

Abstract
Purpose:
To evaluate ultrasonographic accuracy in the differentiation of a bezoar from feces in a small bowel obstruction showing feces-like material just proximal to the transitional zone in abdominal computed tomography (CT).
Methods:
This study included 14 patients who showed feces-like material just proximal to the transitional zone, among 302 patients diagnosed with small bowel obstruction on abdominal CT. The diagnostic signs of a bezoar on ultrasonography included an arc-like surfaced intraluminal mass, posterior acoustic shadow and twinkling artifacts. The diagnostic performance of ultrasonography in each patient was compared with a final diagnosis that was surgically or clinically made.
Results:
Among the 14 patients, seven were ultrasonographically diagnosed as having a bezoar, and five of the seven were surgically diagnosed as having a phytobezoar. The remaining two of the seven showed complete symptomatic improvement before surgery. The other seven patients were ultrasonographically diagnosed as not having a bezoar. Among them, six patients were conservatively treated with symptomatic improvement, suggesting the absence of a bezoar. The remaining one patient was confirmed not to have a bezoar during adhesiolysis. In all patients, the ultrasonographic diagnosis agreed with the clinically confirmed diagnosis.
Conclusion:
Ultrasonography might be an accurate method for the differential diagnosis of feces-like material just proximal to the transitional zone in abdominal CT. It can help radiologists to quickly and easily diagnose a bezoar.
Keywords: Ultrasonography; Bezoars; Intestinal obstruction; Intestine, small
Introduction
A bezoar is a rare cause of small bowel obstruction, accounting for 2%-4% of small bowel obstruction cases [1]. However, the diagnosis of a bezoar as a cause of small bowel obstruction is important for clinicians because bezoar-induced obstruction seldom improves with conservative treatment, and early surgical intervention is practically required [2]. Until now, computed tomography (CT) has exhibited a superior diagnostic accuracy in evaluating the cause of small bowel obstruction [3]. A small-bowel bezoar presents itself as a well-defined, oval, feces-like material (intraluminal mottled gas-patterned mass) with a dilated proximal small-bowel loop [4]. However, other causes of small bowel obstruction, such as adhesion, can show similar findings that mimic a bezoar when localized. Therefore, it is difficult to completely differentiate a bezoar from feces only by CT, although several CT techniques, such as floating fat-density debris signs, exist to differentiate between them [5]. Usually, CT diagnosis is not definitive enough to confirm the diagnosis of a bezoar [5]. There are also many difficult cases that may confuse a radiologist as they show findings of both a bezoar and feces.
Until now, characteristic findings for a bezoar on ultrasonography (US), such as a hyper-echoic, arc-like surfaced mass with a posterior acoustic shadow having a twinkling artifact at the front of the mass, have been reported by previous studies [6]. Although several cases of bezoar-induced small bowel obstructions have been reported, no study has yet evaluated a secondary ultrasonogram performed after a CT scan to diagnose bezoar-induced small bowel obstruction [7,8].
The aim of our study is to evaluate the accuracy and efficacy of US in the differentiation of a bezoar from feces in the case of small bowel obstruction, showing feces-like material just proximal to the transitional zone in a primary abdominal CT scan, which confuses radiologists with respect to the accurate diagnosis of a bezoar.
Materials and Methods
Our Institutional Review Board approved this study, and the study required neither patient approval nor informed consent.
Patients
Between March 2008 and June 2014, 14 patients (6 males and 8 females; mean age, 60 years; age, 37 to 98 years) who were suspicious of bezoar-induced small bowel obstruction following a primary CT scan at our institution’s emergency department were selected among 302 patients having small bowel obstruction. We prospectively performed US on these 14 patients, and their charts were retrospectively reviewed. Old age was defined as 65 years or above according to convention.
Image Evaluation and Diagnostic Strategies for Lesions
All CT scans were performed on a multi-detector CT scanner (SOMATOM Definition and SOMATOM Definition AS+, Siemens Medical Solution, Forchheim, Germany). CT findings that suggested bezoar-induced small bowel obstruction were defined as those satisfy the following criteria: (1) dilated small-bowel lumen filled with mottled gas-patterned, feces-like material just proximal to the transitional zone; (2) no evidence of mural thickening or mass lesion at the transitional zone; (3) collapsed bowel loop, distal to the transitional zone; and (4) presence or absence of evidence of ascites.
