

Abstract
Ectopic varices are unusual with portal hypertension and can involve any site along the digestive tract outside the gastroesophageal region. Hemorrhage from ectopic varices generally are massive and life threatening. Diagnosis of ectopic varices is difficult and subsequent treatment is also difficult; the optimal treatment has not been established. Recently, interventional radiology and endoscopic treatments have been carried out successfully for hemorrhage from ectopic varices.
Keywords: Portal hypertension, Endoscopic injection sclerotherapy, Balloon-occluded retrograde transvenous obliteration, Ectopic varices, Endoscopic band ligation, Percutaneous transhepatic obliteration, Transjugular intrahepatic portosystemic shunts
Core tip: Ectopic varices with portal hypertension are considered to be the cause of hemorrhage presenting as lower gastrointestinal bleeding. Recently, interventional radiology and endoscopic procedures have been performed successfully as a treatment option for ectopic varices.
INTRODUCTION
Portal hypertension results from an increase in the resistance of blood flow in the intrahepatic portal vein and can cause the reopening of embryonic channels[1]. Portal venous pressure is critical in the liver function of cirrhosis and esophageal varices are the most common complication of cirrhosis. Ectopic varices are portosystemic collaterals along the digestive tract outside the gastroesophageal region and are unusual[2,3]. Endoscopic procedures such as endoscopic injection sclerotherapy (EIS) and endoscopic band ligation (EBL) have been carried out for treating esophageal varices[4,5]. Balloon-occluded retrograde transvenous obliteration (B-RTO) is an angiographic technique for fundic varices of stomach[6]. But, the optimal procedure has not been defined for hemorrhage from ectopic varices.
Here, we review the options in the treatment of hemorrhaging ectopic varices.
ECTOPIC VARICES
The majority of portosystemic collaterals with portal hypertension are located in the esophagus and stomach and, especially, esophageal varices are the most common site. Ectopic variceal bleeding is massive and serious condition. Other sites of ectopic varices are the duodenum, small intestine, colon, rectum, and the peritoneum[7]. A current survey of ectopic varices in Japan has been reported and the most frequent sites of ectopic varices are the rectum in 44.5%, followed by the duodenum in 32.9%[8].
Rectal varices
Rectal varices are a consequence of portosystemic collaterals from the superior rectal veins to the middle inferior rectal veins. Endoscopy can detect the discrete dilated submucosal varices in the rectum and some investigators have reported that rectal varices occur at a high frequency[9-11]. Hemorrhage from rectal varices occurs at a low frequency from 0.5% to 3.6%[12-14].
Several medical procedures have been performed for controlling rectal variceal bleeding, however, a standard treatment has not been established.
Surgical procedures such as portosystemic shunting, ligation, and under-running suturing, also have been reported[9]. Interventional radiologic techniques, including transjugular intrahepatic portosystemic shunts (TIPS), have been performed successfully for bleeding rectal varices[15-17].
As an endoscopic treatment, Wang et al[18] used EIS for rectal variceal bleeding. EBL has been performed as an effective procedure for rectal varices[19-21] and Levine et al[19] used EBL successfully for the rectal varices remaining after EIS. EBL is a safe and effective treatment for rectal varices. However, a retrospective study comparing EIS and EBL concluded that recurrence rate tended to be greater with EBL[22] and stated that 5% ethanolamine oleate of the sclerosant should be carefully injected using fluoroscopy, avoiding injection into the systemic circulation. Sato et al[22] evaluated the efficacy of EIS for rectal varices and reported that EIS was a useful and safe treatment for rectal varices with regard to effectiveness and complication[23].
Case presentation
EBL for rectal varices: Endoscopic finding of liver cirrhosis with anal bleeding revealed enlarged and tortuous, erosion positive rectal varices (Figure 1A), and endoscopic band ligation was performed successfully (Figure 1B).
Figure 1.
