

Abstract
Angina pectoris is a common symptom imperiling patients’ life quality. The aim of this study is to evaluate the efficacy and safety of acupuncture for stable angina pectoris. Clinical randomized-controlled trials (RCTs) comparing the efficacy of acupuncture to conventional drugs in patients with stable angina pectoris were searched using the following database of PubMed, Medline, Wanfang and CNKI. Overall odds ratio (ORs) and weighted mean difference (MD) with their 95% confidence intervals (CI) were calculated by using fixed- or random-effect models depending on the heterogeneity of the included trials. Total 8 RCTs, including 640 angina pectoris cases with 372 patients received acupuncture therapy and 268 patients received conventional drugs, were included. Overall, our result showed that acupuncture significantly increased the clinical curative effects in the relief of angina symptoms (OR=2.89, 95% CI=1.87-4.47, P<0.00001) and improved the electrocardiography (OR=1.83, 95% CI=1.23-2.71, P=0.003), indicating that acupuncture therapy was superior to conventional drugs. Although there was no significant difference in overall effective rate relating reduction of nitroglycerin between two groups (OR=2.13, 95% CI=0.90-5.07, P=0.09), a significant reduction on nitroglycerin consumption in acupuncture group was found (MD=-0.44, 95% CI=-0.64, -0.24, P<0.0001). Furthermore, the time to onset of angina relief was longer for acupuncture therapy than for traditional medicines (MD=2.44, 95% CI=1.64-3.24, P<0.00001, min). No adverse effects associated with acupuncture therapy were found. Acupuncture may be an effective therapy for stable angina pectoris. More clinical trials are needed to systematically assess the role of acupuncture in angina pectoris.
Keywords: Stable angina pectoris, acupuncture, meta-analysis
Introduction
Angina pectoris, induced by rapid, transient myocardial ischemia and hypoxi, is a common symptom in the chest [1]. It is characterised by short-lasting squeezing pain and substernal pain that radiates to the neck, jaw, shoulder, back, arm and epigastric region [2]. Coronary artery disease is the most common risk factor of angina pectoris [3]. Patients with angina pectoris have the risk of acute myocardial infarction and sudden death, and the prognosis considerably depends on the extent of coronary artery disease and the severity of heart function. The incidence of angina pectoris varies between countries. It has been estimated that 49 to 125 and 50 to 92 per 1000 man and woman will occur angina pectoris every year, respectively [4]. The occurrence rate of angina in China has increased yearly, and the onset age has become much younger. According to a survey of a community in Beijing, the incidence of angina pectoris and myocardial infarction is 30.7% (male 26.2%, female 33.7%) and 2.9% (male 4.8%, female 1.7% ), respectively [5].
Nitrates, beta blockers, calcium antagonists, aspirin and ACE inhibitors, holding that angina pectoris is the clinical syndrome caused by paroxysmal coronary artery blood supply insufficiency, acute myocardial ischemia and oxygen deficiency, are the current modern treatments to improve prognosis of angina pectoris and reduce ischemic symptoms. However, these drugs can have undesirable effects. For example, nitrate treatment carries the risks of tolerance and rebound, and can cause headaches, flushed cheeks and other adverse reactions [6]. Thus, there is an urgent need to explore novel therapy.
Acupuncture, well known as an oriental healing technique, is one aspect of the Chinese medical sub-discipline “acupuncture and moxibustion” (zhenjiu) and is a traditional medicine that’s been practiced in China and other Asian countries for over 2,000 years [7]. Acupuncture is the stimulation of specific points on the body [8], and its classic form consists of inserting needles into acupuncture points [9]. The category of acupuncture therapy is classical manual acupuncture, electroacupuncture, ear-acupuncture, scalp-acupuncture and moxibustion [10]. The National Institutes of Health (NIH) Consensus has recommended acupuncture as an alternative and complementary treatment for many health conditions [11]. Previous meta-analysis have shown that acupuncture is an effective therapy in numerous diseases, such as acute hypertensive intracerebral hemorrhage [12], acute ischemic stroke [13], and chronic pain [14]. Acupuncture is often promoted for treating cardiovascular diseases as well including heart failure [15] and angina pectoris [16,17]. Therefore, we conducted this meta-analysis to determine systematically whether acupuncture is a safe and effective method in patients with stable angina pectoris.
