

Abstract
Background:
Trauma leads to considerable morbidity and mortality. The aim of this study is to elucidate the pattern and characteristics of trauma at Benue State University Teaching Hospital (BSUTH), Makurdi, Nigeria.
Materials and Methods:
Case records of all patients who presented to the Accident and Emergency (A and E) Department with trauma between January and December 2013 were analyzed for demographic data, types of injuries sustained, causes and circumstances of injuries, as well as outcome of treatment were extracted from the case files and entered onto a computerized questionnaire. Data were analyzed using the software Statistical Package for Social Sciences for Windows version 15.0 (SPSS Inc; Chicago, Illinois).
Results:
A total of 250 traumatized patients were studied consisting of 203 (81.2%) males and 47 (18.8%) females with a modal age group of 21–30 years. Unintentional injuries were the most predominant form of trauma (n = 209, 83.6%) with road traffic accidents being the leading cause (n = 180, 72.0%). Open wounds (n = 95, 28.2%) were the most common form of injury sustained and the extremities (n = 148, 43.5%), the most frequently injured body region. Most patients (n = 133, 53.2%) were treated and discharged home without permanent disabilities, while death occurred in 15.2%.
Conclusion:
Trauma in Makurdi is a predominantly young adult male occurrence with road traffic accidents being the leading etiological factor. Reducing road traffic accidents will likely reduce mortality and morbidity due to trauma.
Keywords: Injuries, Makurdi, Nigeria, road traffic accidents, trauma
INTRODUCTION
Trauma is no more considered accidental but a preventable epidemic with a unique pattern of host, agent, and environment working in unison to produce injury.[1] Traumatic injuries are associated with significant morbidity and mortality and are of particular relevance currently with technological sophistication in all spheres of life and upsurge in armed conflicts globally. An injury is said to be a bodily lesion at organic level resulting from acute exposure to energy in amounts that exceeds the threshold of physiologic tolerance or the absence of such essentials as heat or oxygen.[2]
Injuries accounted for 16% of the global burden of disease and an estimated 5.8 million deaths in 1998 with injury-related mortality predicted to increase by 40% between 2002 and 2030.[2,3] Mortality statistics, in isolation, do not adequately depict the magnitude of injury as for each death there are many more injuries that resulted in hospitalization, treatment in emergency departments, treatment by practitioners outside the formal health sector, or never received treatment at all.[4] To accurately characterize the burden of injury, nonfatal outcomes are also measured by using disability-adjusted life years (DALYs) which combine the number of years of life lost from premature death with the loss of health from disability among persons with nonfatal injuries.[2]
Patterns and causes of trauma differ from place to place. Road traffic accidents, falls, assaults, firearm injuries, burns, sports injuries, animal bites, and industrial accidents are some causes of of trauma.[5,6] Road traffic accidents are the most common in most studies.[5,6,7] Deaths from road traffic accidents are predicted to increase from 1.2 million in 2002 to 1.9 million in 2020 globally, to become the third leading cause of DALYs losses.[8] Increasing waves of terrorism and civil conflicts are expected to lead to a surge in violence-related injuries.
Trauma care in most developing nations is at infancy level despite the fact that about 90% of injury deaths occur in these nations.[2] Dearth of trauma centers, nonexistent ambulance services and prehospital care, and unavailability of data on trauma are some of the impediments to trauma management in Nigeria. Trauma has been recognized to be preventable over the past few decades and methods for the scientific study of injury prevention have been established.[2] However, the development of effective trauma prevention measures depends on reliable and detailed information on the characteristics and pattern of injury. The aim of this study is to elucidate the pattern and characteristics of trauma at Benue State University Teaching Hospital (BSUTH), Makurdi, Nigeria.
MATERIALS AND METHODS
Study design and setting
This was a hospital-based study of trauma patients of all age groups and gender who presented to the Accident and Emergency (A and E) Department of BSUTH, Makurdi, Nigeria from January to December 2013. BSUTH is a tertiary care and teaching hospital for the Benue State University and is located along the shores of River Benue. There is no trauma center in the city as such most seriously injured patients are referred to the facility. It provides trauma care for inhabitants of the city and surrounding areas of north central Nigeria.