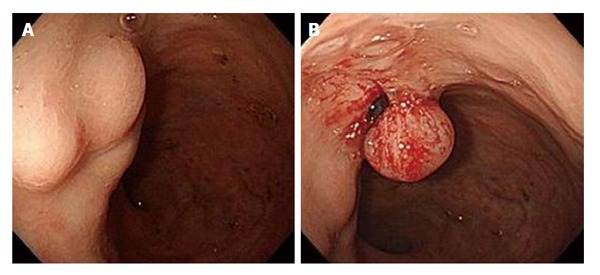
Endoscopy showed enlarged and tortuous, erosion positive rectal varices in a cirrhotic patient with anal bleeding (A) and endoscopic band ligation was performed successfully (B).
EIS for rectal varices: EIS was performed using a flexible gastrointestinal endoscope, with a transparent hood attached to the tip, and the injection needle was placed into the varices (Figure 2A). Fluoroscopic observation with infusion of 5% ethanolamine oleate with iopamidol was made to determine the extent of the varices (Figure 2B).
Figure 2.
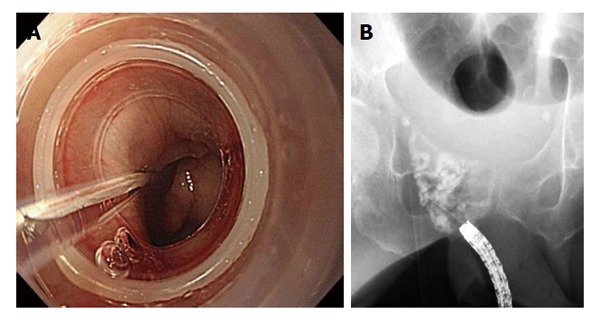
Endoscopic injection sclerotherapy was performed using a transparent hood attached to the tip and injection needle placed into the varices (A) and fluoroscopic observation with infusion of 5% ethanolamine oleate with iopamidol was made to determine the extent of the varices (B).
Duodenal varices
Hemorrhage from duodenal varices is low frequent, however, it is often serious condition[24]. The hemodynamics of duodenal varices involved the development of collateral veins between the portal vein trunk or superior mesenteric vein and the inferior vena cava[25]. Hemorrhage from duodenal varices is generally massive and fatal[25,26]. The diagnosis of duodenal varices is done ordinary by endoscopic examination, however, it is often difficult to observe hemorrhaging duodenal varices. The common site of duodenal varices is the duodenal bulb[26], ranked next the second portion of the duodenum[27]. In the United States and Europe, varices of the duodenal bulb occur most frequently because of extrahepatic portal obstruction, causing portal hypertension. On the other hand, in Japan, common site of duodenal varices is the second portion of the duodenum. In addition, hemorrhage from duodenal varices in the distal third portion is very rare[28,29].
Recently, interventional radiology and endoscopic treatments have been performed successfully for duodenal varices. EBL is useful for obtaining hemostasis[30,31], however, re-bleeding of varices is an weak point with EBL. EIS has been performed successfully for the treatment of duodenal variceal bleeding[32,33] but there were serious problem of re-bleeding of the varices[34,35]. N-butyl-2-cyanoacrylate is a tissue glue monomer; upon contact with blood, it immediately polymerizes and solidifies, resultings in hemostasis of variceal bleeding. Endoscopic therapy using N-butyl-2-cyanoacrylate is also very useful for massive duodenal variceal bleeding[29,30] because of the high blood velocity and blood flow. Interventional radiologic techniques such as TIPS, B-RTO, and percutaneous transhepatic obliteration (PTO) are options for hemorrhaging duodenal varices and successful treatments have been reported, including TIPS[26] and B-RTO[35-37]. B-RTO is able to obliterate the afferent and efferent veins and may be considered as a treatment option for duodenal varices. PTO also has been used successfully in some cases[38,39].
Case presentation
Endoscopic treatment using cyanoacrylate for duodenal varices: Endoscopy of liver cirrhosis with massive melena revealed tortuous duodenal varices in the anterior wall of the second portion (Figure 3A). N-butyl-2-cyanoacrylate was injected with contrast medium into the duodenal varices on fluoroscopic observation (Figure 3B).
Figure 3.