In these patients, all secondary ultrasound examinations were performed with a 5-12-MHz transducer and an IU 22 unit (Philips Medical Systems, Bothell, WA, USA). US was performed by one gastrointestinal radiologist with 19 years of experience. US was performed within 24 hours (range, 1 to 24 hours) after the CT scan. Indirect US findings for small bowel obstruction were determined as a dilated small-bowel loop with increased bowel motility, and ascites. Confirmatory findings that suggested a bezoar included an arc-like surfaced intraluminal mass, a strong posterior acoustic shadow of the mass and a twinkling artifact in front of the mass. In patients who underwent US before 2014, the presence or absence of color Doppler twinkling artifacts was not evaluated. A bezoar was diagnosed on US when the lesion showed more than two of the abovementioned confirmatory findings.
The standard for diagnostic confirmation was set in two ways: surgical intervention for patients who were suspected of having a bezoar after US and conservative management for the others. The latter group was assumed to be free from bezoars when symptomatic improvement occurred spontaneously.
Results
Average 71 seconds (range, 22 to 150 seconds) were taken to find a diagnostic lesion for the differential diagnosis. Among the 14 patients, seven showed US findings compatible with bezoar-induced small bowel obstruction. Five of these patients were confirmed as having a phytobezoar following surgical and pathological confirmations. The patients underwent two types of surgical intervention for the removal of the bezoar: (1) fragmentation and milking out and (2) extraction via enterotomy.
Two patients who showed compatible findings for a bezoar, showed complete symptomatic improvement before surgical intervention and, therefore, did not undergo surgical intervention, and their follow-up US showed that bezoar-suspicious lesion had disappeared. Both these patients had a lesion in the terminal or distal ileum, and the bezoar, as estimated by US, was about 3.0 cm and 3.2 cm in diameter, respectively.
The other seven patients who showed no compatible findings for a bezoar underwent conservative management, and except for one patient, they all showed symptomatic improvement. The absence of a bezoar was confirmed in the remaining patient during adhesiolysis.
All cases of bezoars showed US findings of an arc-like surfaced intraluminal mass with a strong acoustic shadow and all cases, since 2014, showed a twinkling artifact generated from the mass; all the lesions were proven to be bezoars (Fig. 1). The other cases did not show these findings and instead had dirty posterior enhancement or moving intraluminal mass contents (Fig. 2).
Fig. 1. An 85-year-old man with bezoar-induced small bowel obstruction.
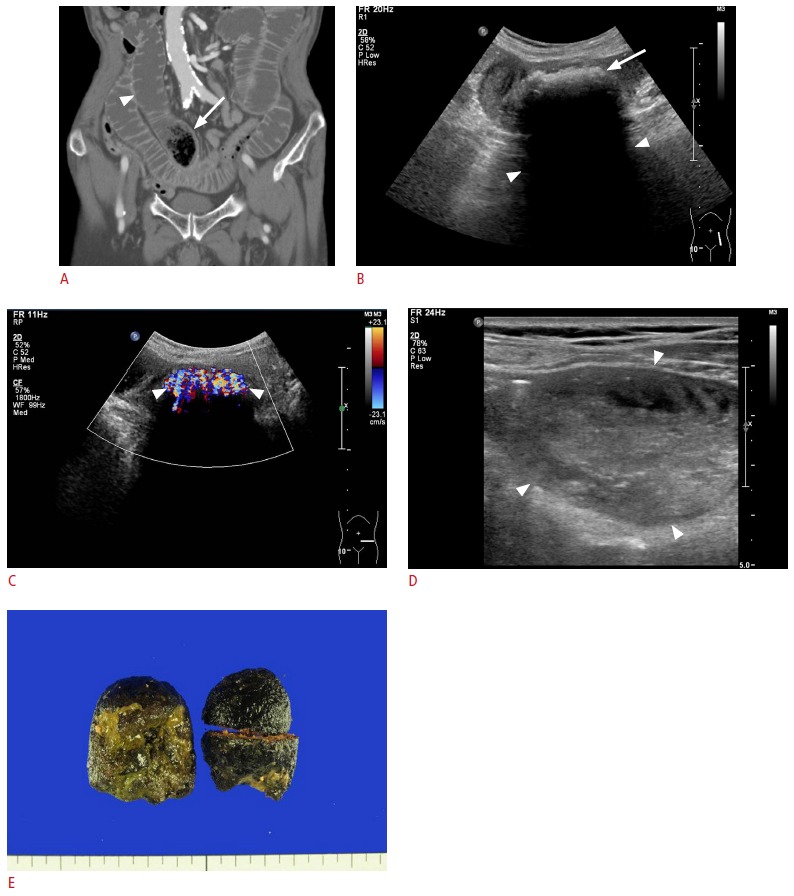
A. Computed tomography shows a mottled gas-patterned intraluminal mass (arrow) suspicious of a bezoar just proximal to the transitional zone of the ileum with the dilated small bowel in front (arrowhead). B. Gray-scale sonogram shows an arc-like surfaced intraluminal mass (arrow) with a strong posterior acoustic shadow (arrowheads). This mass was confirmed as a bezoar after surgery. C. Color Doppler sonogram shows a prominent twinkling artifact (arrowheads) in front of the intraluminal mass. D. Dilated lumen is filled with feces (arrowheads) at the proximal portion of the small-bowel loop. E. The photograph shows the phytobezoar extracted via enterotomy.
