

Abstract
This study examines the academic abilities of children and adolescents who were once diagnosed with an autism spectrum disorder (ASD), but who no longer meet diagnostic criteria for this disorder. These individuals have achieved social and language skills within the average range for their ages, receive little or no school support and are referred to as having achieved “optimal outcomes” (OO). Performance of 32 individuals who achieved OO, 41 high-functioning individuals with a current ASD diagnosis (HFA), and 34 typically-developing peers (TD) was compared on measures of decoding, reading comprehension, mathematical problem solving and written expression. Groups were matched on age, sex and nonverbal IQ; however, the HFA group scored significantly lower than the OO and TD groups on verbal IQ. All three groups performed in the average range on all subtests measured and no significant differences were found in performance of the OO and TD groups. The HFA group scored significantly lower on subtests of reading comprehension and mathematical problem solving than the OO group. These findings suggest that the academic abilities of individuals who achieved OO are similar to those of their TD peers, even in areas where individuals who have retained their ASD diagnoses exhibit some ongoing difficulty.
Autism Spectrum Disorders (ASDs) are considered by many to be lifelong conditions. However, several studies have indicated that a small percentage of individuals who are diagnosed with ASDs early in childhood respond particularly well to early intervention or show striking reductions in symptomatology with maturation, to such a degree that they no longer meet diagnostic criteria for any ASD (reviewed in Helt et al, 2008).
Lovaas initially introduced the phenomenon of “recovery” or “best outcome” in 1987, when he reported that 47% of his sample performed in the average range on measures of cognitive functioning after receiving an early, intensive, behavioral intervention program for ASDs. Since this study, a number of others have reported that a small number of participants performed in the average range on some outcome measures following intensive behavioral interventions (Cohen et al., 2006; Harris & Handleman, 2007; Sallows & Graupner, 2005; Weiss, 1999; Zachor et al., 2007). Several longitudinal studies examining outcomes of ASDs in middle childhood, adolescence and adulthood have also reported that 1-25% of their samples no longer met diagnostic criteria for ASDs by the conclusion of the studies (Howlin et al., 2004, Rutter, 1970; Sigman & Ruskin, 1999; Seltzer et al., 2004; Szatmari et al., 1989; Venter et al., 1992). Characterizing residual difficulties in these children who achieve this level of optimal outcome (OO) can have theoretical implications for understanding the core deficits of ASD and practical implications for assessing service needs. The few studies that have focused on a group of children who achieved OO (i.e., diagnosed with ASD in early childhood, but by middle childhood no longer meet diagnostic criteria for ASD, had average IQs and were mainstreamed in regular classrooms without extra assistance) revealed the presence of attentional difficulties, mild perseverative interests and occasional repetitive motor movements (Fein et al, 2005). Subtle difficulties have also been detected in pragmatic and semantic language, specifically in comprehension of second order theory of mind, use of mental state verbs, inductive reasoning and narrative production (i.e., including causal explanation for events and explanation of characters' motivations in narrative) (Kelley et al., 2006, 2010). These residual difficulties were not severe enough to warrant an ASD diagnosis.
Research examining academic abilities among individuals who achieve OO remains limited and it is unclear whether academic intervention is necessary for this group. To date, only two studies reported on standardized measures of academic functioning (Butter et al., 2006; Sallows & Graupner, 2005) in this group and both found low average to average performance on measures of achievement. However, because the primary focus of these papers was not on academic functioning, the scope of these papers was somewhat limited. Specifically, Sallows and Graupner (2005) assessed reading, arithmetic and spelling, but did not report on written expression. Butter and colleagues (2006) described academic performance using an overall composite score, which may have masked the presence of residual difficulties within a single academic domain. Furthermore, both studies examined children of preschool to elementary school ages. During this period, academic tasks tend to rely on rote abilities, which are typically a relative strength among children with ASDs (Minshew et al., 1992; Wing, 1981). Therefore, it seems possible that academic deficits will be observed as children who achieve OO mature and academic tasks require more abstract reasoning.
We would expect that if residual deficits in academic functioning appear in children with OO, they are likely to affect the relatively weak domains in age-matched individuals with high-functioning autism (HFA). Academic abilities among middle to high school mainstreamed students with HFA are generally in the average range (Mayes et al., 2000; Mayes & Calhoun, 2003). However, some studies have reported relative weaknesses in reading comprehension, written expression and mathematical problem solving (Griswold et al., 2002; Mayes & Calhoun, 2003; Myles et al., 2001; Wahlberg & Magliano, 2004). These weaknesses may reflect previously identified deficits associated with ASDs, including social and communication deficits, circumscribed interests, difficulties with inferring meaning, comprehension of ambiguity and abstract concepts, as well as the ability to discriminate relevant from irrelevant information (Attwood, 1998; Dennis et al., 2001; Griswold et al., 2002; Happe, 1994; Jolliffe & Baron-Cohen, 1999; Jones et al., 2009; Tager-Flusberg, 1981; Wahlberg & Magliano, 2004).
The current study aims to examine the reading, writing, and arithmetic problem solving of a group of children and adolescents who were diagnosed with ASDs in early childhood, but who no longer meet diagnostic criteria for these disorders. We predict that the OO group will exhibit residual deficits in these domains but that these residual deficits will not be as pronounced in the OO group as they will in the HFA group. Because phonological decoding has not been identified as an area of weakness among individuals with HFA, deficits in this domain are not expected.
Methods
Participants
Participants included 32 individuals with a history of ASD who achieved OO, 41 high-functioning individuals with a current ASD diagnosis (HFA), and 34 typically developing peers (TD). These sample sizes were sufficient to detect effects in the medium to large range (Cohen, 1988). The participants in the study ranged from 8 years, 3 months to 21 years, 8 months. The groups were matched on age, gender, and nonverbal IQ (NVIQ) but were significantly different on verbal IQ (VIQ) (see Table 1). Seven participants in the HFA group and three participants in the OO group were recruited and evaluated at Queen's University in Kingston, Canada. These participants did not significantly differ from the larger sample on any of the measures. Participants were predominantly Caucasian, with only 8 participants reporting other races or ethnicities (3 in OO group, 2 in HFA group and 3 in TD group).
