

Abstract
Yoga is an ancient oriental discipline that emerged from mystical and philosophical concepts. Today it is practiced in the west, partly due to the promotion of its benefits to improve the lifestyle and overall health. As compared to non-Hatha Yoga (HY) practitioners, healthier and better-eating patterns have been observed in those who practice it. Agreement with the brought benefits, HY can be used as a therapeutic method to correct abnormal eating behaviors (AEB), obesity, and some metabolic diseases. However, the energy expenditure during traditional protocols of HY is not high; hence, it is not very effective for reducing or maintaining body weight or to improve cardiovascular conditioning. Even so, several observational studies suggest significant changes in eating behaviors, like a reduction in dietary fat intake and increments in that of fresh vegetables, whole grains and soy-based products, which in turn may reduce the risk for cardiovascular diseases. Given the inconsistency of the results derived from cross-sectional studies, more case–control studies are needed to demonstrate the efficacy of HY as an alternative method in the clinical treatment of disordered eating and metabolic diseases.
Keywords: Bioenergetics, complementary medicine, eating disorders, exercise, lifestyles
INTRODUCTION
Yoga originated around 3000 years B.C., under mystical and philosophical concepts in the Hindu tradition. It was transmitted exclusively from teacher to student up until the mid-19th century. Its principles rest in metaphysics, which are hard to understand in Western countries and for those who do not practice it. Some authors, who have gone deep into its study and practice, have tried to explain it. Etymologically, yoga means to “add,” “join,” “unite” or “attach” (Sanskrit, ioga) where the body (anga), mind (chitta), emotions and the soul (atma or atman). A complete explanation of this ancient discipline was given by Eliade[1] in his treatise “Yoga, immortality and freedom,” and defined as a collection of specific techniques to seek a truth hidden in the silence and in the inner calm of people, a fundamental truth which enables one to free the soul from false reality, a state of liberation of the waves of thought or ecstasy (“Samadhi”; Sanskrit, sam o samialk [complete] and ādhi [mentally absorbed]).”
Currently, there are several categories of Yoga. The one practiced in Western societies is an integral Yoga described by Patañjali (II century B.C.).[2] He condenses in his Yoga sūtras, a collection of aphorisms in a Buddhist/Hindi text or manual, the traditions and practices of ancient and contemporary practitioners (yogis). This type of yoga was brought to the American continent by Swami Vivekananda at the end of the 19th century (1894–1896) and was scientifically and philosophically enriched by Eliade.[1] However, through the years Yoga has undergone many transformations and adaptations, thereby changing its original principles and fundamentals.[3] As opposed to the traditional practice, physical focus on Yoga became very popular in the west beginning in the second half of the 20th century and is often referred simply as to Hatha Yoga (HY).
Hatha Yoga refers to a set of physical (Asanas) and mental exercises, designed to align the body and mind, in such way the vital energy (prāṇa) can flow freely. It consists of respiratory exercises (pránáyámas or shatkarma), physical stretching postures, isometric force, balance, relaxation (yoganidra) and concentration (dharana), whose purpose is to ensure that Anga is fit for meditation (dhyana). These elements are conducive to a unique level of consciousness and self-realization, leading to liberation (kaivalya) of the self (atman).[2]
Hatha Yoga reduces stress,[4] improves overall physical fitness and reduces some risk factors for cardiovascular diseases.[5,6,7] Other health effects include prevention of cardiac arrhythmias,[8] hypertension,[9] insomnia,[10] cardiopulmonary disorders,[11] depression and anxiety, epilepsy, cancer, menopause symptoms[12] and chronic back pain.[13] That is why it is adopted as part of a healthy lifestyle or as a therapeutic resource in alternative medicine.[14,15] To give just an example, Ross et al.,[16] postulate that the frequency of yoga practice at home favorably predicted (P < 0.001): Mindfulness, subjective well-being, healthy body mass index (BMI), fruit and vegetable consumption, vegetarian status and vigor. Moreover, specifics components of yoga practice (e.g., physical poses, breath work, meditation, and study of yoga philosophy) improve health behaviors or lifestyle-related health conditions.
However, its benefits in other physical and mental disturbances remain not conclusive, and even harmful effects have even been reported when practiced incorrectly, by unskilled people or disabled.[17,18] Anyhow, HY should be considered as a preventive strategy for improving several metabolic conditions although its utility in complementary medicine, as compared with conventional medical therapies, is under-recognized by the health care community.[19] Lastly, yoga is also a lifestyle, so the physiological events are complemented with other environmental factors such as the change in eating patterns. Here's a conceptual review of this subject, with particular emphasis on the changes in eating behaviors (EBs) and “bioenergy” (BE) management in yogis and the practice of HY as a mean to improve lifestyle and eating patterns in nonyoga practitioners.
