

Abstract
Background:
Obesity in adolescence is crucial as it represents an important stage in human life. Dietary habits are greatly associated with lifestyle. Many reports suggested direct relationship between adolescent fatness and increased risk of cardiovascular diseases (CVD) which will be found in young adult population.
Aim:
Determine the prevalence of overweight and obesity among male adolescents in Arar city, Saudi Arabia (KSA). We estimated the future risk of developing cardiovascular diseases in this age‐group and its possible correlation to different lifestyles and dietary habits.
Results:
A total of 523 male students with a mean age of 16.7 ± 0.9 years participated in the current study in which 30.4% of those students were obese and 17.2% were overweight. A direct relationship was found between body weight and different dietary and lifestyle habits. The risk of CVD based on waist height ratio (WHtR) was found in 33.5% of participants (30.4% obese, 2.1% overweight and 1% normal weight); moreover, the risk of CVD was strongly related to different dietary and lifestyle habits.
Conclusion:
Overweight and obesity were high among adolescent male students in Arar, who became susceptible to the risk of CVD. Arar showed the highest rate of obesity all over KSA. Both obesity and risk of CVD were strongly related to bad dietary habits and lifestyle.
Keywords: Cardiovascular, disease, lifestyle, obesity
Introduction
Obesity is an important public health problem. Its prevalence is increasing in both developed and developing nations.(1) In many countries the problem of childhood obesity is worsening at a dramatic rate.(2) All over the world, there are a total 155 million children overweight, and 30-45 million classified as obese.(3) In the Kingdom of Saudi Arabia (KSA), one in every six children aged 6-18-years-old is obese(4), but information on regional differences is scanty.(5) Obesity of adolescents is very important as adolescence represents a crucial stage in human life during which lifestyles are formed and become established. Dietary habits appear to be established in close association with lifestyle.(6) In addition, the greatest health problems in this age-group will be found in young adult populations. Finally, costs to the health services and the burden carried by the individuals involved will be other great problems.(2) Many reports suggested direct relationship between adolescent fatness and increased risk of cardiovascular diseases (CVD) and diabetes.(2,7,8,9) A better understanding of the relationship between body mass index (BMI) and different dietary habits and lifestyles among young people is very important for effective prevention of CVD. The aim of the present study was to determine the prevalence of overweight and obesity among male adolescent students in Arar city, KSA. We studied the association between BMI and different lifestyles and dietary habits. Finally, we estimated the future risk of developing cardiovascular diseases in this age-group and its possible correlation to different lifestyles and dietary habits.
Materials and Methods
Study design
A cross-sectional study was conducted on 523 male adolescent students who were randomly selected from different schools in Arar, a city formed of about 240000 inhabitants and lying in the northern borders region of KSA. This study was conducted over a two month period (March and April 2012).
Written consents were taken from the students and their parents according to the World Medical Association (WMA) Declaration of Helsinki Sixth revision guide lines(10) and following the guidelines of ethical research committee in Northern Borders University. Students with any form of obesity other than exogenous dietetic had been excluded.
Data collection
Questionnaire and anthropometric measurements were used for data collection.
Questionnaires were conducted on different dietary habits and lifestyles. The dietary habit questionnaire included number of meal/day, daily skipping breakfast, drinking coke, and weekly eating fast food. In addition, the daily eating snacks and junk food as well as vegetables and fruits was also recorded. The lifestyle questionnaire was about the exercise practicing hours, and TV watching hours at both school days and weekend.