Study population
The case records of all patients seen with injuries at the A and E Department during the study period were retrieved. Demographic data, types of injuries sustained, causes and circumstances of injuries, as well as outcome of treatment were extracted from the case files and entered onto a computerized questionnaire.
Statistical analysis
Data were analyzed using the software Statistical Package for Social Sciences for Windows version 15.0 (SPSS Inc; Chicago, Illinois). Descriptive statistics were used to display single variable quantities using means and standard deviations (SD) for continuous variables or proportions for categorical variables unless otherwise stated.
RESULTS
Demographic data
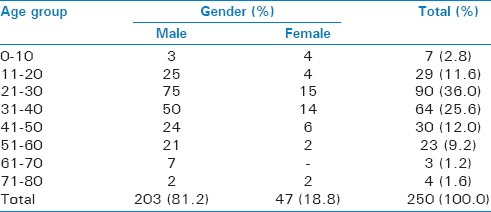
A total of 250 patients were included in the study. There were 203 (81.2%) males and 47 (18.8%) females with a male to female ratio of 4.3:1. Their ages ranged from 3 to 74 years with a mean of 32 ± 13.1 years. The modal age group was 21–30 years. Table 1 shows the sex distribution of patients with respect to age groups.
Table 1.
Sex distribution of patients with respect to age groups
Circumstances of injury
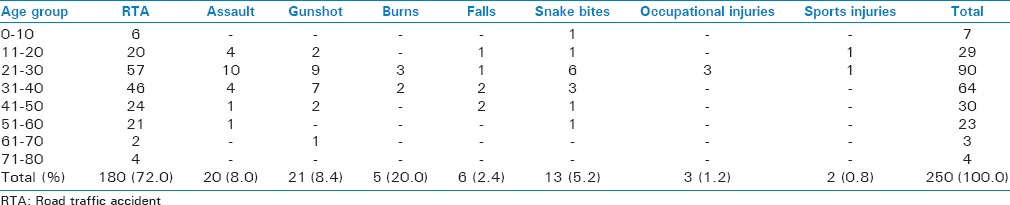
Unintentional injuries were the predominant form of trauma (n = 209, 83.6%). Road traffic accidents were the most common cause (n = 180, 72.0%). This was followed by gunshot injuries (n = 21, 8.4%) and assault (n = 20, 8.0%). Table 2 shows the etiologies of trauma with respect to age groups.
Table 2.
Etiologies of trauma with respect to age groups
The extremities were the most commonly injured body region (n = 148, 43.5%). This was followed by the head (n = 112, 32.9%), chest (n = 46, 13.5%), abdomen (n = 16, 4.7%), spine (n = 10, 2.9%), and pelvis (n = 8, 2.4%). Open wounds (abrasions and lacerations) were the most common injury type sustained (n = 95, 28.2%). Table 3 shows the distribution of injuries sustained by trauma patients. Isolated injuries occurred in 166 (66.4%) patients, while 84 (33.6%) patients were multiply-injured. One hundred and twenty-one patients (48.8%) sustained severe/profound injuries.
Table 3.
Distribution of injuries sustained by patients
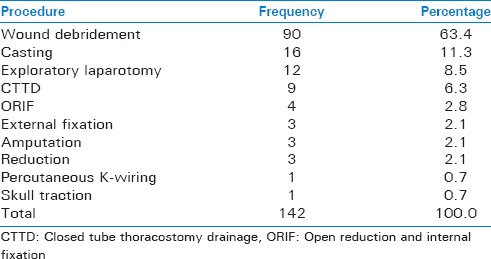
The majority of patients (n = 138, 55.2%) were admitted and treated in the A and E, 110 (44.0%) in the general/pediatric surgical and orthopedic wards and two (0.8%) in the intensive care unit. Of the 250 patients, 142 were treated surgically of which surgical wound debridement (n = 90, 63.3%) was the most common procedure carried out. Table 4 shows the distribution of patients according to surgical procedures done. Length of hospital stay ranged between 1 and 160 days with a mean duration of about 8 days.
