

Abstract
Low-grade endometrial stromal sarcoma (ESS) is a kind of uterine malignancy. Total hysterectomy and bilateral salpingo-oophorectomy was the main treatment. We evaluate the feasibility of fertility-sparing management in five patients with low-grade ESS who desired for childbearing. The patients aged 28-36 years old presented with symptoms of menometrorrhagia or without symptom. Ultrasound examinations demonstrated leiomyomas (with the diameter of 3.5-6 cm respectively). All the patients received conservative surgeries of local resection of the mass with uterine reconstruction. Then the adjuvant endocrine therapy was given to them with megestrol acetate (160-320 mg/day) or triptorelin (3.75 mg/28 days) for 5-6 months. The follow-up lasted 21-55 months. All the patients survived. Three of them underwent an uncomplicated pregnancy, and received cesarean delivery of a liveborn neonate. One of them is alive without disease recurrence. The other one found disease recurred during the megestrol acetate treatment, and received hysterectomy. We consider that fertility-sparing treatment is suitable in selected in young low-grade ESS patients especially for those whose lesion was with a clear borderline. Adjuvant endocrine therapy is recommended for about 6 months after operation.
Keywords: Endometrial stromal sarcoma, fertility-conservative, endocrine therapy
Introduction
Uterine sarcomas are rare tumors, accounting for less than 3% of all female genital tract malignancies and 3% to 7% of malignant tumors of the uterine corpus [1]. According to an analysis of the Surveillance, Epidemiology, and End Results Program data, the annual incidence of ESS was only 0.19 in 100,000 [2].
Endometrial stromal sarcomas have been classified traditionally into low-grade and high-grade tumors, the latter currently defined as undifferentiated endometrial sarcoma. Low-grade ESS, typically composed of cells resembling endometrial stromal cells of the proliferative endometrium, are invasive cancers with a slow-growing plexiform vasculature, mild cytologic atypia, no cell necrosis, and usually no more than 10 mitotic figures per 10 high-power fields [3].
Because of the malignant nature of disease, the initial treatment of low-grade ESS includes surgery with total hysterectomy and bilateral salpingo-oophorectomy, and the adjuvant treatment often includes radiation therapy and endocrine therapy. Low-grade ESS shows a peak of incidence before menopause and has an indolent clinical behavior with 80% to 100% 5-year overall survival [4]. In Chinese patients, the mean age of low-grade ESS was 42.4 years old and 91.5% of them were premenopausal [5]. Unfortunately, some of patients were young and desired to child-bearing in the future. Fertility-sparing management of ESS has been demonstrated, while reports of pregnancy after such management is rare.
We tried to preserve the fertility in a series of five patients with low-grade ESS who desired for child-bearing in the future and succeeded in four patients.
Material and methods
Clinical data of five low-grade ESS patients who received fertility-sparing treatment in Peking Union Medical College Hospital from Mar. 2010 to Jan. 2014 were collected. All patients gave written informed consent to participate in the study.
Results
Case 1
A 36-year-old woman (gravida 0, para 0) underwent laparoscopic myomectomy because of a leiomyoma was found by B ultrasound in the left anterior wall of the uterine body with the diameter of 4.5 cm. A clear borderline lesion was found during the operation. The postoperative patho-histological analysis showed low grade ESS. Then megestrol acetate 320 mg/day was given to her for five months. She remained disease free for 20 months. She succeeded in conceive afterwards and C-section was given to her at 39 weeks’ gestation. She delivered a male neonate weighted 3500 g. She remained disease free for 3 months postpartum.
Case 2
A 28-year-old woman (gravida 0, para 0) complaining of 2 year of abnormal vaginal bleeding was admitted to hospital. B ultrasound examination demonstrated a leiomyoma in the anterior wall of the uterine body with the diameter of 6 cm. Laparoscopic myomectomy was given to her. The final postoperative pathohistologic analysis misdiagnosed as endometrial stromal nodule. Another lesion was found in the uterus after 15 months about 5.2 cm with the presentation of menorrhagia. Abdominal myomectomy was performed. A clear borderline lesion was found in the anterior wall of uterus. The postoperative pathohistologic analysis showed low grade ESS. Then megestrol acetate 160 mg/day was given to her for six months. Three months after the end of the treatment, she found pregnancy. She underwent an uncomplicated pregnancy, and received cesarean delivery of a liveborn female neonate (weigh 3400 g) at 38 weeks of gestation. A leiomyoma about 4cm was found by ultrasound at 21 months postpartum.
