

Abstract
Background
Recent data indicate the presence of immunomodulating properties of Helicobacter pylori (Hp) (Hp Sydney Strain-1 antigen) in an experimental model of multiple sclerosis (MS), and there are limited contradictory epidemiologic data regarding Hp serology in MS patients.
Methods
The aim of this prospective, comparative study was to validate the incidence of active Hp infection by histology and the endoscopic abnormalities, in 44 patients with relapsing-remitting MS and 20 anemic controls.
Results
The overall prevalence of histologically confirmed active Hp infection in 44 MS patients was 86.4% vs. 50% in 20 matched anemic control participants (P=0.002, odds ratio 6.33, 95%CI 1.85-21.64). Concomitant diseases of autoimmune origin including hypothyroidism and ulcerative colitis were exclusively present in MS patients. Moreover, a trend of increased presence of pathological endoscopic findings such as hiatus hernia, Barrett’s esophagus and duodenal ulcer disease was observed in MS patients compared with controls; Barrett’s esophagus and duodenal ulcers were exclusively observed in MS patients. Likewise, Hp (+) MS patients showed exclusive presence of hiatus hernia, esophagitis and duodenal ulcer disease compared with Hp (-) MS patients.
Conclusion
Hp infection appears to be more frequent in MS patients. If confirmed, this might indicate either a common factor that causes susceptibilities to both MS and Hp infection or that Hp might be a causal factor for developing MS. If a causal link between Hp infection and MS is confirmed in the future, this may have a major impact on the pathophysiology and management of MS.
Keywords: Helicobacter pylori, multiple sclerosis, autoimmune disorders, epidemiology, neurodegenerative disorders
Introduction
Multiple sclerosis (MS) is a complex, multifactorial, chronic neuroinflammatory/neurodegenerative disease of the central nervous system (CNS). The pathogenesis of MS remains unclear; probably a combination of infectious and non-infectious environmental factors trigger the pathogenetic process in individuals with a genetic predisposition [1].
A high Helicobacter pylori (Hp) frequency has been reported in various disorders of both CNS, including cerebrovascular diseases, mild cognitive impairment, Alzheimer’s disease (AD), Parkinson’s disease, seizure disorders, migraine, or possibly MS [2-4] and peripheral nervous system such as acute immune polyneuropathies [5].
More recent data indicate the presence of immunomodulating properties of Hp Sydney Strain-1 antigen (Hp-SS1 antigen) administration in an experimental model of MS, suggesting the possible role of Hp infection in the pathophysiology of the disease [6]. In this regard, relative evidence indicates the existence of a shared neurodegenerative process between MS and AD [7] and very recent experimental data indicate that injection of only Hp filtrate increases Aβ42 production by enhancing the activity of γ-secretase, thereby inducing cognitive impairment through interrupting the synaptic function [8]; these data support our relative clinical surveys reporting that Hp eradication may positively influence AD manifestations and 5-year survival rate [9], and suggest that Hp might be a direct causative factor in AD. However, it is as yet not clarified whether Hp is indeed a direct causative factor in MS or an epiphenomenon via induction of immunological responses.
Therefore, the aim of this observational prospective study was to evaluate the increased incidence of active Hp infection by histology in patients with MS. The positive association could possibly support the notion that in susceptible MS individuals Hp infection may influence the disease pathophysiology.
Patients and methods
In the present study, 44 patients with relapsing-remitting MS (30 females, mean age: 38.05±1.3 years, range: 20-53 years), fulfilling the current internationally established criteria for diagnosis of the disease [10] were enrolled. All the patients were of Caucasian origin, resided in Northern Greece, had detailed hospitalization medical records [age, sex, age of onset, symptoms and signs, results of magnetic resonance imaging, visual evoked potential and cerebrospinal fluid examination, expanding disability status scale (EDSS)] (Table 1). All patients were followed at the Multiple Sclerosis Unit of the Neurology Department of “Papageorgiou” General Hospital of Thessaloniki.
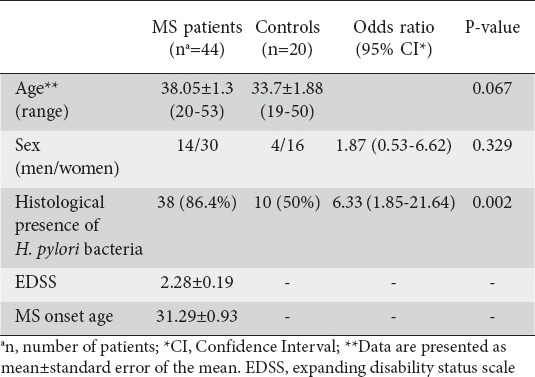
Table 1.