Anthropometric measurements
Weight was measured in light clothing to the nearest 0.1 Kg using a digital balance. Two measures were taken and the mean was used.(11) Waist circumference (WC) was measured using a non-elastic flexible tape. The height was measured without shoes using a portable stadiometer to the nearest centimetre. WC was measured twice at midpoint between iliac crest and lower border of the tenth rib directly against the skin without compressing the skin while the students were standing.(11,12) Waist to height ratio (WHtR) was calculated as the ratio of waist (cm) to height (cm). The cut-off point for a WHtR was 0.5 for both adult and children.(13) Students who exceeded 0.5 were considered to be “at risk” of CVD.(14)
Adolescents’ BMI was calculated as weight/height2, with weight being in kilograms and height being in meters.(15) The 2000 center for disease control (CDC) growth reference and related software were used to determine the corresponding BMI-for-age and sex. The CDC cut-offs were used for the definition of prevalence of overweight and obesity (overweight was defined as BMI ≥85-95 percentile and obesity was defined as a BMI ≥95 percentile).(16)
Statistical analysis
The statistical analysis was conducted using SPSS program version 20. Frequency counts (%), mean, standard deviation (SD), and standard error (SE) were calculated for all variables. The categorical variables were analysed by using the Chi-square test (cross tab). Multiple logistic regression analysis of the risk of developing CVD (dependable variable) versus predictor variables was done. It was chosen as the dependent variable was dichotomous. The specific logistic regression equation fitted to the data was: Logit (risk of developing cardiovascular disease) = bo + b1 (TV watching in ordinary day) + b2 (TV watching in weekend) + b3 (exercise activity) + b4 (snack food) + b5 (fruits eating) + b6 (vegetables eating) + b7 (eating junk food) + b8 (drinking coke) + b9 (fast food) + b10 (skipping breakfast) + b11 (number of meals). (Where b0 is a constant. b1 to b11 are logistic coefficients or estimates for the parameters 1-11). All statistical tests used were two-sided with a type I error (α) of 0.05, and P values < 0.05 were considered statistically significant.
Results
Demographic data
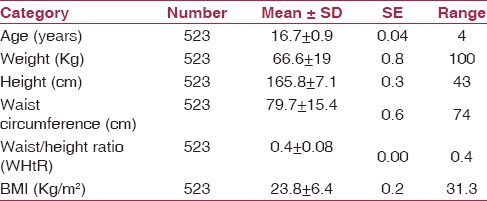
A total of 523 male students participated in the current study, with a mean age of 16.7 ± 0.9 years ranging from 15-19 years. Their mean weight, height and waist circumference were 66.6 ± 19 Kg, 165.8 ± 7.1 cm and 79.7 ± 15.4 cm respectively. Finally, their mean BMI and WHtR were 23.8 ± 6.4 Kg/m2 and 0.4 ± 0.08 respectively [Table 1].
Table 1.
Demographic characteristics of the studied students
BMI and indicators of central obesity
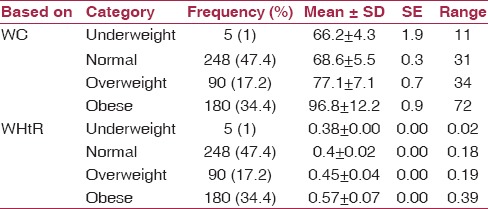
Based on BMI CDC centiles categories, 1% of the sharing students were underweight (their WC and WHtR means were 66.2 ± 4.3 cm and 0.38 ± 0.00 respectively). 47.4% of the students were normal (their WC and WHtR means were 68.6 ± 5.5 cm and 0.4 ± 0.02 respectively). 17.2% were overweight (their WC, and WHtR means were 77.1 ± 7.1 cm, and 0.45 ± 0.04 respectively). Finally 34.4% were obese (their WC, and WHtR means were 96.8 ± 12.2 cm, and 0.57 ± 0.07 respectively) [Table 2].