Materials and methods
Literature search
We performed a medical literature retrieval in the following electronic database: PubMed, Medline, Wanfang and CNKI (China National Knowledge Infrastructure) published between January 2000 and July 2014. The key words used for the search were: “acupuncture or electroacupuncture or acupressure or moxibustion or cupping”, “angina pectoris or angina”, and “coronary heart disease” as well as their combinations. The corresponding Chinese terms were used in the Chinese library. The reference lists of all relevant articles were searched for further studies.
Inclusion criteria
The inclusion criteria were as follows: 1) the paper should be randomized-controlled trials (RCT); 2) all the patients met angina pectoris’s diagnostic criteria formulated by WHO; 3) patient diagnosed with stable angina pectoris since at least three months, acupuncture treatment at least one week and observational period at least 10 days; 4) patients in experiment group should be treated with acupuncture (stimulating acupuncture points with needling such as acupuncture and electroacupuncture; non-penetrating acupuncture point stimulation such as cupping, acupressure and moxibustion); acupuncture therapy point are PC 6 (Neiguan), BL 17 (Geshu point), CV 17 (Danzhong point), PC 4 (Ximen), BL 15 (Xinshu point), PC 7 (Daling point), PC 5 (Jianshi point), HT 7 (Shenmen point), PC 3 (Quze point), BL 18 (Ganshu point), L 20 (Pishu point), BL 23 (Shenshu point), HT 5 (Tongli point), CV 6 (Qihai point), and ST36 (Zusanli point); 5) patients in control group treated with conventional drugs such as compound Tanshen tablets, Shanhai Dan capsule, isosorbide dinitrate or metoprolol; 6) the primary outcomes were the clinical curative effects of angina relief and improvement of electrocardiography, the secondary outcomes were the time to onset of angina relief, consumption of existing anti-anginal medications and adverse effect; 7) data including therapeutic effects and adverse events were available to extract.
Data collection
Two investigators independently screened the searched studies and assessed the quality of the included trials according to the titles and abstracts provided by the authors. Any disagreement was subsequently resolved by discussion with a third expert to reach a consensus. The following information was extracted from each article: first author, publication year, mean age, total numbers, observational course, types of interventions in experiment group and control group.
Statistical analysis
Statistical analyses were conducted in Review Manager (RevMan version 5.2, the Cochrane Collaboration, Oxford, England). For dichotomous data, odds ratios (ORs), risk ratios (RRs) with their 95% confidence intervals were calculated; for continuous data, mean difference (MD) was calculated. A P-value less than 0.05 was considered statistically significant. Heterogeneity between trials was tested using the Q-statistic test and a standard I2 test. A P-value less than 0.10 for the Q-test and I2 more than 50% was considered significant among the studies. Funnel plots was employed to detect the publication biases and small-study effects.
Results
Study selection and characteristics
The electronic database search identified 216 references. After applying the inclusion criteria, 8 articles were ultimately included in the systematic review and meta-analysis. The study selection process was shown in Figure 1. All the 8 trials were conducted in China [18], including 640 angina pectoris cases with 372 patients received acupuncture therapy (experimental group) and 268 patients received conventional drugs (control group). The number of participants varied from 62 to 128 and the duration of treatment course was between 10 days and 6 weeks. The mean age was more than 45 years old. One study contained two comparable groups [19]. The detailed characteristics of the studies included were shown in Table 1.
Figure 1.
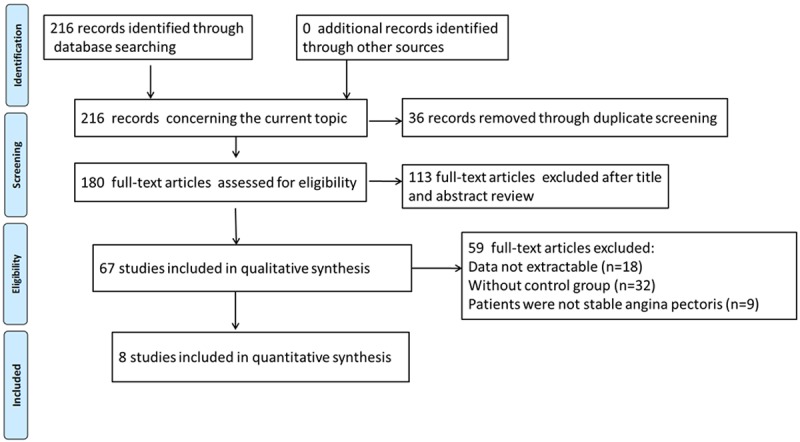
Flow chart of the search process.
