

Abstract
Background:
The Balance Error Scoring System (BESS) is a useful means of measuring postural stability, which frequently exhibits deficits after a concussion. However, it has limited applicability for children since there is insufficient normative data available for the BESS in the pediatric population. The purposes of this study were to report scores for the BESS in children 10 to 17 years old with no history of concussion and to identify whether BESS score is correlated with age, sex, sports participation, height, weight, or body mass index.
Hypothesis:
Baseline BESS scores will be related to age and sports participation.
Study Design:
Descriptive laboratory study.
Level of Evidence:
Level 3.
Methods:
One examiner recruited 100 participants 10 to 17 years old over a period of 4 months; performed all of the BESS tests; surveyed participants regarding age, sex, and sports participation; recorded participants’ heights and weights; and calculated body mass indices. Intrarater reliability was measured. The main outcome measures were total, firm, and foam surface BESS scores. We assessed data for normality using the Shapiro-Wilk test and used the Spearman rank test to determine whether BESS scores correlated with sex, age, sports participation, height, weight, or body mass index.
Results:
There was no correlation between the BESS firm surface (5.37 ± 4.4), BESS foam surface (12.28 ± 4.43), or total surface scores (17.64 ± 7.52) and age, anthropometrics, or sports participation. Male and female subjects had similar scores except in the 10- to 13-year-old age group on the foam surface, where girls performed better than boys (10.42 ± 4.53 vs 13.07 ± 4.23; P = 0.02).
Conclusion:
Baseline BESS scores in children aged 10 to 17 years were normally distributed and were not related to age, sex, height, weight, body mass index, or sports participation.
Clinical Relevance:
These results provide a reference for clinicians using BESS to evaluate and manage children and teens with concussions.
Keywords: concussion, traumatic brain injury, pediatrics, balance, postural stability
Concussions in sports have recently received a great deal of attention as more of the potential adverse and potentially long-term effects of these injuries are being identified, including deficits in complex visual stimuli processing, lower grade point averages, second-impact syndrome, and postconcussion syndrome.5,13 As a result, there has been an impetus to develop valid and reliable tools to assist with evaluation and management of athletes with concussions. These include computerized neuropsychological testing, symptom inventories, and measures of postural stability.2,5,11 However, none of these tools has been well-researched in children younger than 14 years. Given that pediatric populations compose the majority of the estimated 1.6 to 3.8 million annual mild traumatic brain injuries, it is important to determine whether these tools are appropriate for the pediatric age group.5,11
The Balance Error Scoring System (BESS) is a valid, objective, quick, and inexpensive means of measuring postural stability, which frequently exhibits deficits in the first 48 to 72 hours after a concussion.1-4,12,15 The BESS score can be compared with a preinjury (baseline) score if available or with population norms.9
Unfortunately, while normative data have been reported for BESS scores in adults 20 to 69 years old, the BESS currently has limited applicability for children, since there is insufficient normative data available for the BESS in the pediatric population—especially in children younger than 13 years.9,10 Previous studies using force platforms show that children and adolescents demonstrate greater sway velocity and less postural stability than adults.7,8 The purposes of this study were to report scores for the BESS in children 10 to 17 years old with no history of concussion and to identify whether BESS score is correlated with age, sex, sports participation, height, weight, or body mass index (BMI). These variables were evaluated to allow for better clinical interpretation of BESS scores in the context of differing patient characteristics increasing the clinical applicability of the BESS.
Materials and Methods
Subjects
This study was approved by the Institutional Review Board at Ann & Robert H. Lurie Children’s Hospital of Chicago. We recruited 100 children and adolescents from orthopaedic and sports medicine clinics at a large children’s hospital in Chicago. Potential participants were identified based on chart review, and eligibility was confirmed by screening for exclusion criteria during clinic visits. Inclusion criterion was being 10 to 17 years of age. Exclusion criteria were a history of concussion, balance or neurological disorders, acute or chronically symptomatic lower extremity injury, pes planovalgus, subtalar overpronation, genu valgum, a positive Trendelenburg test, and history of ankle sprain.