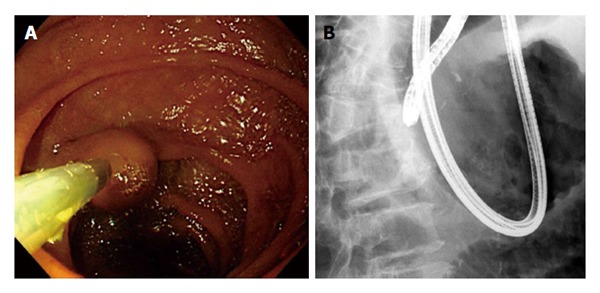
Endoscopy revealed tortuous duodenal varices in the anterior wall of the second portion (A) and N-butyl-2-cyanoacrylate was injected with contrast medium into the duodenal varices on fluoroscopic observation (B).
Small intestinal varices
Bleeding from jejunal and ileal varices may be massive and serious and it is difficult to achieve early diagnosis. Most cases are detected following intra-abdominal surgery. The development of collateral circulation via the post-operative adhesions is a risk factor of small intestinal varices in patients with portal hypertension.
Many literatures of hemorrhaging jejunal[40-45] and ileal varices[46-54] have been described. Bleeding small intestinal varices are as follows: portal hypertension, hematochezia without hematemesis, and previous abdominal surgery[55]. Several treatments are available for jejunal varices, such as surgery[40], portal venous stenting[42,44,45] and percutaneous embolization[40,43], and surgery has been used successfully for bleeding ileal varices[50,51,56,57]. In ileal variceal patients with a serious condition, angiographic techniques including TIPS have been used successfully as a non-surgical approach[3,52,54]. B-RTO is also practical for treating ileal varices[58,59] and it also may be used for patients in a serious condition.
CONCLUSION
Ectopic varices in patients with portal hypertension are considered to be the cause of hemorrhage presenting with lower gastrointestinal bleeding, and recently, their frequency has been increasing.
The diagnosis of ectopic varices and subsequent treatment are difficult. Recently, interventional radiology and endoscopic treatments have been performed successfully for ectopic varices. More investigations are necessary in a large number of patients.
Footnotes
P- Reviewer: Genesca J, Ong HT S- Editor: Ji FF L- Editor: A E- Editor: Liu SQ
Conflict-of-interest: The author declared no conflicts of interest.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: January 18, 2015
First decision: February 7, 2015
Article in press: April 14, 2015
References
- 1.Walsh G, Williams MP. Case report: giant pararectal varices--computed tomographic appearances. Br J Radiol. 1995;68:203–204. doi: 10.1259/0007-1285-68-806-203. [DOI] [PubMed] [Google Scholar]
- 2.Kinkhabwala M, Mousavi A, Iyer S, Adamsons R. Bleeding ileal varicosity demonstrated by transhepatic portography. AJR Am J Roentgenol. 1977;129:514–516. doi: 10.2214/ajr.129.3.514. [DOI] [PubMed] [Google Scholar]
- 3.Norton ID, Andrews JC, Kamath PS. Management of ectopic varices. Hepatology. 1998;28:1154–1158. doi: 10.1002/hep.510280434. [DOI] [PubMed] [Google Scholar]
- 4.Prophylactic sclerotherapy for esophageal varices in men with alcoholic liver disease. A randomized, single-blind, multicenter clinical trial. The Veterans Affairs Cooperative Variceal Sclerotherapy Group. N Engl J Med. 1991;324:1779–1784. doi: 10.1056/NEJM199106203242505. [DOI] [PubMed] [Google Scholar]
- 5.Goff JS, Reveille RM, Van Stiegmann G. Endoscopic sclerotherapy versus endoscopic variceal ligation: esophageal symptoms, complications, and motility. Am J Gastroenterol. 1988;83:1240–1244. [PubMed] [Google Scholar]
