parentheses are standard error.
Muscle ACSA and Meniscal Cartilage MRI Relaxation Times
Results are shown in TABLE 4. After accounting for age, gender, and BMI, the QuadML ACSA ratio (β = .30, P = .046), but not the QH ACSA ratio (β = −.09, P = .563), had a positive association with global meniscus T1rho relaxation times. Neither predictor had a significant relationship with global meniscus T2 relaxation times (P>.05). Both the QH ACSA ratio (β = .36, P = .003) and QuadML ACSA ratio (β = .26, P = .049) had a significant positive relationship with the medial-lateral ratio of meniscus T1rho relaxation time. Similar relationships were not observed for the medial-lateral ratio of meniscus T2 relaxation times (P>.05).
DISCUSSION
The aims of this study were (1) to analyze the relationship of the QH and QuadML ACSA ratios with walking mechanics, and (2) to analyze the relationship of the QH and QuadML ACSA ratios with articular and meniscal cartilage T1rho and T2 relaxation times in young, healthy people. Results show that higher QH and QuadML ACSA ratios are associated with higher KAM and KAM impulse during walking in young, healthy volunteers, in accordance with our first hypothesis. The results partly support our second hypothesis, as we observed positive associations between muscle ACSA ratios and some of the articular and meniscal cartilage T1rho and T2 relaxation-time variables. These findings highlight the relationships between different knee tissues and knee mechanics in young, healthy individuals. We found that QH and QuadML ACSA ratios were positively related with peak KAM and KAM impulse in this cohort of young, healthy individuals. Overall, these associations were strong (β>.25, P≤.006), but the QH ACSA ratio demonstrated a stronger relationship (β>.45, P<.001) with these loading variables, compared to the QuadML ACSA ratio (.25<β<.45, P≤.006). Earlier studies have shown that in young, healthy individuals, muscle ACSA is strongly associated with joint moments assessed using dynamometry.5,8 In people with knee OA, it was shown that quadriceps strength is not related to KAM25 and that a program of quadriceps strengthening did not lead to a change in KAM.24 It has also been shown that quadriceps strength is not related to impact loading in the same population.17 Net joint moments during gait do not take into account muscle coactivations and hence may underestimate joint loads. Musculoskeletal modeling approaches have demonstrated that muscle forces are critical to balancing the external loads during dynamic activities.19,20,38 Hence, knowledge of muscle ACSA and ratios provides additional insight into the role of muscles in counterbalancing external loads. Our data demonstrate that larger quadriceps relative to hamstrings and larger medial quadriceps relative to lateral quadriceps are associated with greater frontal plane loading. Higher frontal plane loading is known to be associated with onset and progression of knee OA.4,29 The magnitude of the muscle ACSA ratio at which the imbalance pre-disposes individuals to cartilage degeneration and whether a similar relationship may exist in people with pre-existing disease remain to be seen.
We did not find significant relationships between thigh muscle ACSA ratios and sagittal plane moment in this cohort. Instrumented knee prosthesis and modeling studies suggest that sagittal moment also needs to be taken into consideration to better characterize knee loading during walking.19,56 For example, if the KAM decreases and the knee flexion moment decreases, then one can be fairly, although not 100%, confident that the medial contact force has decreased. If both increase, it is likely that medial contact force will also increase. When the moments change in opposite directions, it is difficult to infer what might be occurring at the joint. It may be possible that the differences in the relative sizes of thigh muscles and their corresponding force-generation ability are more critical to balancing frontal plane loads than sagittal plane loads, although this is hard to conclude from these data.