Fig. 2. A 49-year-old woman with small bowel obstruction.
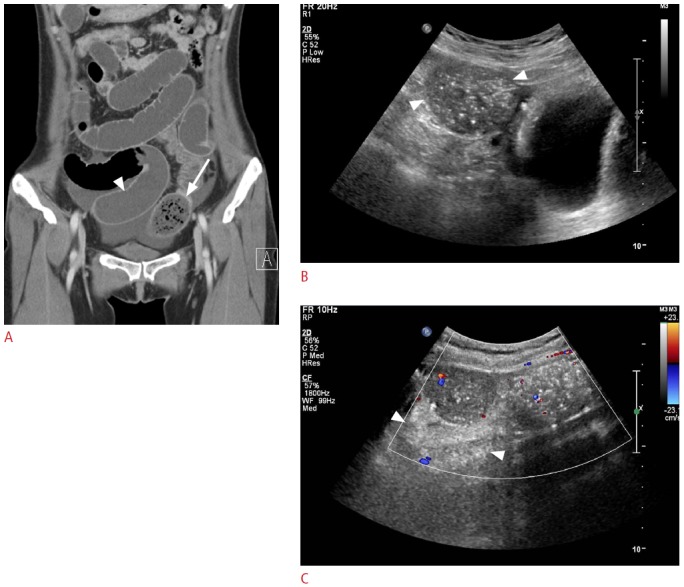
A. Computed tomography (CT) shows a mottled gas-patterned intraluminal mass (arrow) suspicious of a bezoar just proximal to the transitional zone of the ileum with the dilated small bowel in front (arrowhead), which is similar to the findings shown in Fig. 1A. This lesion was clinically diagnosed as feces after spontaneous symptomatic improvement. B. Gray-scale sonogram shows no posterior acoustic shadow or arc-like surfaced mass at the site of lesion corresponding to CT (arrowheads). C. Color Doppler sonogram shows no twinkling around the lesion. Posterior acoustic enhancement (arrowheads) is observed behind the mass-like lesion.
Among the five bezoar-confirmed patients, except one patient, all had one or more risk factors of bezoars, such as old age, a history of gastric surgery, and/or diabetes. Further, one of the two patients who showed compatible US findings for a bezoar (not surgically confirmed), had bezoar risk factors of old age and diabetes (Table 1).
Table 1.