- 6.Kanagawa H, Mima S, Kouyama H, Gotoh K, Uchida T, Okuda K. Treatment of gastric fundal varices by balloon-occluded retrograde transvenous obliteration. J Gastroenterol Hepatol. 1996;11:51–58. doi: 10.1111/j.1440-1746.1996.tb00010.x. [DOI] [PubMed] [Google Scholar]
- 7.Lebrec D, Benhamou JP. Ectopic varices in portal hypertension. Clin Gastroenterol. 1985;14:105–121. [PubMed] [Google Scholar]
- 8.Watanabe N, Toyonaga A, Kojima S, Takashimizu S, Oho K, Kokubu S, Nakamura K, Hasumi A, Murashima N, Tajiri T. Current status of ectopic varices in Japan: Results of a survey by the Japan Society for Portal Hypertension. Hepatol Res. 2010;40:763–776. doi: 10.1111/j.1872-034X.2010.00690.x. [DOI] [PubMed] [Google Scholar]
- 9.Hosking SW, Smart HL, Johnson AG, Triger DR. Anorectal varices, haemorrhoids, and portal hypertension. Lancet. 1989;1:349–352. doi: 10.1016/s0140-6736(89)91724-8. [DOI] [PubMed] [Google Scholar]
- 10.Wang TF, Lee FY, Tsai YT, Lee SD, Wang SS, Hsia HC, Lin WJ, Lin HC, Lai KH, Chan CY. Relationship of portal pressure, anorectal varices and hemorrhoids in cirrhotic patients. J Hepatol. 1992;15:170–173. doi: 10.1016/0168-8278(92)90031-j. [DOI] [PubMed] [Google Scholar]
- 11.Chawla Y, Dilawari JB. Anorectal varices--their frequency in cirrhotic and non-cirrhotic portal hypertension. Gut. 1991;32:309–311. doi: 10.1136/gut.32.3.309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.McCormack TT, Bailey HR, Simms JM, Johnson AG. Rectal varices are not piles. Br J Surg. 1984;71:163. doi: 10.1002/bjs.1800710236. [DOI] [PubMed] [Google Scholar]
- 13.Johansen K, Bardin J, Orloff MJ. Massive bleeding from hemorrhoidal varices in portal hypertension. JAMA. 1980;244:2084–2085. [PubMed] [Google Scholar]
- 14.Wilson SE, Stone RT, Christie JP, Passaro E. Massive lower gastrointestinal bleeding from intestinal varices. Arch Surg. 1979;114:1158–1161. doi: 10.1001/archsurg.1979.01370340064011. [DOI] [PubMed] [Google Scholar]
- 15.Katz JA, Rubin RA, Cope C, Holland G, Brass CA. Recurrent bleeding from anorectal varices: successful treatment with a transjugular intrahepatic portosystemic shunt. Am J Gastroenterol. 1993;88:1104–1107. [PubMed] [Google Scholar]
- 16.Shibata D, Brophy DP, Gordon FD, Anastopoulos HT, Sentovich SM, Bleday R. Transjugular intrahepatic portosystemic shunt for treatment of bleeding ectopic varices with portal hypertension. Dis Colon Rectum. 1999;42:1581–1585. doi: 10.1007/BF02236211. [DOI] [PubMed] [Google Scholar]
- 17.Fantin AC, Zala G, Risti B, Debatin JF, Schöpke W, Meyenberger C. Bleeding anorectal varices: successful treatment with transjugular intrahepatic portosystemic shunting (TIPS) Gut. 1996;38:932–935. doi: 10.1136/gut.38.6.932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wang M, Desigan G, Dunn D. Endoscopic sclerotherapy for bleeding rectal varices: a case report. Am J Gastroenterol. 1985;80:779–780. [PubMed] [Google Scholar]
- 19.Levine J, Tahiri A, Banerjee B. Endoscopic ligation of bleeding rectal varices. Gastrointest Endosc. 1993;39:188–190. doi: 10.1016/s0016-5107(93)70067-x. [DOI] [PubMed] [Google Scholar]
- 20.Firoozi B, Gamagaris Z, Weinshel EH, Bini EJ. Endoscopic band ligation of bleeding rectal varices. Dig Dis Sci. 2002;47:1502–1505. doi: 10.1023/a:1015802732217. [DOI] [PubMed] [Google Scholar]