METHODOLOGY
The issues to be addressed in the following sections of this critical review, derived from a systematic search for information on 5 databases (Medline [PubMed], Lilacs [Scielo], Latindex, Science direct, Google Scholar) are recognized in the field of yoga and its health impacts. The following Medical Subject Headings (MeSH, Tree number) were used in combination with “Yoga” and “HY” with the purpose of gathering and evaluating judiciously: Energy metabolism (EM) (MESH: G03.495.335), energy expenditure (EE) (MESH: G03.495.335), food (MESH: J02.500), diet (MESH: G07.610.240), eating disorders (ED) (MESH: F03.375), EBs (MESH: F01.145.113.547, F01.145.407), eating (MESH: G07.610.593.260, G07.700.620.260, G10.261.326.240), anorexia nervosa (MESH: F03.375.100), bulimia nervosa (MESH: F03.375.250) and binge eating. Anticipating the specificity and unexplored nature of certain topics, the information gathered from these databases was complemented with certain unpublished findings from the authors.
YOGA BIOENERGETICS
Within the philosophy of yoga, the body's energy is studied from a more subtle and difficult way to measure, which plays a part on the control of total energy intake (TEI) and total energy expenditure (TEE). So, a more holistic view of energy balance has to be addressed, here referred to as BE or kundalini energy.
With the purpose of achieving the desired freedom (kaivalya) of the inner self (atman), the yogi tries to control the body's energy centers (kundalini-chakras) and senses (jnanendriya). The kundalini energy comes in three states: The common dormant, the aroused and the awakened states. When dormant, one's spiritual understanding is restricted, and everything is perceived and interpreted according to a mundane and selfish perspective. When aroused, it gives a sudden temporary state of spiritual insight and spiritual energy, but it is not stable. Only the awakened kundalini energy gives stable transformations of consciousness and progressive realization.[20]
The yogi is not interested in developing physical strength or athletic abilities, at least not in the way they are perceived in the West. The yogi is only interested in the control of its body for the development of atman. To achieve this bioenergetic level, the yogi integrates abstinence (yamas), purity, moderation, and modesty (niyamas) into his/her daily life, and even some dietary[21] and physical activity aspects[22,23] rely on these principles. Therefore, it is somewhat meaningless for the yogi to seek athletic ability using kundalini energy. Nevertheless, some studies using subjective methods to study the effect of HY in BE demonstrate that systematic practice improves the yogi`s vitality and perception of its own physical condition, social functioning and quality of life.[24] Also, because of the nature of physical exercises (Asanas) performed in HY, it is common to find exceptional physical abilities in trained yogis especially in muscular flexibility, strength[25] and stress control.[4,26]
Given the mystical-philosophical roots of HY, the contemporary yogi continues to strive for something more than merely physical and mental health.[27] However, due to the benefits of overall health, it is important to continue to study in detail the subject of BE of HY as compared to other exercise protocols.[23] In the following paragraphs, only the “measurable” energetic aspects are evaluated from the TEE point of view and in terms of changes in EBs which in turn modify TEI. On the metaphysical aspect of HY, psychology and anthropology can provide better arguments and theories, an aspect that escapes the purpose of this review. However, there are very complete comprehensive reviews on this topic.[1,28,29]
YOGA AND ENERGY EXPENDITURE
Scientific studies on EM are focused on measuring TEI or TEE. The latter is generally measured at rest (resting energy expenditure [REE]) or at sleep (basal, basal energy expenditure) or as a result of different pathological, pharmacological, physiological or nutritional modifications.[30] At cellular and molecular levels, many ionic, enzymatic, biosynthetic and genetic mechanisms are involved with either TEI or TEE. Consequently, several metabolic indicators, forms of measurement and equations to estimate the study of the body`s energy balance and body weight control[31] have been generated.
However little or nothing is known about TEE during activation of kundalini energy. Recently Goshvarpour et al.[32,33] reported chaotic heart rate signals as a result of kundalini meditation, which are quite different from those observed in Chinese Chi meditation. From a physiological perspective, meditation is a physiological state of demonstrated reduced metabolic activity – different from sleep – that elicits physical and mental relaxation. Therefore, the EE involved in kundalini meditation is REE. Also, while performing HY (Asanas) the physical intensity measured as consumption of oxygen (VO2) or metabolic equivalents (METs), is low; in fact, it is lesser than that expended in other physical activities such as walking, jogging, running, cycling and swimming. Clay et al.,[34] while studying young adults, found that the METs while performing HY (asanas + pranayamas + dhyana) is 53% less than jogging at 3.5 mill/h (2.2 vs. 3.3 METs); Hagins et al.,[35] found that it is similar to walking at 2 mill/h (~2.5 METs), and that asanas performed in sitting or lying position expend lesser energy (1.5 METs) than those performed in standing positions (2.3 METs).
