

Abstract
The purpose of the current meta-analysis was to compare the efficacy of core decompression (CD) and conservative treatment (CT) for saving femoral heads in patients with avascular necrosis of femoral head (ANFH). Four RCTs and two CCTs involving 323 hips with 24- to 48-months follow-up were included in this review. Our results suggested CD had a trend of favorable results in contrast to other CT (OR 3.28; 95% CI 0.77-14.02; P = 0.11) but saved much less hips compared to biophysical treatments [odds ratio (OR) 0.37; 95% CI 0.18-0.74; P = 0.005]. In the stratified survival rate analysis by ANFH stage, interestingly, CD group got a significantly higher successful rate of hip joint conservation than other CT group in both stage I and stage II-III (stage I: OR 4.43; 95% CI 1.34-14.65; P = 0.01; stage II-III: OR 6.75; 95% CI 2.18-20.90; P = 0.0009). In the biophysical stimulation subgroup, however, an even higher frequency of survived hips were observed compared to CD group at stage II-III (CD vs. biophysical stimulation: OR 0.34; 95% CI 0.17-0.67; P = 0.002). In conclusion, performing CD for ANFH is effective for preventing femoral collapse within a short-term follow-up, but an even higher successful rate were expected by biophysical stimulations. Nevertheless, the short-term follow-up, the small sample size of the current meta-analysis only provide limited quality of evidence, which required confirmation from further large-scale, well-designed RCT with longer follow-up.
Keywords: Avascular necrosis, osteonecrosis, core decompression, conservative treatment, meta-analysis
Introduction
Osteonecrosis or avascular necrosis of femoral head (ANFH) is a disabling clinical disease that affects 20,000 persons each year in the United States. The progressive diseases is characterized by reduced local blood flow, death of the osteocytes and the bone marrow [1], leading to a progressive destruction of bone architecture, subchondral fracture, extensive hip pain and loss of joint function. Ultimately, after collapse of femoral head, a standard total hip arthroplasty (THA) is indicated [2,3].
However, because of the young age of many of these patients, a hip replacement cannot be expected to last the patient’s lifetime; therefore, when feasible, attempts should be made to save the femoral head prior to collapse with less invasive treatment modalities [4-6]. Core decompression (CD) is an easy-performed and popular procedure which has been used for the treatment of the osteonecrosis for approximately three decades [7-9]. CD performs the therapeutic effect mainly through the reduction of intra-medullary pressure, therefore preventing neurovascular compression and promoting healthy new bone formation [10]. A systematic review has revealed that the total clinical success rate of CD, with or without cancellous bone grafting, was 63.5%, and the rate for subsequent joint replacement surgery or hip salvage surgery was about 33% of the patients [8].
In the last decade, non-invasive treatment options with potential benefits were also widely considered for this population. Pharmacologic agents, which have been used to treat osteonecrosis of the hip are statins [11,12], anticoagulants [13,14], prostacyclin [15,16], and bisphosphonates (Bps) [17-26]. Moreover, extracorporeal shock-wave therapy (ESWT) [27-29] and electromagnetic therapy [30-32], have shown effective for early ANFH due to the increased ingrowth of neovascularization and new bone formation. However, there is still considerable controversy concerning effectiveness of such conservative treatments (CT) [9,10].
In order to achieve a practical clinical decision, an integrative understanding of the clinical successful rate was needed for patients in CD group and CT group. From our literature search, there are 3 reviews aiming to compare the two therapeutic treatments in ANFH patients. Nevertheless, all of them only included uncontrolled trials and did not clarify all the varied CT procedures, which dramatically impaired the strength and complicated the interpretation of their conclusions [7-9].
Therefore, it is still unclear whether CD or CT has a better efficacy. It is necessary to perform a quantitative synthesis of the controlled trials using rigorous methods. Herein, we conducted the current study to analyze and evaluate the survival rates of femoral heads treated with CD or CT by summarizing all available controlled clinical trials in a meta-analysis manner.
Methods
Literature search
Electronic databases (PubMed, EMBASE, and the Cochrane Central Register of Controlled Trials) were searched restricted to “clinical trials” by two independent investigators (HYC. and LT.), which were updated in October, 2014. The search used terms and Boolean operators as follows: “(osteonecrosis of the femoral head OR femoral head necrosis OR necrosis of femoral head) AND (core decompression OR center decompression)”. There was no limitation on year of publication, or publication status. We manually searched reference lists of review articles and included studies to identify other potentially eligible studies as well.
Identification of eligible studies
Trials were included if they contained all of the following: (1) The study was randomized controlled trials (RCTs) or controlled clinical trials (CCTs); (2) The study exclusively targeted patients with ANFH; (3) The treatments arms comprised both CD group and CT group; (4) The study provided with adequate data on clinical successful rates after treatments (5) The language of publication was English. After exclusion of duplicates, 2 reviewers (ZHM. and LT) performed an initial title and abstract screening of articles to discard those that were clearly ineligible, then 2 reviewers (HYC. and ZHM.) independently examined the full article to assess the trials for eligibility for inclusion, with disagreements resolved by discussion. Citations were excluded if (1) They were non-controlled clinical trials; or (2) They combined CD with other procedures to treat ANFH; or (3) No information of survival rate of hips was provided. If necessary, we attempted to contact the author of the original report to obtain further details. In addition, the level of evidence of each study was rated on basis of Oxford Centre for Evidence-based Medicine-Levels of Evidence (March 2009) [33]. Disagreement was resolved by discussion [34].