Profile of 14 patients and US findings
| Patient No. | Sex | Age (yr) | Risk factor of bezoar | History of operation | Confirm method | Final diagnosis | Location and US findings |
||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Location (on CT) | Size (Ф, cm) | Configuration | Posterior imaging artifact | Twinkling artifact | |||||||
| 1 | M | 44 | No | No | Surgical | Bezoar | Distal ileum | 3.7 | Arc-like surfaced mass | Acoustic shadow | Unchecked |
| 2 | F | 98 | Old age | No | Surgical | Bezoar | Jejunum | 2.9 | Arc-like surfaced mass | Acoustic shadow | Yes |
| 3 | M | 85 | Old age | Yes | Surgical | Bezoar | Distal jejunum | 4.0 | Arc-like surfaced mass | Acoustic shadow | Yes |
| 4 | M | 66 | DM, old age | No | Surgical | Bezoar | Terminal ileum | 2.9 | Arc-like surfaced mass | Acoustic shadow | Unchecked |
| 5 | F | 81 | Gastric surgery, old age | Yes | Surgical | Bezoar | Distal jejunum | 5.0 | Arc-like surfaced mass | Acoustic shadow | Unchecked |
| 6 | M | 70 | DM, old age | No | Clinical | Bezoar | Terminal ileum | 3.0 | Arc-like surfaced mass | Acoustic shadow | Unchecked |
| 7 | M | 50 | No | No | Clinical | Bezoar | Distal ileum | 3.2 | Arc-like surfaced mass | Acoustic shadow | Unchecked |
| 8 | F | 37 | No | No | Clinical | Ileus | Distal ileum | Unmeasurable | Mottled substance | No | Unchecked |
| 9 | M | 54 | No | Yes | Surgical | Adhesive ileus | Jejunum | Unmeasurable | Mottled substance | No | Unchecked |
| 10 | F | 50 | DM | No | Clinical | Ileus | Ileum | Unmeasurable | Mottled substance | No | Unchecked |
| 11 | F | 49 | No | No | Clinical | Ileus | Distal ileum | Unmeasurable | Mottled substance | Acoustic enhancement | Unchecked |
| 12 | F | 54 | DM | Yes | Clinical | Ileus | Ileum | Unmeasurable | Mottled substance | Acoustic enhancement | No |
| 13 | F | 49 | No | No | Clinical | Ileus | Ileum | Unmeasurable | Mottled substance | No | Unchecked |
| 14 | F | 48 | No | No | Clinical | Ileus | Ileum | Unmeasurable | Mottled substance | Acoustic enhancement | No |
US, ultrasonography; CT, computed tomography; DM, diabetes mellitus.
Discussion
A bezoar, which is a mass found trapped in the gastrointestinal system, is one of the rare causes of small bowel obstruction [1]. Its contents vary from ingestible food material to hair. It is characterized by its hardness and mass formation. A bezoar has various risk factors for its development, such as history of gastric surgery, consumption of persimmons, old age, and diabetes mellitus [9]. Five of our patients among seven had at least one of these risk factors, and this was in line with a previous study [9]. Further, most of our patients were of relatively old age. This suggests that radiologists need to know patient history and consider the presence of a bezoar more carefully when the patient has one of the abovementioned risk factors.
The purpose of this study was to differentiate feces-like material just proximal to the transitional zone from a bezoar in small bowel obstruction. This study was conducted to solve the diagnostic dilemma of insufficient accuracy by a single modality study using only CT. Until now, the primary diagnostic imaging method of a bezoar and small bowel obstruction has been CT [3]. However, a single-modality study is not definitive enough when bezoars and small bowel obstruction are intermingled. This is the reason we selected patients who showed feces-like material just proximal to the transitional zone in small bowel obstruction. This confuses radiologists in terms of whether the observed mass is a bezoar or feces. We used a two-step examination of a primary CT scan and a secondary US follow-up for patients who were suspected of having a bezoar-induced small bowel obstruction.
In our study, the radiological diagnosis after the ultrasound agreed with the surgical and pathological confirmations. The negative findings were clinically and surgically confirmed. This suggests that secondary US can serve a supplementary clues to distinguish feces-like material in terms of whether it is a bezoar or feces. This outcome might be because of the ultrasound’s sensitivity to the hardness of a bezoar and the real-time observation of the lesion obstructing the bowel movement. When faced with a single-modality examination, it is not easy to diagnose the cause of small bowel obstruction only by ultrasound or to differentiate a bezoar from small-bowel feces only by CT. However, when CT and US are performed in sequence, each modality compensates for the other’s diagnostic weaknesses.
Kim et al. [6] reported some cases of a small-bowel bezoar with a positive twinkling artifact. We confirmed this and also confirmed that a fecal lesion shows neither a posterior shadow nor twinkling artifacts. Twinkling artifacts are observed as a rapidly changing colored noise on color Doppler and in a highly reflecting and rough-surfaced structure. Fecal material has relatively soft and movable features compared with a bezoar, as it cannot produce a rough surface to show twinkling artifacts and high acoustic impedance differences with the internal structure to show posterior acoustic shadows. Therefore, our results show that the shape of the mass can provide a radiological diagnosis.