On the other hand, Danucalov et al.,[36] and Wallace and Benson,[37] found relevant reductions in VO2 during meditation and relaxation (yoganidra) as compared to resting conditions (~2.6 vs. 4.0 ml of O2/kg of body mass/min). All of the above indicates that common protocols of HY are characterized as being of very low intensity, with little possibility of cardiovascular benefits. However, there is a possibility to improve the physical performance, hemodynamic function and increased cardio-respiratory reserve in HY, in spite of the low exercise stimulus; this as a consequence of concerted physical and mental events, such as local muscular adaptation during some physically intense asanas, breathing exercises (Prāṇāyāma) and psycho-physiological control (concentration).[38] It is noteworthy that asanas performed at different intensities may increase TEE up to 3.0 kcal/min while that expended on breathing exercises or during meditation is 2.0 and 1.4 kcal/min, respectively. In view of these arguments, from a cardiopulmonary conditioning standpoint, it is necessary to include complementary aerobic exercises into the HY routine or to perform it with greater intensity.[6,7]
Sun Salutation (Surya Namaskar) is one of the oldest yoga exercises known to man and is one of the most popular and well-acclaimed yoga postures.[39] It has been practiced for centuries and consists of 10–12 different postures[40] which are preferably performed at dawn.[41,42] Each posture counteracts the preceding one producing a balance between flexion and extension with synchronized breathing and aerobic activity.[39] The posture cycle can be repeated several times and at different velocities in the same workout, thereby placing more emphasis on increase of TEE and cardiovascular conditioning. However, Surya Namaskar requires, for its proper performance, an adequate amount of flexibility and muscular strength which is why the studies of this practice have only been done on people who are young or physically fit.[41] Further, the execution must be rhythmic in nature, with each posture and its transition being executed in smooth cadence, and the postures must be performed with minimal jerks or ungainly movements.[40]
The physical intensity of Surya Namaskar is between 3.6 and 9.5 METs. Mody,[41] reported VO2 of 26 ml/kg/min during each round, resulting in an TEE of 234 Kcal during a 30 min session for a 60 kg individual. That EE is enough to maintain body weight or to improve aerobic conditioning.[43] In view of this and in accordance with its intensity and TEE, Surya Namaskar is classified as a moderate-to-high intensity exercise that can be used, when performed at high rhythms, as a form of cardiopulmonary conditioning for people who are young or physically fit. Furthermore, it could be included in contemporary HY sessions. In order to demonstrate that Surya Namaskar is a safe exercise, Omkar et al.,[40] studied the force and moment effects on specific joints (wrist, elbow, shoulder, hip, knee and ankle) during practice of Surya Namaskar. Using a mathematical model, they found that none of the joints were overstressed during Surya Namaskar practice, and concluded that the joints involved are subjected to submaximal loadings as compared to more high impact exercises for which the EE is comparable. “This is of particular importance for older people and for those who have functional limitations in performing aerobic training.”[19,44]
Other alternatives for increasing TEE and cardiovascular conditioning while performing HY, is increasing its intensity and duration of the sessions or adding complementary aerobic and muscular resistance exercises.[6,7] Ray et al.,[45] also demonstrated improved aerobic capacity and decreased perceived exertion after the maximal exercise of HY. Ramos-Jiménez et al.,[7] found that 11 weeks of an intensive HY program, under a more intense protocol than usual performed by trained practitioners of yoga, produced an increase in VO2 max (~3 ml/kg/min), a decrease in body fat (~1.5 kg), systolic blood pressure (~5.5 mmHg) and diastolic blood pressure (~3 mmHg), as well as a weekly TEE of ~1000 kcal. So, intense HY would fulfill the minimum guidelines of the American College of Sports Medicine for maintaining body weight.[43]
In conclusion, given the growing popularity of HY, it can be considered as an alternative to increase the level of physical activity. However, it is recommended to increase the intensity and duration and to include alternative exercises like Surya Namaskar to ensure a maximal TEE and cardiovascular fitness.[43] For instance, the practice of asanas could be an optimal method for preserving the physical function in older people if exercise series are adapted to muscle and join performance[46] as demonstrated in the Yoga Empowers Senior Study.[44] Lastly, the Surya Namaskar could be a better alternative for cardiovascular health, but this should be practiced with caution, especially in people with low fitness levels.
YOGA AND EATING BEHAVIOR
The dietary pattern of a person is one of the most important predictors of health risk. There is substantial evidence that a diet rich in fruits, vegetables, whole grain cereals, lean meat, and fish are inversely associated with the risk of chronic illnesses like cardiovascular disease, cancer, or diabetes.[21,47] However, the food selection is a complex behavioral process since individuals and groups make dietary choices based on food familiarity, availability, cost, cultural norms, taste preferences, health, and convenience, among other factors.[48,49,50,51] The current environment of modern food, with the wide variety of food options, can be so large that it can become difficult to identify a consistent food pattern among people.
Healthy eating can also be considered a practice to seek for and attain harmonic body/mind balance. According to Yoga philosophy, there are intimate connections of diet with mind, and foods have an unknown subtle essence difficult to prove through modern scientific methods. According to Yoga, there are three types of foods: Sattvic, Rajasic and Tamasic.
The Sattvic diet (pure and balanced) is believed to increase energy, produces happiness, calmness, and mental clarity. It could enhance longevity, health, and spirituality. According to Maha Narayana Upanishad (~5000 B.C.) it promotes a life expectancy of 100–150 years and it is recommended for “Saints”. All foods included in this diet are fresh, juicy, nutritious, and tasty, thus including the consumption of fresh fruits and vegetables, sprouted grains, roots, tubers, nuts, cow milk, curd, and honey. The sattvic dietary pattern appears to be similar to a modern but prudent dietary pattern.