We observed that larger quadriceps ACSA relative to hamstrings ACSA (greater QH ACSA ratio) was associated with higher global knee articular cartilage T2 relaxation times. Larger medial quadriceps relative to the lateral quadriceps (greater QuadML ACSA ratio) was associated with higher global T1rho and T2 relaxation times. Similar to the associations between muscle ACSA ratios and frontal plane loading metrics, the QH ratio (β>.25, P = .009) demonstrated stronger associations with articular cartilage MRI relaxation times than the QuadML ratio (β<.25, P = .041). Higher T1rho and T2 relaxation times indicate relatively lower proteoglycan content and greater collagen disruption. The only other study with a similar objective found a higher vastus medialis-vastus lateralis ratio to be associated with higher knee articular cartilage T2 times in people with knee OA.37 The present study supports those findings and extends those results to young, healthy individuals. The present study found a high QuadML ratio to be related to higher articular cartilage global T1rho and T2 relaxation times. There was a difference in the vastus medialis-vastus lateralis ratio found in that previous study37 (approximately 1.12) compared to our results (0.44). In the Osteoarthritis Initiative study,37 ACSA was measured at a location 15 cm above the patella, which was defined as the mid thigh. We defined mid thigh as the middle 50% of the thigh, which could have led to underrepresentation of the vastus medialis in this study and an underestimation of the vastus lateralis in the Osteoarthritis Initiative study.37 The difference may also be attributable to the different sample populations of the 2 studies.
For the meniscus, we found that a higher QH ACSA ratio was associated with a higher medial-lateral ratio of meniscus T1rho relaxation times. A higher QuadML ACSA ratio was associated with higher meniscus global T1rho relaxation times and the medial-lateral ratio of T1rho relaxation times. As for articular cartilage, the QH ratio (β>.25, P = .003) demonstrated stronger associations with the meniscus MRI relaxation times than the QuadML ratio (β>.25, P = .049). These results suggest that larger quadriceps relative to the hamstrings and, perhaps, larger medial quadriceps relative to lateral quadriceps are associated with relatively lower proteoglycan in the medial meniscus relative to the lateral meniscus. Because both QH and QuadML ratios were positively related to frontal plane loading, it is possible that the impact of muscle ACSA ratios on cartilage composition is mediated through abnormal frontal plane loading. Longitudinal studies would be needed to confirm this speculation.
Our findings show different relationships of muscle ACSA ratios with articular and meniscal cartilage T1rho and T2 relaxation times. T1rho relaxation time is related to the proteoglycan content of the cartilage, whereas the T2 relaxation-time parameter is related to collagen integrity.23 Furthermore, the structure of articular and meniscal cartilage is very different. The knee menisci are fibrocartilaginous and composed primarily of type 1 collagen, whereas the articular cartilage is hyaline cartilage primarily composed of type 2 collagen and has a larger proteoglycan concentration compared to the knee meniscus. During loading, the knee menisci carry 45% to 70% of the compressive knee load, respond by converting vertical loads into hoop stresses, and help in load transmission.10,45,48 These differences between T1rho and T2 relaxation times, and between articular and meniscal cartilage structure, may be reflected in the results from this study.
There are limitations in this study that need to be addressed when interpreting the results. A mid-thigh ACSA was employed instead of volume for describing muscle morphology. However, a number of studies have demonstrated that single-slice ACSA is predictive of muscle volume and that muscle ACSA measurements are predictive of muscle strength and joint moments, and are sensitive to changes due to disuse/training.7,8,11,16,27 In our study, the ACSA for the vastus medialis might have been underestimated, which could have influenced our findings related to the QuadML ACSA ratio but is unlikely to have influenced those related to the QH ACSA ratio, because mid-thigh ACSA is considered adequate for overall quadriceps and hamstrings volume.11 We also did not take into consideration fascicle length and pennation angle, which are used to calculate physiological CSA. However, studies have shown that ACSA of the quadriceps correlates well with physiological CSA.8,31 Due to the small sample size, the results of this study are only generalizable to young, healthy, physically active adults. A P value of less than .05 was considered significant for each individual GEE model. Due to the large number of GEE models, P values close to .05 need to be interpreted with caution. Also, muscle activation during walking was not assessed; these data could have provided further insight into the relationship between CSA and walking mechanics. Finally, another limitation is that the MRI and motion analysis were not performed in immediate succession but with an average gap of 1 week between collections. Because the response of cartilage to loading is cumulative in nature, and none of our subjects sustained any injuries between the 2 sessions, the gap is unlikely to have affected our data.