Helicobacter pylori (H. pylori) positively detected by histology in patients with multiple sclerosis (MS) and anemic control participants
Patients were enrolled in the study regardless of disease duration and throughout their participation in the study continued to receive disease modifying treatment. Exclusion criteria included: 1) evidence of disease relapse 30 days prior to and following endoscopic procedure, either on the basis of the patient history, or neurologically documented; 2) EDSS score >5; 3) use of drugs in the preceding 4 weeks (corticosteroids, H2-receptor antagonists, proton pump inhibitors, antibiotics, bismuth compounds or non-steroidal anti-inflammatory drugs, anticoagulant therapy); and 4) alcohol abusers.
Twenty age- and sex-matched individuals with mild iron deficiency anemia (IDA) served as controls. In addition to endoscopic evaluation of the lower digestive tract, control participants also underwent upper gastrointestinal endoscopy for histological evaluation of Hp infection. Control participants were excluded if they had active systemic disease, presence of neurological diseases including MS, malignancy, and liver disease, or if they had received treatment for anemia (FeSO4 or folic acid) prior to completion of the study.
Participants of both groups underwent an esophagogastroduodenoscopy and histological evaluation for Hp detection, as described previously [11]. All participants were informed about the study protocol and provided a written consent; the protocol was approved by the local Ethics Committee and conformed to the principles of the Declaration of Helsinki (1964).
Statistical analysis
The continuous quantitative variables are described as mean ± standard error of mean (SE). Categorical variables are described as sheer numbers and/or percentages. Comparisons between groups were conducted by the use of chi-square test or Fischer’s exact test for categorical variables and Independent sample t-test for quantitative variables. Furthermore, odds ratios and 95% confidence intervals (CI) were calculated for categorical variables. Statistical significance was set at P=0.05. Analysis was performed with the statistical program SPSS 17.0 for Windows (SPSS Inc. Chicago, IL).
Results
Age and sex ratio did not differ between the two groups (MS vs. controls, P=0.067 and odds ratio: 1.87, 95% CI: 0.53-6.62, P=0.329) (Table 1). Patients with MS were treated mostly with interferon-β-1a.
MS patients had significantly higher rate of histologically confirmed active Hp infection than controls (86.4% vs. 50%, odds ratio: 6.33, 95% CI: 1.85-21.64, P=0.002) (Table 1).
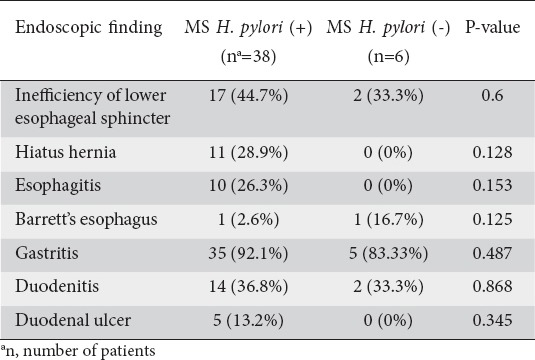
There were no differences in symptoms and concomitant diseases of the digestive tract, biliary tract and other accompanying extradigestive diseases between the two groups (Table 2). However, concomitant diseases of autoimmune origin, including hypothyroidism and ulcerative colitis, were exclusively present in MS patients (Table 2). Moreover, a trend of increased presence of pathological endoscopic findings such as hiatus hernia, Barrett’s esophagus (BE) and duodenal ulcer disease was observed in MS patients compared with controls; BE and duodenal ulcers were exclusively observed in MS patients (Table 3). Likewise, Hp (+) MS patients showed exclusive presence of hiatus hernia, esophagitis, and duodenal ulcer disease compared with Hp (-) MS patients (Table 4).
Table 2.