Table 2.
WC, WHR and WHtR in the different CDC centiles groups
Dietary habits and lifestyles
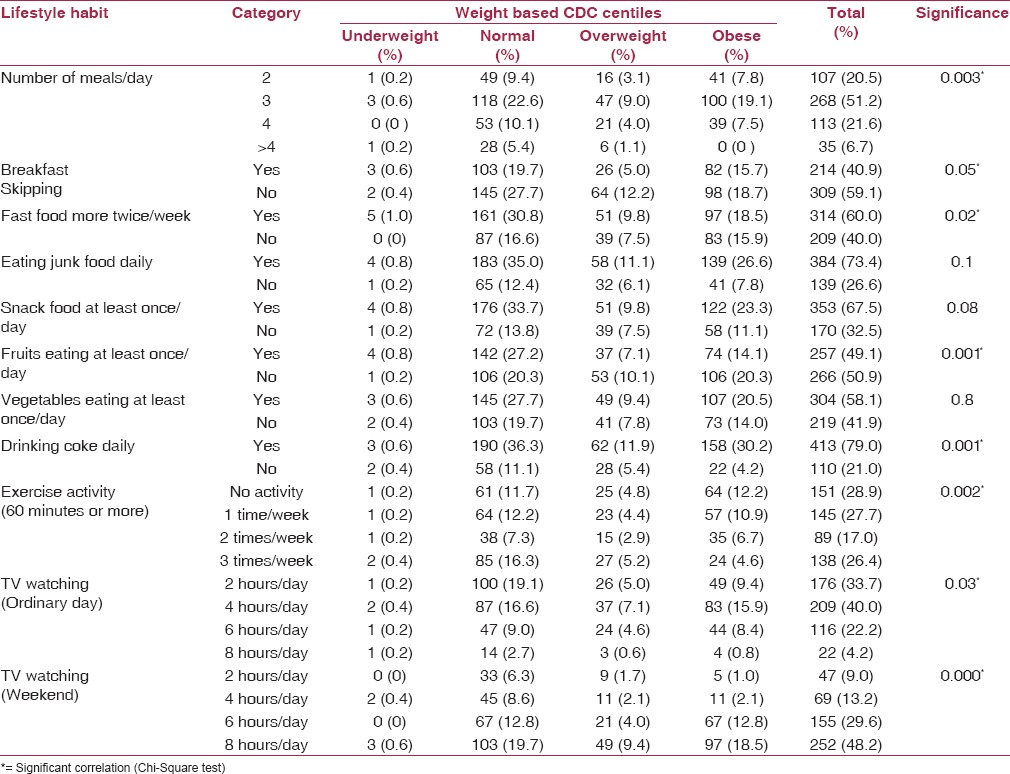
Concerning the number of daily meals, more than half of the students (51.2%) of the four centile groups (underweight, normal, overweight and obese) were eating three meals/day, 20.5% and 21.6% were eating two and four meals/day respectively, and only 6.7% were eating more than four meals/day (P < 0.05). Skipping breakfast was present in 40.9% of the participants while 60% were eating fast food more than twice /week, and this was statistically significant (P < 0.05). Among our students, 73.4%, 67.5, 49.1% and 58.1% were respectively eating junk food, snack food, fruits and vegetables at least once/day. All these habits, away from fruit eating, were statistically insignificant (P > 0.05). The majority of them were significantly drinking coke daily (79%). Lack of exercise activity was found in a significant number of participants (28.9%) and presented mainly in the obese group (12.2%) followed by the normal group (11.7%). One of the constant significant daily activities for all the students was T.V watching. The number of hours for the majority (40%) was 4 hours during the school days, which was increased at the weekend to become 8 hours (48.2%) [Table 3].
Table 3.
Correlations between CDC centile groups and different dietary and lifestyle habits
Risk of development of CVD
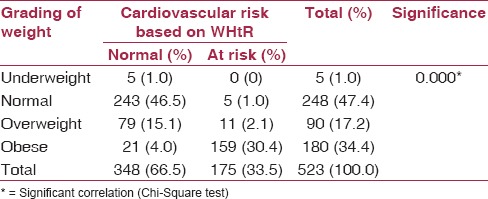
A positive highly significant correlation (P = 0.000) was found between the different CDC centile groups and the cardiovascular risk based on WHtR in which nearly one third of the shared students (33.5%) were at risk of developing CVD (30.4% were of the obese students, 2.1% and 1% were of the overweight and normal ones) [Table 4].
Table 4.
Risk of development of cardiovascular disease based WHtR
Cardiovascular risk and dietary habits and lifestyles
The results of the binary logistic regression analysis show that all the independent variables together was statistically significant, X2 = 85.3, df = 11, P = 0.000. Of the all independent variables, only TV watching (weekend), exercise activity, fruits eating, drinking coke, fast food eating and the number of meals were significantly predict current risk of developing cardiovascular disease (dependable variable) [Table 5].
Table 5.
Multiple logistic regression analysis of cardiovascular risk (dependent variable) versus predictors’ variables
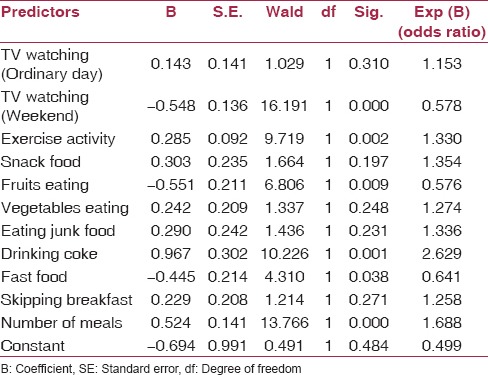
The study correctly classified 70.4% of the cases. The “pseudo” R estimates indicated that the current study explained between 15.1% (Cox & Snell R Squared) and20.9% (Nagelkerke R Squared) of the variance in the frequent risk of developing cardiovascular diseases. Table 5 presented a summary of the raw score binary logistic regression coefficients, Wald statistics and odds ratios [(Exp (B)]. Wald statistics indicated that indicated the variables significantly predict the risk of the cardiovascular diseases.