Table 1.
Participant characteristics.
| HFA | OO | TD | F/χ2 | p | Tukey | |
|---|---|---|---|---|---|---|
| N | 41 | 32 | 34 | |||
|
| ||||||
| Sex | 37 M; 4 F | 25 M; 7 F | 31 M; 3 F | 3.12 | 0.21 | |
|
| ||||||
| Age | 13.81 | 12.91 | 13.87 | 1.14 | 0.32 | |
| (2.67) | (3.47) | (2.58) | ||||
| (8.6-20.0) | (8.1-21.2) | (9.9-21.7) | ||||
|
| ||||||
| VIQa | 104.93 | 112.97 | 112.00 | 4.04 | 0.02 | HFA<OO, TD |
| (14.55) | (14.08) | (11.17) | ||||
| (81–142) | (80–137) | (93–138) | ||||
|
| ||||||
| NVIQa | 110.00 | 109.75 | 112.79 | 0.56 | 0.57 | |
| (13.02) | (15.17) | (11.32) | ||||
| (78–147) | (81–142) | (89–139) | ||||
|
| ||||||
| Vineland Communicationb | 82.76 | 98.26 | 93.32 | 14.97 | <.001 | HFA<OO, TD |
| (13.93) | (12.41) | (9.35) | ||||
| (42–108) | (79–122) | (74–119) | ||||
|
| ||||||
| Vineland Socializationb | 76.11 | 101.71 | 101.74 | 54.23 | <.001 | HFA<OO, TD |
| (16.33) | (8.61) | (8.56) | ||||
| (46–109) | (80–118) | (86–120) | ||||
|
| ||||||
| Vineland Daily Livingb | 75.92 | 91.65 | 88.76 | 13.98 | <.001 | HFA<OO, TD |
| (14.36) | (15.94) | (9.26) | ||||
| (46–110) | (65–120) | (74–115) | ||||
|
| ||||||
| ADOS–Communication | 3.59 | 0.47 | 0.41 | 124.99 | <.001 | HFA>OO, TD |
| (1.43) | (0.62) | (0.56) | ||||
| (2–7) | (0–2) | (0–2) | ||||
|
| ||||||
| ADOS–Socialization | 6.85 | 1.13 | 0.50 | 174.94 | <.001 | HFA>OO, TD |
| (2.25) | (1.34) | (0.75) | ||||
| (4–13) | (0–4) | (0–2) | ||||
Note. Table reports means, followed by SDs and ranges.
WASI subtest mean=100, SD=10.
VABS subtest mean=100, SD=10.
A subset of each group completed a standardized measure of written expression. No significant group differences were observed in the demographic characteristics of participants who completed this additional measure and those who did not. The measure used to assess writing ability for this study was developed for use in individuals younger than 17 years, 11 months of age; consequently, seven participants who were older than 17 years, 11 months were excluded from these analyses.
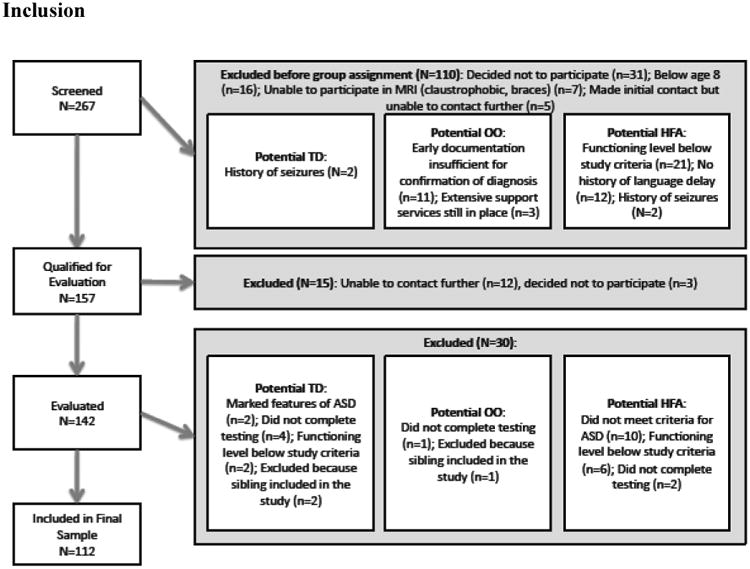
Recruitment was done through media outlets (newspaper stories, radio interviews), private practices, and clinic referrals. Recruitment materials stated that the study followed individuals “who have lost their ASD diagnosis and have reached an excellent outcome” and that individuals “with high functioning autism,” as well as with “typical development” were sought to participate as well. All three groups were recruited using the same materials and the same sites were used to recruit participants for the HFA and OO groups. In some cases, therapists contacted parents of children to participate either as OO or HFA participants, and in some cases, parents saw media reports and contacted the investigators. Participants were also referred from the principal investigators' private practices, the Psychological Services Clinic at the University of Connecticut, and from other ongoing studies at the University of Connecticut. Finally, some participants in each group were informed about the study by other participants' families. The study was approved by the Institutional Review Boards of the University of Connecticut, the Institute of Living Hartford Hospital, Children's Hospital of Philadelphia, and Queens University. See Figure 1 for a flow chart of inclusion and exclusion.
Figure 1. Flow Chart of Participant Inclusion.
Inclusion criteria
All participants were required to have verbal, nonverbal, and full-scale IQ standard scores greater than 77 (within 1.5 standard deviations of the average of 100). Other eligibility requirements applied specifically to the participant groups, as described below.