The Rajasic diet (over stimulating) is believed to produce jealousy, anger, unfaithfulness, fantasies, and selfishness. It is recommended to leaders and fighters since it may cause excitement, confidence and increase in intelligence. The foods in this diet are bitter, tart, salty, spicy, hot, and dry; they also include white sugar, radishes, and fried foods.
The Tamasic diet (weakens and makes sleepy) is believed to increase pessimism, weakness, laziness, and doubt. The yoga practitioners mention[21,52,53] that this dietary pattern makes one dull, enhances anger and criminal tendency and impedes spiritual progress. The life expectancy is low, and it is bad for health. The foods in this diet include meats from big tamed animals, onions, mushrooms, stale, undercooked-and highly fried foods, high fat fried foods, salt, sugar, spices, chilies pepper, butter and liquor; medicines and stimulants are also included.
Agte and Chiplonkar[21] compiled a database of nutrient contents of 110-food items in two nonconsecutive 24 h-dietary recall of 109 apparently healthy adults. They classified the foods according to their gunas; the Sattvic food had the highest micronutrient density, followed by Rajasic and Tamasic. Although fiber content was quite similar (~14 mg/kcal), the fat content was 18%, 42%, and 72%, respectively. Dietary intake of Sattvic, Rajasic and Tamasic were ~802, ~61 and ~213 g/d. They also included associations among micronutrients food, gunas, and anxiety. Sattvic food intake had the highest correlation with food micronutrients (~r = 0.5, P < 0.01), Rajasic only with thiamin intake (r = 0.47, P < 0.01) and Tamasic with zinc (r = 0.23, P < 0.01), iron (r = 0.30, P < 0.01) and the presence of anxiety (r = 0.37, P < 0.01). From this evidence, the authors argued that Sattvic food have the better health benefits. The authors included in their study a diet plan that would allow reduction of Tamasic and Rajasic foods and an increase in those Sattvic.
It is noteworthy that Sattvic food included a significant amount of functional foods such as soy milk (flavonoids), tomatoes (lycopene), herbal teas (polyphenols) and red amaranth (bioactive peptides). There is also some evidence that practicing other disciplines in which the mind-body axis is used (e.g. Tai Chi), changes the pattern of food consumption. In this respect, practitioners (mainly from Asian countries) of these disciplines have diets based on a wide variety of vegetables, fruits, vegetables, and spices,[52,53] thereby obtaining a high intake of micronutrients and functional ingredients,[54,55] in addition to a reduced amount of dietary fat.[52,56]
Cross-sectional studies show that yoga practitioners have better dietary patterns than their sedentary counterparts. Palasuwan et al.,[56] when evaluating dietary intake and cardiovascular risk factors in pre and postmenopausal Thai women who practice Yoga versus. Tai Chi practitioners or sedentary women, found that yoga practitioners have lower intakes of fats and (BMI, kg/m2); the enzymatic antioxidant activity were similar among groups. When multidisciplinary interventions in which dietary habits, physical activity, stress management and HY are included, significant improvements in overall health is shown as a result of the intervention.[57] Ross et al.[16] postulate that home practice of yoga predicts healthy lifestyle changes including an increased intake of fresh fruits and vegetables. Also, preliminary data obtained from a dietary evaluation in Mexican HY practitioners indicate important changes toward a healthier and adequate diet [Table 1] and the gradual inclusion of functional ingredients such as fiber foods, lignans and flavonoids [Figure 1].
Table 1.
Daily nutrient adequacy (%) of Mexican yoga practitioners *from Northern Mexico
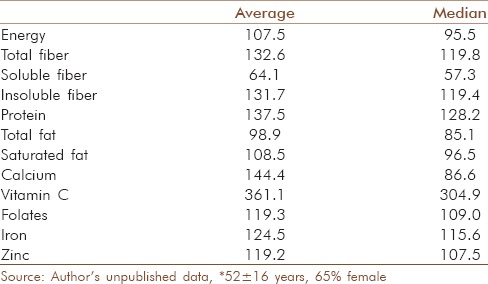
Figure 1.