CONCLUSION
Higher QH and QuadML ACSA ratios were associated with higher KAM and KAM impulse during walking in young, healthy subjects. Higher QH and QuadML ACSA ratios were also positively related to some of the parameters of articular and meniscal cartilage T1rho and T2 relaxation times. These findings highlight the relationships between different knee tissues and knee mechanics in young, healthy individuals.
KEY POINTS.
FINDINGS: Higher QH and QuadML ACSA ratios were associated with higher KAM and KAM impulse during walking in young, healthy subjects. Higher QH and QuadML ACSA ratios were also positively related to some of the parameters of articular and meniscal cartilage T1rho and T2 relaxation times.
IMPLICATIONS: These results show that the relative size of quadriceps and hamstrings, and that of medial and lateral quadriceps, is related to frontal plane loading and may be related to cartilage and meniscus composition.
CAUTION: Because these analyses were performed on young, healthy, physically active adults, the observed relationships would need to be investigated in people with knee OA. Also, these results would need to be replicated in larger samples and the subjects followed longitudinally to ascertain the long-term relationship of muscle ACSA with loading and cartilage health.
ACKNOWLEDGEMENTS
The authors thank Anthony Luke for providing equipment and facilities for motion capture, and Lorenzo Nardo, Nishant Neel, and Kelly Bauer for data processing.
This study was funded by the University of California San Francisco Radiology Seed Grant #11-07, NIH-NIAMS P50AR060752, NIH-NIAMS R01AR046905, and NIH-NIAMS R01AR046905-11A1. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The protocol for this study was approved by the University of California San Francisco Institutional Review Board (UCSF CHR #11-06473). The authors certify that they have no affiliations with or financial involvement in any organization or entity with a direct financial interest in the subject matter or materials discussed in the article.
REFERENCES
- 1.Aaboe J, Bliddal H, Alkjaer T, Boesen M, Henriksen M. The influence of radiographic severity on the relationship between muscle strength and joint loading in obese knee osteoarthritis patients. Arthritis. 2011;2011:571519. doi: 10.1155/2011/571519. http://dx.doi.org/10.1155/2011/571519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Akella SV, Regatte RR, Gougoutas AJ, et al. Proteoglycan-induced changes in T1rho-relaxation of articular cartilage at 4T. Magn Reson Med. 2001;46:419–423. doi: 10.1002/mrm.1208. http://dx.doi.org/10.1002/mrm.1208. [DOI] [PubMed] [Google Scholar]
- 3.Alizai H, Nardo L, Karampinos DC, et al. Comparison of clinical semi-quantitative assessment of muscle fat infiltration with quantitative assessment using chemical shift-based water/fat separation in MR studies of the calf of post-menopausal women. Eur Radiol. 2012;22:1592–1600. doi: 10.1007/s00330-012-2404-7. http://dx.doi.org/10.1007/s00330-012-2404-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Andriacchi TP, Mündermann A. The role of ambulatory mechanics in the initiation and progression of knee osteoarthritis. Curr Opin Rheumatol. 2006;18:514–518. doi: 10.1097/01.bor.0000240365.16842.4e. http://dx.doi.org/10.1097/01.bor.0000240365.16842.4e. [DOI] [PubMed] [Google Scholar]