We obtained written parental consent from all parents and written assent from all subjects older than 11 years. Some of these children (n = 3) were unable to sign the assent form because of hand injuries, but were informed of all procedures and policies before verbally agreeing to participate.
Testing
One examiner (N.K.K.) performed all BESS tests, administered a survey to determine the number of sports participants played, and recorded participants’ heights and weights. The examiner was taught how to administer the BESS by a certified athletic trainer (K.B.) and practiced scoring approximately 15 patients in a pediatric sports medicine clinic over 1 week. We then measured intrarater reliability prior to subject enrollment as follows: The examiner watched videos of 30 patients performing the BESS test and scored them. One week later, he watched the same videos and rescored the same 30 patients. The intraclass correlation coefficient was 0.99, and the standard error of measurement was 0.41 for the total BESS score.
After enrollment, we informed subjects and parents of the BESS testing procedures and what constituted an error. We administered the BESS test once for each subject in the same clinics from which subjects were recruited and in the same manner as described in previous studies.4,8 We tested 3 positions (feet touching side-by-side, a single leg stance on the nondominant leg, and a heel-to-toe stance with the dominant foot in front) for 20 seconds each on a firm surface and then on a 50 cm × 41 cm × 6 cm–thick foam pad (Airex Balance-Pad Elite; Airex). We identified the dominant leg by asking subjects which foot they would use to kick a ball. We instructed subjects to close their eyes and place hands on hips for 20 seconds. Subjects were also told that the clock would not stop running during testing, so if they ever came out of the starting position, they should make any necessary adjustments and return to the position as quickly as possible. One error point was given every time the subject moved hands off hips, opened eyes, stepped, stumbled, abducted or flexed the hip greater than 30°, lifted the forefoot or heel from the testing surface, or remained out of the testing position for more than 5 seconds. The maximum score for any 1 trial was 10 points. If a subject could not maintain 1 of the positions for a minimum of 5 seconds at any point during a trial, we assigned the maximum score of 10 for that trial. We calculated the total BESS score (sum of scores from all 6 trials), the firm surface score (sum of scores from the 3 firm surface trials), and foam surface score (sum of scores from the 3 foam surface trials).
We calculated the mean, median, standard deviation, and percentile ranks for total BESS score, the firm surface score, and foam surface score. We assessed these data for normality using the Shapiro-Wilk test. We used the Spearman rank test to determine whether BESS scores correlated with sex, age, sports participation, height, weight, or BMI. We also used the Mann-Whitney U test for pairwise comparisons of BESS scores between age groups (10-13 and 14-17 years of age) and between sexes.
Results
Of the 100 subjects, 65 (65%) were boys (Table 1). Eight-seven percent (n = 87) of subjects played at least 1 sport. For this group of subjects who played sports, 63 (72.41%) were boys; the mean age was 12.48 ± 2.00 years, and 22 different sports were reported. The total BESS scores and the foam surface scores followed a normal distribution, but the firm surface scores were not normally distributed (Figure 1, Table 2).
Table 1.
Subjects’ characteristics
| Range | Mean (SD) | |
|---|---|---|
| Age, y | 10-17 | 12.47 (2.01) |
| Height, m | 1.22-1.93 | 1.56 (0.14) |
| Mass, kg | 23.59-108.86 | 53.26 (17.35) |
| Body mass index, kg/m2 | 13-37 | 21.63 (5.13) |
Figure 1.