Case 3
A 37-year-old woman (gravida 0, para 0) received treatment because of primary infertility. During the process of in vitro fertilization and embryo transfer (IVF-ET), a leiomyoma of 4.0×3.5 cm was found after ovulation. She received laparoscopic myomectomy and found a leiomyoma in anterior wall of the uterus with a clear borderline. The postoperative pathohistologic analysis showed low grade ESS (Figure 1), Estrogen receptor (ER (80%++)), Progesterone receptor (PR (90%+++)). Then megestrol acetate 160-320 mg/day was given to her for six months. She received frozen embryo transfer three months after the treatment. She succeeded in conceive and C-section was given to her at 41 weeks’ gestation because of failed labor induction and a healthy female neonate (weighed 3160 g) was delivered. She was five months postpartum and remained disease free.
Figure 1.
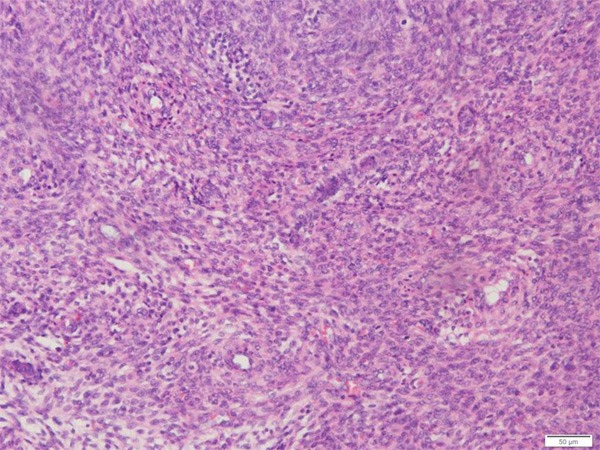
Pathologic diagnosis of endometrial stromal sarcoma of case 3. This is a pathology image from the excised tumor specimen of case 3 demonstrating endometrial stromal sarcoma.
Case 4
A 32-year-old woman (gravida 0, para 0) underwent laparoscopic myomectomy because of a leiomyoma was found by B ultrasound at the right corner of the uterus with the diameter of 5cm. A clear borderline lesion was found during the operation. The tumor was crisp and yellowish. The postoperative pathohistologic analysis showed low grade ESS mixed with Leiomyoma; IHC showed ER (+++), PR (+++). Then triptorelin 3.75 mg was given to her every four weeks for five months. She remained disease free for 39 months.
Case 5
A 29-year-old woman (gravida 1, para 0) complained of dysmenorrhea for 3 years was diagnosed as adenomyoma. The lesion about 6 cm was on the posterior wall of the uterus with unclear borderline. Triptorelin 3.75 mg was given to her for 3 months then she received laparoscopic surgery. The lesion was excised. The postoperative pathohistologic analysis showed low grade ESS; Immunohistochemistry showed ER (±), PR (+). Megestrol acetate 320 mg/day was given to her for 3 months. B ultrasound found a heterogeneous echo lesion on the posterior wall about 3.2×2.7 cm. Another laparoscopic was given to her and the lesion was excised again. The postoperative pathohistologic analysis showed low-grade ESS infiltrated in smooth muscle tissue (Figure 2). Megestrol acetate 320 mg/day was given to her for another 2 months. B ultrasound found another heterogeneous echo lesion on the left anterior wall about 2.5×1.7 cm, the borderline was unclear. Hysterectomy was given to her. The pathohistologic analysis showed low grade ESS infiltrated in uterine wall, especially the anterior wall (Figure 3). Then megestrol acetate 320 mg/day was given to her for 6 months. She remained disease free for 10 months.
Figure 2.