- 5.Bamman MM, Newcomer BR, Larson-Meyer DE, Weinsier RL, Hunter GR. Evaluation of the strength-size relationship in vivo using various muscle size indices. Med Sci Sports Exerc. 2000;32:1307–1313. doi: 10.1097/00005768-200007000-00019. [DOI] [PubMed] [Google Scholar]
- 6.Barrios JA, Davis IS, Higginson JS, Royer TD. Lower extremity walking mechanics of young individuals with asymptomatic varus knee alignment. J Orthop Res. 2009;27:1414–1419. doi: 10.1002/jor.20904. http://dx.doi.org/10.1002/jor.20904. [DOI] [PubMed] [Google Scholar]
- 7.Berry PA, Teichtahl AJ, Galevska-Dimitrovska A, et al. Vastus medialis cross-sectional area is positively associated with patella cartilage and bone volumes in a pain-free community-based population. Arthritis Res Ther. 2008;10:R143. doi: 10.1186/ar2573. http://dx.doi.org/10.1186/ar2573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Blazevich AJ, Coleman DR, Horne S, Cannavan D. Anatomical predictors of maximum isometric and concentric knee extensor moment. Eur J Appl Physiol. 2009;105:869–878. doi: 10.1007/s00421-008-0972-7. http://dx.doi.org/10.1007/s00421-008-0972-7. [DOI] [PubMed] [Google Scholar]
- 9.Buchner DM, Larson EB, Wagner EH, Koepsell TD, de Lateur BJ. Evidence for a non-linear relationship between leg strength and gait speed. Age Ageing. 1996;25:386–391. doi: 10.1093/ageing/25.5.386. http://dx.doi.org/10.1093/ageing/25.5.386. [DOI] [PubMed] [Google Scholar]
- 10.Bullough PG, Munuera L, Murphy J, Weinstein AM. The strength of the menisci of the knee as it relates to their fine structure. J Bone Joint Surg Br. 1970;52:564–567. [PubMed] [Google Scholar]
- 11.Cotofana S, Hudelmaier M, Wirth W, et al. Correlation between single-slice muscle anatomical cross-sectional area and muscle volume in thigh extensors, flexors and adductors of perimenopausal women. Eur J Appl Physiol. 2010;110:91–97. doi: 10.1007/s00421-010-1477-8. http://dx.doi.org/10.1007/s00421-010-1477-8. [DOI] [PubMed] [Google Scholar]
- 12.Foroughi N, Smith R, Vanwanseele B. The association of external knee adduction moment with biomechanical variables in osteoarthritis: a systematic review. Knee. 2009;16:303–309. doi: 10.1016/j.knee.2008.12.007. http://dx.doi.org/10.1016/j.knee.2008.12.007. [DOI] [PubMed] [Google Scholar]
- 13.Fosang A, Baker R. A method for comparing manual muscle strength measurements with joint moments during walking. Gait Posture. 2006;24:406–411. doi: 10.1016/j.gaitpost.2005.09.015. http://dx.doi.org/10.1016/j.gaitpost.2005.09.015. [DOI] [PubMed] [Google Scholar]
- 14.Harridge SD, Kryger A, Stensgaard A. Knee extensor strength, activation, and size in very elderly people following strength training. Muscle Nerve. 1999;22:831–839. doi: 10.1002/(sici)1097-4598(199907)22:7<831::aid-mus4>3.0.co;2-3. http://dx.doi.org/10.1002/(SICI)1097-4598(199907)22:7<831::AIDMUS4>3.0.CO;2-3. [DOI] [PubMed] [Google Scholar]
- 15.Hudelmaier M, Glaser C, Englmeier KH, Reiser M, Putz R, Eckstein F. Correlation of knee-joint cartilage morphology with muscle cross-sectional areas vs. anthropometric variables. Anat Rec A Discov Mol Cell Evol Biol. 2003;270:175–184. doi: 10.1002/ar.a.10001. http://dx.doi.org/10.1002/ar.a.10001. [DOI] [PubMed] [Google Scholar]