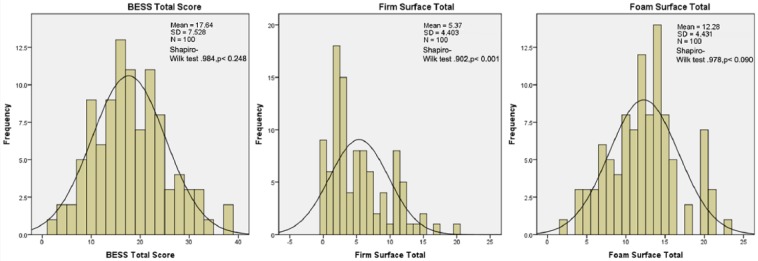
Histograms showing the distribution of BESS Total Scores, Firm Surface Total Scores, and Foam Surface Total Scores with respective sample sizes, means, standard deviations, and Shapiro-Wilk test scores. BESS, Balance Error Scoring System.
Table 2.
BESS score means, medians, and percentiles
| Percentile | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Median | >90th | 76th to 90th | 25th to 75th | 10th to 24th | 2nd to 9th | <2nd | |
| Firm surface score | 5.37 | 4.40 | 4.00 | 0-0 | 1-2 | 2-8 | 8-11 | 12-17 | 17-20 |
| Foam surface score | 12.28 | 4.43 | 12.00 | 0-0 | 0-2 | 2-5 | 5-10 | 10-10 | 10-10 |
| Total BESS score | 17.64 | 7.52 | 17.00 | 2-7 | 7-9 | 10-15 | 15-18 | 20-21 | 21-23 |
BESS, Balance Error Scoring System.
No correlation was found between age and firm surface score (r = −0.14, P = 0.18), foam surface score (r = −0.08, P = 0.42), or total BESS score (r = −0.13, P = 0.19) (Table 3). In addition to analyzing age as a continuous variable, we also analyzed age categorically by grouping subjects into either the middle school age group (10-13 years) or the high school age group (14-17 years). These age groups were defined to create large enough sample sizes for adequate statistical analysis while also keeping the age ranges of both groups narrow enough to maintain clinical significance. When age was analyzed categorically, there were also no differences between younger (10-13 years) and older (14-17 years) subjects for firm surface score (P = 0.34), foam surface score (P = 0.69), or total BESS score (P = 0.69) (Table 3).
Table 3.
BESS scores by sex, sports participation, and age group
| Mean Firm Surface Score (SD) | Mean Foam Surface Score (SD) | Mean Total BESS Score (SD) | |
|---|---|---|---|
| Boys (n = 65) | 5.35 (4.36) | 12.80 (4.35) | 18.14 (7.33) |
| Girls (n = 35) | 5.40 (4.54) | 11.31 (4.49) | 16.71 (7.90) |
| No sport participation (n = 13) | 5.62 (3.71) | 12.92 (3.99) | 18.54 (6.31) |
| Sport participation (n = 87) | 5.33 (4.52) | 12.18 (4.51) | 17.51 (7.72) |
| Age group | |||
| 10-13 years (n = 68) | 5.69 (4.63) | 12.13 (4.49) | 17.81 (7.75) |
| 14-17 years (n = 32) | 4.69 (3.85) | 12.59 (4.36) | 17.28 (7.15) |
| Total Sample (n = 100) | 5.37 (4.40) | 12.28 (4.43) | 17.64 (7.53) |
BESS, Balance Error Scoring System.
There were no correlations between firm surface score, foam surface score, or total BESS score and height (r = −0.18, P = 0.07; r = −0.14, P = 0.17; r = −0.19, P = 0.07, respectively), weight (r = −0.06, P = 0.58; r = −0.08, P = 0.44; r = −0.08, P = 0.43, respectively), or BMI (r = 0.03, P = 0.74; r = 0.01, P = 0.94; r = 0.02, P = 0.85, respectively).
Firm surface scores, foam surface scores, and total BESS scores were also not different between subjects who participated in sports and those who did not play any sports (P = 0.56, P = 0.52, and P = 0.48, respectively) (Table 3).