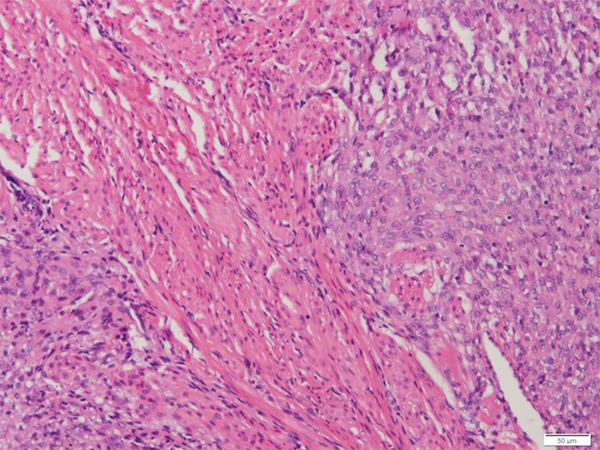
Pathologic diagnosis of endometrial stromal sarcoma of case 5. This is a pathology image from the excised tumor specimen of case 5 demonstrating endometrial stromal sarcoma and the tumor cells infiltrated in smooth muscle tissue.
Figure 3.
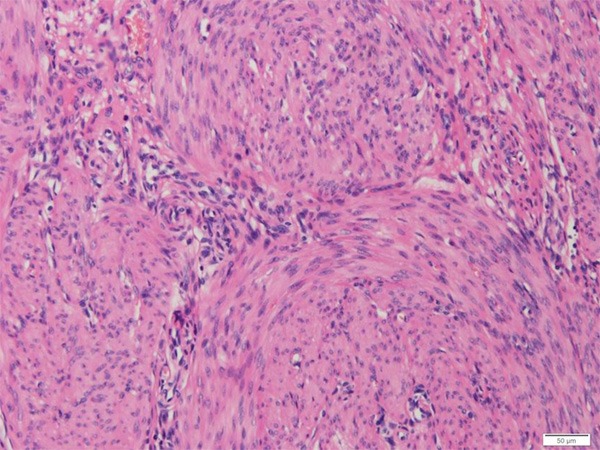
Hysterectomy specimen of case 5. This is a pathology image from the hysterectomy specimen of case 5 demonstrating low grade ESS infiltrated in uterine wall.
Discussion
Recent studies have demonstrated that low-grade ESS and high-grade ESS, which now defined as UES, are separate entities [6]. Low-grade endometrial stromal sarcoma is a hormone-sensitive low-grade malignancy that generally follows an indolent course with a tendency for late recurrence, while high-grade endometrial stromal sarcoma is characterized by an aggressive clinical course. The main treatment for low-grade ESS includes total hysterectomy and bilateral salpingo-oophorectomy. For the young patients who desire child-bearing in the future, is it possible to preserve their fertility?
Few reports have been published about the low-grade ESS patients treated with fertility-preserving procedures and revealed completely different outcomes. Koskas M et al [7] reported a 34-year-old woman treated conservatively for low grade ESS who conceived rapidly after hysteroscopic resection of the tumor but had severe peritoneal recurrence in the postpartum period. Delaney AA et al [8] reported a 16-year-old nulligravid adolescent girl underwent local resection of the low-grade ESS mass with uterine reconstruction. The patient was given high-dose daily megestrol acetate therapy and remained disease-free for 8 years before achieving pregnancy spontaneously and remained disease free postpartum. Yan et al [9] reported a high-grade ESS patient who treated with local wide resection of the lesion and uterine reconstruction followed with adjuvant chemotherapy. She conceived spontaneously and underwent an uncomplicated pregnancy. Cesarean delivery was given to her at 39 weeks of gestation. It seemed that local resection of low-grade endometrial stromal sarcoma is a safe procedure. Because most of the cases of low grade ESS were misdiagnosed as leiomyoma, the patients would be given the surgery as myomectomy. In our opinion, if the borderline of the tumor is clear, removal of the tumor like myomectomy is enough, just like cases 1-4 in our series. It seemed that it is no need to perform local wide resection. Blurred borderline tumor is a high risk factor for disease recurrence, just like case 5. The follow-up of such patients should include regular intensive surveillance, perhaps with hysterectomy and bilateral oophorectomy after the delivery.
