

Abstract
Aspiration of loose teeth is a well-known complication of endo-tracheal intubation hence the importance of oral check by anesthetist prior to ventilation. Artificaial teeth crown (single) or bridges (multiple) can be fixed or removable by the patient. The presence of a foreign body in the lung tissue or airways is a clinical situation that needs aggressive management as it can lead to refractory infections and possible death. We report this unique case of aspirarin of a three bridge teeth (10 mm × 30 mm) following cardiac surgery. The case is complicated by pneumonia, chronic cough and severe bouts of cyanosis and finally removed by spontaneous expulsion after 6 months following forceful cough.
Keywords: Aspiration, coronary artery bypass grafting, teeth bridge
INTRODUCTION
Aspiration of tooth is much more common in children.[1,2] Adult reported cases are mainly during trauma or absence of gag reflex secondary to neurological problems or during intubation. The main treatment approach is by removing the foreign body using rigid or flesible bronchoscope as soon as the condition is discovered.[3,4] To our knowledge this is the first case to be reported in the literature as a delayed spontaneous expulsion of such a big (10 mm × 30 mm) foreign body after a delayed period of 6 months duration from the aspiration date.
CASE REPORT
A 60-year-old lady known to have ischemic heart disease underwent coronary artery bypass grafting. She is also known to have multiple dental problems with two fixed bridge treatments (three teeth each) being stable for years. After the recovery of her cardiac surgery, she and the family noticed that one of her three teeth bridge is missing. Five day's postsurgery her condition was complicated by right sided pneumonia that required prolonged treatment [Figures 1 and 2]. She was discharged home 3 weeks later, but continued to have irritating severe continuous bouts of cough. Six months later; during one of her strongest bouts of cough she had spontaneous expulsion of her intact three teeth bridge and brought it to her doctor [Figure 3]. Cough subsided, and her chest X-ray and computed tomography scan showed no evidence of bronchiectasis as a consequence of the condition [Figure 4].
Figure 1.
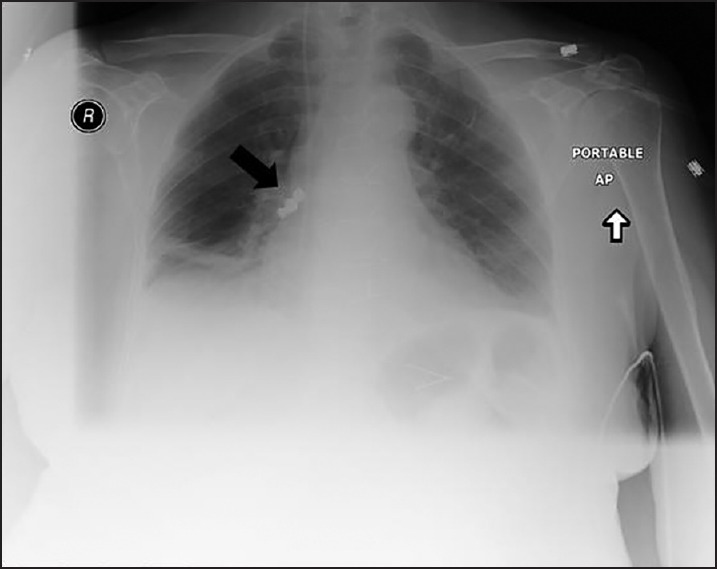
Portable antero-posterior chest X-ray postsurgery, note the foreign body in the right middle lobe (black arrow)
Figure 2.
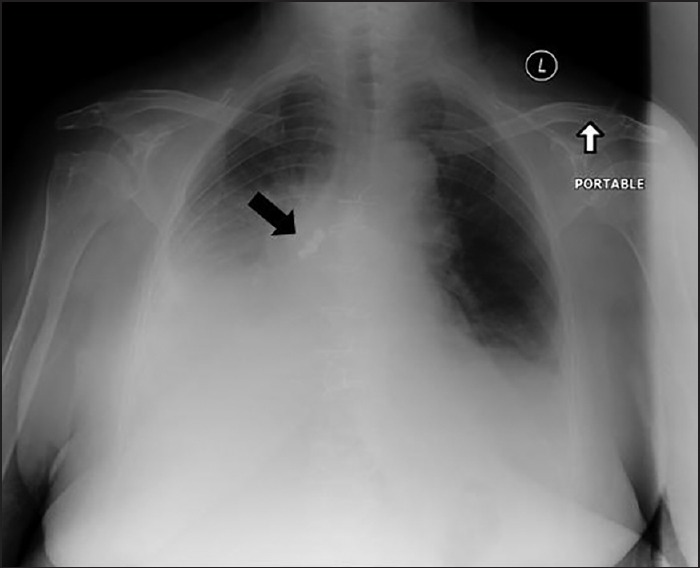
Portable antero-posterior chest X-ray with right sided lobe collapse/consolidation pneumonia
Figure 3.