For the OO group:
Participants had a documented ASD diagnosis made by a physician or psychologist specializing in autism before the age of 5, verified in a written diagnostic report provided by parents. Early language delay (no words by 18 months or no phrases by 24 months) documented in the report was required. As a second step in confirming diagnosis, the report was edited to remove information about diagnosis, summary, and recommendations but leaving descriptions of behavior. An expert in diagnosis of ASD and Director of the University of Connecticut Psychological Services Clinic, reviewed these reports, blind to early diagnosis and current group membership. In addition to potential OO participants, she reviewed 24 “foil” reports for children with non-ASD diagnoses, such as global delay or language disorder. The blind reviewer had to determine whether enough core features of ASD were clearly evident to warrant an ASD diagnosis. Four potential OO participants were rejected for insufficient early documentation, and were dropped from the study. All 24 foils were correctly rejected. While this was not a prospective study, it is noteworthy that 11 of 32 OO participants (34%) received their initial diagnosis by members of this research team. In addition, the early diagnostic report of seven (22%) additional OO participants documented a standardized assessment of ASD symptomatology (i.e., included an ADOS, Autism Diagnostic Interview, or Childhood Autism Rating Scale).
Participants could not currently meet criteria for any ASD according to the Autism Diagnostic Observation Schedule (ADOS; Lord et al, 2000) administered by a research-reliable interviewer. In addition, the ADOS of all potential OO cases was reviewed by a clinician with more than 15 years of autism diagnostic experience who confirmed that ADOS scores were below ASD thresholds and that in their expert clinical judgment, an ASD was not present.
Participants' scores on the communication and socialization domains of the Vineland Adaptive Behavior Scales (VABS; Sparrow et al., 1984) had to be greater than 77 (within 1.5 SDs of the mean of 100) (see Table 4).
Participants had to be included in regular education classrooms with no one-on-one assistance and no special education services to address autism deficits (e.g., no social skills training). However, participants in this group could be receiving limited special education services to address impairments not specific to ASDs, such as attention or academic difficulties.
Table 4.
Performance on Passage Comprehension and Word Attack subtests of WJ-III.
| HFA | OO | TD | F/χ2 | p | ηp2 | Games-Howell | |
|---|---|---|---|---|---|---|---|
| N | 41 | 32 | 34 | ||||
|
| |||||||
| Word Attack | 103.49 | 102.75 | 104.50 | 0.28 | 0.76 | 0.01 | |
| (10.33) | (8.73) | (9.26) | |||||
| (82–127) | (83–121) | (86–129) | |||||
|
| |||||||
| Passage Comprehension | 99.90 | 107.59 | 110.91 | 8.28 | <.001 | 0.14 | HFA<TD |
| (12.08) | (14.80) | (8.78) | |||||
| (66–128) | (74–133) | (97–137) | |||||
Note. Table reports means, followed by SDs and ranges. WJ-III subtest mean=100, SD=15.
For the HFA group:
Following Collaborative Programs of Excellence in Autism diagnostic guidelines (Luyster et al, 2005), participants had to meet criteria for ASD on the ADOS (both Social and Communication domains and total score) and according to best estimate clinical judgment.
For the TD group:
Participants could not meet criteria for any ASD at any point in their development, by parent report. Parents had to deny having any social concerns about their child. In addition, parents completed as measured by the Social Communication Questionnaire (SCQ; Berument et al, 1999; TD mean=1.5, range: 0-4, well below the recommended instrument cutoff of 15).
Participants did not have a first-degree relative with an ASD.
Participants could not meet current diagnostic criteria for an ASD on the ADOS, or by clinical judgment (see Table 1). There was no attempt to exclude TD children for other learning or psychiatric disorders (but see general exclusion criteria).
Scores on the Communication and Socialization domains of the Vineland had to be greater than 77 (see Table 4).
Exclusion criteria
Potential participants for any group were excluded from the study if (1) at the time of the telephone screening they exhibited symptoms of major psychopathology (e.g., active psychotic disorder) that would impede their full participation in the study, (2) they had severe visual or hearing impairments, or (3) they had a history of seizure disorder, Fragile X syndrome, or significant head trauma with loss of consciousness.
Procedure
Phone screenings based on study criteria were conducted with parents of each potential participant. Those who passed initial screening were scheduled for an assessment. For participants under 18, parent consent and child assent was obtained prior to testing. For participants 18 and over, their informed consent was obtained. The evaluation was administered over two or three testing sessions at the University of Connecticut, the Institute of Living of Hartford Hospital, Queens University or the participant's home. Testing was conducted in a quiet room and lasted approximately six hours. In most cases, parent interviews were conducted concurrently by a second examiner and lasted approximately three hours for the OO and HFA groups and 1.5 hours for the TD group. Participants received monetary incentives for participation, even if testing could not be completed.
Measures
The Autism Diagnostic Observation Schedule (Lord et al., 2000) was used to determine whether the participants met diagnostic criteria for ASD at the time of the study. The “lifetime” score of the Social Communication Questionnaire (SCQ; Berument et al, 1999) was used to screen out TD children with a history of possible ASD. Cognitive abilities were measured using the Wechsler Abbreviated Scale of Intelligence (WASI; Wechsler, 1999). The Vineland Adaptive Behavior Scales (Sparrow et al., 1984) is a parent report measure used to evaluate adaptive functioning in Communication, Daily Living Skills and Socialization. The same cutoff for inclusion used in the OO and TD groups was not required of the HFA group on the VABS, because deficits in adaptive socialization and communication abilities are expected in this group. Academic functioning was assessed with subtests from the Woodcock-Johnson III, Test of Achievement (WJ-III; McGrew & Woodcock, 2001). Passage Comprehension was used to measure reading comprehension and asks the examinee to identify a key word that is missing from a written passage. The Word Attack subtest was used to assess decoding of phonically regular non-words. Mathematical problem solving was measured using the Applied Problems subtest.