Data abstraction, conversion and analysis
From each article we extracted the following details: authors, year of publication, and geographical location of study, study design, study population (hips/patients), patient gender/age, stage of ANFH, detection of ANFH, CT type, and follow-up duration by using standardized forms.
The outcome of our interest primarily focused on the conservation of femoral head after treatment of CD or CT. The femoral head survival rates were defined as avoidance of THA or any other further intervention at the end of follow-up. Those data across the inclusion studies were pooled and summarized estimates of treatment effect as odds ratio (OR) with 95% confidence intervals (CI) using the Mantel-Haenszel method. We also assessed the inconsistency I2 to describe the percentage of the variability in effect estimates due to the heterogeneity. We considered P value of I2 less than 0.05 as the substantial heterogeneity. Fixed effects model would be applied if there were no statistical heterogeneity among the studies; otherwise, we used the random effects model [34].
Although various classification systems were applied among studies, they shared fundamental similarities and therefore the equivalent classification systems were converted in accordance with Ficat classification system [4,35]. Then stratified survival rate was analyzed, in which the extracted follow-up data were investigated after equivalent stage classification being made, including group 1: stage I and group 2: stage II-III. The combination of stage II and III were due to the insufficient number of patients in an individual stage. In addition, subgroup analysis will be performed according to the varied CT type in each study to explain the substantial heterogeneities, if applicable.
The Review Manager (RevMan 5.3) software program (The Nortic Cochrane Centre, Copenhagen, Denmark, provided by The Cochrane Collaboration) was used for graphical representation of the pooled data.
To assess for publication bias, we conducted funnel plots to examine sample size versus treatment effect across included studies. Results from small studies scatter widely at the bottom of the graph, whereas the spread narrows for larger studies. In the absence of bias, the plot resembles a symmetrical inverted funnel. Conversely, if there is bias, funnel plots are often skewed and asymmetrical [34]. In addition, we performed post hoc sensitivity analysis by omitting the every single study from the main meta-analysis to determine their influences to overall effects [36].
Results
tudy identification
Figure 1 detailed articles identification, inclusion, and exclusion. Our search strategy initially yielded 169 citations. Of these, we included 4 RCTs and 1 CCTs. Additionally, we found 1 relevant CCT [37] from the references of a review article [8]. Therefore, 6 studies with 323 hips (CD group: 160 hips and CT group: 163 hips) providing usable information were included in this meta-analysis [37-42]. Table 1A and 1B shows the characteristics of the included articles. All studies were comparing CD and CT treatments in ANFH patients with follow-up of 24-48 months, among which, the conservative strategies varied in CT group and there are 4 studies using pulsing electromagnetic fields (PEMF) [42], physical therapy [38], restricted weight bearing [39], or extracorporeal shock wave treatment (ESWT) [40], respectively. The other 2 studies did not specify the conservative procedures [37,41]. The included studies exclusively targeted ANFH patients, most of whom were caused by chronic usage of steroid or alcohol. Only one study targeted patients with sickle cell disease and did not provide stratified survival rates [38]. The studied patients were all within stage III according to Ficat system [37,39,42], Steinberg (University of Pennsylvania staging system) [38], or Association Research Circulation Osseous (ARCO staging system) [40,41]. Overall, the level of evidence for the mentioned studies ranged from 1b to 2b1 [33].
Figure 1.
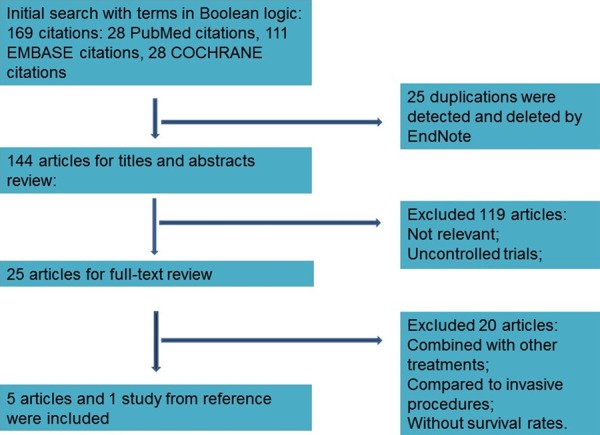
A flow diagram demonstrates the method of article selection for clinical study inclusion.
Table 1A.