Discussion
The prevalence of overweight and obesity in KSA is well-documented, but there is an obvious lack of information on regional differences.(5) Arar is a city in the northern borders region in KSA with a population of about 240000 inhabitants. Up to our knowledge no previous detailed research conducted on overweight and obesity in this region at any age. The only study was conducted on this region was a part of study of three regions in KSA and was concerned only with the prevalence of obesity and overweight; its age range was very wide (1-18 years) and was conducted on both sex.(5) The privilege of our current study was its narrow age range (15-19 years) and this age is nearer to adult age so we studied their future dietary habits and lifestyles. In addition, the CVD health problem in the future adult can be estimated. Our second concern was only the male adolescents as many authors reported the lower rate of obesity among female students and they attributed this finding to the concern of females with their body images during adolescence.(17) A great percentage of the students (51.6%) sharing in the current study had BMI exceeding its normal level (17.2% and 34.4% for overweight and obesity respectively). The combined overweight and obesity in Arar is the highest when compared to other regions in KSA (24.8% and 13.1% for overweight and obesity in the central region) and (16.9% and 9.6% for overweight and obesity in the south west region).(5) In addition, the obesity among our studied students and to little extent overweight exceeded their matched age and sex of other gulf countries (21% for obesity in Bahrain; 30% and 14.7% for overweight and obesity in Kuwait and only 4.3% and 2.5% in Iran).(3) More than half of the shared students (51.2%) were eating 3 meals/day, and only 28.3 % were eating ≥4 meals/day. So it seems that gaining weight is related to quality rather than quantity of the diet meals. Compared with the Dietary Reference Intake, carbohydrate and fat intakes in Saudi diet were higher.(18) In addition, 50.9% and 41.9% of the students in our study neglected eating fruits and vegetables daily; most of them were of the combined overweight and obesity categories (30.4% and 21.8% respectively). Vegetables and fruits are low in energy density. Therefore, adding them to a diet reduces its overall energy intake.(19) Moreover, fruits are taken as a dessert, so they lose their satiety effect.(20) Other unhealthy bad dietary habits among the sharing students were skipping breakfast and taking fast food more than twice/week (40.9% and 60% respectively); 50% of the former and 47% of the later were belonging to the overweight and obese groups. Moreover, 73.4% and 67.5% respectively of the students were eating junk food and snack food daily. Finally, 79.0% of them (42.1% of the combined obesity and overweight) were drinking coke daily. All these habits might be a reflection to the economic development of KSA during the last three decades.(21) Food become more affordable to larger number as the price has decreased, and the concept of food has changed to a marker of lifestyle and a source of pleasure.(21) Another obvious cause to the high percentage of obesity observed in the current study was the lacking of exercise practice observed in 28.9% of the students, the rest of them were practicing exercises 1-3 times/week. The previous physical activity levels did not meet the minimal weekly needed hours to enhance health.(22) Combined with all these, all the students were either watching TV at least 2 hours/day. At the ordinary days, the average watching hours were 4 hours/day, increasing to become 8 hours/day for the majority (48.2%) at weekends. Watching TV more than 2 hours/day is associated with consuming higher amounts snack foods and soft drinks, as well as consuming more calories during snacks.(23) There is debating in the literature about the association between TV watching and pediatric overweight or obesity; some authors found a significant association(24); others found no significant association.(25) In our study the association was highly significant especially in the weekend. In addition, TV watching promotes a sedentary lifestyle by infringing on the time available for physical activity.(23) Nearly third of the shared students (33.5%) were at a risk of the development of CVD (30.4% were of the obese students, 2.1% and 1 % were of the overweight and normal ones). Because childhood obesity persists into adulthood, a rising number of adults will be at increased risk of CVD.(26) In the current study, the risk of development of CVD had no significant associations to skipping breakfast, snack food eating or vegetable eating habits. On the other hand, we found that the risk for development CVD had significant increased with those who were eating fast food, junk food, and drinking coke.