The spontaneous writing sample from the Test of Written Language, Third Edition (TOWL-3; Hammill & Hresko, 1994) was used to measure written expression. Participants were asked to generate stories about a picture of a space scene and their narratives were used to assess three writing components: Contextual Conventions (e.g., punctuation, spelling), Contextual Language (e.g., sentence structure, vocabulary), and Story Construction (e.g., use of prose, action of the story). A second rater who was blind to group membership reviewed 10% of the stories and excellent inter-rater agreement was found for all three scores (all ICCs >0.95). The written narratives produced by each participant were also coded for lexical and pragmatic variables (see Table 2).
Table 2.
Performance on written expression measures.
| HFA | OO | TD | F | p | ηp2 | Tukey | |
|---|---|---|---|---|---|---|---|
| N | 30 | 27 | 29 | ||||
|
| |||||||
| TOWL-3 subtests: | |||||||
|
| |||||||
| Contextual Conventions | 10.10 | 11.22 | 10.34 | 0.99 | 0.38 | 0.02 | |
| (3.53) | (3.41) | (2.62) | |||||
| (3–19) | (4–18) | (6–16) | |||||
|
| |||||||
| Contextual Language | 10.47 | 11.89 | 12.24 | 2.36 | 0.10 | 0.05 | |
| (3.40) | (3.12) | (3.42) | |||||
| (5–18) | (7–18) | (4–20) | |||||
|
| |||||||
| Story Construction | 9.83 | 11.19 | 10.79 | 2.33 | 0.10 | 0.05 | |
| (2.69) | (1.86) | (2.65) | |||||
| (5–17) | (8–16) | (7–17) | |||||
|
| |||||||
| Lexical Variables: | |||||||
|
| |||||||
| Length in words | 145.79 | 190.38 | 198.67 | 1.66 | 0.20 | 0.04 | |
| (100.48) | (133.65) | (91.75) | |||||
| (42–487) | (61–619) | (47–385) | |||||
|
| |||||||
| Length in sentences | 9.14 | 15.69 | 15.19 | 4.33 | 0.02 | 0.10 | HFA<OO, TD |
| (6.80) | (11.03) | (8.01) | |||||
| (1–30) | (3–48) | (1–35) | |||||
|
| |||||||
| Mean sentence length | 15.68 | 13.20 | 15.18 | 1.10 | 0.34 | 0.03 | |
| (6.55) | (4.98) | (7.51) | |||||
| (6.6–39.5) | (6.4–23.3) | (7.3–47) | |||||
|
| |||||||
| Mean word length | 4.29 | 4.19 | 4.16 | 1.23 | 0.30 | 0.03 | |
| (0.38) | (0.29) | (0.29) | |||||
| (3.5–5) | (3.5–4.8) | (3.6–5.1) | |||||
|
| |||||||
| Pragmatic Variables: | |||||||
|
| |||||||
| Social words | 7.15 | 8.65 | 8.42 | 1.01 | 0.37 | 0.03 | |
| (4.53) | (3.64) | (4.42) | |||||
| (0–17.4) | (0–14.4) | (1.9–20.7) | |||||
|
| |||||||
| Positive emotion words | 0.86 | 1.03 | 1.48 | 1.81 | 0.17 | 0.04 | |
| (0.92) | (1.12) | (1.62) | |||||
| (0–2.9) | (0–3.7) | (0–7.1) | |||||
|
| |||||||
| Negative emotion words | 2.29 | 2.17 | 1.10 | 1.56 | 0.22 | 0.04 | |
| (3.46) | (3.06) | (1.07) | |||||
| (0–13.4) | (0–13.3) | (0–3.8) | |||||
|
| |||||||
| Cognitive words | 6.15 | 5.22 | 5.84 | 0.80 | 0.45 | 0.02 | |
| (3.01) | (2.25) | (2.93) | |||||
| (1.2–11.7) | (1.0–11.2) | (1.3–12.0) | |||||
|
| |||||||
| Causal attributions | 1.50 | 0.73 | 0.83 | 1.35 | 0.29 | 0.14 | |
| (2.51) | (0.75) | (1.33) | |||||
| (0–6) | (0–5) | (0–5) | |||||
Note. Table reports means, followed by SDs and ranges. TOWL-3 subtest mean=10, SD=3. Contextual Conventions measures conventional aspects of writing (e.g., punctuation, spelling, etc.). Contextual Language measures linguistic aspects of writing (e.g., sentence structure, vocabulary, etc.). Story Construction measures conceptual aspects of writing (e.g., use of prose, plot, etc.). Lexical variables were used to measure length of narrative by assessing total number of words and sentences (“length in words” and “length in sentences,” respectively), as well as the average number of words per sentence (“mean sentence length”) and characters per word (“mean word length”). Pragmatic variables included: percentage of words describing social processes (“social words”), positive emotions (“positive emotion words”), negative emotions (“negative emotions words”), cognitive processes (“cognitive words”) and causes of an action (“causal attributions”) relative to the total number of words in narrative.
Results
Scores of most measures met the assumptions of normality and homogeneity of variance. When homogeneity of variance was violated, the Games-Howell post-hoc test was used; in all other cases, the Tukey post-hoc test was used. One-way multivariate analyses of variance (MANOVAs) were run to examine group differences on subtests of reading and writing abilities. When overall tests were significant, univariate main effects were examined. Because the mathematics domain was measured by a single task, a one-way univariate analysis of variance (ANOVA) was conducted to examine group differences. These analyses were repeated with VIQ included as a covariate. Finally, chi-square tests were used to examine proportions of individuals within each group who scored more than one SD below the mean. Table 3 summarizes the significant findings.