Characteristics of the included studies
| Author/Year/Area | Study design | Number of hips | Gender (F/M) | Average age (year) | |||
|---|---|---|---|---|---|---|---|
|
|
|
|
|||||
| CD | CT | CD | CT | CD | CT | ||
| Aaron/1989/USA | CCT | 50 | 56 | NA | NA | 43 ± 2 | 43 ± 3 |
| Koo/1995/Korea | RCT | 18 | 19 | NA | NA | 47 (18-68) | 47 (18-68) |
| Neumayr/2006/USA | RCT | 17 | 21 | 9 | 10/11 | 24.67 | 26.41 |
| Robinson/1993/USA | CCT | 19 | 16 | NA | NA | NA | NA |
| Stulberg/1990/USA | RCT | 29 | 26 | NA | NA | 38.6 (15-65) | 38.6 (15-65) |
| Wang/2005/Taiwan | RCT | 28 | 29 | 2/23 | 3/20 | 39.9 ± 9.3 | 39.8 ± 12.1 |
Abbreviations: CD: core decompression; CT: conservative treatments; CCT: controlled clinical trial; RCT: randomized controlled trial; NA: Not available.
Table 1B.
Characteristics of the included studies
| Author/Year/Area | Stage of ANFH (n) | CT type | Average follow-up (month) | Level of evidence* | |
|---|---|---|---|---|---|
|
| |||||
| CD | CT | ||||
| Aaron/1989/USA | Ficat stage II (26), III (24), | Ficat stage II (23), III (33), | PEMF | CD: 38 ± 3; CT: 35 ± 2 | 2b |
| Koo/1995/Korea | ARCO: stage I, II (19); III (11) | ARCO: stage I, II (25); III (6) | No Specified | 24-45 | 1b |
| Neumayr/2006/USA | Upenn stage I (2), II (5), III (10), | Upenn stage I (8), II (6), III (7), | Physical Therapy | 36 | 1b |
| Robinson/1993/USA | Ficat stage 0 (4) I (6); II (9) | Ficat stage 0 (2) I (3); II (11) | No Specified | 48 | 2b |
| Stulberg/1990/USA | Ficat stage I (10); II (7); III (11) | Ficat stage I (5); II (7); III (10) | Nonweight bearing | 26.8 | 1b |
| Wang/2005/Taiwan | ARCO: stage I (2); II (17); III (9) | ARCO: stage I (3); II (10); III (16) | EWST | 24 | 1b |
Abbreviations: CD: core decompression; CT: conservative treatments; ANFH: avascular necrosis of femoral head PEMF: pulsing electromagnetic fields; ARCO: Association Research Circulation Osseous; Upenn: University of pennsylvania system (Steinberg); ESWT: extracorporeal shock wave treatment;
The level of evidence was rated on basis of Oxford Centre for Evidence-based Medicine-Levels of Evidence (March 2009).
Survival rate of femoral head treated with CD group vs. CT group
As an end-point of follow-up, all of the six included studies reported the survival rate. The main meta-analysis were performed using the six studies with 323 hips (CD group 160 hips and CT group 163 hips were followed) [37-42]. From Figure 2, substantial heterogeneities were observed across the included studies in the comparison of overall rate of surviving femoral head between CD group and CT group (I2 = 81%, P < 0.0001), thereby the random effects model was used. The heterogeneities mainly stemmed from the varied conservative strategies across studies. For instance, the efficacies of biophysical intervention adopted by Aaron’s (PEMF) [42] and Wang’s study (ESWT) [40], are much stronger than the other conservative treatment, like restricted weight-bearing [39]. Our subgroup analysis divided by the CT type (CD vs. biophysical stimulation or CD vs. other CT) confirmed this assumption, heterogeneities were almost absent among CD vs. biophysical stimulation studies (I2 = 0%, P = 0.93; Figure 2) and in the rest studies the inconsistencies were reduced (I2 = 69%, P = 0.02; Figure 2). Interestingly, the comparison of CD vs. biophysical stimulation implied CD had a significantly less survival rate of hips compared to biophysical treatments (OR 0.37; 95% CI 0.18-0.74; P = 0.005; Figure 2). However, a trend of favorable results for CD was found in contrast to other CT (OR 3.28; 95% CI 0.77-14.02; P = 0.11; Figure 2) in the comparison of CD vs. other CT. In addition, our sensitive analysis suggested that, by omitting Neumayr’s study [38], the advantage of CD vs. other CT turned out to be statistically significant (CD vs. other CT: OR 5.15; 95% CI 1.02-26.01; P < 0.05). The participants of this study were much younger (24.7-26.4 years) and with a distinct etiology of ANFH (sickle disease) might be the reason (Table 1A and 1B).
Figure 2.
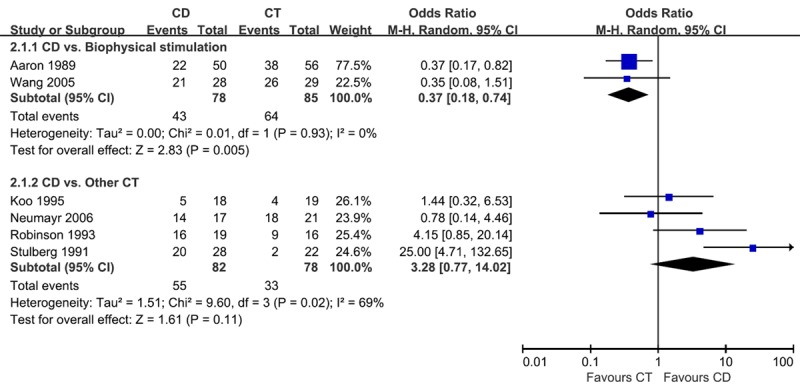
Graph showing comparing overall survival rate of femoral heads between core decompression (CD) and conservative treatment (CT) group in all the included patients. Then the results were divided into biophysical stimulation and other CT subgroups. The size of each square is proportional to the weight of the study. Z: p value of weighted test for overall effect, CI: confidence interval, df: degree of freedom, I2 test statistic.