The highest percentage of the students (18.5%) who were at risk of CVD were those eating three meals/day, so CVD risk seems to be related to quality rather than quantity of meal. Contrary to that, fruits seem to protect against the CVD risk(20) as the risk decreased to 13.2% among the students eaters compared to 20.3% of the non-eaters. Many researchers have shown positive associations between prolonged television viewing and obesity and health conditions.(23) The risk of CVD in the current study increased significantly with the increase TV watching/computer working hours. The risk of 6 and 8 hours was very high (12.4% and 18.4%) when compared with that of 2 and 4 hours (0.8% and 1.9%).
The higher percentage of the students at a risk of CVD (12.6%) in the current study was those who were not practicing exercises. This percentage of risk decreased remarkably with the increase times of exercise practicing/week (9.8%, 6.7% and 4.4% for one time, two times, and three times/week). Engaging in 30 minutes of moderate intensity physical activity on at least 5 days a week helps to prevent many diseases including coronary heart disease.(27) The strongest predictor of developing risk of CVD was coke drinking. Its odds of developing risk of cardiovascular diseases were increased by a factor of 2.6 if the students were drinking coke when controlled for other variables. The logistic model employed explained 20.9% of the variance in the frequent risk of developing CVD. It correctly classified 70.4% of the cases.
We concluded that overweight and obesity were high among adolescent male students who became susceptible to risk of CVD. Both obesity and risk of CVD were strongly correlated to many bad dietary habits and lifestyles. So, we recommend the adolescent students to control obesity to keep their physical fitness. Proper lifestyle habits with regular exercise as well as nutrition education with correct nutritional information are very important to keep body health and to decrease the risk of developing CVD. We expect to use the results as the basic data to develop and implement the nutrition programs in KSA especially in northern borders region having a significant high rate of obesity to maintain proper body weight. A follow-up longitudinal study is recommended in the future on a large sample for both sexes.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Flegal KM, Graubard BI, Williamson DF, Gail MH. Excess deaths associated with underweight, overweight, and obesity. JAMA. 2005;293:1861–7. doi: 10.1001/jama.293.15.1861. [DOI] [PubMed] [Google Scholar]
- 2.Lobstein T, Baur L, Uauy R. IASO International Obesity Task Force. Obesity in children and young people: A crisis in public health. Obes Rev. 2004;5(Suppl 1):4–104. doi: 10.1111/j.1467-789X.2004.00133.x. [DOI] [PubMed] [Google Scholar]
- 3.Mirmiran P, Sherafat-Kazemzadeh R, Jalali-Farahani S, Azizi F. Childhood obesity in the Middle East: A review. East Mediterr Health J. 2010;16:1009–17. [PubMed] [Google Scholar]
- 4.al-Nuaim AR, Bamgboye EA, al-Herbish A. The pattern of growth and obesity in Saudi Arabian male school children. Int J Obes Relat Metab Disord. 1996;20:1000–5. [PubMed] [Google Scholar]
- 5.El Mouzan MI, Al Herbish AS, Al Salloum AA, Al Omar AA, Qurachi MM. Regional variation in prevalence of overweight and obesity in Saudi children and adolescents. Saudi J Gastroenterol. 2012;18:129–32. doi: 10.4103/1319-3767.93818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sweeting H, Anderson A, West P. Socio-demographic correlates of dietary habits in mid to late adolescence. Eur J Clin Nutr. 1994;48:736–48. [PubMed] [Google Scholar]
- 7.Eisenmann JC, Wickel EE, Welk GJ, Blair SN. Relationship between adolescent fitness and fatness and cardiovascular disease risk factors in adulthood: The Aerobics Center Longitudinal Study (ACLS) Am Heart J. 2005;149:46–53. doi: 10.1016/j.ahj.2004.07.016. [DOI] [PubMed] [Google Scholar]
- 8.Eckel RH, Krauss RM. American Heart Association call to action: Obesity as a major risk factor for coronary heart disease. AHA Nutrition Committee. Circulation. 1998;97:2099–100. doi: 10.1161/01.cir.97.21.2099. [DOI] [PubMed] [Google Scholar]