Table 3. Summary of Results.
| Skill: | Significant Group Differences: |
|---|---|
| Reading: | |
| Word Decoding | -- |
| Passage Comprehension | HFA<TD |
| Writing: | |
| Conventional Aspects | -- |
| Linguistic Aspects | -- |
| Conceptual Aspects | -- |
| Lexical Aspects | Total number of sentences: HFA<TD, OO |
| Pragmatic Aspects | -- |
| Arithmetic: | |
| Mathematical Problem Solving | HFA<OO |
Reading
Participants in all three groups performed in the average range on the Passage Comprehension and Word Attack subtests of the WJ-III (see Table 4). A one-way MANOVA revealed a significant multivariate main effect for group (Wilks' λ=0.85, F(4,206)=4.431, p=.002, ηp2=.08). Univariate main effects showed that performance on Word Attack did not differ significantly among groups (F(2,104)=0.28, p=.76, ηp2=.01). However, a significant large univariate main effect was obtained for group membership on Passage Comprehension (F(2,104)=8.28, p<.001, ηp2=.14; Cohen, 1988). This difference remained significant when controlling for VIQ (F(2,103)=4.93, p=.01, ηp2=0.09). The Games-Howell post-hoc test revealed that the HFA group scored significantly lower on the Passage Comprehension subtest than the TD group (p<.001), while the difference between the OO and HFA group approached significance (p=.07). The OO and TD groups did not differ.
No significant group differences were found in the frequency of participants scoring lower than one SD below the mean on the reading subtests.
Written Expression
Participants in all three groups performed in the average range on the subtests of the TOWL-3 (see Table 2). A one-way MANOVA revealed no significant main effect for group (Wilks' λ=0.89, F(6,162)=1.56, p=.16, ηp2=.06). A secondary one-way MANOVA revealed no significant group differences on the lexical variables examining the number of words and sentences included in the writing samples, as well as the length of the sentences and words used (Wilks' λ=0.86, F(8,150)=1.47, p=.17, ηp2=.07), or on the pragmatic variables assessed (Wilks' λ=0.85, F(12,148)=0.99, p=.47, ηp2=.07). One-way ANOVAs, however, showed one significant group difference (Number of sentences) and two trends (Contextual Language and Story Construction), in which the HFA group scored lower than the other two groups.
No significant group differences for number of low-scoring participants were found on the Contextual Conventions and Contextual Language subtests. However, the HFA group had more participants (N=3) with low scores on the Story Construction subtest than both the OO and TD groups, who had none (χ2=5.91, p=.05).
Mathematical Problem Solving
Participants in all three groups scored solidly in the average range (see Table 5). One HFA participant was excluded from these analyses because his score on this measure fell more than two SDs below the mean and was considered an outlier. A one-way ANOVA revealed a significant group difference on this subtest (F(2,102)=4.49, p=.01, ηp2=0.09), which remained when controlling for NVIQ (F(2,101)=6.07, p=.01; ηp2=0.11) and approached significance when controlling for VIQ (F(2,101)=2.89, p=.06; ηp2=0.05). The HFA group scored significantly lower than the OO group on this measure (p=.01), while the difference in scores between the HFA and TD groups approached significance (p=.06). The OO and TD groups on this subtest did not differ. No group differences were found in the frequency of low-scoring participants.
Table 5.
Performance on Applied Problems subtest of WJ-III.
| HFA | OO | TD | F | p | ηp2 | Tukey | |
|---|---|---|---|---|---|---|---|
| N | 40 | 32 | 34 | ||||
|
| |||||||
| Applied Problems | 104.23 | 112.42 | 109.68 | 5.294 | 0.01 | 0.09 | HFA<OO |
| (12.79) | (11.81) | (10.54) | |||||
| (80–129) | (87–133) | (76–133) | |||||
Note. Table reports means, followed by SDs and ranges. WJ-III subtest mean=100, SD=15.
Discussion
This study investigated the academic abilities of individuals diagnosed with an ASD in early childhood, but who currently do not meet diagnostic criteria for any ASD. They presented with average IQs and adaptive skills, and were included in regular-education classrooms with no one-on-one support or special education services to address autism deficits. Two general findings are evident from the results of this study. First, contrary to predictions, the findings of this study suggest that the academic abilities of individuals who achieved OO are similar to those of their TD peers, even in areas where participants who have retained their ASD diagnoses exhibit some difficulty. Furthermore, the means of all three groups fell in the average range on the academic measures included. Second, significant academic differences were detected between the TD and HFA groups, helping to clarify the field's understanding of academic functioning among older children and adolescents with HFA.
Reading comprehension scores indicated no significant differences between the OO and TD groups, suggesting that individuals who achieve OO do not exhibit weaknesses in this academic domain. As predicted, the OO group scored higher than the HFA group on a measure of reading comprehension although it is important to reiterate that the HFA group also reached average levels on this measure. This is consistent with previous reports suggesting that despite average scores on measures of reading comprehension, children and adolescents with ASDs perform lower on these tasks than would be expected given their cognitive functioning and other academic skills (Church et al., 2000; Dennis et al., 2001; Goldstein et al., 1994; Jones et al., 2009; Mayes & Calhoun, 2003; Myles et al., 2001, 2002; Nation et al., 2006; Wahlberg & Magliano, 2004).
A lack of group difference in decoding is also consistent with prior studies documenting proficient reading accuracy in high-functioning students with ASDs (Goldstein et al., 1994; Mayes & Calhoun, 2003; Nation et al., 2006), and suggests that lower scores of the HFA group on reading comprehension are unlikely to be the result of decoding ability. In addition, group differences in reading comprehension remained significant even after controlling for VIQ and NVIQ, suggesting that this relative weakness is not due exclusively to the influence of cognitive ability. Instead, the lower than expected reading comprehension scores of the HFA group may reflect previously identified weaknesses, including interpreting language too literally, having trouble understanding idioms and metaphors, having difficulty inferring intentions of characters and constructing causal inferences between story events (Attwood, 1998; Happe, 1994; Jolliffe & Baron-Cohen, 1999; Tager-Flusberg, 1981).