Stratified survival rate of femoral head treated with CD group vs. CT group
Four studies involved with 54 hips described usable data in pre-collapse phase (Ficat stage I) of osteonecrosis but the results from Wang’s study (ESWT) [40] were not estimable due to the 100% survival rate in both groups. The data from the rest three studies using other CT were used for meta-analysis and only moderate heterogeneities were detected (I2 = 58%, P = 0.09; Figure 3) [37,39,41]. The fixed effects model was therefore applied and we found hips (66%, 21 of 32 hips; Figure 3) treated with CD survived more than those treated with other CT (40%, 5 of 20 hips; OR 4.43; 95% CI 1.34-14.65; P = 0.01; Figure 3). Thus, CD group got a significantly higher successful rate of hip joint conservation than CT group when treatment was performed at stage I.
Figure 3.
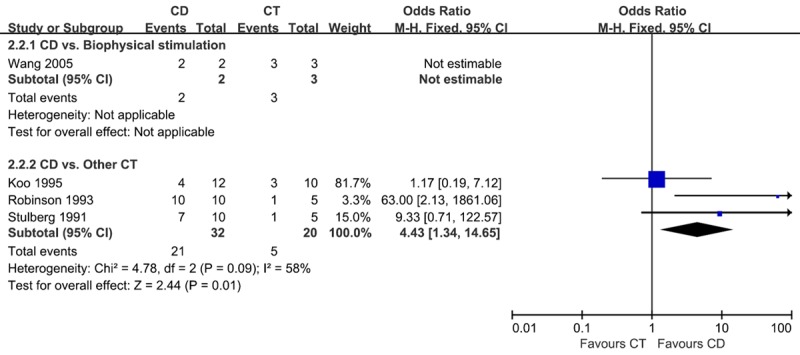
Graph showing comparing survival rate of femoral heads between core decompression (CD) and conservative treatment (CT) group in all the included patients at stage I. Then the results were divided into biophysical stimulation and other CT subgroups. The size of each square is proportional to the weight of the study. Z: p value of weighted test for overall effect, CI: confidence interval, df: degree of freedom, I2 test statistic.
In the treatment of the ANFH with Ficat stage II-III, 5 studies with a total of 228 hips were reported [37,39-42]. The remarkable heterogeneities were observed among the five studies (I2 = 80%, P = 0.0006). Similarly, when separately analyzed by CT type, heterogeneities were greatly decreased to be insignificant in both subgroups (CD vs. biophysical stimulation studies: I2 = 0%, P = 0.62; CD vs. other CT studies: I2 = 56%, P = 0.10; Figure 4). Therefore meta-analysis was conducted in fixed effect model. In the comparison of CD vs. biophysical stimulation, 39 of 76 hips (51%; Figure 4) treated in CD group were preserved, and a significantly higher frequency of survived hips were observed in biophysical intervention group (74%, 61 of 82 hips; CD vs. biophysical stimulation: OR 0.34; 95% CI 0.17-0.67; P = 0.002; Figure 4). In the later comparison, other CT seemed disappointedly inadequate to save hips, only 7 of 37 hips (19%; Figure 4) survived, which was obviously less than that in CD group (61%, 20 of 33 hips; CD vs. Other CT: OR 6.75; 95% CI 2.18-20.90; P = 0.0009; Figure 4).
Figure 4.
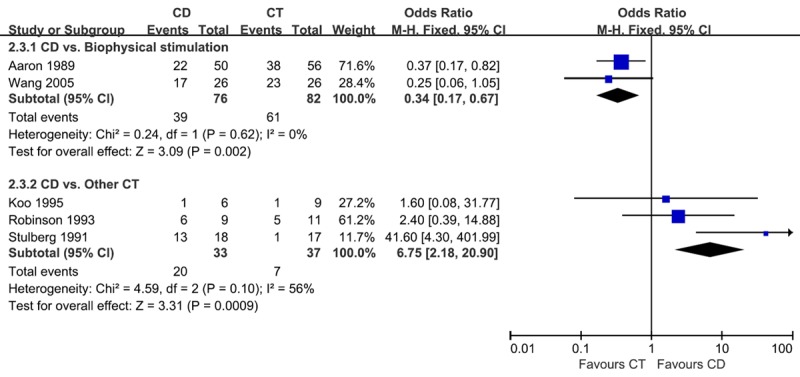
Graph showing comparing survival rate of femoral heads between core decompression (CD) and conservative treatment (CT) group in all the included patients at stage II-III. Then the results were divided into biophysical stimulation and other CT subgroups. The size of each square is proportional to the weight of the study. Z: p value of weighted test for overall effect, CI: confidence interval, df: degree of freedom, I2 test statistic.