Table 1.
Main characteristic of included trials
| First author | Year | Mean age | Total number | Types of interventions | Course | ||
|---|---|---|---|---|---|---|---|
|
|
|
||||||
| T | C | T | C | ||||
| Diao LH | 2003 | 56.46±5.32 | 57.32±5.25 | 40 | 30 | T: Acupuncture + moxibustion | 4 weeks |
| C: Shanhai Dan capsule | |||||||
| Huang J | 2004 | 56±15 | 57±14 | 40 | 40 | T: Electroacupuncture | 4 weeks |
| C: Compound Tanshen tablets | |||||||
| Chang PF | 2005 | 59.5±10.2 | 61.1±9.9 | 30 | 22 | T: Acupuncture | 2 weeks |
| C: Isosorbide dinitrate or metoprolol | |||||||
| Chen L | 2005 | 66.4 | 64.2 | 30 | 22 | T: Acupuncture + ear pressure | 10 days |
| C: Compound Tanshen tablets | |||||||
| Zhou W | 2007 | 68.70 | 65.20 | 72 | 56 | T: Acupuncture | 6 weeks |
| C:Isosorbide dinitrate + metoprolol + aspirin | |||||||
| Chen JW | 2008 | 45-65 | 45-65 | 30 | 29 | T: Acupuncture + cupping | 20 days |
| C: Isosorbide | |||||||
| Yin LH | 2009 | 52.6±4.8 | 52.2±5.0 | 42 | 38 | T: Acupuncture + cupping | 30 days |
| C: Isosorbide | |||||||
| Liu JR-a | 2010 | 50.4±8.5 | 49.2±7.3 | 58 | 32 | T: Acupuncture + moxibustion | 4 weeks |
| C: Compound Tanshen tablets | |||||||
| Liu JR-b | 2010 | 48.6±6.9 | 49.2±7.3 | 30 | 32 | T: Acupuncture | 4 weeks |
| C: Compound Tanshen tablets | |||||||
T, treated group or experiment group; C, control group.
Effect of acupuncture on angina symptoms
All the eight trials reported the clinical curative effects of angina relief. No significant heterogeneity between trials was observed (I2=0%, P=0.57), and the fixed-effect model was employed to calculate the effect. The rate of overall angina relief was higher in experimental group than that in control group (90.1% versus 75.7%). As shown in Figure 2, we found that patients treated with acupuncture therapy statistically increased the curative effects and reduced angina symptoms than that in patients with conventional drugs (OR=2.89, 95% CI=1.87-4.47, P<0.00001).
Figure 2.
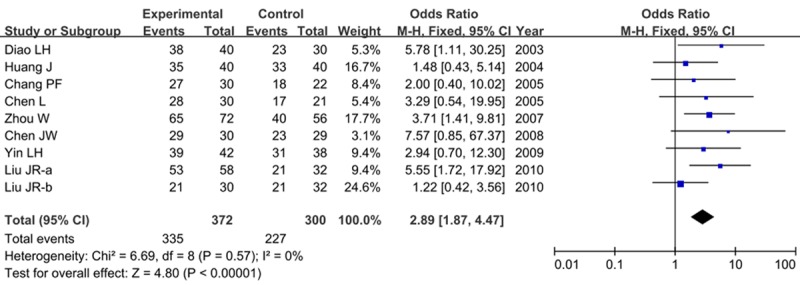
Forest plot of the clinical curative effects in effective improvement of angina symptoms between experiment group (acupuncture therapy) and control group (conventional drugs).
Improvement of electrocardiography (ECG) with acupuncture
Seven studies reported the efficacy of acupuncture in ECG improvement. There was no significant heterogeneity among studies (I2=0%, P=0.67), and the fixed-effect model was used. Our results demonstrated that acupuncture therapy was superior compared with the conventional drugs for the improvement of ST segment ischemia (OR=1.83, 95% CI=1.23-2.71, P=0.003) as shown in Figure 3.
Figure 3.