An examination of writing abilities revealed that all three groups demonstrated a similarly developed level of mastery of the arbitrary conventions of written language, language use in writing, and the ability to construct a story. Participants in all three groups produced written narratives of similar lengths and included comparable number of descriptions of social, emotional, cognitive, and causal processes. The current results are contrary to the findings of Kelley and colleagues (2006), who found that the spoken narratives produced by the OO sample included significantly fewer references to causal processes than did TD peers. This inconsistency may be the result of the older sample included in this study (Kelley et al.'s sample was aged 5-9 years), as well as the difference in task used by the researchers (Kelley et al. asked children to narrate a story from a picture book).
These results also indicate that, on average, this HFA group did not exhibit deficits in writing ability that have been previously identified in the literature (i.e., Griswold et al, 2002; Mayes & Calhoun, 2003; Myles et al., 2001). However, significantly more members of the HFA group had some difficulty with story composition than both the OO and TD groups. In addition, the HFA group tended to score lower than the other groups in story construction and grammatical aspects of story constructions. It is possible that this HFA group performed better on measures of written expression than has been reported previously because participants were older and had higher cognitive abilities than in prior studies.
Performance of the OO group on a measure of mathematical problem solving also revealed no residual deficits in this domain. The HFA group got significantly lower scores on this task than did the OO group and this difference in scores was not driven by group differences in cognitive ability. Despite the significantly lower mean score, participants in the HFA group scored solidly in the average range on this measure. These results are consistent with the some previous reports of mathematical problem solving ability that documented scores in the average range, but lower than would be predicted by cognitive functioning abilities (Chiang & Lin, 2007; Griswold et al., 2002). The lower than expected performance on this measure of problem solving may result from inattention, impaired ability to understand abstract concepts and difficulty processing auditory information; all are common deficits seen in children with HFA (Attwood, 1998; Wing, 1981).
Taken together, these findings suggest that children and adolescents who achieve OO show high average to superior levels on tasks of decoding, reading comprehension, writing, and mathematical problem solving. From the results of this study it does not appear that this group exhibits any residual academic difficulties that would require intervention or academic support. These results also suggest that high-functioning children and adolescents with ASD also generally perform in the average range on measures of academic achievement. However, this group does exhibit significant relative weaknesses in the area of reading comprehension and mathematical problem solving that may require some academic support.
Limitations and Future Directions
The sample included in this study was relatively small and homogeneous in terms of functioning level, ethnic background and socioeconomic status. Consequently, it is difficult to determine how these results would generalize to a broader ASD sample.
Rather unexpectedly, given the required minimum of 77, the OO group's mean IQ fell in the high-average range. This raises the possibility that recruitment procedures and eligibility criteria may have skewed the group's functioning level upward. However, no minimum academic functioning level was required for participation. In other words, participants could have any IQ score above 77 and any level of academic functioning consistent with placement in a regular education classroom. However, no participants had to be excluded from the OO group because their functioning level fell below the study's criteria (see Figure 1) and academic skills of the OO group fell solidly in the average range, suggesting that the enrollment criteria do not account for the high-functioning level of the OO group. One possible explanation is that the above average intellectual abilities of the OO group are what allowed some individuals with ASD to compensate for some deficits and achieve OOs. It is also possible that families with children who are higher functioning were more likely to participate in this study. It is important to note that throughout the study, the groups were well-matched on NVIQ, suggesting that any sampling bias having to do with functioning was equivalent across groups. Another possibility to explain the high functioning level of the OO group is that the definition of OO used in recruitment (i.e., “reached excellent outcomes”) may have dissuaded participation among those who no longer met diagnostic criteria for ASD, but whose outcome was less than “excellent”. This definition was used to recruit individuals who achieved the most optimal outcome and may have excluded individual who no longer meet diagnostic criteria for ASD, but continue to exhibit cognitive deficits (such cases were described by Piven et al., 1996). While this group warrants further research, it is not the central goal of this study, which aimed to describe the best possible outcomes.
A power analysis revealed that the sample size used in this study would be sufficient to detect a medium to large sized effect, but was not large enough to detect a small to medium effect. Including a larger sample would allow for detecting subtle differences between the groups. These effects, however, would be of limited clinical significance.
To ensure accuracy of early ASD diagnoses of participants in the OO group, these diagnoses had to be made by an expert in diagnosing ASDs, documented in a diagnostic report, confirmed by a reviewer blind to early diagnosis and current group membership, (see Inclusion Criteria for more details). However, we recognize that a retrospective record review study is not ideal and that a prospective study would be preferable. Review of the literature suggests that fewer than anywhere between 3 and 25% of children diagnosed with ASD may achieve OOs (Helt et al., 2008) and specific predictors of OOs are unknown. Consequently, prospective studies of this group would require a longitudinal follow-up of a large sample of children with ASDs in order to gain a large enough sample of individuals who achieve an OO and are not lost to attrition. Such a prospective study would be very costly, but would ensure that early diagnoses were accurately made. In addition, having access to measures of early abilities for participants who go on to achieve OO would also allow researchers to draw conclusions about early factors that have contributed to this outcome.
Measures of academic functioning included in this study were collected in an optimal environment in which distractions were limited and an adult was present to encourage the participant to remain on task. It is difficult to determine how these results would differ if measures of academic abilities were collected in a classroom environment. Given the findings that individuals who achieve OO exhibit significantly more symptoms of attentional difficulties than TD peers (Fein et al., 2005; Tyson et al., 2010), it is possible that this group would exhibit residual weaknesses in academic abilities if these were measured in a less ideal environment.
Finally, it is possible that the measures selected to examine academic functioning for this study were not sensitive enough to detect subtle differences in academic skills that exist between the TD and OO groups. Future studies may benefit from examining residual deficits between the OO and TD groups using more extensive and complex academic tasks, including persuasive writing assignments and reading comprehension tasks that require reading longer passages and answering more complex questions. If residual deficits are uncovered, more extensive measures of academic ability will enable researchers to examine aspects necessary for each academic domain. This will allow for the identification of specific skills that present difficulties for the OO group and will allow for more targeted, and likely more effective intervention.