- 16.Hudelmaier M, Wirth W, Himmer M, Ring-Dimitriou S, Sänger A, Eckstein F. Effect of exercise intervention on thigh muscle volume and anatomical cross-sectional areas—quantitative assessment using MRI. Magn Reson Med. 2010;64:1713–1720. doi: 10.1002/mrm.22550. http://dx.doi.org/10.1002/mrm.22550. [DOI] [PubMed] [Google Scholar]
- 17.Hunt MA, Hinman RS, Metcalf BR, et al. Quadriceps strength is not related to gait impact loading in knee osteoarthritis. Knee. 2010;17:296–302. doi: 10.1016/j.knee.2010.02.010. http://dx.doi.org/10.1016/j.knee.2010.02.010. [DOI] [PubMed] [Google Scholar]
- 18.Kaya D, Citaker S, Kerimoglu U, et al. Women with patellofemoral pain syndrome have quadriceps femoris volume and strength deficiency. Knee Surg Sports Traumatol Arthrosc. 2011;19:242–247. doi: 10.1007/s00167-010-1290-2. http://dx.doi.org/10.1007/s00167-010-1290-2. [DOI] [PubMed] [Google Scholar]
- 19.Kumar D, Manal KT, Rudolph KS. Knee joint loading during gait in healthy controls and individuals with knee osteoarthritis. Osteoarthritis Cartilage. 2013;21:298–305. doi: 10.1016/j.joca.2012.11.008. http://dx.doi.org/10.1016/j.joca.2012.11.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kumar D, Rudolph KS, Manal KT. EMG-driven modeling approach to muscle force and joint load estimations: case study in knee osteoarthritis. J Orthop Res. 2012;30:377–383. doi: 10.1002/jor.21544. http://dx.doi.org/10.1002/jor.21544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kumar D, Schooler J, Zuo J, et al. Trabecular bone structure and spatial differences in articular cartilage MR relaxation times in individuals with posterior horn medial meniscal tears. Osteoarthritis Cartilage. 2013;21:86–93. doi: 10.1016/j.joca.2012.09.014. http://dx.doi.org/10.1016/j.joca.2012.09.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Li X, Cheng J, Lin K, et al. Quantitative MRI using T1rho and T2 in human osteoarthritic cartilage specimens: correlation with biochemical measurements and histology. Magn Reson Imaging. 2011;29:324–334. doi: 10.1016/j.mri.2010.09.004. http://dx.doi.org/10.1016/j.mri.2010.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Li X, Ma CB, Link TM, et al. In vivo T(1rho) and T(2) mapping of articular cartilage in osteoarthritis of the knee using 3 T MRI. Osteoarthritis Cartilage. 2007;15:789–797. doi: 10.1016/j.joca.2007.01.011. http://dx.doi.org/10.1016/j.joca.2007.01.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lim BW, Hinman RS, Wrigley TV, Sharma L, Bennell KL. Does knee malalignment mediate the effects of quadriceps strengthening on knee adduction moment, pain, and function in medial knee osteoarthritis? A randomized controlled trial. Arthritis Rheum. 2008;59:943–951. doi: 10.1002/art.23823. http://dx.doi.org/10.1002/art.23823. [DOI] [PubMed] [Google Scholar]
- 25.Lim BW, Kemp G, Metcalf B, et al. The association of quadriceps strength with the knee adduction moment in medial knee osteoarthritis. Arthritis Rheum. 2009;61:451–458. doi: 10.1002/art.24278. http://dx.doi.org/10.1002/art.24278. [DOI] [PubMed] [Google Scholar]
- 26.Lohmander LS. Articular cartilage and osteoarthrosis. The role of molecular markers to monitor breakdown, repair and disease. J Anat. 1994;184(pt 3):477–492. [PMC free article] [PubMed] [Google Scholar]
- 27.Maganaris CN, Baltzopoulos V, Tsaopoulos D. Muscle fibre length-to-moment arm ratios in the human lower limb determined in vivo. J Biomech. 2006;39:1663–1668. doi: 10.1016/j.jbiomech.2005.04.025. http://dx.doi.org/10.1016/j.jbiomech.2005.04.025. [DOI] [PubMed] [Google Scholar]