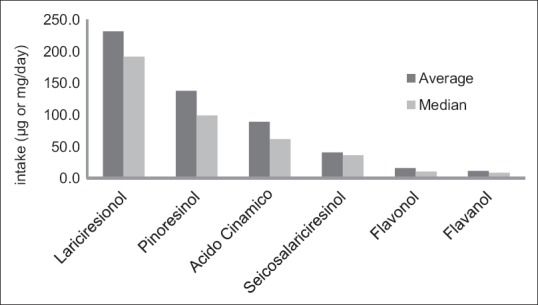
Lignans (μg/d) and flavonoid intake (mg/d) of Mexican yoga practitioners *from Northern Mexico. Source: Author's unpublished data; *52 ± 16 years old, 65% female
However, there are still important questions about the relationship between diet and yoga, particularly on how a practice of yoga changes other specific aspects of the diet (e.g., antioxidant intake) or how it modifies other biomarkers of dietary change (e.g., homocysteine). Studies on these issues should not only consider the qualitative and quantitative aspects involved but also the holistic nature of the phenomenon. Nevertheless and despite very few studies involving dietary assessment in yoga practitioners (beginners and/or advanced), it can be safely concluded that the improvement in the spiritual well-being results in a healthier EB in the long-term.[58] In this sense, Ayurvedic (Sanskrit: Ayus [meaning life] and Veda [knowledge]) treatments which consists of use herbal preparations, diet, yoga, meditation, and other practices, is gaining recognition in Western societies as a holistic alternative intended to treat many metabolic and neuropsychiatric disorders from a predictive, preventive and personalized medicine standpoint.[59]
YOGA AND EATING DISORDERS
The Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition, Text Revision,[60] lists three major types of ED: Anorexia nervosa, bulimia nervosa, and unidentified disorders. Anxiety and depression are common neuropsychiatric conditions in individuals with ED, being seen in ~60% of patients with anorexia and bulimia nervosa.[61] On the other hand, binge eating is a disorder that is characterized by several criteria[60] which include consuming large amounts of food accompanied by feeling of a lack of control. Clinical, community, and population studies have reported that this disorder is associated with being overweight and severe adiposity.[62] The treatment for the different forms of ED is based mainly on cognitive-behavioral and interpersonal therapy with the purpose of inducing positive behavioral changes concerning the people's food intake. However, the lack of progress in treatment development, at least in part, reflects the fact that little is known about the pathophysiologic mechanisms that account for the development and persistence of ED.[63]
Yoga, while seeking for the harmony of the mind and body, benefits people at risk or with established ED. Dittmann and Freedman,[53] when studying body self-perception, attitudes toward food, and the spiritual beliefs of 158 female Yoga practitioners, observed improvements in body satisfaction and self-acceptance along with reduced disordered eating associated to their Yoga practice. Similarly, intervention programs in which Yoga is included as an alternative to the treatment of ED in persons with chronic obesity have shown that 12 weeks of HY practice reduces compulsive eating (binge eating), lengthens meal times and improves food quality.[64] Other interventions, in which problems of anorexia and bulimia nervosa are dealt with Yoga practice, also show similar results. Carei et al.,[65] when studying 54 girls (11–21 years) with ED, found that 1 h/2 times/week sessions of Yoga for 8 weeks reduces symptoms of depression, anxiety, and worries about food as compared to girls with ED treated with conventional clinical methods. However, other studies have shown the opposite, especially when Yoga is compared to other psychological strategies. For example, Mitchell et al.,[66] when studying ED in school age women through Yoga and cognitive dissonance techniques, found that Yoga fails to change these disorders, but cognitive dissonance reduced anxiety and the inability to express emotions (alexithymia), improving self-perception of the body as well. It is important to note at this point that the success of clinical interventions for patients with ED, depends on many factors, but some of them have to do with age, the type of disorder and the severity of symptoms that often accompany them.[67] In conclusion, these and other studies show that the common practice of HY can impact positively on several EDs. However, more studies are needed that compare HY versus alternative clinical treatments for ED.
CONCLUSION
Contemporary HY (asanas + pranayamas + dhyana), seen holistically, is effective for certain health problems such as hypertension, ED, stress, among others. However, due to their low intensity and low EE, they are not recommended for weight loss or improving cardiovascular conditioning. There are alternative exercises like Surya Namaskar, which can be included in its everyday practice, thereby improving health benefits. Also, the practice of Yoga is associated to healthy EBs such a higher consumption of fresh vegetables, dairy products, whole-grains and functional foods (e.g. soy-based products), which could help in ED, but more case–control studies are needed to recommend it as a clinical approach in eating disorders.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Eliade M. Princeton: Princeton University Press; 1969. Yoga: Immortality and freedom. [Google Scholar]