Overall, male and female subjects had similar firm surface scores (P = 0.98), foam surface scores (P = 0.08), and total BESS scores (P = 0.38) (Table 3). When BESS scores were analyzed by age group, there were also no significant sex differences except in the 10- to 13-year-old age group on the foam surface, where girls performed better than boys (10.42 ± 4.53 vs 13.07 ± 4.23, P = 0.02; Figure 2).
Figure 2.

Comparison of mean BESS Total Scores, BESS Firm Surface Scores, and BESS Foam Surface Scores between boys and girls among different age groups. Bars represent standard deviation of the mean. BESS, Balance Error Scoring System.
Discussion
The mean BESS score in this pediatric sample (17.64 ± 7.53) is higher than the mean BESS scores reported for adult populations.9 A study of collegiate male football players12 found a mean BESS score of 12.73 ± 7.57, and Iverson and Koehle9 recorded a mean BESS score of 11.0 ± 4.8 for 20- to 29-year-olds in the general population. This age difference in BESS scores is in agreement with prior studies using force platforms that showed the mean baseline body sway velocity of children 6 to 15 years of age significantly differs from that of adults.7 Children in this age group were also shown to have a greater increase in sway velocity than other age groups when tested on a foam, plastic-covered surface similar to the foam surface used in the BESS.7 Additionally, Hirabayashi and Iwasaki6 demonstrated that at 14 to 15 years of age, adolescents continued to exhibit deficiencies in vestibular function with regard to postural stability as compared with adults, further supporting the need for age-specific norms when evaluating BESS performance.
Prior studies assessing the test-retest reliability and learning effects of the BESS in children 9 to 14 years old have provided their samples’ mean BESS scores. In one study with a sample of 49, the mean total BESS score was 15.54 ± 5.82.16 In another with a sample of 25, the mean total BESS score was 14.96 ± 4.61.17 These scores are also lower than those reported in our study, but to a lesser degree than the reported BESS scores of adults.
We found no significant differences in BESS scores between athletes and nonathletes, which suggests the norms reported here may be used as a reference in both populations.
We found no correlation between BESS score and age or sex, with 1 exception: In the 10- to 13-year age group, girls performed significantly better on the foam surface than boys. Similar sex differences in postural stability were also found in a study of high school athletes where 13- to 14-year-old girls performed significantly better than their male counterparts on a modified BESS test.10 Other studies assessing body sway have demonstrated similar findings with girls 7 to 8 years old, demonstrating superior vestibular function with regard to postural stability, and boys younger than 10 years swaying significantly more than similarly aged girls.6,14 Conversely, Iverson and Koehle’s9 data on adults showed slightly better BESS performance in men than in women, although they noted that the effect size was very small. This suggests that postural stability may mature earlier in girls.
While we did not find any correlation between BESS and subject anthropometrics, Iverson and colleagues found small correlations between BESS score and weight and BESS score and BMI in adults.8,9 However, the sample sizes used in their studies were larger (n = 589 and n = 1236, respectively), and thus could more reliably assess these associations.
Limitations
The sample size was small (N = 100) and thus may have been underpowered to detect significant associations between BESS scores and the measured variables. As the study’s primary purpose was descriptive in nature, no a priori power analysis was performed. The small sample size and the large variety of sports played by participants did not allow analysis of the effect of specific sports on BESS performance. Subjects were recruited from sports medicine clinics where the vast majority was being treated for upper extremity injuries. It is possible these injuries may have affected the BESS scores. In addition, these subjects may have had poorer baseline postural stability, which precipitated their current injuries. The distribution of athletes and nonathletes was not equal, which may have limited the comparison between these groups. Our analysis was based on chronological age rather than maturational stage, and it is possible that BESS scores correlate better with maturational stage than chronological age. Finally, in this study, subjects underwent BESS testing only once. As such, clinicians should be cautioned that the values reported in this study may only be applicable to a patient’s initial BESS test.
Conclusion
These results suggest that it may be necessary to use a different set of BESS norms to act as comparative data in pediatric versus adult populations when baseline testing is unavailable.