- 21.Sato T, Yamazaki K, Toyota J, Karino Y, Ohmura T, Suga T. Two cases of rectal varices treated by endoscopic variceal ligation. Dig Endosc. 1999;11:66–69. [Google Scholar]
- 22.Sato T, Yamazaki K, Toyota J, Karino Y, Ohmura T, Suga T. The value of the endoscopic therapies in the treatment of rectal varices: a retrospective comparison between injection sclerotherapy and band ligation. Hepatol Res. 2006;34:250–255. doi: 10.1016/j.hepres.2006.01.007. [DOI] [PubMed] [Google Scholar]
- 23.Sato T. Treatments for rectal varices with portal hypertension. J Gastroint Dig Syst. 2013:S6. [Google Scholar]
- 24.D’Imperio N, Piemontese A, Baroncini D, Billi P, Borioni D, Dal Monte PP, Borrello P. Evaluation of undiluted N-butyl-2-cyanoacrylate in the endoscopic treatment of upper gastrointestinal tract varices. Endoscopy. 1996;28:239–243. doi: 10.1055/s-2007-1005435. [DOI] [PubMed] [Google Scholar]
- 25.Khouqeer F, Morrow C, Jordan P. Duodenal varices as a cause of massive upper gastrointestinal bleeding. Surgery. 1987;102:548–552. [PubMed] [Google Scholar]
- 26.Jonnalagadda SS, Quiason S, Smith OJ. Successful therapy of bleeding duodenal varices by TIPS after failure of sclerotherapy. Am J Gastroenterol. 1998;93:272–274. doi: 10.1111/j.1572-0241.1998.270_3.x. [DOI] [PubMed] [Google Scholar]
- 27.Wang CS, Jeng LB, Chen MF. Duodenal variceal bleeding--successfully treated by mesocaval shunt after failure of sclerotherapy. Hepatogastroenterology. 1995;42:59–61. [PubMed] [Google Scholar]
- 28.Shiraishi M, Hiroyasu S, Higa T, Oshiro S, Muto Y. Successful management of ruptured duodenal varices by means of endoscopic variceal ligation: report of a case. Gastrointest Endosc. 1999;49:255–257. doi: 10.1016/s0016-5107(99)70498-0. [DOI] [PubMed] [Google Scholar]
- 29.Yoshida Y, Imai Y, Nishikawa M, Nakatukasa M, Kurokawa M, Shibata K, Shimomukai H, Shimano T, Tokunaga K, Yonezawa T. Successful endoscopic injection sclerotherapy with N-butyl-2-cyanoacrylate following the recurrence of bleeding soon after endoscopic ligation for ruptured duodenal varices. Am J Gastroenterol. 1997;92:1227–1229. [PubMed] [Google Scholar]
- 30.Ota K, Shirai Z, Masuzaki T, Tanaka K, Higashihara H, Okazaki M, Arakawa M. Endoscopic injection sclerotherapy with n-butyl-2-cyanoacrylate for ruptured duodenal varices. J Gastroenterol. 1998;33:550–555. doi: 10.1007/s005350050131. [DOI] [PubMed] [Google Scholar]
- 31.Selçuk H, Boyvat F, Eren S, Korkmaz M, Gür G, Yilmaz U, Boyacioğlu S. Duodenal varices as an unusual cause of gastrointestinal bleeding due to portal hypertension: a case report. Turk J Gastroenterol. 2004;15:104–107. [PubMed] [Google Scholar]
- 32.Gertsch P, Blumgart LH. Cure of a bleeding duodenal varix by sclerotherapy. Br J Surg. 1988;75:717. doi: 10.1002/bjs.1800750731. [DOI] [PubMed] [Google Scholar]
- 33.Barbish AW, Ehrinpreis MN. Successful endoscopic injection sclerotherapy of a bleeding duodenal varix. Am J Gastroenterol. 1993;88:90–92. [PubMed] [Google Scholar]
- 34.Hashiguchi M, Tsuji H, Shimono J, Azuma K, Fujishima M. Ruptured duodenal varices: an autopsy case report. Hepatogastroenterology. 1999;46:1751–1754. [PubMed] [Google Scholar]