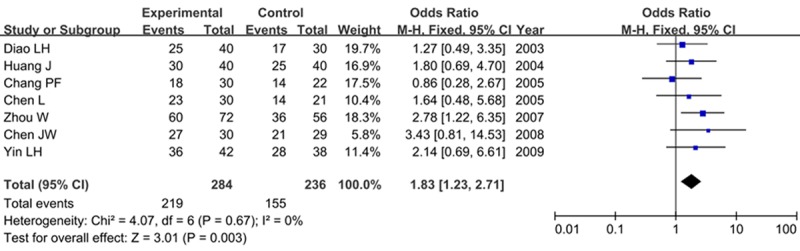
Forest plot of the efficacy of acupuncture in improving electrocardiography.
Effect of acupuncture on the time to onset of angina relief
Only one study reported the effect of acupuncture on the time to onset of angina relief. The fixed-effect model was employed to conduct this meta-analysis in which no combined effect was applied. The result showed that acupuncture had a slower onset of action compared to nitrates (MD=2.44, 95% CI=1.64-3.24, P<0.00001, min) as shown in Figure 4.
Figure 4.

Forest plot on the time to onset of angina relief between experiment group and control group.
Reduction of nitroglycerin consumption with acupuncture
Four trials reported the consumption of existing anti-anginal medications. Two reported the response rate of nitroglycerin withdrawal, while the others reported the nitroglycerin consumption. For dichotomous data, our results showed that there was no significant difference in overall effective rate between two groups (OR=2.13, 95% CI=0.90-5.07, P=0.09) in a fixed-effect model as shown in Figure 5A. No significant difference was found in the complete effective rate (OR=2.01, 95% CI=0.90-4.46, P=0.09, Figure 5B) or the partial effective rate (OR=0.95, 95% CI=0.45-1.98, P=0.88, Figure 5C) as well.
Figure 5.
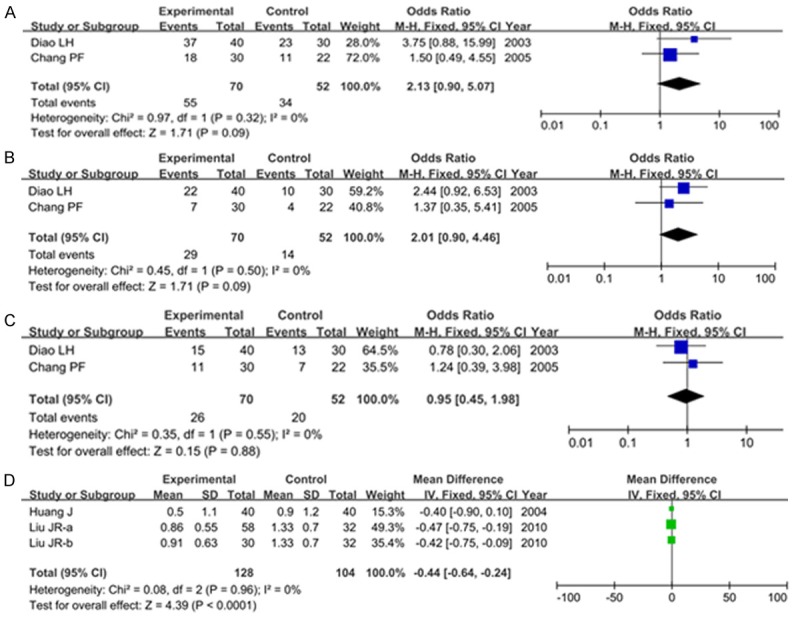
Forest plot on reduction of nitroglycerin with acupuncture: A. Overall effective rate; B. Complete effective rate; C. Partial effective rate; D. Reduction on nitroglycerin consumption.
For continuous data, we found a significant reduction on nitroglycerin consumption in acupuncture group than that in control group (MD=-0.44, 95% CI=-0.64, -0.24, P<0.0001, mg) in a fixed-effect model as shown in Figure 5D.
Adverse event
None of the studies reported any adverse effects associated with acupuncture therapy.
Publication bias
Funnel plots of above results detected no obvious publication bias, indicating that the results are reliable as shown in Figure 6.
Figure 6.

Funnel plot of the clinical curative effects of angina symptoms relief in this meta-analysis.
