

Abstract
Chronic renal insufficiency and osteoporosis have become very common among old people in China. Hyperparathyroidism caused by renal insufficiency would result in turbulence of bone metabolism and unbalance between serum calcium and phosphorus. The aim of this study is to investigate the BMD, PTH, CT and 25(OH)-Vit’s significance for screening and diagnosing chronic renal insufficiency. In this study, seventy cases with chronic renal insufficiency from Jun. 2010 to Oct. 2013 were selected as the observation group. Meanwhile, another 70 volunteers with normal renal functions were set as the control group. The level of BMD, PTH, CT and 25(OH)-Vit were detected by using ELISA assay. DPX bone density meters (UNIGAMMA X-RAY PLUS) were used for the detection of BMD. The results indicated that BMD levels of the proximal femur (include Troch, Shaft, Total, Neck, Ward) and lumbar vertebra in the observation group were significantly lower while the PTH and CT were significantly higher compared with the control group (P<0.05). A positive correlation was identified between the serum creatinine (Scr) concentrations and CT, PTH, while the correlation with 25(OH)-Vit was considered to be negative. In conclusion, the BMD, PTH, CT, and 25 (OH)-Vit would provide reference in diagnosing and treatment for chronic renal insufficiency. These indexes would be important clinical significance for screening and early diagnose of osteoporosis in these patients.
Keywords: Chronic renal insufficiency, correlation, progress, bone mineral density, influence factors
Introduction
The morbidities of both osteoporosis and chronic renal insufficiency are increasing yearly, especially in the elderly population. By now the two diseases have become very common among old people in China, which greatly affect the quality of living and life [1]. It has been widely accepted that bone density would decreased when human grow old. Particularly, hyperparathyroidism caused by renal insufficiency would result in turbulence of bone metabolism and the unbalance between serum calcium and phosphorus. All these finally lead to a worse situation of bone loss and lower bone mineral density. In order to study the regulation of bone mineral density (BMD), parathyroid hormone (PTH), calcitonin (CT), 25-hydroxyvitamin D (25(OH)-Vit) in patients suffering chronic renal insufficiency, this study was designed. 70 patients with chronic renal insufficiency from Jun. 2010 to Oct. 2013 in our hospital were selected as the observation group. In the meanwhile 70 volunteers with normal renal function were also studied as the control group. The levels of BMD, PTH, CT and 25(OH)-Vit were detected and analyzed in the two groups. The whole study progress was reported as follows.
Materials and methods
Patient ascertainment
Seventy patients with chronic renal insufficiency from Jun. 2010 to Oct. 2013 in our hospital were selected as the observation group. This group included 48 males and 22 females patients, the age ranges of the patients are from 72-89, the average age is 82.88±6.2. At the same time period, 70 volunteers were chosen as the control group, including 39 males and 31 females with the age range 74-88. The average age of the control group is 83.81±4.9. During the whole study, any patients who had taken heparin or glucocorticoid were excluded. Also before the study, patients with prostate cancer, hyperthyroidism, hypothyroidism, liver cirrhosis, tumor metastasis or paralysis would not be accepted into this clinical study.
Measurement for BMD
DPX bone density meters (UNIGAMMA X-RAY PLUS) were used for the detection of BMD. The sections for detection included left collum femoris, greater trochanter, Ward triangle, femoral trochanteric and the whole thigh bone. All data collected were shown with the form of bone mineral density [2]. The accuracy of this equipment could reach 1%. The errors of the detection results between the repeated measurements were controlled to be less than 1%. All operation processes were performed by experienced specialists blinded to this study [3].
Measurement for the biochemical indexes of the patients and volunteers
Blood samples were collected by venous sampling. The levels of serum creatinine were tested by automatic biochemical analyzer. Enzyme-linked immuno sorbent assay (ELISA) was used to detect the serum 25(OH)-Vit, which could reflect the level of Vit D inside the body. CT and PTH were analyzed by Chemiluminescence [4-7].
Statistical analysis
SPSS 10.0 was used for the statistical analysis. All data were reported as means ± SEM. Comparisons of the data between the two groups were performed with Student’s t test. The correlation analysis was performed by using the pearson correlation analysis in this study.
Results
BMD level decreases in chronic renal insufficiency patients
In our study, it was observed that BMD levels in all parts of proximal femur (including proximal femur) and lumbar vertebra were significantly lower in the observation group compared with the control group. The differences were statistically significant (Figure 1, P<0.05). Details were shown in Table 1.