- 28.McCulloch CE, Searle SR, Neuhaus JM. Generalized, Linear, and Mixed Models. 2nd ed. Wiley; Hoboken, NJ: 2008. [Google Scholar]
- 29.Miyazaki T, Wada M, Kawahara H, Sato M, Baba H, Shimada S. Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann Rheum Dis. 2002;61:617–622. doi: 10.1136/ard.61.7.617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Moisio K, Chang A, Eckstein F, et al. Varus-valgus alignment: reduced risk of subsequent cartilage loss in the less loaded compartment. Arthritis Rheum. 2011;63:1002–1009. doi: 10.1002/art.30216. http://dx.doi.org/10.1002/art.30216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Morse CI, Degens H, Jones DA. The validity of estimating quadriceps volume from single MRI cross-sections in young men. Eur J Appl Physiol. 2007;100:267–274. doi: 10.1007/s00421-007-0429-4. http://dx.doi.org/10.1007/s00421-007-0429-4. [DOI] [PubMed] [Google Scholar]
- 32.Mündermann A, Dyrby CO, Andriacchi TP. Secondary gait changes in patients with medial compartment knee osteoarthritis: increased load at the ankle, knee, and hip during walking. Arthritis Rheum. 2005;52:2835–2844. doi: 10.1002/art.21262. http://dx.doi.org/10.1002/art.21262. [DOI] [PubMed] [Google Scholar]
- 33.Mündermann A, Dyrby CO, Hurwitz DE, Sharma L, Andriacchi TP. Potential strategies to reduce medial compartment loading in patients with knee osteoarthritis of varying severity: reduced walking speed. Arthritis Rheum. 2004;50:1172–1178. doi: 10.1002/art.20132. http://dx.doi.org/10.1002/art.20132. [DOI] [PubMed] [Google Scholar]
- 34.Murdock GH, Hubley-Kozey CL. Effect of a high intensity quadriceps fatigue protocol on knee joint mechanics and muscle activation during gait in young adults. Eur J Appl Physiol. 2012;112:439–449. doi: 10.1007/s00421-011-1990-4. http://dx.doi.org/10.1007/s00421-011-1990-4. [DOI] [PubMed] [Google Scholar]
- 35.Narici MV, Hoppeler H, Kayser B, et al. Human quadriceps cross-sectional area, torque and neural activation during 6 months strength training. Acta Physiol Scand. 1996;157:175–186. doi: 10.1046/j.1365-201X.1996.483230000.x. http://dx.doi.org/10.1046/j.1365-201X.1996.483230000.x. [DOI] [PubMed] [Google Scholar]
- 36.Ostchega Y, Dillon CF, Lindle R, Carroll M, Hurley BF. Isokinetic leg muscle strength in older Americans and its relationship to a standardized walk test: data from the National Health and Nutrition Examination Survey 1999-2000. J Am Geriatr Soc. 2004;52:977–982. doi: 10.1111/j.1532-5415.2004.52268.x. http://dx.doi.org/10.1111/j.1532-5415.2004.52268.x. [DOI] [PubMed] [Google Scholar]
- 37.Pan J, Stehling C, Muller-Hocker C, et al. Vastus lateralis/vastus medialis cross-sectional area ratio impacts presence and degree of knee joint abnormalities and cartilage T2 determined with 3T MRI – an analysis from the incidence cohort of the Osteoarthritis Initiative. Osteoarthritis Cartilage. 2011;19:65–73. doi: 10.1016/j.joca.2010.10.023. http://dx.doi.org/10.1016/j.joca.2010.10.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Pandy MG, Andriacchi TP. Muscle and joint function in human locomotion. Annu Rev Biomed Eng. 2010;12:401–433. doi: 10.1146/annurev-bioeng-070909-105259. http://dx.doi.org/10.1146/annurev-bioeng-070909-105259. [DOI] [PubMed] [Google Scholar]