- 2.Varambally S, Gangadhar BN. Yoga: A spiritual practice with therapeutic value in psychiatry. Asian J Psychiatr. 2012;5:186–9. doi: 10.1016/j.ajp.2012.05.003. [DOI] [PubMed] [Google Scholar]
- 3.Askegaard S, Eckhardt GM. Glocal yoga: Re-appropriation in the Indian consumptionscape. Mark Theory. 2012;12:45–60. [Google Scholar]
- 4.Li AW, Goldsmith CA. The effects of yoga on anxiety and stress. Altern Med Rev. 2012;17:21–35. [PubMed] [Google Scholar]
- 5.Javnbakht M, Hejazi Kenari R, Ghasemi M. Effects of yoga on depression and anxiety of women. Complement Ther Clin Pract. 2009;15:102–4. doi: 10.1016/j.ctcp.2009.01.003. [DOI] [PubMed] [Google Scholar]
- 6.Ramos-Jiménez A, Hernández-Torres RP, Wall-Medrano A, Muñoz-Daw MD, Torres-Durán PV, Juárez-Oropeza MA. Cardiovascular and metabolic effects of intensive Hatha Yoga training in middle-aged and older women from northern Mexico. Int J Yoga. 2009;2:49–54. doi: 10.4103/0973-6131.60044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ramos-Jiménez A, Hernández-Torres RP, Wall-Medrano A. Hatha yoga program determinants on cardiovascular health in physically active adult women. J Yoga Phys Ther. 2011;1:103. [Google Scholar]
- 8.Dabhade AM, Pawar BH, Ghunage MS, Ghunage VM. Effect of pranayama (breathing exercise) on arrhythmias in the human heart. Explore (NY) 2012;8:12–5. doi: 10.1016/j.explore.2011.10.004. [DOI] [PubMed] [Google Scholar]
- 9.Okonta NR. Does yoga therapy reduce blood pressure in patients with hypertension?: An integrative review. Holist Nurs Pract. 2012;26:137–41. doi: 10.1097/HNP.0b013e31824ef647. [DOI] [PubMed] [Google Scholar]
- 10.Afonso RF, Hachul H, Kozasa EH, Oliveira Dde S, Goto V, Rodrigues D, et al. Yoga decreases insomnia in postmenopausal women: A randomized clinical trial. Menopause. 2012;19:186–93. doi: 10.1097/gme.0b013e318228225f. [DOI] [PubMed] [Google Scholar]
- 11.Raub JA. Psychophysiologic effects of Hatha Yoga on musculoskeletal and cardiopulmonary function: A literature review. J Altern Complement Med. 2002;8:797–812. doi: 10.1089/10755530260511810. [DOI] [PubMed] [Google Scholar]
- 12.Büssing A, Michalsen A, Khalsa SB, Telles S, Sherman KJ. Effects of yoga on mental and physical health: A short summary of reviews. Evid Based Complement Alternat Med. 2012;2012:165410. doi: 10.1155/2012/165410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tilbrook HE, Cox H, Hewitt CE, Kang’ombe AR, Chuang LH, Jayakody S, et al. Yoga for chronic low back pain: A randomized trial. Ann Intern Med. 2011;155:569–78. doi: 10.7326/0003-4819-155-9-201111010-00003. [DOI] [PubMed] [Google Scholar]
- 14.Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complementary and alternative medicine use among adults: United States, 2002. Adv Data. 2004;343:1–19. [PubMed] [Google Scholar]
- 15.Field T. Yoga clinical research review. Complement Ther Clin Pract. 2011;17:1–8. doi: 10.1016/j.ctcp.2010.09.007. [DOI] [PubMed] [Google Scholar]
- 16.Ross A, Friedmann E, Bevans M, Thomas S. Frequency of yoga practice predicts health: Results of a national survey of yoga practitioners. Evid Based Complement Alternat Med. 2012;2012:983258. doi: 10.1155/2012/983258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Dacci P, Amadio S, Gerevini S, Moiola L, Del Carro U, Radaelli M, et al. Practice of yoga may cause damage of both sciatic nerves: A case report. Neurol Sci. 2013;34:393–6. doi: 10.1007/s10072-012-0998-9. [DOI] [PubMed] [Google Scholar]
- 18.Zhu JK, Wu LD, Zheng RZ, Lan SH. Yoga is found hazardous to the meniscus for Chinese women. Chin J Traumatol. 2012;15:148–51. [PubMed] [Google Scholar]
- 19.Akhtar P, Yardi S, Akhtar M. Effects of yoga on functional capacity and well being. Int J Yoga. 2013;6:76–9. doi: 10.4103/0973-6131.105952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Selby J. USA: Random House Publishing Group; 1992. Kundalini Awakening: A Gentle Guide to Chakra Activation and Spiritual Growth. [Google Scholar]
- 21.Agte VV, Chiplonkar SA. Linkage of concepts of good nutrition in yoga and modern science. Curr Sci. 2007;92:956–61. [Google Scholar]
- 22.Ragoonaden K, Cherkowski S, Berg S. New directions in daily physical activity: Integral education, yoga and physical Literacy. PHEnex. 2012;4:1–16. [Google Scholar]
- 23.Ross A, Thomas S. The health benefits of yoga and exercise: A review of comparison studies. J Altern Complement Med. 2010;16:3–12. doi: 10.1089/acm.2009.0044. [DOI] [PubMed] [Google Scholar]