Picture of the expelled three teeth bridge
Figure 4.
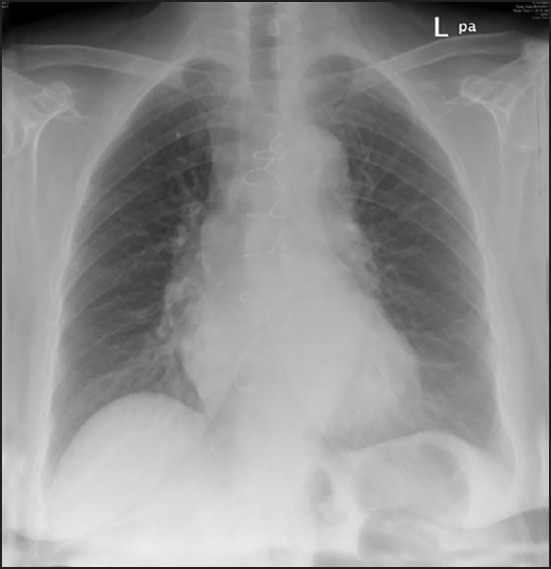
Postero-anterior chest X-ray after teeth expulsion
DISCUSSION
Aspiration of loose teeth or teeth segments in adults are a well-known complication of oral manipulation during intubation or bronchoscope.[5] Extreme caution is needed during this situation. The usual anatomical preference for an aspirated foreign body is the right bronchus.[6] Clinical presentation is variable commonest of which are acute shortness of breath, wheezes, and cyanosis due to complete obstruction of the bronchus. Bronchitis, pneumonia, bronchiectasis, lung abscess, lung collapse and emphysema are also well-known complications. Simple chronic cough can be a manifestation of foreign body aspiration as well.[7] Management plan should be tailored according to the presentation and the degree of obstruction. Encouragement of forceful coughing and treatment of the underlying infection are essential. Urgent approach with chest and the abdominal thrust.[8] until a definite removal is achieved. Bronchoscope are sometimes needed.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.McGuirt WF, Holmes KD, Feehs R, Browne JD. Tracheobronchial foreign bodies. Laryngoscope. 1988;98(6 Pt 1):615–8. doi: 10.1288/00005537-198806000-00007. [DOI] [PubMed] [Google Scholar]
- 2.Pyman C. Inhaled foreign bodies in childhood. A review of 230 cases. Med J Aust. 1971;1:62–8. [PubMed] [Google Scholar]
- 3.Kant S, Verma SK, Mahajan V. Spontaneous expulsion of aspirated teeth in left lung following maxillofacial trauma. Internet J Pulm Med. 2007;8 http://ispub.com/IJPM/8/2 . [Google Scholar]
- 4.Mizuno M, Miyakawa K, Miyakawa M. The diagnostic use of pulmonary scintigrapy for endobronchial foreign bodies in children. J Jpn Bronchoesophagol Soc. 1979;30:252–9. [Google Scholar]
- 5.Ostrinsky Y, Cohen Z. Images in clinical medicine. Tooth aspiration. N Engl J Med. 2006;354:e25. doi: 10.1056/NEJMicm050561. [DOI] [PubMed] [Google Scholar]
- 6.Zhang M, Zhou GJ, Zhao S, Yang JX, Lu X, Gan JX, et al. Delayed diagnosis of tooth aspiration in three multiple trauma patients with mechanical ventilation. Crit Care. 2011;15:424. doi: 10.1186/cc10148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hedblom CA. Foreign bodies of dental origin in a bronchus pulmonary complication. Ann Surg. 1920;71:568–80. doi: 10.1097/00000658-192005000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Leonidas JC, Stuber JL, Rudavsky AZ, Abramson AL. Radionuclide ling scanning in the diagnosis of encobronchial foreign bodies in children. J Pediatr. 1973;83:628–30. doi: 10.1016/s0022-3476(73)80227-6. [DOI] [PubMed] [Google Scholar]