Figure 1.
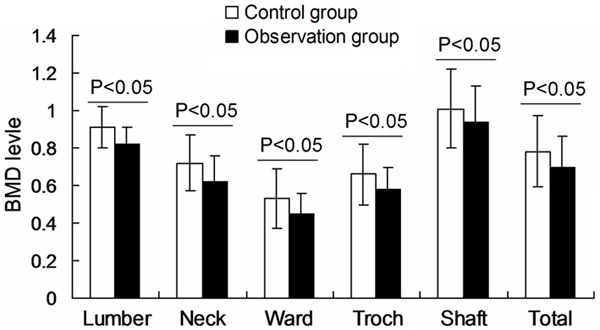
BMD levels in all parts of proximal femur and lumbar vertebra. The different values of observation group compared with the control group were illustrated in figure.
Table 1.
Comparison of the BMD in observation and control group (mean ± SEM)
| Groups | No. s | lumbar | Neck | Ward | Troch | Shaft | Total |
|---|---|---|---|---|---|---|---|
| Control group | 70 | 0.91±0.11 | 0.72±0.15 | 0.53±0.16 | 0.66±0.16 | 1.01±0.21 | 0.78±0.19 |
| Observation group | 70 | 0.82±0.09 | 0.62±0.14 | 0.45±0.11 | 0.58±0.12 | 0.94±0.19 | 0.70±0.16 |
Biochemical indexes increases significantly in chronic renal insufficiency patients
In our study, Cr, PTH and CT in observation group were higher compared to the control group. And the differences were statistically significant (Figure 2; Table 2, P<0.05). However, no significant differences were found in the level of 25(OH)-Vit between the two groups (Table 2, P>0.05).
Figure 2.
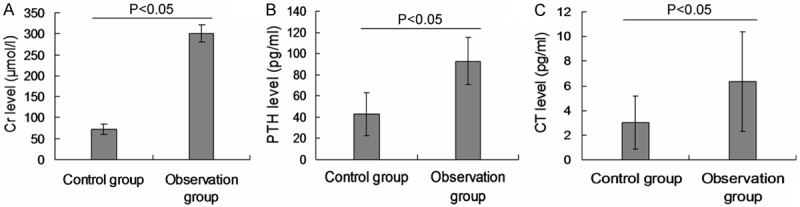
The Cr level, PTH level and CT level in control and observation group. A. The Cr level; B. The PTH level; C. The Ct level. The different values of observation group compared with the control group were illustrated in figure.
Table 2.
Comparison of the biochemical indexes and renal function (mean ± SEM)
| Groups | No. s | Cr (μmol/l) | PTH (pg/ml) | CT (pg/ml) | 25(OH)-Vit (nmol/L) |
|---|---|---|---|---|---|
| Control group | 70 | 72.51±12.11 | 42.72±20.35 | 3.03±2.16 | 56.76±18.16 |
| Observation group | 70 | 300.82±121.19 | 92.92±72.41 | 6.35±4.01 | 54.89±19.27 |
Scr correlates with CT and PTH positively, and with 25(OH)-Vit negatively
In order to investigate the correlation between Scr and the CT, PTH, 25(OH)-Vit, the pearson correlation analysis was used in this study. The present study showed that in all 140 people (all are elder people) of this research, the levels of Scr were positively correlated with CT and PTH, while negatively correlated with 25(OH)-Vit (Table 3).
Table 3.