Funnel plots did not demonstrate evidence of publication bias for overall survival rate of femoral heads between CD and CT group in all studies (Figure 5).
Figure 5.
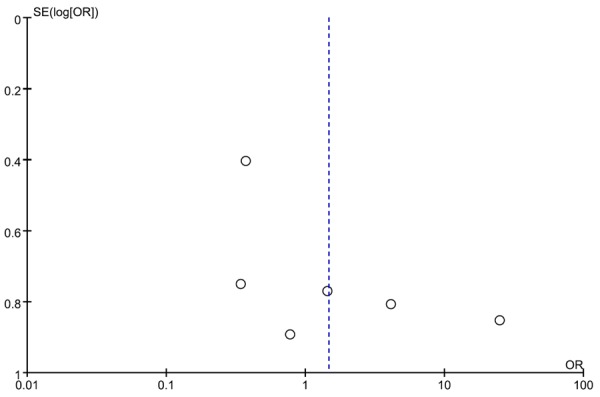
Funnel plot for overall survival rate of femoral heads between core decompression (CD) and conservative treatment (CT) group in all studies showed no publication bias in visual.
Discussion
The treatment for ANFH remains controversial and it is divided in conservative therapy and surgical procedures. Surgical interventions include core decompression, vascularized or non-vascularized bone-grafting, muscle pedicle grafting, rotational osteotomy, and total hip arthroplasty. While non-operative treatments include the use of bisphosphonates, statins, anticoagulants, biophysical stimulation with PEMF and ESWT [4,43].
CD is a widely used treatment for patients with ANFH, and the core track may promote the formation of healthy bone by reducing bone marrow pressure as well as inducing neovascularization. The clinical efficacy of CD was reported to closely associate with the stage and the size of necrotic lesion [27]. According to a previous systematic review conducted by Mont et al [8], stratification of the core decompression group into Ficat stages revealed better results for treatment of osteonecrosis in its early stages. Femoral head survival rate (clinical success) was 84% (190 of 227 hips) for Stage I, 65% (155 of 239 hips) for Stage II, and 47% (40 of 86 hips) for Stage III. Stratification by other etiologic and demographic factors did not influence overall percentages. Another two review articles reported similar results [7,9], therefore all of these 3 reviews suggested CD would have better results than CT group for treating ANFH especially at early stage [7-9]. However, lack of controlled trials and insufficient detailed explanation of the varied conservative procedures, which dramatically impaired the strength and complicated the interpretation of their conclusions.
In our meta-analysis, all the included studies were performed in a comparative manner. To achieve better clinical and practical understanding, the results from meta-analysis were stratified into Ficat stage I and stage II-III. However, the substantial heterogeneities were detected, which might due to varied procedures in CT groups. Subsequently, the most distinct aspect of our current meta-analysis was we successfully clarified the sources of such heterogeneities by our subgroup analysis. Also, the subgroup analysis was able to extensively explain the discrepancy of clinical results between biophysical intervention and other CT.
Specifically, the distinct mechanism of individual CT adopted in the included studies might be the reason. For example, reduced weight-bearing on the affected hip joint was adopted in one of our included studies as CT group, which have been advised with the expectation of prevention of femoral head collapse during the healing process of ANFH but it has been now been universally agreed this is not adequate to serve the purpose [44]. It is because the uncoupling bone formation and bone resorption in the necrotic area could not be reversed or retarded by the reduced loading [44]. Accordingly, our meta-analysis suggested CD generated a higher survival rate of femoral head than CT, such as restricted weight-bearing, both in stage I and stage II-III ANFH. This is also consistent with previous reviews [7-9]. On the other hand, the rationale for the use of ESWT or electromagnetic therapy for ANFH rested on that their stimulating neovascularization and new bone formation [44]. From literature search, the recent clinical trials regarding ESWT [27-29] and electromagnetic therapy [30-32] for early ANFH provided very encouraging results. Importantly, our current meta-analysis was first to support that biophysical intervention, like PEMF and ESWT were clearly more effective for preventing femoral head collapse compared to CD even at stage II-III. Although in stage I the data from Wang’s study (ESWT) was not estimable using meta-analysis, the observed 100% survival rates in both CD and ESWT group at this stage suggested a stronger curative efficacy of ESWT at earlier stage ANFH.
In addition, physical therapy achieved a relatively high successful rate (86%, 18 of 21 hips) which is comparable to that in CD group (82%, 14/17 hips) in Neumayr’s study [38]. This study recruited much younger patients (24.7-26.4 years old) with sickle disease which might imply the age and the etiology of ANFH might influence the outcome of conservative treatments although further research should be carried out to confirm this.