- 24.Lee SW, Mancuso CA, Charlson ME. Prospective study of new participants in a community-based mind-body training program. J Gen Intern Med. 2004;19:760–5. doi: 10.1111/j.1525-1497.2004.30011.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Tracy BL, Hart CE. Bikram yoga training and physical fitness in healthy young adults. J Strength Cond Res. 2013;27:822–30. doi: 10.1519/JSC.0b013e31825c340f. [DOI] [PubMed] [Google Scholar]
- 26.Smith C, Hancock H, Blake-Mortimer J, Eckert K. A randomised comparative trial of yoga and relaxation to reduce stress and anxiety. Complement Ther Med. 2007;15:77–83. doi: 10.1016/j.ctim.2006.05.001. [DOI] [PubMed] [Google Scholar]
- 27.Srinivasan TM. Review of kundalini yoga meditation for complex psychiatric disorders. J Altern Complement Med. 2011;17:875–6. [Google Scholar]
- 28.Alter JS. Sacrifice, the body, and yoga: Theoretical entailments of embodiment in hathayoga. South Asia. 2012;35:408–33. [Google Scholar]
- 29.Burley M. USA: Routledge; 2007. Classical Samkhya and Yoga: An Indian Metaphysics of Experience. [Google Scholar]
- 30.Hall KD. Modeling metabolic adaptations and energy regulation in humans. Annu Rev Nutr. 2012;32:35–54. doi: 10.1146/annurev-nutr-071811-150705. [DOI] [PubMed] [Google Scholar]
- 31.Hall KD, Heymsfield SB, Kemnitz JW, Klein S, Schoeller DA, Speakman JR. Energy balance and its components: Implications for body weight regulation. Am J Clin Nutr. 2012;95:989–94. doi: 10.3945/ajcn.112.036350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Goshvarpour A, Goshvarpour A. Chaotic behavior of heart rate signals during Chi and kundalini meditation. Int J Image Graph Signal Process. 2012;2:23–9. [Google Scholar]
- 33.Goshvarpour A, Shamsi M, Goshvarpour A. Spectral and time based assessment of meditative heart rate signals. Int J Image Graph Signal Process. 2013;4:1–10. [Google Scholar]
- 34.Clay CC, Lloyd LK, Walker JL, Sharp KR, Pankey RB. The metabolic cost of hatha yoga. J Strength Cond Res. 2005;19:604–10. doi: 10.1519/15144.1. [DOI] [PubMed] [Google Scholar]
- 35.Hagins M, Moore W, Rundle A. Does practicing hatha yoga satisfy recommendations for intensity of physical activity which improves and maintains health and cardiovascular fitness? BMC Complement Altern Med. 2007;7:40. doi: 10.1186/1472-6882-7-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Danucalov MA, Simões RS, Kozasa EH, Leite JR. Cardiorespiratory and metabolic changes during yoga sessions: The effects of respiratory exercises and meditation practices. Appl Psychophysiol Biofeedback. 2008;33:77–81. doi: 10.1007/s10484-008-9053-2. [DOI] [PubMed] [Google Scholar]
- 37.Wallace RK, Benson H. The physiology of meditation. Sci Am. 1972;2:86–91. [Google Scholar]
- 38.Ray US, Pathak A, Tomer OS. Hatha yoga practices: Energy expenditure, respiratory changes and intensity of exercise. Evid Based Complement Alternat Med. 2011;2011:241294. doi: 10.1093/ecam/neq046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Omkar SN. Surya Namaskaar for holistic well being: A comprehensive review of Surya Namaskaar. J Yoga Phys Ther. 2012;2:e109. [Google Scholar]
- 40.Omkar SN, Mour M, Das D. A mathematical model of effects on specific joints during practice of the Sun Salutation – A sequence of yoga postures. J Bodyw Mov Ther. 2011;15:201–8. doi: 10.1016/j.jbmt.2009.07.008. [DOI] [PubMed] [Google Scholar]
- 41.Mody BS. Acute effects of Surya Namaskar on the cardiovascular and metabolic system. J Bodyw Mov Ther. 2011;15:343–7. doi: 10.1016/j.jbmt.2010.05.001. [DOI] [PubMed] [Google Scholar]
- 42.Sinha B, Ray US, Sinha TD. Physiological study of Surya Namaskar, a yogic practice. Altern Ther Health Med. 2011;17:62–3. [PubMed] [Google Scholar]
- 43.Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, et al. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116:1081–93. doi: 10.1161/CIRCULATIONAHA.107.185649. [DOI] [PubMed] [Google Scholar]
- 44.Greendale GA, Kazadi L, Mazdyasni S, Ramirez E, Wang MY, Yu SS, et al. Yoga Empowers Seniors Study (YESS): Design and Asana Series. J Yoga Phys Ther. 2012;2:pii: 107. doi: 10.4172/2157-7595.1000107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Ray US, Sinha B, Tomer OS, Pathak A, Dasgupta T, Selvamurthy W. Aerobic capacity and perceived exertion after practice of Hatha yogic exercises. Indian J Med Res. 2001;114:215–21. [PubMed] [Google Scholar]
- 46.Krucoff C, Carson K, Peterson M, Shipp K, Krucoff M. Teaching yoga to seniors: Essential considerations to enhance safety and reduce risk in a uniquely vulnerable age group. J Altern Complement Med. 2010;16:899–905. doi: 10.1089/acm.2009.0501. [DOI] [PubMed] [Google Scholar]