- 35.Ohta M, Yasumori K, Saku M, Saitsu H, Muranaka T, Yoshida K. Successful treatment of bleeding duodenal varices by balloon-occluded retrograde transvenous obliteration: a transjugular venous approach. Surgery. 1999;126:581–583. [PubMed] [Google Scholar]
- 36.Akazawa Y, Murata I, Yamao T, Yamakawa M, Kawano Y, Nomura N, Isomoto H, Mizuta Y, Murase K, Kohno S. Successful management of bleeding duodenal varices by endoscopic variceal ligation and balloon-occluded retrograde transvenous obliteration. Gastrointest Endosc. 2003;58:794–797. doi: 10.1016/s0016-5107(03)02008-x. [DOI] [PubMed] [Google Scholar]
- 37.Sonomura T, Horihata K, Yamahara K, Dozaiku T, Toyonaga T, Hiroka T, Sato M. Ruptured duodenal varices successfully treated with balloon-occluded retrograde transvenous obliteration: usefulness of microcatheters. AJR Am J Roentgenol. 2003;181:725–727. doi: 10.2214/ajr.181.3.1810725. [DOI] [PubMed] [Google Scholar]
- 38.Menu Y, Gayet B, Nahum H. Bleeding duodenal varices: diagnosis and treatment by percutaneous portography and transcatheter embolization. Gastrointest Radiol. 1987;12:111–113. doi: 10.1007/BF01885117. [DOI] [PubMed] [Google Scholar]
- 39.Sato T, Yamazaki K, Toyota J, Karino Y, Ohmura T, Akaike J, Kuwata Y, Suga T. Efficacy of color Doppler ultrasonography for the diagnosis of duodenal varices successfully treated with percutaneous transhepatic obliteration. J Med Ultrasonics. 2007;34:59–63. doi: 10.1007/s10396-006-0129-4. [DOI] [PubMed] [Google Scholar]
- 40.Lim LG, Lee YM, Tan L, Chang S, Lim SG. Percutaneous paraumbilical embolization as an unconventional and successful treatment for bleeding jejunal varices. World J Gastroenterol. 2009;15:3823–3826. doi: 10.3748/wjg.15.3823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Yuki N, Kubo M, Noro Y, Kasahara A, Hayashi N, Fusamoto H, Ito T, Kamada T. Jejunal varices as a cause of massive gastrointestinal bleeding. Am J Gastroenterol. 1992;87:514–517. [PubMed] [Google Scholar]
- 42.Sakai M, Nakao A, Kaneko T, Takeda S, Inoue S, Yagi Y, Okochi O, Ota T, Ito S. Transhepatic portal venous angioplasty with stenting for bleeding jejunal varices. Hepatogastroenterology. 2005;52:749–752. [PubMed] [Google Scholar]
- 43.Sasamoto A, Kamiya J, Nimura Y, Nagino M. Successful embolization therapy for bleeding from jejunal varices after choledochojejunostomy: report of a case. Surg Today. 2010;40:788–791. doi: 10.1007/s00595-009-4129-z. [DOI] [PubMed] [Google Scholar]
- 44.Hiraoka K, Kondo S, Ambo Y, Hirano S, Omi M, Okushiba S, Katoh H. Portal venous dilatation and stenting for bleeding jejunal varices: report of two cases. Surg Today. 2001;31:1008–1011. doi: 10.1007/s005950170013. [DOI] [PubMed] [Google Scholar]
- 45.Ota S, Suzuki S, Mitsuoka H, Unno N, Inagawa S, Takehara Y, Sakaguchi T, Konno H, Nakamura S. Effect of a portal venous stent for gastrointestinal hemorrhage from jejunal varices caused by portal hypertension after pancreatoduodenectomy. J Hepatobiliary Pancreat Surg. 2005;12:88–92. doi: 10.1007/s00534-004-0941-4. [DOI] [PubMed] [Google Scholar]
- 46.Falchuk KR, Aiello MR, Trey C, Costello P. Recurrent gastrointestinal bleeding from ileal varices associated with intraabdominal adhesions: case report and review of the literature. Am J Gastroenterol. 1982;77:859–860. [PubMed] [Google Scholar]