There are some limitations of this study should be discussed. First of all, only published studies were included in the present meta-analysis. Thus, publication bias may have occurred. But, secondly, the heterogeneity, as one of the major concerns in meta-analysis for the validity of meta-analysis [35], may distort the meta-analysis. However, the potential confounding bias and inconsistencies were clearly discussed by sensitivity analysis and subgroup analysis. Last, there were only six studies with short- and mid-term follow-up included in the current analysis and the number of studies in the subgroup analysis was also limited. Nevertheless, the current meta-analysis is the first comparing CD with CT in a comparative manner by summarizing all the available RCTs and CCTs, which was expected to provide evidence with higher quality for clinical practice or future research.
Bearing in mind the above-mentioned limitations, the interpretation of above finding has clinical significances. Owing to the young age of many of these patients, a hip replacement cannot be expected to last the patient’s lifetime. Therefore, the clinical goal of intervention was to save the femoral head prior to collapse, and the use of less invasive treatment modalities is preferred [4-6]. Our results confirmed when compared to conventional CT, CD is an effective strategy for ANFH. However, non-invasive biophysical stimulation, such as PEMF and ESWT, is even more promising even at stage II-III than invasive CD.
In conclusion, performing CD for ANFH is effective for preventing femoral collapse within a short-term follow-up, but an even higher successful rate were suggested by biophysical stimulations. Nevertheless, the short-term follow-up, the small sample size of the current meta-analysis only provide limited quality of evidence, which required confirmation from further large-scale, well-designed RCT with longer follow-up.
Acknowledgements
All authors contributed to the conceptions of the study and interpretation of data. The study was designed by SJB, HYC and ZHM. HYC, and LT performed the literature search and collected data. ZHM and LT analyze and interpret data. HYC, LT and SJB drafted the manuscript with input from all the authors. The approval of the final version of the manuscript was given by all the authors. SJB acts as the guarantor. All the authors had full access to all of the data, including statistical reports and figures, in the study and can take responsibility for the integrity of the data and the accuracy of the analysis. This work is supported by Department of Science and Technology, Zhejiang Province (2013C33G2010401).
Disclosure of conflict of interest
None.
References
- 1.Seamon J, Keller T, Saleh J, Cui Q. The pathogenesis of nontraumatic osteonecrosis. Arthritis. 2012;2012:601763. doi: 10.1155/2012/601763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mont MA, Seyler TM, Plate JF, Delanois RE, Parvizi J. Uncemented total hip arthroplasty in young adults with osteonecrosis of the femoral head: a comparative study. J Bone Joint Surg Am. 2006;88(Suppl 3):104–109. doi: 10.2106/JBJS.F.00451. [DOI] [PubMed] [Google Scholar]
- 3.Mont MA, Seyler TM, Marker DR, Marulanda GA, Delanois RE. Use of metal-on-metal total hip resurfacing for the treatment of osteonecrosis of the femoral head. J Bone Joint Surg Am. 2006;88(Suppl 3):90–97. doi: 10.2106/JBJS.F.00543. [DOI] [PubMed] [Google Scholar]
- 4.Marker DR, Seyler TM, McGrath MS, Delanois RE, Ulrich SD, Mont MA. Treatment of early stage osteonecrosis of the femoral head. J Bone Joint Surg Am. 2008;90(Suppl 4):175–187. doi: 10.2106/JBJS.H.00671. [DOI] [PubMed] [Google Scholar]
- 5.Berry DJ, Harmsen WS, Cabanela ME, Morrey BF. Twenty-five-year survivorship of two thousand consecutive primary Charnley total hip replacements: factors affecting survivorship of acetabular and femoral components. J Bone Joint Surg Am. 2002;84-A:171–177. doi: 10.2106/00004623-200202000-00002. [DOI] [PubMed] [Google Scholar]
- 6.Dorr LD, Takei GK, Conaty JP. Total hip arthroplasties in patients less than forty-five years old. J Bone Joint Surg Am. 1983;65:474–479. [PubMed] [Google Scholar]
- 7.Castro FP Jr, Barrack RL. Core decompression and conservative treatment for avascular necrosis of the femoral head: a meta-analysis. Am J Orthop (Belle Mead NJ) 2000;29:187–194. [PubMed] [Google Scholar]
- 8.Mont MA, Carbone JJ, Fairbank AC. Core decompression versus nonoperative management for osteonecrosis of the hip. Clin Orthop Relat Res. 1996:169–178. doi: 10.1097/00003086-199603000-00020. [DOI] [PubMed] [Google Scholar]