- 9.Krauss RM, Winston M, Fletcher BJ, Grundy SM. Obesity: Impact on cardiovascular disease. Circulation. 1998;98:1472–6. [PubMed] [Google Scholar]
- 10.Schmidt H, Mehring S, McMillan J. Interpreting the declaration of Helsinki (2008): “Must”, “should” and different kinds of obligation. Med Law. 2010;29:565–91. [PubMed] [Google Scholar]
- 11.Mamun AA, O’Callaghan MJ, Williams G, Najman JM. Television watching from adolescence to adulthood and its association with BMI, waist circumference, waist-to-hip ratio and obesity: A longitudinal study. Public Health Nutr. 2013;16:54–64. doi: 10.1017/S1368980012002832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Heydari ST, Ayatollahi SM, Zare N. Diagnostic value of bioelectrical impedance analysis versus body mass index for detection of obesity among students. Asian J Sports Med. 2011;2:68–74. doi: 10.5812/asjsm.34777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.McCarthy HD, Cole TJ, Fry T, Jebb SA, Prentice AM. Body fat reference curves for children. Int J Obes (Lond) 2006;30:598–602. doi: 10.1038/sj.ijo.0803232. [DOI] [PubMed] [Google Scholar]
- 14.Weili Y, He B, Yao H, Dai J, Cui J, Ge D, et al. Waist-to-height ratio is an accurate and easier index for evaluating obesity in children and adolescents. Obesity (Silver Spring) 2007;15:748–52. doi: 10.1038/oby.2007.601. [DOI] [PubMed] [Google Scholar]
- 15.Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ. 2000;320:1240–3. doi: 10.1136/bmj.320.7244.1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Barlow SE. Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics. 2007;120(Suppl 4):S164–92. doi: 10.1542/peds.2007-2329C. [DOI] [PubMed] [Google Scholar]
- 17.Field AE, Cheung L, Wolf AM, Herzog DB, Gortmaker SL, Colditz GA. Exposure to the mass media and weight concerns among girls. Pediatrics. 1999;103:E36. doi: 10.1542/peds.103.3.e36. [DOI] [PubMed] [Google Scholar]
- 18.Washi SA, Ageib MB. Poor diet quality and food habits are related to impaired nutritional status in 13-to 18-year-old adolescents in Jeddah. Nutr Res. 2010;30:527–34. doi: 10.1016/j.nutres.2010.07.002. [DOI] [PubMed] [Google Scholar]
- 19.Rolls BJ, Ello-Martin JA, Tohill BC. What can intervention studies tell us about the relationship between fruit and vegetable consumption and weight management? Nutr Rev. 2004;62:1–17. doi: 10.1111/j.1753-4887.2004.tb00001.x. [DOI] [PubMed] [Google Scholar]
- 20.Al-Rethaiaa AS, Fahmy AE, Al-Shwaiyat NM. Obesity and eating habits among college students in Saudi Arabia: A cross sectional study. Nutr J. 2010;9:39. doi: 10.1186/1475-2891-9-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Amin TT, Al-Sultan AI, Ali A. Overweight and obesity and their relation to dietary habits and socio-demographic characteristics among male primary school children in Al-Hassa, Kingdom of Saudi Arabia. Eur J Nutr. 2008;47:310–8. doi: 10.1007/s00394-008-0727-6. [DOI] [PubMed] [Google Scholar]
- 22.Al-Hazzaa HM. Physical activity, fitness and fatness among Saudi children and adolescents: Implications for cardiovascular health. Saudi Med J. 2002;23:144–50. [PubMed] [Google Scholar]
- 23.Bowman SA. Television-viewing characteristics of adults: Correlations to eating practices and overweight and health status. Prev Chronic Dis. 2006;3:A38. [PMC free article] [PubMed] [Google Scholar]
- 24.Hume C, Singh A, Brug J, Mechelen WV, Chinapaw M. Dose-response associations between screen time and overweight among youth. Int J Pediatr Obes. 2009;4:61–4. doi: 10.1080/17477160802199992. [DOI] [PubMed] [Google Scholar]
- 25.Crooks DL. Food consumption, activity, and overweight among elementary school children in an Appalachian Kentucky community. Am J Phys Anthropol. 2000;112:159–70. doi: 10.1002/(SICI)1096-8644(2000)112:2<159::AID-AJPA3>3.0.CO;2-G. [DOI] [PubMed] [Google Scholar]
- 26.Fontaine KR, Redden DT, Wang C, Westfall AO, Allison DB. Years of life lost due to obesity. JAMA. 2003;289:187–93. doi: 10.1001/jama.289.2.187. [DOI] [PubMed] [Google Scholar]
- 27.Geneva, Switzerland: WHO Press; 2010. World Health Organization, Global Recommendations on Physical Activity for Health. [PubMed] [Google Scholar]