Acknowledgments
The authors would like to thank Dr Jay Smith and Kelli Kyle for their assistance with intrarater reliability testing.
Footnotes
The authors reported the following potential conflicts of interest: Funding was provided by Northwestern University’s Feinberg School of Medicine.
References
- 1. Bell DR, Guskiewicz KM, Clark MA, Padua DA. Systematic review of the Balance Error Scoring System. Sports Health. 2011;3:287-295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Ellemberg D, Henry LC, Macciocchi SN, Guskiewicz KM, Broglio SP. Advances in sport concussion assessment: from behavioral to brain imaging measures. J Neurotrauma. 2009;26:2365-2382. [DOI] [PubMed] [Google Scholar]
- 3. Guskiewicz KM, Perrin DH, Gansneder BM. Effect of mild head injury on postural stability in athletes. J Athl Train. 1996;31:300-306. [PMC free article] [PubMed] [Google Scholar]
- 4. Guskiewicz KM, Ross SE, Marshall SW. Postural stability and neuropsychological deficits after concussion in collegiate athletes. J Athl Train. 2001;36:263-273. [PMC free article] [PubMed] [Google Scholar]
- 5. Halstead ME, Walter KD; Council on Sports Medicine and Fitness. Clinical report—sport-related concussion in children and adolescents. Pediatrics. 2010;126:597-615. [DOI] [PubMed] [Google Scholar]
- 6. Hirabayashi S, Iwasaki Y. Developmental perspective of sensory organization on postural control. Brain Dev. 1995;17:111-113. [DOI] [PubMed] [Google Scholar]
- 7. Hytonen M, Pyykko I, Aalto H, Starck J. Postural control and age. Acta Otolaryngol. 1993;113:119-122. [DOI] [PubMed] [Google Scholar]
- 8. Iverson GL, Kaarto ML, Koehle MS. Normative data for the Balance Error Scoring System: implications for brain injury evaluations. Brain Inj. 2008;22:147-152. [DOI] [PubMed] [Google Scholar]
- 9. Iverson GL, Koehle MS. Normative data for the Balance Error Scoring System in adults. Rehabil Res Pract. 2013;2013:846418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Jinguji TM, Bompadre V, Harmon KG, et al. Sport Concussion Assessment Tool—2: baseline values for high school athletes. Br J Sports Med. 2012;46:365-370. [DOI] [PubMed] [Google Scholar]
- 11. Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury. J Head Trauma Rehabil. 2006;21:375-378. [DOI] [PubMed] [Google Scholar]
- 12. McCrea M, Guskiewicz KM, Marshall SW, et al. Acute effects and recovery time following concussion in collegiate football players: the NCAA Concussion Study. JAMA. 2003;290:2556-2563. [DOI] [PubMed] [Google Scholar]
- 13. Moser RS, Schatz P, Jordan BD. Prolonged effects of concussion in high school athletes. Neurosurgery. 2005;57:300-306. [DOI] [PubMed] [Google Scholar]
- 14. Riach C, Hayes K. Maturation of postural sway in young children. Dev Med Child Neurol. 1987;29:650-658. [DOI] [PubMed] [Google Scholar]
- 15. Riemann BL, Guskiewicz KM. Effects of mild head injury on postural stability as measured through clinical balance testing. J Athl Train. 2000;35:19-25. [PMC free article] [PubMed] [Google Scholar]
- 16. Valovich McLeod TC, Barr W, McCrea M, Guskiewicz KM. Psychometric and measurement properties of concussion assessment tools in youth sports. J Athl Train. 2006;41:399-408. [PMC free article] [PubMed] [Google Scholar]
- 17. Valovich McLeod TC, Perrin DH, Guskiewicz KM, Shultz SJ, Diamond R, Gansneder BM. Serial administration of clinical concussion assessments and learning effects in healthy young athletes. Clin J Sport Med. 2004;14:287-295. [DOI] [PubMed] [Google Scholar]