Concomitant diseases in multiple sclerosis (MS) patients and anemic control participants
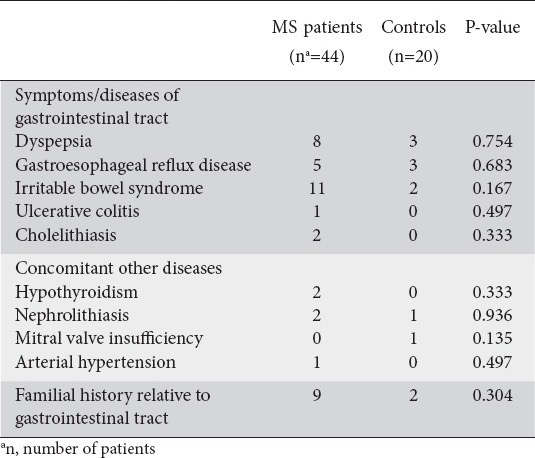
Table 3.
Endoscopic findings between multiple sclerosis (MS) patients and anemic control participants
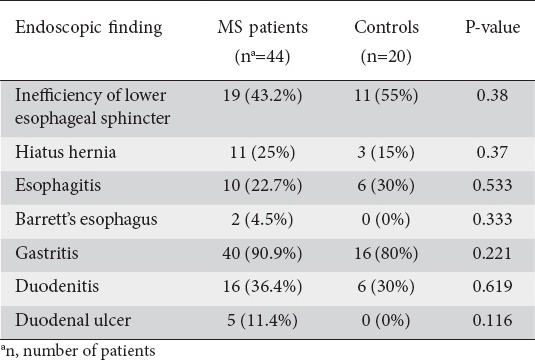
Table 4.
Endoscopic findings in Helicobacter pylori (H. pylori) positive (+) versus H. pylori negative (-) multiple sclerosis (MS) patients
Discussion
The findings of the present study showed increased histologic presence of Hp infection in patients with MS further confirming the findings of our initial pilot study [12]. Although culture is the theoretical gold standard for the detection of this bacterium, it has been shown that there is an excellent correlation with the histological method for the detection of this infection [13]. There are no similar data published to support the relationship between the histological presence of Hp infection and MS, but there are few comparatively and contradictory data concerning the correlation of Hp seropositivity and MS. A study from Poland showed that Hp seropositivity was observed in 18.9% of patients with MS, which is much lower than the proportion of positive anti-Hp IgG antibodies in the general population of Poland [14]. Likewise, other investigators from Japan reported a significantly lower Hp seropositivity in conventional MS (22.6%) compared with healthy controls (42.4%) [15]. A recent study from China showed Hp seropositivity in 73.8% of patients with MS, though it did not differ significantly compared with controls (59.3%, P=0.726) [16]. Nevertheless, these Asian studies reported a positive association between Hp infection and neuromyelitis optica [17]. Finally, a study from Sardinia showed no significant relationship of HP986 protein of Hp with MS [18]. These conflicting findings between the aforementioned studies and the present study may be due to ethnic, population-related and methodological differences [19].
In this respect, it is emphasized that the serological presence of Hp infection utilized in the mentioned studies holds a disadvantage because it cannot discriminate between active and past Hp infection. This distinction is crucial because only the presence of active Hp infection induces humoral and cellular immune responses that through common homologous epitopes (molecular mimicry) cross-react with components of the host’s nervous tissue, thereby affecting or exacerbating the nerve cell damage that characterizes the neurodegenerative diseases, possibly including MS [2,3].
It is important to note that regarding the mild IDA controls used in our series, the link between Hp and IDA was well supported in the literature; such anemic controls have been employed before; the British Society of Gastroenterology and the recent Maastricht IV guidelines recommend Hp eradication in all patients with unexplained and/or recurrent IDA with a normal esophagogastroduodenoscopy and colonoscopy [20,21]. Therefore, it was a “disadvantage” for us to use IDA controls, expected to exhibit a high Hp prevalence. However, we believed that it was not ethical to submit healthy subjects for endoscopic and histologic investigation [20].
Regarding the endoscopic findings, our series showed, for the first time, that BE, a complication of gastroesophageal reflux disease (GERD) and well-recognized premalignant condition that predisposes for subsequent development of esophageal adenocarcinoma (EA), and duodenal ulcer disease are exclusively present in our MS patients. Apart from peptic ulcer disease, recent epidemiologic and molecular data indicated that Hp might be also involved in the GERD-BE-EA sequence, at least in certain geographic ethnic subpopulations [22]. In this regard, there were few relations between the geographic distribution of MS and that of malignancies including upper gastrointestinal cancer [23]. However, due to the very small number of our patients, further large-scale relative studies are needed to verify the potential association of MS Hp (+) patients with upper gastrointestinal tract pathologies.