Correlation between the serum creatinine and other indexes
| Index | PTH (pg/ml) | CT (pg/ml) | 25(OH)-Vit (nmol/l) | |||
|---|---|---|---|---|---|---|
|
| ||||||
| r | P | r | P | r | P | |
| Cr | 0.50 | <0.01 | 0.48 | <0.01 | 0.17 | >0.05 |
Discussion
In the elder population, renal insufficiency is a common phenomenon. Clinical symptoms related to the osseous tissue would appear in more than half of the elderly when the glomerular filtration rate decreases to half of the normal level [8-10]. Age related bone loss could cause a higher morbidity of osteoporosis when accompanied with renal insufficiency. The nephrons of patients with renal insufficiency are usually damaged and thus decrease the activity of hydroxylase, which is secreted by the nephrons [11]. This physiological change in turn restrict the biosynthesis of 25(OH)-Vit inside the kidney, resulting in a worse intestinal absorption for calcium. Meanwhile, blood calcium could gradually decline in some patients because of the loss of calcium in urine. Finally, the significant reduction in blood calcium would stimulate parathyroid glands to secret more PTH, a hormone with the function of promoting calcium from bone to blood. All these pathophysiology changes would take the body into a situation of secondary hyperparathyroidism. More cytokines could be released when renal function declines. These inflammation cytokines could gathered in the compact bone substance, promoting bone resorption Meanwhile the function and proliferative activity of osteoblast were inhibited because of the existence of these cytokines, which in turn aggravate the tendency of bone resorption. Thus, all the factors including the 25(OH)-Vit metabolism, excretion of phosphate, disorder of the acid-base balance, increase of PTH and decrease of serum calcium together cause the osteodystrophy in patients with renal insufficiency. The growth and differentiation of chondrocytes were affected, resulting in the decrease of bone stiffness and abnormal change in the shape of the cartilage tissue. Besides, it was reported that the expression of proteins and mRNA of the PTH related receptors, bioactive factors in cartilage tissue formation and vascular endothelial growth factors (VEGFs) were reduced in these patients. Since all these factors contribute to the growth of bone, their decrease would reduce osteogenesis in the body [12]. Other biological signal proteins such as insulin like growth factor (IGF), growth hormone receptor (GFR) et al, which help regulating the growth and metabolism of bone, were also reported to show a tendency of decline, leading to a higher probability of bone fracture in these patients. Otherwise, since sex hormones such as estrogen in male and estrogen in female also began to decrease in elder population, these aged patients also face such problems and thus could not get help from these sex hormones which could help restrain bone loss.
Our present research showed that PTH level in the renal insufficiency patients were more than double the level in normal volunteers. The results revealed the existence of Parathyroid hormone hyper function in this group [13]. Under such environments, the blood calcium is lower while serum phosphorus higher in these patients. Besides, 25(OH)-Vit is composed in the mitochondria inside hepatocytes with the absorbed Vitamin D as the material. The composed 25(OH)-Vit is further transformed to 1,25-(OH)2D3. Thus the level of 25(OH)-Vit is relevant to the liver function. In our study, patients in the observation group showed a normal level of 25(OH)-Vit during initial period when their renal insufficiency were still not that bad [14,15]. However, our study revealed that the level of serum creatinine was positive correlated to CT while negative to 25(OH)-Vit, this finding is in accordance with the fact that 25(OH)-Vit slowly decreased along with the increase of serum creatinine. In our study, we noticed that serum CT in patients with renal insufficiency was significantly higher than normal people. This peptide is secreted by C cells in parathyroid glands. The function of CT is the regulation of calcium and phosphorous homeostasis. When renal function is damaged, serum phosphorous would increase, and thus C cells in parathyroid glands are activated, secreting more CT to cause an increase in the level of serum CT. Except previous results, our findings also identified that BMD in femur and lumbar vertebra are significantly lower in the observation group. Taking the previous analysis into consideration, this is the result of bone loss caused by renal sufficiency.
In conclusion, BMD in all parts of proximal femur (Troch, Shaft, Total, Neck, Ward) and lumbar vertebra significantly declined while PTH and CT significantly increased in renal insufficiency patients. Besides 25(OH)-Vit did not seem to affect the renal function. We also found that the level of CT in all groups positively correlated to PTH while negative correlated to 25(OH)-Vit. These four indexes provide some clinical references for the diagnosing and treatment for chronic renal insufficiency. The analysis of these indexes is also of important clinical significance in helping physicians during the early diagnosis and screening of osteoporosis.
Disclosure of conflict of interest
None.