Low-grade ESS is a kind of steroid receptor positive tumor, it is reasonable to give the patients, who received fertility-sparing surgery, hormonal therapy to prevent the disease recurrence. Most of the tumors are positive for ERα and PR, but lack of ERβ expression [10]. Progestin therapy should be routinely considered for adjuvant therapy. The treatment period is not determined. Mizuno et al [11] reported long time (median 64 months) treatment of medroxyprogesterone acetate (MPA) was better to eliminate the residual or recurrent disease. Because of the side effect, we consider that short time of progestin treatment is better for the patients without residual disease. We think the treatment period around six months is reasonable. Since progestins are poorly tolerated due to side effects, other available hormonal therapies including aromatase inhibitors and gonadotropin-releasing hormone analogues have become effective treatment alternative.
In the conclusion, low grade ESS is a kind of malignancy with good prognosis. Fertility-sparing treatment is suitable in selected in young ESS patients especially for those whose lesion was with a clear borderline. Adjuvant endocrine therapy is recommended.
Disclosure of conflict of interest
None.
References
- 1.Oláh KS, Gee H, Blunt S, Dunn JA, Kelly K, Chan KK. Retrospective analysis of 318 cases of uterine sarcomas. Eur J Cancer. 1991;27:1095–1099. doi: 10.1016/0277-5379(91)90300-3. [DOI] [PubMed] [Google Scholar]
- 2.Harlow BL, Weiss NS, Lofton S. The epidemiology of sarcomas of the uterus. J Natl Cancer Inst. 1986;76:399–402. [PubMed] [Google Scholar]
- 3.Norris HJ, Taylor HB. Mesenchymal tumors of the uterus. A clinical and pathological study of 53 endometrial stromaltumors. Cancer. 1966;19:755–766. doi: 10.1002/1097-0142(196606)19:6<755::aid-cncr2820190604>3.0.co;2-u. [DOI] [PubMed] [Google Scholar]
- 4.Gadducci A, Sartori E, Landoni F, Zola P, Maggino T, Urgesi A, Lissoni A, Losa G, Fanucchi A. Endometrial stromal sarcoma: analysis of treatment failures and survival. Gynecol Oncol. 1996;63:247–253. doi: 10.1006/gyno.1996.0314. [DOI] [PubMed] [Google Scholar]
- 5.Jin Y, Pan LY, Wang XQ, Dai Z, Huang H, Guo L, Shen K, Lian L. Clinical Characteristics of Endometrial Stromal Sarcoma From an Academic Medical Hospital in China. Int J Gynecol Cancer. 2010;20:1535–1539. [PubMed] [Google Scholar]
- 6.Nam JH, Park JY. Update on treatment of uterine sarcoma. Curr Opin Obstet Gynecol. 2010;22:36–42. doi: 10.1097/GCO.0b013e328334d90f. [DOI] [PubMed] [Google Scholar]
- 7.Koskas M, Morice P, Yazbeck C, Duvillard P, Walker F, Madelenat P. Conservative management of low-grade endometrial stromal sarcoma followed by pregnancy and severe recurrence. Anticancer Res. 2009;29:4147–4150. [PubMed] [Google Scholar]
- 8.Delaney AA, Gubbels AL, Remmenga S, Tomich P, Molpus K. Successful pregnancy after fertility-sparing local resection and uterinereconstruction for low-grade endometrial stromal sarcoma. Obstet Gynecol. 2012;20:486–489. doi: 10.1097/AOG.0b013e31825a7397. [DOI] [PubMed] [Google Scholar]
- 9.Yan L, Tian Y, Fu Y, Zhao X. Successful pregnancy after fertility-preserving surgery for endometrial stromal sarcoma. Fertil Steril. 2010;93:269, e1–3. doi: 10.1016/j.fertnstert.2009.09.024. [DOI] [PubMed] [Google Scholar]
- 10.Chu MC, Mor G, Lim C, Zheng W, Parkash V, Schwartz PE. Low-grade endometrial stromal sarcoma: hormonal aspects. Gynecol Oncol. 2003;90:170–176. doi: 10.1016/s0090-8258(03)00258-0. [DOI] [PubMed] [Google Scholar]
- 11.Mizuno M, Yatabe Y, Nawa A, Nakanishi T. Long-term medroxyprogesterone acetate therapy for low-grade endometrial stromal sarcoma. Int J Clin Oncol. 2012;17:348–354. doi: 10.1007/s10147-011-0299-y. [DOI] [PubMed] [Google Scholar]