- 47.Arst HF, Reynolds JD. Acute ileal variceal hemorrhage secondary to esophageal sclerotherapy. J Clin Gastroenterol. 1986;8:603–604. doi: 10.1097/00004836-198610000-00026. [DOI] [PubMed] [Google Scholar]
- 48.Højhus JH, Pedersen SA. Cirrhosis and bleeding ileal varices without previous intraabdominal surgery. A case report. Acta Chir Scand. 1986;152:479–480. [PubMed] [Google Scholar]
- 49.Lewis P, Warren BF, Bartolo DC. Massive gastrointestinal haemorrhage due to ileal varices. Br J Surg. 1990;77:1277–1278. doi: 10.1002/bjs.1800771126. [DOI] [PubMed] [Google Scholar]
- 50.Ohtani T, Kajiwara E, Suzuki N, Kawasaki A, Sadoshima S, Sakata H, Sasaguri Y, Onoyama K. Ileal varices associated with recurrent bleeding in a patient with liver cirrhosis. J Gastroenterol. 1999;34:264–268. doi: 10.1007/s005350050255. [DOI] [PubMed] [Google Scholar]
- 51.Kobayashi K, Yamaguchi J, Mizoe A, Isomoto I, Koshiishi T, Izawa K, Kanematsu T. Successful treatment of bleeding due to ileal varices in a patient with hepatocellular carcinoma. Eur J Gastroenterol Hepatol. 2001;13:63–66. doi: 10.1097/00042737-200101000-00012. [DOI] [PubMed] [Google Scholar]
- 52.Guth E, Katz MD, Hanks SE, Teitelbaum GP, Ralls P, Korula J. Recurrent bleeding from ileal varices treated by transjugular intrahepatic portosystemic shunt: value of Doppler ultrasonography in diagnosis and follow-up. J Ultrasound Med. 1996;15:67–69. [PubMed] [Google Scholar]
- 53.Varanasi RV, Fleisher AS, Darwin PE, King CE, Haluszka O. Colonoscopic sclerotherapy of ileal varices. Gastrointest Endosc. 2000;52:109–111. doi: 10.1067/mge.2000.106538. [DOI] [PubMed] [Google Scholar]
- 54.López-Benítez R, Seidensticker P, Richter GM, Stampfl U, Hallscheidt P. [Case report: massive lower intestinal bleeding from ileal varices: treatment with transjugular intrahepatic portosystemic shunt (TIPSS)] Radiologe. 2007;47:407–410. doi: 10.1007/s00117-005-1279-x. [DOI] [PubMed] [Google Scholar]
- 55.Cappell MS, Price JB. Characterization of the syndrome of small and large intestinal variceal bleeding. Dig Dis Sci. 1987;32:422–427. doi: 10.1007/BF01296297. [DOI] [PubMed] [Google Scholar]
- 56.Ueda J, Yoshida H, Mamada Y, Taniai N, Mizuguchi Y, Shimizu T, Matsumoto S, Kakinuma D, Ishikawa Y, Kanda T, et al. Successful emergency enterectomy for bleeding ileal varices in a patient with liver cirrhosis. J Nippon Med Sch. 2006;73:221–225. doi: 10.1272/jnms.73.221. [DOI] [PubMed] [Google Scholar]
- 57.Mashimo M, Hara J, Nitta A, Oohira M, Yamaguchi S, Yamada S, Tanaka H, Higuchi K, Arakawa T. [A case of ruptured ileal varices associated with alcoholic liver cirrhosis] Nihon Shokakibyo Gakkai Zasshi. 2007;104:561–567. [PubMed] [Google Scholar]
- 58.Haruta I, Isobe Y, Ueno E, Toda J, Mitsunaga A, Noguchi S, Kimura T, Shimizu K, Yamauchi K, Hayashi N. Balloon-occluded retrograde transvenous obliteration (BRTO), a promising nonsurgical therapy for ectopic varices: a case report of successful treatment of duodenal varices by BRTO. Am J Gastroenterol. 1996;91:2594–2597. [PubMed] [Google Scholar]
- 59.Sato T, Yamazaki K, Toyota J, Karino Y, Ohmura T, Akaike J. Ileal varices treated with balloon-occluded retrograde transvenous obliteration. Gastroenterol Res. 2009;2:122–5. doi: 10.4021/gr2009.04.1286. [DOI] [PMC free article] [PubMed] [Google Scholar]