Table 4.
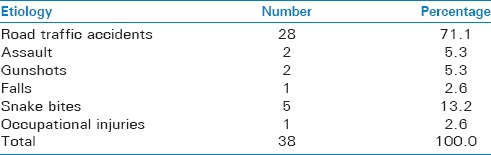
Mortality pattern of traumatized patients
Outcome
Majority of patients (n = 133, 53.2%) were treated and discharged without permanent disability. Eleven (4.4%) were discharged with permanent disability (paraplegia, limb loss, etc.), 56 (22.4%) opted for discharge against medical advice, while 12 (4.8%) were referred. Thirty-eight patients died giving a death rate of 15.2%. Snake bites were the most fatal with 38.4% of patients expiring. Table 4 shows the mortality pattern of trauma patients.
DISCUSSION
The burden of trauma in this study is mostly borne by young males, a finding similar to those from other studies.[3,7,9] Male predominance is likely to be due to the fact that males are more involved in risk-taking activities and more exposed to the elements being the main revenue-earners in families. Involvement of the active and productive segment of the society suggests huge losses to the economy. The impact of trauma on this group may be reduced by incorporating preventive measures into children's school curriculum so as to particularly target boys in their formative years.
Road traffic injuries are a major cause of death and disability globally, with a disproportionate number occurring in developing countries.[10] They were the leading cause of injury in this study in a similar manner to a number of studies[5,6,7,9] and accounted for over 70% of the mortality. Developing countries accounted for more than 85% of all deaths due to road traffic crashes globally in 1998. Reasons put forward for this high burden of road traffic accidents in developing countries include growth in motor vehicle numbers, poor enforcement of traffic safety regulations, and poor access to health services.[10]
Passengers and pedestrians constituted the majority of road traffic injured patients in this study in keeping with studies from other developing countries.[5,11] This is in contradistinction to findings from the United states where drivers are the majority of the injured.[10] This may be because of frequent crashes involving multi-passenger vehicles like buses and trucks as well as nonexistent pedestrian walkways on most roads in low-income countries.
Firearms are the most destructive of readily available weapons in modern society and injuries resulting from them are associated with a high morbidity and mortality.[12,13] Firearm injuries were the second leading cause of trauma in this study constituting over 20% of overall causes. This figure is much higher than Thanni et al.,[1] and Wolde et al.,[4] reported. The high rate of gunshot injuries in this study is likely to be due to an armed conflict between nomadic herdsmen and local farmers over rights to grazing land in the study area. Designating special grazing zones along the seasonal migration route of the herdsmen and establishing open channels for conflict resolution may go a long way to help mitigate future occurrences.
Snake bites constituted the most fatal of all the causes of trauma in this study with about 40% mortality rate. Most patients got bitten while working on farms in remote areas and late presentation to hospital prevented early institution of treatment. Provision of personnel and facilities to administer anti-snake venom at primary healthcare centers in the countryside before referral to tertiary centers may help improve the outcome of treatment.
The overall death rate was higher than findings in other studies.[1,4,14] About half of the deaths were as a result of head injuries. Use of approved safety helmets by at-risk individuals like construction workers and motorcyclists is known to reduce the incidence traumatic head injury. In fact, severe head injury among motorcyclists is said to be a reflection of low usage of helmets.[15] The high mortality from head injuries in this study may be due to the culture of poor usage of safety helmets that is prevalent in developing countries.[15,16] Stricter enforcement of safety measures on the roads and workplaces may help.