Discussion
Angina pectoris is a common condition with worrying symptoms and an increased risk of suffering cardiovascular complications such as acute myocardial infarction or death. It attributes to continuous imbalance between myocardial oxygen delivery and oxygen demand. Angina pectoris can be stable or unstable. Stable angina pectoris is due to a flow/demand imbalance between reduced blood flow through narrow coronary arteries and the demand placed on the heart [20]. Cessation of the ischemic event will result in rapid angina relief. Nitrates and beta-blocking agents are the most effective, commonly used drugs in the treatment of angina pectoris [21,22]. Nitrates can increase venous capacitance and decrease left ventricular volume, but it also may increase oxygen supply by favorably redistributing flow to ischemic zones [23]. The beta-blocking agent propranolol can decrease both heart rate and contractility but tends to increase left ventricular volume [24]. These adverse effect limit the usefulness of drugs in patients with stable angina pectoris. Therefore, there is an urgent need to explore new drugs or treatment methods.
In this meta-analysis, we assessed the effectiveness and safety of acupuncture therapy for angina pectoris. Our results found that patients with acupuncture therapy significantly increased the clinical curative effects of angina relief, improved the electrocardiography, and reduced the nitroglycerin consumption than that with conventional drugs. No acupuncture related adverse effect was found.
Acupuncture, an important component of traditional Chinese medicine, is the insertion and stimulation of needles at specific points on the body to bring a general sense of wellness. The manipulation of the needles on the channels (jingluo) regulates the balance of qi, yinyang and wuxing in the body [25]. It has been recorded in China and other Asian countries for thousands of years. Nowadays, it is widely used in the West countries as well. According to the latest estimates, at least 3 million adults and children use acupuncture every year in United States [26].
Studies have demonstrated that acupuncture can be effective for certain health problems, such as some types of chronic pain. Acupuncture is a useful adjunctive therapy in reducing dyspnea on exertion in patients with chronic obstructive pulmonary disease [27]. Traditional acupuncture results in intermediate effects on autonomic function in stable ischemic heart disease patients [28]. Both acupuncture and bee venom acupuncture showed promising results as adjuvant therapies for Parkinson’s disease [29]. Acupuncture combined with exercise is effective for shoulder pain after stroke [30]. Acupuncture has been used in angina pectoris for several decades. Richter et al. have found that acupuncture showed a beneficial effect in patients with severe, intensively treated angina pectoris [31]. Zhou et al. have identified that the time from the end of exercise to the disappearance of angina pectoris in acupuncture group was shorter than that in the control groups (P<0.05) [32]. Ballegaard et al. have suggested that acupuncture may improve cardiac work capacity in patients with angina pectoris, refractory to medical treatment [33]. They also concluded that acupuncture, due to hemodynamic alterations, might have a specific effect on angina pectoris in addition to drug treatments [16]. The addition of acupuncture was found to be cost beneficial in patients with advanced angina pectoris [34]. Patients with acupuncture of supplementing and activating Zongqi could effectively treat stable and exertional angina pectoris [35].
Acupuncture combined with conventional drugs (ACCD) can play a role in the treatment of several diseases. Acupuncture plus Plantain and Senna Granule (Chinese herbs) can significantly decrease gastrointestinal transit time and defecation cycle in patients with functional constipation [36]. Acupuncture combined with paroxetine can accelerate the clinical response to selective serotonin reuptake inhibitors and prevent the aggravation of depression [37]. Acupuncture combined with Chinese herbal medicine is an effective therapy for cardiovascular disease [38]. ACCD acts as an therapy of angina pectoris as well. Xu et al. found a significant difference between ACCD group (treatment group) and conventional drugs group (control group), with the total effective rates for symptoms and electrocardiogram were 88.6% and 62.9% in the treatment group and 60.0% and 31.4% in the control group, respectively, indicating that ACCD is safe and effective for intractable angina pectoris and it can improve short-term prognosis [39]. Li et al. showed that ACCD, which is better than western medicine on the aspects of serum lipid, blood flow virility, syndrome and antioxidant, is one of effective methods for angina pectoris and can effectively increase therapeutic effect of angina pectoris than simple Chinese herbs [40]. Zhao et al. suggested that ACCD is a better method for treatment of angina pectoris [41]. Cao et al. demonstrated that ACCD can increase therapeutic effect than western medicine on unstable angina pectoris and clinically, it is one of effective methods for angina pectoris [42]. A meta-analysis conducted by Chen et al. investigating 21 RCTs found that ACCD reduced the occurrence of acute myocardial infarction, relieved angina symptoms and improved ECG [43]. A recent review showed that combination of conventional drug therapy and acupuncture would considerably decrease the frequency and the required dosage of drug taking, thereby decreasing the unpleasant side effects of the drug therapy [17].