- 9.Rajagopal M, Balch Samora J, Ellis TJ. Efficacy of core decompression as treatment for osteonecrosis of the hip: a systematic review. Hip Int. 2012;22:489–493. doi: 10.5301/HIP.2012.9748. [DOI] [PubMed] [Google Scholar]
- 10.Lieberman JR, Engstrom SM, Meneghini RM, SooHoo NF. Which factors influence preservation of the osteonecrotic femoral head? Clin Orthop Relat Res. 2012;470:525–534. doi: 10.1007/s11999-011-2050-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Pritchett JW. Statin therapy decreases the risk of osteonecrosis in patients receiving steroids. Clin Orthop Relat Res. 2001:173–178. doi: 10.1097/00003086-200105000-00022. [DOI] [PubMed] [Google Scholar]
- 12.Wang GJ, Cui Q, Balian G. The Nicolas Andry award. The pathogenesis and prevention of steroid-induced osteonecrosis. Clin Orthop Relat Res. 2000:295–310. doi: 10.1097/00003086-200001000-00030. [DOI] [PubMed] [Google Scholar]
- 13.Wang Y, Yin L, Li Y, Liu P, Cui Q. Preventive effects of puerarin on alcohol-induced osteonecrosis. Clin Orthop Relat Res. 2008;466:1059–1067. doi: 10.1007/s11999-008-0178-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Glueck CJ, Freiberg RA, Sieve L, Wang P. Enoxaparin prevents progression of stages I and II osteonecrosis of the hip. Clin Orthop Relat Res. 2005:164–170. doi: 10.1097/01.blo.0000157539.67567.03. [DOI] [PubMed] [Google Scholar]
- 15.Jager M, Tillmann FP, Thornhill TS, Mahmoudi M, Blondin D, Hetzel GR, Zilkens C, Krauspe R. Rationale for prostaglandin I2 in bone marrow oedema--from theory to application. Arthritis Res Ther. 2008;10:R120. doi: 10.1186/ar2526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Disch AC, Matziolis G, Perka C. The management of necrosis-associated and idiopathic bone-marrow oedema of the proximal femur by intravenous iloprost. J Bone Joint Surg Br. 2005;87:560–564. doi: 10.1302/0301-620X.87B4.15658. [DOI] [PubMed] [Google Scholar]
- 17.Chen CH, Chang JK, Lai KA, Hou SM, Chang CH, Wang GJ. Alendronate in the prevention of collapse of the femoral head in nontraumatic osteonecrosis: a two-year multicenter, prospective, randomized, double-blind, placebo-controlled study. Arthritis Rheum. 2012;64:1572–1578. doi: 10.1002/art.33498. [DOI] [PubMed] [Google Scholar]
- 18.Agarwala S, Shah SB. Ten-year follow-up of avascular necrosis of femoral head treated with alendronate for 3 years. J Arthroplasty. 2011;26:1128–1134. doi: 10.1016/j.arth.2010.11.010. [DOI] [PubMed] [Google Scholar]
- 19.Agarwala S, Shah S, Joshi VR. The use of alendronate in the treatment of avascular necrosis of the femoral head: follow-up to eight years. J Bone Joint Surg Br. 2009;91:1013–1018. doi: 10.1302/0301-620X.91B8.21518. [DOI] [PubMed] [Google Scholar]
- 20.Nishii T, Sugano N, Miki H, Hashimoto J, Yoshikawa H. Does alendronate prevent collapse in osteonecrosis of the femoral head? Clin Orthop Relat Res. 2006;443:273–279. doi: 10.1097/01.blo.0000194078.32776.31. [DOI] [PubMed] [Google Scholar]
- 21.Lai KA, Shen WJ, Yang CY, Shao CJ, Hsu JT, Lin RM. The use of alendronate to prevent early collapse of the femoral head in patients with nontraumatic osteonecrosis. A randomized clinical study. J Bone Joint Surg Am. 2005;87:2155–2159. doi: 10.2106/JBJS.D.02959. [DOI] [PubMed] [Google Scholar]
- 22.Agarwala S, Jain D, Joshi VR, Sule A. Efficacy of alendronate, a bisphosphonate, in the treatment of AVN of the hip. A prospective open-label study. Rheumatology (Oxford) 2005;44:352–359. doi: 10.1093/rheumatology/keh481. [DOI] [PubMed] [Google Scholar]
- 23.Agarwala S, Sule A, Pai BU, Joshi VR. Alendronate in the treatment of avascular necrosis of the hip. Rheumatology (Oxford) 2002;41:346–347. doi: 10.1093/rheumatology/41.3.346-a. [DOI] [PubMed] [Google Scholar]
- 24.Young ML, Little DG, Kim HK. Evidence for using bisphosphonate to treat Legg-Calve-Perthes disease. Clin Orthop Relat Res. 2012;470:2462–2475. doi: 10.1007/s11999-011-2240-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Cardozo JB, Andrade DM, Santiago MB. The use of bisphosphonate in the treatment of avascular necrosis: a systematic review. Clin Rheumatol. 2008;27:685–688. doi: 10.1007/s10067-008-0861-9. [DOI] [PubMed] [Google Scholar]
- 26.Chen SQ SB-G, Cai YJ, Zhou HM, Qin J. Clinical efficacy of alendronate treatment of early-stage adult nontraumatic avascular necrosis of femoral head. Chinese Journal of Geriatrics. 2011;30:661–663. [Google Scholar]