Regarding the concomitant other diseases associated with MS, this study also showed that diseases of autoimmune origin, including hypothyroidism and ulcerative colitis, are exclusively present in our MS patients. These data are in accordance with other large-scale studies that also reported a co-occurrence of MS with other autoimmune diseases, such as autoimmune thyroid diseases and inflammatory bowel diseases [24,25].
Recent data indicated the presence of immunomodulatory properties of Hp (Hp-SS1 antigen) in an experimental model of MS, suggesting the possible role of Hp infection in the pathophysiology of the disease [6]. Remarkably, very recent experimental data indicated that intraperitoneal injection of Hp filtrate, but not Escherichia coli, increases Aβ42 production by enhancing the activity of γ-secretase, thereby inducing cognitive impairment by interrupting the synaptic function [8]. At present time, similar data with injection of Hp filtrate in MS models are not available. Moreover, the present study has certain limitations including the small number of participants, thereby requiring large-scale relative studies to clarify these fields.
In conclusion, the present study showed that Hp infection appears to be more frequent in MS patients. If confirmed, this might indicate either a common factor that causes susceptibilities to both MS and Hp infection or that Hp might be a causal factor for developing MS.
Summary Box.
What is already known:
There are limited contradictory epidemiologic data regarding Helicobacter pylori (Hp) serology in patients with multiple sclerosis (MS)
What the new findings are:
This study showed, for the first time, a trend of increased presence of upper gastrointestinal tract endoscopic pathological findings in MS patients with Hp infection confirmed histologically
Biography
Aristotle University of Thessaloniki, Ippokration Hospital; AHEPA University Hospital, Aristotle University of Thessaloniki; Papageorgiou Hospital, Thessaloniki, Greece
Footnotes
Conflict of Interest: None
References
- 1.Smyk DS, Alexander AK, Walker M, Walker M. Acute disseminated encephalomyelitis progressing to multiple sclerosis: Are infectious triggers involved? Immunol Res. 2014;60:16–22. doi: 10.1007/s12026-014-8499-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kountouras J, Tsolaki M, Boziki M, et al. Association between Helicobacter pylori infection and mild cognitive impairment. Eur J Neurol. 2007;14:976–982. doi: 10.1111/j.1468-1331.2007.01827.x. [DOI] [PubMed] [Google Scholar]
- 3.Kountouras J, Tsolaki M, Gavalas E, et al. Relationship between Helicobacter pylori infection and Alzheimer disease. Neurology. 2006;66:938–940. doi: 10.1212/01.wnl.0000203644.68059.5f. [DOI] [PubMed] [Google Scholar]
- 4.Nielsen HH, Qiu J, Friis S, Wermuth L, Ritz B. Treatment for Helicobacter pylori infection and risk of Parkinson’s disease in Denmark. Eur J Neurol. 2012;19:864–869. doi: 10.1111/j.1468-1331.2011.03643.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kountouras J, Deretzi G, Zavos C, et al. Association between Helicobacter pylori infection and acute inflammatory demyelinating polyradiculoneuropathy. Eur J Neurol. 2005;12:139–143. doi: 10.1111/j.1468-1331.2004.00977.x. [DOI] [PubMed] [Google Scholar]
- 6.Boziki M, Grigoriadis N, Deretzi G, et al. Helicobacter pylori immunomodulative properties in a mouse model of multiple sclerosis. Immunogastroenterology. 2012;1:34–39. [Google Scholar]
- 7.Xia Z, Chibnik LB, Glanz BI, et al. A putative Alzheimer’s disease risk allele in PCK1 influences brain atrophy in multiple sclerosis. PLoS One. 2010;5:e14169. doi: 10.1371/journal.pone.0014169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wang XL, Zeng J, Feng J, et al. Helicobacter pylori filtrate impairs spatial learning and memory in rats and increases β-amyloid by enhancing expression of presenilin-2. Front Aging Neurosci. 2014;6:66. doi: 10.3389/fnagi.2014.00066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kountouras J, Boziki M, Gavalas E, et al. Five-year survival after Helicobacter pylori eradication in Alzheimer disease patients. Cogn Behav Neurol. 2010;23:199–204. doi: 10.1097/WNN.0b013e3181df3034. [DOI] [PubMed] [Google Scholar]