Several limitations were presented in this meta-analysis. Firstly, conventional drugs in control group were different, this may bring some deviation. Secondly, for outcome of the time to onset of angina relief with acupuncture, only one trial included. Thirdly, the result of some outcomes presented in different expression method such as nitroglycerin consumption. Fourthly, acupuncture combined with traditional medicines or other factors may play a role in angina pectoris.
In conclusion, we found that acupuncture therapy was superior to the conventional drugs in increasing the clinical curative effects of angina relief, improving the electrocardiography, and reducing the nitroglycerin consumption, indicating that acupuncture therapy may be effective and safe for treating stable angina pectoris. However, further clinical trials are needed to systematically and comprehensively evaluate acupuncture therapy in angina pectoris.
Acknowledgements
This work was supported by Traditional Chinese Medicine Program on Senile Disease Research (2012-32).
Disclosure of conflict of interest
None.
References
- 1.Wang J, Liao E, Huang C, Qi H. Internal medicine (for 8-year and 7-year clinical and other professional) Vol 283. Beijing: People’s Medical Publishing House; 2010. p. 292. [Google Scholar]
- 2.Gibbons RJ, Abrams J, Chatterjee K, Daley J, Deedwania PC, Douglas JS, Ferguson TB, Fihn SD, Fraker TD, Gardin JM. ACC/AHA 2002 guideline update for the management of patients with chronic stable angina-summary articlea report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Chronic Stable Angina) J Am Coll Cardiol. 2003;41:159–168. doi: 10.1016/s0735-1097(02)02848-6. [DOI] [PubMed] [Google Scholar]
- 3.Lo MY, Bonthala N, Holper EM, Banks K, Murphy SA, McGuire DK, de Lemos JA, Khera A. A risk score for predicting coronary artery disease in women with angina pectoris and abnormal stress test finding. Am J Cardiology. 2013;111:781–785. doi: 10.1016/j.amjcard.2012.11.043. [DOI] [PubMed] [Google Scholar]
- 4.Skalidis EI, Vardas PE. Guidelines on the management of stable angina pectoris. Eur Heart J. 2006;27:2606–2606. doi: 10.1093/eurheartj/ehl257. [DOI] [PubMed] [Google Scholar]
- 5.Feng K. The Epidemiology Study of Risk Factors of Angina and Myocardial Infarction in Elderly. Beijing: Med Coll of Chin people’s Liberation Army; 2006. pp. 18–19. [Google Scholar]
- 6.Parker JD, Parker JO. Nitrate Therapy for Stable Angina Pectoris. Survey of Anesthesiology. 1999;43:6. [Google Scholar]
- 7.Acupuncture N. Acupuncture. JAMA. 1998;280:1518–1524. [PubMed] [Google Scholar]
- 8.Stux G. Basics of Acupuncture. Springer; 2003. [Google Scholar]
- 9.White A, Cummings TM, Filshie J. An introduction to western medical acupuncture. 2008. [Google Scholar]
- 10.White AR, Rampes H, Liu JP, Stead LF, Campbell J. Acupuncture and related interventions for smoking cessation. Cochrane Database Syst Rev. 2014;23:1. doi: 10.1002/14651858.CD000009.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.NIH Consensus Conference. Acupuncture. JAMA. 1998;280:1518–1524. [PubMed] [Google Scholar]
- 12.Zheng GQ, Zhao ZM, Wang Y, Gu Y, Li Y, Chen XM, Fu SP, Shen J. Meta-analysis of scalp acupuncture for acute hypertensive intracerebral hemorrhage. J Altern Complement Med. 2011;17:293–299. doi: 10.1089/acm.2010.0156. [DOI] [PubMed] [Google Scholar]