CONCLUSION
Trauma in Makurdi is a predominantly young adult male occurrence with road traffic accidents being the leading etiological factor. Head injuries were the most important cause of mortality. Reducing road traffic accidents will likely reduce mortality and morbidity due to trauma.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Thanni LO, Kehinde OA. Trauma at a Nigerian teaching hospital: Pattern and documentation of presentation. Afr Health Sci. 2006;6:104–7. doi: 10.5555/afhs.2006.6.2.104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Krug EG, Sharma GK, Lozano R. The global burden of injuries. Am J Public Health. 2000;90:523–6. doi: 10.2105/ajph.90.4.523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Peden M, McGee K, Sharma G. Geneva: World Health Organization; 2002. The injury chart book: A graphical overview of the global burden of injuries. [Google Scholar]
- 4.Wolde A, Abdella K, Ahmed E, Tsegaye F, Babaniyi OA, Kobusingye O, et al. Pattern of Injuries in Addis Ababa, Ethiopia: A one-year descriptive study. East Central Afr J Surg. 2008;13:14–22. [Google Scholar]
- 5.Chalya PL, Dass RM, Mchembe MD, Mbelenge N, Ngayomela IH, Chandika AB, et al. Citywide trauma experience in Mwanza, Tanzania: A need for urgent intervention. J Trauma Manag Outcomes. 2013;7:9. doi: 10.1186/1752-2897-7-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Demyttenaere SV, Nansamba C, Nganwa A, Mutto M, Lett R, Razek T. Injury in Kampala, Uganda: 6 years later. Can J Surg. 2009;52:E146–50. [PMC free article] [PubMed] [Google Scholar]
- 7.Tadesse B, Tekilu S, Nega B, Seyoum N. Pattern of injury and associated variables as seen in the emergency department at Tikur Anbessa specialized referral hospital, Addis Ababa, Ethiopia. East Central Afr J Surg. 2014;19:73–82. [Google Scholar]
- 8.Murray CJ, Lopez AD, Jamison DT. The global burden of disease in 1990: Summary results, sensitivity analysis and future directions. Bull World Health Organ. 1994;72:495–509. [PMC free article] [PubMed] [Google Scholar]
- 9.Swarnkar M, Singh P, Dwivedi S. Pattern of trauma in central India: An epidemiological study with special reference to mode of injury. Internet J Epidemiol. 2009;9 [Google Scholar]
- 10.Nantulya VM, Reich MR. The neglected epidemic: Road traffic injuries in developing countries. BMJ. 2002;324:1139–41. doi: 10.1136/bmj.324.7346.1139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Banthia P, Koirala B, Rauniyar A, Chaudhary D, Kharel T, Khadka SB. An epidemiological study of road traffic accident cases attending emergency department of teaching hospital. JNMA J Nepal Med Assoc. 2006;45:238–43. [PubMed] [Google Scholar]
- 12.Mohammed AZ, Edino ST, Ochicha O, Umar AB. Epidemiology of gunshot injuries in Kano, Nigeria. Niger J Surg Res. 2005;7:296–9. [Google Scholar]
- 13.Gotsch KE, Annest JL, Mercy JA, Ryan GW. Surveillance for fatal and nonfatal firearm-related injuries - United States, 1993—1998. Center for Disease Control. [Last accessed on 2014 Mar 22]. Available from: http://www.cdc.gov/mmwr/preview/mmwrhtml/ss5002a1.htm#top .
- 14.Woldemichael K, Berhanu N. Magnitude and pattern of injury in Jimma University Specialized Hospital, South West Ethiopia. Ethiop J Health Sci. 2011;21:155–65. [PMC free article] [PubMed] [Google Scholar]
- 15.Oluwadiya KS, Oginni IM, Olasinde AA, Fadiora SO. Motorcycle limb injuries in a developing country. West Afr J Med. 2004;23:42–7. doi: 10.4314/wajm.v23i1.28080. [DOI] [PubMed] [Google Scholar]
- 16.Nzegwu MA, Aligbe JU, Banjo AA, Akhiwui W, Nzegwu CO. Patterns of morbidity and mortality amongst motorcycle riders and their passengers in Benin-city Nigeria: One-year review. Ann Afr Med. 2008;7:82–5. doi: 10.4103/1596-3519.55675. [DOI] [PubMed] [Google Scholar]