- 27.Vulpiani MC, Vetrano M, Trischitta D, Scarcello L, Chizzi F, Argento G, Saraceni VM, Maffulli N, Ferretti A. Extracorporeal shock wave therapy in early osteonecrosis of the femoral head: prospective clinical study with long-term follow-up. Arch Orthop Trauma Surg. 2012;132:499–508. doi: 10.1007/s00402-011-1444-9. [DOI] [PubMed] [Google Scholar]
- 28.Hausdorf J, Lutz A, Mayer-Wagner S, Birkenmaier C, Jansson V, Maier M. Shock wave therapy for femoral head necrosis-Pressure measurements inside the femoral head. J Biomech. 2010;43:2065–2069. doi: 10.1016/j.jbiomech.2010.04.009. [DOI] [PubMed] [Google Scholar]
- 29.Ludwig J, Lauber S, Lauber HJ, Dreisilker U, Raedel R, Hotzinger H. High-energy shock wave treatment of femoral head necrosis in adults. Clin Orthop Relat Res. 2001:119–126. doi: 10.1097/00003086-200106000-00016. [DOI] [PubMed] [Google Scholar]
- 30.Ishida M, Fujioka M, Takahashi KA, Arai Y, Kubo T. Electromagnetic fields: a novel prophylaxis for steroid-induced osteonecrosis. Clin Orthop Relat Res. 2008;466:1068–1073. doi: 10.1007/s11999-008-0182-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Seber S, Omeroglu H, Cetinkanat H, Kose N. [The efficacy of pulsed electromagnetic fields used alone in the treatment of femoral head osteonecrosis: a report of two cases] . Acta Orthop Traumatol Turc. 2003;37:410–413. [PubMed] [Google Scholar]
- 32.Harrison MH, Bassett CA. The results of a double-blind trial of pulsed electromagnetic frequency in the treatment of Perthes’ disease. J Pediatr Orthop. 1997;17:264–265. doi: 10.1097/00004694-199703000-00022. [DOI] [PubMed] [Google Scholar]
- 33.Phillips Bob DS, Chris B, Badenoch D, Straus S, Haynes B, Dawes M. Oxford Centre for Evidence-based Medicine - Levels of Evidence (March 2009) 2009 [Google Scholar]
- 34.Higgins JPT, Green S Cochrane Collaboration. Cochrane handbook for systematic reviews of interventions. Chichester, England; Hoboken, NJ: Wiley-Blackwell; 2008. [Google Scholar]
- 35.Mont MA, Marulanda GA, Jones LC, Saleh KJ, Gordon N, Hungerford DS, Steinberg ME. Systematic analysis of classification systems for osteonecrosis of the femoral head. J Bone Joint Surg Am. 2006;88(Suppl 3):16–26. doi: 10.2106/JBJS.F.00457. [DOI] [PubMed] [Google Scholar]
- 36.Baujat B, Mahe C, Pignon JP, Hill C. A graphical method for exploring heterogeneity in meta-analyses: application to a meta-analysis of 65 trials. Stat Med. 2002;21:2641–2652. doi: 10.1002/sim.1221. [DOI] [PubMed] [Google Scholar]
- 37.Robinson HJ SJ Jr. Success of core decompression in the management of early stages of avascular necrosis: A four-year prospective study. Orthop Trans. 1992-1993:707. [Google Scholar]
- 38.Neumayr LD, Aguilar C, Earles AN, Jergesen HE, Haberkern CM, Kammen BF, Nancarrow PA, Padua E, Milet M, Stulberg BN, Williams RA, Orringer EP, Graber N, Robertson SM, Vichinsky EP. Physical therapy alone compared with core decompression and physical therapy for femoral head osteonecrosis in sickle cell disease. Results of a multicenter study at a mean of three years after treatment. J Bone Joint Surg Am. 2006;88:2573–2582. doi: 10.2106/JBJS.E.01454. [DOI] [PubMed] [Google Scholar]
- 39.Stulberg BN, Davis AW, Bauer TW, Levine M, Easley K. Osteonecrosis of the femoral head. A prospective randomized treatment protocol. Clin Orthop Relat Res. 1991:140–151. [PubMed] [Google Scholar]
- 40.Wang CJ, Wang FS, Huang CC, Yang KD, Weng LH, Huang HY. Treatment for osteonecrosis of the femoral head: comparison of extracorporeal shock waves with core decompression and bone-grafting. J Bone Joint Surg Am. 2005;87:2380–2387. doi: 10.2106/JBJS.E.00174. [DOI] [PubMed] [Google Scholar]
- 41.Koo KH, Kim R, Ko GH, Song HR, Jeong ST, Cho SH. Preventing collapse in early osteonecrosis of the femoral head. A randomised clinical trial of core decompression. J Bone Joint Surg Br. 1995;77:870–874. [PubMed] [Google Scholar]
- 42.Aaron RK, Lennox D, Bunce GE, Ebert T. The conservative treatment of osteonecrosis of the femoral head. A comparison of core decompression and pulsing electromagnetic fields. Clin Orthop Relat Res. 1989:209–218. [PubMed] [Google Scholar]
- 43.Wang C, Peng J, Lu S. Summary of the various treatments for osteonecrosis of the femoral head by mechanism: A review. Exp Ther Med. 2014;8:700–706. doi: 10.3892/etm.2014.1811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Sen RK. Management of avascular necrosis of femoral head at pre-collapse stage. Indian J Orthop. 2009;43:6–16. doi: 10.4103/0019-5413.45318. [DOI] [PMC free article] [PubMed] [Google Scholar]