- 39.Pearle AD, Warren RF, Rodeo SA. Basic science of articular cartilage and osteoarthritis. Clin Sports Med. 2005;24:1–12. doi: 10.1016/j.csm.2004.08.007. http://dx.doi.org/10.1016/j.csm.2004.08.007. [DOI] [PubMed] [Google Scholar]
- 40.Peterfy CG, Guermazi A, Zaim S, et al. Whole-Organ Magnetic Resonance Imaging Score (WORMS) of the knee in osteoarthritis. Osteoarthritis Cartilage. 2004;12:177–190. doi: 10.1016/j.joca.2003.11.003. http://dx.doi.org/10.1016/j.joca.2003.11.003. [DOI] [PubMed] [Google Scholar]
- 41.Petterson SC, Barrance P, Buchanan T, Binder-Macleod S, Snyder-Mackler L. Mechanisms underlying quadriceps weakness in knee osteoarthritis. Med Sci Sports Exerc. 2008;40:422–427. doi: 10.1249/MSS.0b013e31815ef285. http://dx.doi.org/10.1249/MSS.0b013e31815ef285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Rauscher I, Stahl R, Cheng J, et al. Meniscal measurements of T1rho and T2 at MR imaging in healthy subjects and patients with osteoarthritis. Radiology. 2008;249:591–600. doi: 10.1148/radiol.2492071870. http://dx.doi.org/10.1148/radiol.2492071870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Regatte RR, Akella SV, Lonner JH, Kneeland JB, Reddy R. T1rho relaxation mapping in human osteoarthritis (OA) cartilage: comparison of T1rho with T2. J Magn Reson Imaging. 2006;23:547–553. doi: 10.1002/jmri.20536. http://dx.doi.org/10.1002/jmri.20536. [DOI] [PubMed] [Google Scholar]
- 44.Riddle DL, Stratford PW. Impact of pain reported during isometric quadriceps muscle strength testing in people with knee pain: data from the Osteoarthritis Initiative. Phys Ther. 2011;91:1478–1489. doi: 10.2522/ptj.20110034. http://dx.doi.org/10.2522/ptj.20110034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Seedhom BB, Dowson D, Wright V. Proceedings: functions of the menisci. A preliminary study. Ann Rheum Dis. 1974;33:111. doi: 10.1136/ard.33.1.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Sharma L, Hurwitz DE, Thonar EJ, et al. Knee adduction moment, serum hyaluronan level, and disease severity in medial tibiofemoral osteoarthritis. Arthritis Rheum. 1998;41:1233–1240. doi: 10.1002/1529-0131(199807)41:7<1233::AID-ART14>3.0.CO;2-L. http://dx.doi.org/10.1002/1529-0131(199807)41:7<1233::AID-ART14>3.0.CO;2-L. [DOI] [PubMed] [Google Scholar]
- 47.Shelburne KB, Torry MR, Pandy MG. Contributions of muscles, ligaments, and the ground-reaction force to tibiofemoral joint loading during normal gait. J Orthop Res. 2006;24:1983–1990. doi: 10.1002/jor.20255. http://dx.doi.org/10.1002/jor.20255. [DOI] [PubMed] [Google Scholar]
- 48.Shrive NG, O'Connor JJ, Goodfellow JW. Load-bearing in the knee joint. Clin Orthop Relat Res. 1978:279–287. [PubMed] [Google Scholar]
- 49.Sipilä S, Elorinne M, Alen M, Suominen H, Kovanen V. Effects of strength and endurance training on muscle fibre characteristics in elderly women. Clin Physiol. 1997;17:459–474. doi: 10.1046/j.1365-2281.1997.05050.x. [DOI] [PubMed] [Google Scholar]
- 50.Sogabe A, Mukai N, Miyakawa S, et al. Influence of knee alignment on quadriceps cross-sectional area. J Biomech. 2009;42:2313–2317. doi: 10.1016/j.jbiomech.2009.06.022. http://dx.doi.org/10.1016/j.jbiomech.2009.06.022. [DOI] [PubMed] [Google Scholar]