The current study is one of the first to characterize the academic functioning in a group of children with a history of ASD who have achieved positive outcomes marked by the absence of ASD symptoms, average cognitive and adaptive functioning, as well as inclusion in regular education. These results suggest that individuals who achieve OO are appropriately included in regular-education classrooms and academic intervention does not appear necessary, even in domains that remain weak in high functioning individuals who retain their ASD diagnosis. Overall, these results support the existence of a group of individuals who were diagnosed with ASD in childhood, but who have achieved OO. Future studies should aim to describe the characteristics of the children and the interventions that can lead to such excellent outcome, and to elucidate the mechanisms that make it possible.
Acknowledgments
We thank Drs. Letitia Naigles, Marianne Barton, Elizabeth Kelley, Robert Schultz and Michael Rosenthal for their assistance with this project, our undergraduate research assistants who were immensely helpful with data entry, the parents and children who participated in this study and the funding agency, the National Institutes of Mental Health (R01MH076189).
References
- Attwood T. Asperger's syndrome: A guide to parents and professionals. London: Jessica Kingsley; 1998. [Google Scholar]
- Berument S, Rutter M, Lord C, Pickles A, Bailey A. Autism screening questionnaire: Diagnostic validity. The British Journal of Psychiatry. 1999;175:444–451. doi: 10.1192/bjp.175.5.444. [DOI] [PubMed] [Google Scholar]
- Butter EM, Mulick JA, Metz B. Eight case reports of learning recovery in children with pervasive developmental disorder after early intervention. Behavioral Interventions. 2006;21(4):227–243. [Google Scholar]
- Chiang H, Lin Y. Mathematical ability of students with Asperger syndrome and high-functioning autism. Autism. 2007;11(6):547–556. doi: 10.1177/1362361307083259. [DOI] [PubMed] [Google Scholar]
- Church C, Alisanski S, Amanullah S. The social, behavioral, and academic experiences of children with Asperger Syndrome. Focus on Autism and Other Developmental Disabilities. 2000;15(1):12–20. [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. Second. Hillsdale: Lawrence Erlbaum Associates, Publishers; 1988. [Google Scholar]
- Cohen H, Amerine-Dickens M, Smith T. Early intensive behavioral treatment: Replication of the UCLA model in a community setting. Developmental and Behavioral Pediatrics. 2007;27(2):S145–S155. doi: 10.1097/00004703-200604002-00013. [DOI] [PubMed] [Google Scholar]
- Dennis M, Lazenby AL, Lockyer L. Inferential language in high-functioning children with autism. Journal of Autism and Developmental Disorders. 2001;31(1):47–54. doi: 10.1023/a:1005661613288. [DOI] [PubMed] [Google Scholar]
- Fein D, Dixon P, Paul J, et al. Brief report: Pervasive Developmental Disorder can evolve into ADHD: case illustrations. Journal of Autism and Developmental Disorders. 2005;35(4):525–534. doi: 10.1007/s10803-005-5066-3. [DOI] [PubMed] [Google Scholar]
- Goldstein G, Minshew NJ, Siegel DJ. Age differences in academic achievement in high-functioning autistic individuals. Journal of Clinical and Experimental Neuropsychology. 1994;16(5):671–680. doi: 10.1080/01688639408402680. [DOI] [PubMed] [Google Scholar]
- Griswold DE, Barnhill GP, Myles BS, et al. Asperger syndrome and academic achievement. Focus on Autism and Other Developmental Disorders. 2002;17(2):94–102. [Google Scholar]
- Hammill DD, Hresko WP. Comprehensive Scales of Student Abilities. Austin: PRO-ED, Inc; 1994. [Google Scholar]
- Happe FG. An advanced test of theory of mind: understanding of story characters' thoughts and feelings by able autistic, mentally handicapped, and normal children and adults. Journal of Autism and Developmental Disorders. 1994;24(2):129–54. doi: 10.1007/BF02172093. [DOI] [PubMed] [Google Scholar]
- Harris SL, Handleman JS. Age and IQ at intake as predictors of placement for young children with autism: A four- to six-year follow-up. Journal of Autism and Developmental Disorders. 2000;30(2):137–142. doi: 10.1023/a:1005459606120. [DOI] [PubMed] [Google Scholar]
- Helt M, Kelley E, Kinsbourne M, et al. Can children with autism recover? If so, how? Neuropsychology Review. 2008;18(4):339–366. doi: 10.1007/s11065-008-9075-9. [DOI] [PubMed] [Google Scholar]
- Howlin P, Goode S, Hutton J, et al. Adult outcome for children with autism. Journal of Child Psychology and Psychiatry. 2004;45(2):212–229. doi: 10.1111/j.1469-7610.2004.00215.x. [DOI] [PubMed] [Google Scholar]
- Jolliffe T, Baron-Cohen S. A test of central coherence theory: linguistic processing in high-functioning adults with autism or Asperger syndrome: is local coherence impaired? Cognition. 1999;71(2):149–85. doi: 10.1016/s0010-0277(99)00022-0. [DOI] [PubMed] [Google Scholar]
- Jones CRG, Golden H, Simonoff E, et al. Reading and arithmetic in adolescents with autism spectrum disorders: Peaks and dips in attainment. Neuropsychology. 2009;23(6):718–728. doi: 10.1037/a0016360. [DOI] [PubMed] [Google Scholar]
- Kelley E, Paul JJ, Fein D, et al. Residual language deficits in OO children with a history of autism. Journal of Autism and Developmental Disorders. 2006;36(6):807–828. doi: 10.1007/s10803-006-0111-4. [DOI] [PubMed] [Google Scholar]