References
- 1.Al-Daghri NM, Yakout S, Al-Shehri E, Al-Fawaz HA, Aljohani N, Al-Saleh Y. Inflammatory and bone turnover markers in relation to PTH and vitamin D, status among Saudi postmenopausal women with and without osteoporosis. Int J Clin Exp Med. 2014;7:3528–3535. [PMC free article] [PubMed] [Google Scholar]
- 2.Hussien YM, Shehata A, Karam RA, Alzahrani SS, Magdy H, EI-Shafey AM. Polymorphism in Vitamin D receptor and osteoprotegerin genes in Egyptian rheumatoid arthritis patients with and without osteoporosis. Mol Biol Rep. 2013;40:3675–3680. doi: 10.1007/s11033-012-2443-9. [DOI] [PubMed] [Google Scholar]
- 3.Arteh J, Narra S, Nair S. Prevalence of vitamin D deficiency in chronic liver disease. Dig Dis Sci. 2010;55:2624–2628. doi: 10.1007/s10620-009-1069-9. [DOI] [PubMed] [Google Scholar]
- 4.Gedikli O, Kiris A, Karahan C. Circulating levels of erythropoietin and its relation to arterial stiffness in patients with hypertension. Int J Clin Exp Med. 2013;6:706–711. [PMC free article] [PubMed] [Google Scholar]
- 5.Polak-Jonkisz D, Zwolińska D, Bednorz R, Owczarek H, Nahaczewska W. Usefulness of osteocalcin and CrossLaps as markers of bone turnover in children with chronic renal failure. Pol Merkur Lekarski. 2002;12:257–260. [PubMed] [Google Scholar]
- 6.Takagaki K, Takashima T, Onoda N, Tezuka K, Noda E, Kawajiri H, Ishikawa T, Hirakawa K. Parathyroid hormone-related protein expression, in combination with nodal status, predicts bone metastasis and prognosis of breast cancer patients. Exp Ther Med. 2012;3:963–968. doi: 10.3892/etm.2012.521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kotzmann H, Riedl M, Pietschmann P, Schmidt A, Schuster E, Kreuzer S, Kainberger F, Frisch H, Geyer G, Horl WH, Mayer G, Luger A. Effects of 12 months of recombinant growth hormone therapy on parameters of bone metabolism and bone mineral density in patients on chronic hemodialysis. J Nephrol. 2004;17:87–94. [PubMed] [Google Scholar]
- 8.Doumouchtsis KK, Kostakis AI, Doumouchtsis SK, Grapsa EI, Passalidou IA, Tzjamalis MP, Poulakou MV, Vlachos IS, Perrea DN. The effect of sexual hormone abnormalities on proximal femur bone mineral density in hemodialysis patients and the possible role of RANKL. Hemodial Int. 2008;12:100–107. doi: 10.1111/j.1542-4758.2008.00249.x. [DOI] [PubMed] [Google Scholar]
- 9.Messa P, Mioni G, Turrin D, Guerra UP. The calcitonin-calcium relation curve and calcitonin secretory parameters in renal patients with variable degrees of renalfunction. Nephrol Dial Transplant. 1995;10:2259–2265. doi: 10.1093/ndt/10.12.2259. [DOI] [PubMed] [Google Scholar]
- 10.Boonen S, Mohan S, Dequeker J. Down regulation of the serum stimulatorycomponents of theinsulin-like growth factor (IGF) system (IGF-, IGF-, IGFBp-3 and IGFBp-5) in agerelated (type II) femoral neck osteoporosis. J Bone Miner Res. 1999;14:2150–2158. doi: 10.1359/jbmr.1999.14.12.2150. [DOI] [PubMed] [Google Scholar]
- 11.Adams JS, Hewison M. Update in vitamin D. J Clin Endocrinol Metab. 2010;95:471–478. doi: 10.1210/jc.2009-1773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Santos F, Carbajo-Pérez E, Rodríguez J, Fernandez-Fuente M, Molinos I, Amil B, Garcia E. Alterations of the growth plate in chronic renal failure. Pediatr Nephrol. 2005;20:330–334. doi: 10.1007/s00467-004-1652-4. [DOI] [PubMed] [Google Scholar]
- 13.Tzanno MC, Futata E, Jorgetti V, Duarte A. Immuneresponse in hemodialysis patients: is there any difference when low and high iPTH levels are compared? Clin Nephrol. 2000;54:22. [PubMed] [Google Scholar]
- 14.Kogawa M, Findlay DM, Anderson PH, Ormsby R, Vincent C, Morris HA, Atkins GJ. Osteoclastic metabolism of 25(OH)-vitamin D3: a potential mechanism for optimization of bone resorption. Endocrinology. 2010;151:4613–4625. doi: 10.1210/en.2010-0334. [DOI] [PubMed] [Google Scholar]
- 15.Refaat B, Ashour TH, El-Shemi AG. Ribavirin induced anaemia: the effect of vitamin D supplementation on erythropoietin and erythrocyte indices in normal Wistar rat. Int J Clin Exp Med. 2014;7:2667–2676. [PMC free article] [PubMed] [Google Scholar]