- 51.Souza RB, Baum T, Wu S, et al. Effects of unloading on knee articular cartilage T1rho and T2 magnetic resonance imaging relaxation times: a case series. J Orthop Sports Phys Ther. 2012;42:511–520. doi: 10.2519/jospt.2012.3975. http://dx.doi.org/10.2519/jospt.2012.3975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Souza RB, Fang C, Luke A, Wu S, Li X, Majumdar S. Relationship between knee kinetics during jumping tasks and knee articular cartilage MRI T1rho and T2 relaxation times. Clin Biomech (Bristol, Avon) 2012;27:403–408. doi: 10.1016/j.clinbiomech.2011.10.015. http://dx.doi.org/10.1016/j.clinbiomech.2011.10.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Subburaj K, Kumar D, Souza RB, et al. The acute effect of running on knee articular cartilage and meniscus magnetic resonance relaxation times in young healthy adults. Am J Sports Med. 2012;40:2134–2141. doi: 10.1177/0363546512449816. http://dx.doi.org/10.1177/0363546512449816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Thorp LE, Sumner DR, Block JA, Moisio KC, Shott S, Wimmer MA. Knee joint loading differs in individuals with mild compared with moderate medial knee osteoarthritis. Arthritis Rheum. 2006;54:3842–3849. doi: 10.1002/art.22247. http://dx.doi.org/10.1002/art.22247. [DOI] [PubMed] [Google Scholar]
- 55.Vanwanseele B, Eckstein F, Smith RM, et al. The relationship between knee adduction moment and cartilage and meniscus morphology in women with osteoarthritis. Osteoarthritis Cartilage. 2010;18:894–901. doi: 10.1016/j.joca.2010.04.006. http://dx.doi.org/10.1016/j.joca.2010.04.006. [DOI] [PubMed] [Google Scholar]
- 56.Walter JP, D'Lima DD, Colwell CW, Jr., Fregly BJ. Decreased knee adduction moment does not guarantee decreased medial contact force during gait. J Orthop Res. 2010;28:1348–1354. doi: 10.1002/jor.21142. http://dx.doi.org/10.1002/jor.21142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Willén C, Sunnerhagen KS, Ekman C, Grimby G. How is walking speed related to muscle strength? A study of healthy persons and persons with late effects of polio. Arch Phys Med Rehabil. 2004;85:1923–1928. doi: 10.1016/j.apmr.2003.11.040. [DOI] [PubMed] [Google Scholar]
- 58.Winby CR, Lloyd DG, Besier TF, Kirk TB. Muscle and external load contribution to knee joint contact loads during normal gait. J Biomech. 2009;42:2294–2300. doi: 10.1016/j.jbiomech.2009.06.019. http://dx.doi.org/10.1016/j.jbiomech.2009.06.019. [DOI] [PubMed] [Google Scholar]
- 59.Yang NH, Nayeb-Hashemi H, Canavan PK, Vaziri A. Effect of frontal plane tibiofemoral angle on the stress and strain at the knee cartilage during the stance phase of gait. J Orthop Res. 2010;28:1539–1547. doi: 10.1002/jor.21174. http://dx.doi.org/10.1002/jor.21174. [DOI] [PubMed] [Google Scholar]
- 60.Yusuf E, Bijsterbosch J, Slagboom PE, Rosendaal FR, Huizinga TW, Kloppenburg M. Body mass index and alignment and their interaction as risk factors for progression of knees with radiographic signs of osteoarthritis. Osteoarthritis Cartilage. 2011;19:1117–1122. doi: 10.1016/j.joca.2011.06.001. http://dx.doi.org/10.1016/j.joca.2011.06.001. [DOI] [PubMed] [Google Scholar]
- 61.Zarins ZA, Bolbos RI, Pialat JB, et al. Cartilage and meniscus assessment using T1rho and T2 measurements in healthy subjects and patients with osteoarthritis. Osteoarthritis Cartilage. 2010;18:1408–1416. doi: 10.1016/j.joca.2010.07.012. http://dx.doi.org/10.1016/j.joca.2010.07.012. [DOI] [PMC free article] [PubMed] [Google Scholar]