- 10.Polman CH, Reingold SC, Banwell B, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol. 2011;69:292–302. doi: 10.1002/ana.22366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kountouras J, Mylopoulos N, Chatzopoulos D, et al. Eradication of Helicobacter pylori may be beneficial in the management of chronic open-angle glaucoma. Arch Intern Med. 2002;162:1237–1244. doi: 10.1001/archinte.162.11.1237. [DOI] [PubMed] [Google Scholar]
- 12.Gavalas E, Kountouras J, Deretzi G, et al. Helicobacter pylori and multiple sclerosis. J Neuroimmunol. 2007;188:187–189. doi: 10.1016/j.jneuroim.2007.06.007. [DOI] [PubMed] [Google Scholar]
- 13.Weinstein WM. Gastritis and gastropathies. In: Sleisenger MH, Fordtran JS, editors. Gastrointestinal disease: pathology, diagnosis, management. 5th Edn. Philadelphia, PA: Saunders WB; 1993. pp. 545–571. [Google Scholar]
- 14.Wender M. Prevalence of Helicobacter pylori infection among patients with multiple sclerosis. (Article in Polish) Neurol Neurochir Pol. 2003;37:45–48. [PubMed] [Google Scholar]
- 15.Li W, Minohara M, Su JJ, et al. Helicobacter pylori infection is a potential protective factor against conventional multiple sclerosis in the Japanese population. J Neuroimmunol. 2007;184:227–231. doi: 10.1016/j.jneuroim.2006.12.010. [DOI] [PubMed] [Google Scholar]
- 16.Long Y, Gao C, Qiu W, et al. Helicobacter pylori infection in neuromyelitis optica and multiple sclerosis. Neuroimmunomodulation. 2013;20:107–112. doi: 10.1159/000345838. [DOI] [PubMed] [Google Scholar]
- 17.Li W, Minohara M, Piao H, et al. Association of anti-Helicobacter pylori neutrophil-activating protein antibody response with anti-aquaporin-4 autoimmunity in Japanese patients with multiple sclerosis and neuromyelitis optica. Mult Scler. 2009;15:1411–1421. doi: 10.1177/1352458509348961. [DOI] [PubMed] [Google Scholar]
- 18.Cossu D, Masala S, Cocco E, et al. Are mycobacterium avium subsp. paratuberculosis and Epstein-Barr virus triggers of multiple sclerosis in Sardinia? Mult Scler. 2012;18:1181–1184. doi: 10.1177/1352458511433430. [DOI] [PubMed] [Google Scholar]
- 19.Kountouras J, Zavos C, Gavalas E, Boziki M, Katsinelos P. Helicobacter pylori may hold a variable role in multiple sclerosis based on ethnicity. Med Hypotheses. 2008;71:614–615. doi: 10.1016/j.mehy.2008.05.007. [DOI] [PubMed] [Google Scholar]
- 20.Kountouras J, Zavos C, Chatzopoulos D. Helicobactger pylori and glaucoma. Ophthalmology. 2003;110:2433–2434. doi: 10.1016/j.ophtha.2003.09.014. [DOI] [PubMed] [Google Scholar]
- 21.Wong F, Rayner-Hartley E, Byrne MF. Extraintestinal manifestations of Helicobacter pylori: A concise review. World J Gastroenterol. 2014;20:11950–11961. doi: 10.3748/wjg.v20.i34.11950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kountouras J, Chatzopoulos D, Zavos C, et al. Helicobacter pylori infection might contribute to esophageal adenocarcinoma progress in subpopulations with gastroesophageal reflux disease and Barrett’s esophagus. Helicobacter. 2012;17:402–403. doi: 10.1111/j.1523-5378.2012.00963.x. [DOI] [PubMed] [Google Scholar]
- 23.Materljan E, Materljan M, Materljan B, Vlacić H, Barićev-Novaković Z, Sepcić J. Multiple sclerosis and cancers in Croatia--a possible protective role of the “Mediterranean diet”. Coll Antropol. 2009;33:539–545. [PubMed] [Google Scholar]
- 24.Deretzi G, Kountouras J, Koutlas E, et al. Familial prevalence of autoimmune disorders in multiple sclerosis in Northern Greece. Mult Scler. 2010;16:1091–1101. doi: 10.1177/1352458510375708. [DOI] [PubMed] [Google Scholar]
- 25.Deretzi G, Kountouras J, Polyzos SA, et al. Polyautoimmunity in a Greek cohort of multiple sclerosis. Acta Neurol Scand. 2015;131:225–230. doi: 10.1111/ane.12308. [DOI] [PubMed] [Google Scholar]