- 47.Scarborough P, Nnoaham KE, Clarke D, Capewell S, Rayner M. Modelling the impact of a healthy diet on cardiovascular disease and cancer mortality. J Epidemiol Community Health. 2012;66:420–6. doi: 10.1136/jech.2010.114520. [DOI] [PubMed] [Google Scholar]
- 48.Glanz K, Basil M, Maibach E, Goldberg J, Snyder D. Why Americans eat what they do: Taste, nutrition, cost, convenience, and weight control concerns as influences on food consumption. J Am Diet Assoc. 1998;98:1118–26. doi: 10.1016/S0002-8223(98)00260-0. [DOI] [PubMed] [Google Scholar]
- 49.Popkin BM, Duffey K, Gordon-Larsen P. Environmental influences on food choice, physical activity and energy balance. Physiol Behav. 2005;86:603–13. doi: 10.1016/j.physbeh.2005.08.051. [DOI] [PubMed] [Google Scholar]
- 50.Maillot M, Drewnowski A. A conflict between nutritionally adequate diets and meeting the 2010 dietary guidelines for sodium. Am J Prev Med. 2012;42:174–9. doi: 10.1016/j.amepre.2011.10.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Sharma R, Moffatt RJ. Dyslipidemia: Causes, Diagnosis and Treatment. Nova Publishers: New York; 2012. Diet and nutrition therapy in dyslipidemia management; pp. 1–40. [Google Scholar]
- 52.Charoenkiatkul S, Kosulwat V, Chavasit V, Kosulwat S, Rojroongwasinkul N, Boonpraderm A. Nutritive values of healthy Thai foods. J Natl Res Counc Thail. 2003;35:2–59. [Google Scholar]
- 53.Dittmann KA, Freedman MR. Body awareness, eating attitudes, and spiritual beliefs of women practicing yoga. Eat Disord. 2009;17:273–92. doi: 10.1080/10640260902991111. [DOI] [PubMed] [Google Scholar]
- 54.Charoensiri R, Kongkachuichai R, Suknicom S, Sungpuag P. Beta-carotene, lycopene, and alpha-tocopherol contents of selected Thai fruits. Food Chem. 2009;113:202–7. [Google Scholar]
- 55.Jiwajinda S, Santisopasri V, Murakami A, Kim OK, Kim HW, Ohigashi H. Suppressive effects of edible Thai plants on superoxide and nitric oxide generation. Asian Pac J Cancer Prev. 2002;3:215–23. [PubMed] [Google Scholar]
- 56.Palasuwan A, Margaritis I, Soogarun S, Rousseau AS. Dietary intakes and antioxidant status in mind-body exercising pre- and postmenopausal women. J Nutr Health Aging. 2011;15:577–84. doi: 10.1007/s12603-011-0060-2. [DOI] [PubMed] [Google Scholar]
- 57.Toobert DJ, Glasgow RE, Strycker LA, Barrera M, Jr, Ritzwoller DP, Weidner G. Long-term effects of the Mediterranean lifestyle program: A randomized clinical trial for postmenopausal women with type 2 diabetes. Int J Behav Nutr Phys Act. 2007;4:1. doi: 10.1186/1479-5868-4-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Mullin GE. The heart speaks II: Embracing integrative medicine for heart health. Nutr Clin Pract. 2012;27:568–71. doi: 10.1177/0884533612452612. [DOI] [PubMed] [Google Scholar]
- 59.Morandi A, Tosto C, Roberti di Sarsina P, Dalla Libera D. Salutogenesis and Ayurveda: Indications for public health management. EPMA J. 2011;2:459–65. doi: 10.1007/s13167-011-0132-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.APA. 4th ed. Washington, DC: APA Press; 2000. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) [Google Scholar]
- 61.Swinbourne J, Hunt C, Abbott M, Russell J, St Clare T, Touyz S. The comorbidity between eating disorders and anxiety disorders: Prevalence in an eating disorder sample and anxiety disorder sample. Aust N Z J Psychiatry. 2012;46:118–31. doi: 10.1177/0004867411432071. [DOI] [PubMed] [Google Scholar]
- 62.Kessler RC, Berglund PA, Chiu WT, Deitz AC, Hudson JI, Shahly V, et al. The prevalence and correlates of binge eating disorder in the World Health Organization World Mental Health Surveys. Biol Psychiatry. 2013;73:904–14. doi: 10.1016/j.biopsych.2012.11.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Jáuregui-Lobera I. Neuropsychology of eating disorders: 1995-2012. Neuropsychiatr Dis Treat. 2013;9:415–30. doi: 10.2147/NDT.S42714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.McIver S, McGartland M, O’Halloran P. “Overeating is not about the food”: Women describe their experience of a yoga treatment program for binge eating. Qual Health Res. 2009;19:1234–45. doi: 10.1177/1049732309343954. [DOI] [PubMed] [Google Scholar]
- 65.Carei TR, Fyfe-Johnson AL, Breuner CC, Brown MA. Randomized controlled clinical trial of yoga in the treatment of eating disorders. J Adolesc Health. 2010;46:346–51. doi: 10.1016/j.jadohealth.2009.08.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Mitchell KS, Mazzeo SE, Rausch SM, Cooke KL. Innovative interventions for disordered eating: Evaluating dissonance-based and yoga interventions. Int J Eat Disord. 2007;40:120–8. doi: 10.1002/eat.20282. [DOI] [PubMed] [Google Scholar]
- 67.McFarlane TL, MacDonald DE, Royal S, Olmsted MP. Rapid and slow responders to eating disorder treatment: A comparison on clinically relevant variables. Int J Eat Disord. 2013;46:563–6. doi: 10.1002/eat.22136. [DOI] [PubMed] [Google Scholar]