- 13.Wang Y, Shen J, Wang Xm, Fu Dl, Chen CY, Lu LY, Lu L, Xie Cl, Fang JQ, Zheng GQ. Scalp acupuncture for acute ischemic stroke: a meta-analysis of randomized controlled trials. Evid Based Complement Altern Med. 2012;2012:480950. doi: 10.1155/2012/480950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Vickers AJ, Cronin AM, Maschino AC, Lewith G, MacPherson H, Foster NE, Sherman KJ, Witt CM, Linde K, Collaboration AT. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Int Med. 2012;172:1444–1453. doi: 10.1001/archinternmed.2012.3654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Middlekauff HR. Acupuncture in the treatment of heart failure. Cardiol Rev. 2004;12:171–173. doi: 10.1097/01.crd.0000103650.71735.f0. [DOI] [PubMed] [Google Scholar]
- 16.Ballegaard S, Karpatschoff B, Holck J, Meyer C, Trojaborg W. Acupuncture in angina pectoris: do psycho-social and neurophysiological factors relate to the effect? Acupunct Electrother Res. 1994;20:101–116. doi: 10.3727/036012995816357113. [DOI] [PubMed] [Google Scholar]
- 17.Xu L, Xu H, Gao W, Wang W, Zhang H, Lu DP. Treating angina pectoris by acupuncture therapy. Acupunct Electrother Res. 2013;38:17–35. doi: 10.3727/036012913x13831831849457. [DOI] [PubMed] [Google Scholar]
- 18.Diao L. Clinical observation on acupuncture for angina pectoris. Liaoning journal of traditional Chinese medicine. 2003;30:667–68. [Google Scholar]
- 19.Liu J, Tan Y, Pan W. Clinical observation of acupuncture trerapy in angina pectoris. Journal of New Chinese Medicine. 2010;42:68–70. [Google Scholar]
- 20.Valgimigli M, Biscaglia S. Stable Angina Pectoris. Curr Atheroscler Rep. 2014;16:1–10. doi: 10.1007/s11883-014-0422-4. [DOI] [PubMed] [Google Scholar]
- 21.Wood AJ, Parker JD, Parker JO. Nitrate therapy for stable angina pectoris. N Engl J Med. 1998;338:520–531. doi: 10.1056/NEJM199802193380807. [DOI] [PubMed] [Google Scholar]
- 22.Lahiri A, Rodrigues EA, Al-Khawaja I, Raftery EB, Hinge D. Effects of a new vasodilating beta-blocking drug, carvedilol, on left ventricular function in stable angina pectoris. Am J Cardiol. 1987;59:769–774. doi: 10.1016/0002-9149(87)91089-7. [DOI] [PubMed] [Google Scholar]
- 23.Heidenreich PA, McDonald KM, Hastie T, Fadel B, Hagan V, Lee BK, Hlatky MA. Meta-analysis of trials comparing β-blockers, calcium antagonists, and nitrates for stable angina. JAMA. 1999;281:1927–1936. doi: 10.1001/jama.281.20.1927. [DOI] [PubMed] [Google Scholar]
- 24.Leon MB, Rosing DR, Bonow RO, Lipson LC, Epstein SE. Clinical efficacy of verapamil alone and combined with propranolol in treating patients with chronic stable angina pectoris. Am J Cardiol. 1981;48:131–139. doi: 10.1016/0002-9149(81)90582-8. [DOI] [PubMed] [Google Scholar]
- 25.Napadow V, Ahn A, Longhurst J, Lao L, Stener-Victorin E, Harris R, Langevin HM. The status and future of acupuncture mechanism research. J Altern Complement Med. 2008;14:861–869. doi: 10.1089/acm.2008.SAR-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Barnes PM, Bloom B, Nahin RL, et al. Complementary and alternative medicine use among adults and children: United States, 2007. National Health Statistics Reports. 2008 US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics Hyattsville, MD. [PubMed] [Google Scholar]
- 27.Suzuki M, Muro S, Ando Y, Omori T, Shiota T, Endo K, Sato S, Aihara K, Matsumoto M, Suzuki S. A randomized, placebo-controlled trial of acupuncture in patients with chronic obstructive pulmonary disease (COPD): the COPD-acupuncture trial (CAT) Arch Int Med. 2012;172:878–886. doi: 10.1001/archinternmed.2012.1233. [DOI] [PubMed] [Google Scholar]