- Kelley E, Naigles LR, Fein D. An in-depth examination of optimal outcome children with a history of autism spectrum disorders. Research in Autism Spectrum Disorders. 2010;4(3):526–538. [Google Scholar]
- Lord C, Risi S, Lambrecht L, et al. The Autism Diagnostic Observation Schedule-Generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders. 2000;30(3):205–223. [PubMed] [Google Scholar]
- Lovaas OI. Behavioral treatment and normal educational and intellectual functioning in young autistic children. Journal of Consulting and Clinical Psychology. 1987;55(1):3–9. doi: 10.1037//0022-006x.55.1.3. [DOI] [PubMed] [Google Scholar]
- Luyster R, Richler J, Risi S, Hsu WL, Dawson G, Bernier R, et al. Lord C. Early regression in social communication in autistic spectrum disorders: A CPEA study. Developmental Neuropsychology. 2005;27:311–336. doi: 10.1207/s15326942dn2703_2. [DOI] [PubMed] [Google Scholar]
- Mayes SD, Calhoun SL. Ability profiles in children with autism: Influence of age and IQ. Autism. 2003;7(1):65–80. doi: 10.1177/1362361303007001006. [DOI] [PubMed] [Google Scholar]
- Mayes SD, Calhoun SL, Crowell EW. Learning disabilities and ADHD: Overlapping spectrum disorders. Journal of Learning Disabilities. 2000;33(5):417–424. doi: 10.1177/002221940003300502. [DOI] [PubMed] [Google Scholar]
- McGrew KS, Woodcock RJ. Technical manual: Woodcock-Johnson III. Itasca; Riverside: 2001. [Google Scholar]
- Minshew NJ, Goldstein G, Muenz IR, et al. Neuropsychological functioning in nonmentally retarded autistic individuals. Journal of Clinical and Experimental Neuropsychology. 1992;14(5):749–761. doi: 10.1080/01688639208402860. [DOI] [PubMed] [Google Scholar]
- Myles BS, Barnhill GP, Hagiwara T, et al. A synthesis of studies on the intellectual, academic, social/emotional and sensory characteristics of children and youth with Asperger syndrome. Education and Training in Mental Retardation and Developmental Disabilities. 2001;36(September):304–311. [Google Scholar]
- Myles BS, Hilgenfeld TD, Barnhill GP, et al. Analysis of reading skills in individuals with Asperger syndrome. Focus on Autism and Other Developmental Disabilities. 2002;17(1):44–47. [Google Scholar]
- Nation K, Clarke P, Wright B, et al. Patterns of reading ability in children with autism spectrum disorder. Journal of Autism and Developmental Disorders. 2006;36(7):911–919. doi: 10.1007/s10803-006-0130-1. [DOI] [PubMed] [Google Scholar]
- Rutter M. Autistic children: Infancy to adulthood. Seminars in Psychiatry. 1970;2(4):435–450. [PubMed] [Google Scholar]
- Sallows GO, Graupner TD. Intensive behavioral treatment for children with autism: Four-year outcome and predictors. American Journal of Mental Retardation. 2005;110(6):417–438. doi: 10.1352/0895-8017(2005)110[417:IBTFCW]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Seltzer MM, Shattuck P, Abbeduto L, et al. Trajectory of development in adolescents and adults with autism. Mental Retardation and Developmental Disabilities Research Reviews. 2004;10(4):234–247. doi: 10.1002/mrdd.20038. [DOI] [PubMed] [Google Scholar]
- Sigman M, Ruskin E. Continuity and change in the social competence of children with autism, Down syndrome, and developmental delays. Monographs of the Society for Research in Child Development. 1999;64(1):109–113. doi: 10.1111/1540-5834.00002. [DOI] [PubMed] [Google Scholar]
- Sparrow SS, Balla DA, Cicchetti DV. Vineland Adaptive Behavior Scales: Interview Edition, Survey Form Manual. Circle Pines: American Guidance Service; 1984. [Google Scholar]
- Sutera S, Pandey J, Esser EL, et al. Predictors of optimal outcome in toddlers diagnosed with autism spectrum disorders. Journal of Autism and Developmental Disorders. 2007;37(1):98–107. doi: 10.1007/s10803-006-0340-6. [DOI] [PubMed] [Google Scholar]
- Szatmari P, Bartolucci G, Bremner R, et al. A follow-up study of high-functioning autistic children. Journal of Autism and Developmental Disorders. 1989;19(2):213–225. doi: 10.1007/BF02211842. [DOI] [PubMed] [Google Scholar]
- Tager-Flusberg H. Sentence comprehension in autistic children. Applied Psycholinguistics. 1981;2(1):5–24. [Google Scholar]
- Tyson K, Troyb E, Rosenthal M, et al. Psychiatric Symptoms and Comorbidities in Children with a History of Autism who Achieve an “Optimal Outcome”; International Meeting for Autism Research; Philadelphia, USA. 20-22 May 2010.2010. [Google Scholar]
- Venter A, Lord C, Schopler E. A follow-up study of high-functioning autistic children. Journal of Child Psychology and Psychiatry. 1992;33(3):489–597. doi: 10.1111/j.1469-7610.1992.tb00887.x. [DOI] [PubMed] [Google Scholar]
- Wahlberg T, Magliano JP. The ability of high functioning individuals with autism to comprehend written discourse. Discourse Processing. 2004;38(1):119–144. [Google Scholar]
- Wechsler D. Wechsler Abbreviated Scale of Intelligence (WASI) San Antonio: Harcourt Assessment; 1999. [Google Scholar]
- Weiss MJ. Differential rates of skill acquisition and outcomes of early intensive behavioral intervention for autism. Behavioral Interventions. 1999;14(1):3–22. [Google Scholar]
- Wing L. Asperger's syndrome: A clinical account. Psychological Medicine. 1981;11(1):115–129. doi: 10.1017/s0033291700053332. [DOI] [PubMed] [Google Scholar]
- Zachor DA, Ben-Itzchak E, Rabinovich AL, et al. Change in autism core symptoms with intervention. Research in Autism Spectrum Disorders. 2007;1(4):304–317. [Google Scholar]