- 28.Mehta PK, Polk DM, Zhang X, Li N, Painovich J, Kothawade K, Kirschner J, Qiao Y, Ma X, Ida YD. A randomized controlled trial of acupuncture in stable ischemic heart disease patients. Int J Cardiol. 2014;176:367–74. doi: 10.1016/j.ijcard.2014.07.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cho SY, Shim SR, Rhee HY, Park HJ, Jung WS, Moon SK, Park JM, Ko CN, Cho KH, Park SU. Effectiveness of acupuncture and bee venom acupuncture in idiopathic Parkinson’s disease. Parkinsonism Relat Disord. 2012;18:948–952. doi: 10.1016/j.parkreldis.2012.04.030. [DOI] [PubMed] [Google Scholar]
- 30.Lee JA, Park SW, Hwang PW, Lim SM, Kook S, Choi KI, Kang KS. Acupuncture for shoulder pain after stroke: a systematic review. J Altern Complement Med. 2012;18:818–823. doi: 10.1089/acm.2011.0457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Richter A, Herlitz J, Hjalmarson A. Effect of acupuncture in patients with angina pectoris. Eur Heart J. 1991;12:175–178. doi: 10.1093/oxfordjournals.eurheartj.a059865. [DOI] [PubMed] [Google Scholar]
- 32.Zhou X, Liu J. [Metrological analysis for efficacy of acupuncture on angina pectoris] . Zhongguo Zhong Xi Yi Jie He Za Zhi. 1993;13:212–214. 196. [PubMed] [Google Scholar]
- 33.Ballegaard S, Jensen G, Pedersen F, Nissen VH. Acupuncture in severe, stable angina pectoris: a randomized trial. Acta Medica Scandinavica. 1986;220:307–313. doi: 10.1111/j.0954-6820.1986.tb02770.x. [DOI] [PubMed] [Google Scholar]
- 34.Ballegaard S, Johannessen A, Karpatschof B, Nyboe J. Addition of acupuncture and self-care education in the treatment of patients with severe angina pectoris may be cost beneficial: an open, prospective study. J Altern Complement Med. 1999;5:405–413. doi: 10.1089/acm.1999.5.405. [DOI] [PubMed] [Google Scholar]
- 35.Li Y, Guo L. [Thirty-five cases of stable and exertional angina pectoris treated with acupuncture of supplementing and activating Zongqi] . Zhongguo Zhen Jiu. 2013;33:173–174. [PubMed] [Google Scholar]
- 36.Guo L, Zhang C, Guo X. [Acupuncture combined with Chinese herbal medicine Plantain and Senna Granule in treatment of functional constipation: a randomized, controlled trial] . Zhong Xi Yi Jie He Xue Bao. 2011;9:1206–1214. doi: 10.3736/jcim20111108. [DOI] [PubMed] [Google Scholar]
- 37.Qu SS, Huang Y, Zhang ZJ, Chen JQ, Lin RY, Wang CQ, Li GL, Wong HK, Zhao CH, Pan JY. A 6-week randomized controlled trial with 4-week follow-up of acupuncture combined with paroxetine in patients with major depressive disorder. J Psychiatr Res. 2013;47:726–732. doi: 10.1016/j.jpsychires.2013.02.004. [DOI] [PubMed] [Google Scholar]
- 38.Xu J, Wu H. Chinese herbal medicine and acupuncture for the treatment of cardiovascular disease. J Geriatr Cardiol. 2009;6:56–61. [Google Scholar]
- 39.Xu F, Wang J. [Clinical observation on acupuncture combined with medication for intractable angina pectoris] . Zhongguo Zhen Jiu. 2005;25:89–91. [PubMed] [Google Scholar]
- 40.LI HX, WANG J, LU GR. Comparison study on angina pectoris treated with combination therapy and simple Chinese herbs. Chinese Journal of Information on TCM. 2005;2:010. [Google Scholar]
- 41.Yanling Z, Chenguang T, Wei Z. Clinical therapeutic effect of combination of acupuncture and medicine and effects on plasma et and cgrp contents in the patient of angina pectoris . Chinese Acuponcture Moxibustion. 2001;2:002. [Google Scholar]
- 42.Jianping C, Feng G, Kan L. Clinical Therapeutic effect of acupuncture combined with medication on unstable angina pectoris and observation on dynamic ECG. Chinese Acuponcture Moxibustion. 2002;6:000. [Google Scholar]
- 43.Chen J, Ren Y, Tang Y, Li Z, Liang F. Acupuncture therapy for angina pectoris: a systematic review. J Traditl Chin Med. 2012;32:494–501. doi: 10.1016/s0254-6272(13)60061-8. [DOI] [PubMed] [Google Scholar]