Further, some minor findings such as dilated small-bowel loop, ascites or bowel wall movement at the transitional zone can be helpful in differentiating a suspicious lesion. If the surface of the suspicious mass-like lesion is movable or compressed easily, the lesion is far from a bezoar.
Additionally, the two patients in our case study who were diagnosed on US as having bezoar-induced small bowel obstruction but showed symptomatic improvement without surgical intervention provide some clues about treatment of bezoars. They each had a bezoar with a diameter of about 3.0 cm at the terminal or distal ileum. When patients show such findings, we can expect a spontaneous distal migration upon short-term follow-up of the bezoar.
With these results in mind, we propose a diagnostic flow for bezoar-induced small bowel obstruction. For patients who are suspicious of bezoar-induced small bowel obstruction following a CT scan, a radiologist needs to perform secondary US upon completion of the CT scan. If the lesion shows the findings of a strong posterior acoustic shadow, twinkling artifact, and arc-like surfaced mass, the radiologist can confirm it as a bezoar. Further, when the bezoar is located in the terminal ileum and is relatively small in size (grossly less than 3 cm), the radiologist can recommend observation and follow-up US of the lesion to a surgeon according to the patient condition.
This study has several limitations. First, the number of cases of bezoar-induced small bowel obstruction was relatively small. A further study with a greater number of cases is required. Second, we observed a twinkling artifact, which is one of the major US findings for a bezoar, only in patients who underwent US since 2014. Third, the diagnosis of two of patients who were considered to have bezoar-induced small bowel obstruction in the final clinical diagnosis was not confirmed on a surgical and pathological basis.
In conclusion, although bezoar-induced small bowel obstruction is a rare type of small bowel obstruction, when the bezoar cannot be differentiated by a CT scan alone, adding an ultrasound can provide an accurate diagnosis and suggest treatment options to clinicians.
Acknowledgments
This study was supported in part by the Research Fund of the Korean Society of Ultrasound in Medicine.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Salemis NS, Panagiotopoulos N, Sdoukos N, Niakas E. Acute surgical abdomen due to phytobezoar-induced ileal obstruction. J Emerg Med. 2013;44:e21–e23. doi: 10.1016/j.jemermed.2011.06.059. [DOI] [PubMed] [Google Scholar]
- 2.Dirican A, Unal B, Tatli F, Sofotli I, Ozgor D, Piskin T, et al. Surgical treatment of phytobezoars causes acute small intestinal obstruction. Bratisl Lek Listy. 2009;110:158–161. [PubMed] [Google Scholar]
- 3.Boudiaf M, Soyer P, Terem C, Pelage JP, Maissiat E, Rymer R. Ct evaluation of small bowel obstruction. Radiographics. 2001;21:613–624. doi: 10.1148/radiographics.21.3.g01ma03613. [DOI] [PubMed] [Google Scholar]
- 4.Ripolles T, Garcia-Aguayo J, Martinez MJ, Gil P. Gastrointestinal bezoars: sonographic and CT characteristics. AJR Am J Roentgenol. 2001;177:65–69. doi: 10.2214/ajr.177.1.1770065. [DOI] [PubMed] [Google Scholar]
- 5.Delabrousse E, Lubrano J, Sailley N, Aubry S, Mantion GA, Kastler BA. Small-bowel bezoar versus small-bowel feces: CT evaluation. AJR Am J Roentgenol. 2008;191:1465–1468. doi: 10.2214/AJR.07.4004. [DOI] [PubMed] [Google Scholar]
- 6.Kim HC, Yang DM, Kim SW, Park SJ, Ryu JK. Color Doppler twinkling artifacts in small-bowel bezoars. J Ultrasound Med. 2012;31:793–797. doi: 10.7863/jum.2012.31.5.793. [DOI] [PubMed] [Google Scholar]
- 7.Oh SH, Namgung H, Park MH, Park DG. Bezoar-induced small bowel obstruction. J Korean Soc Coloproctol. 2012;28:89–93. doi: 10.3393/jksc.2012.28.2.89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bae KS, Jeon KN, Ryeom HK. Bezoar associated with small bowel obstruction: comparison of CT and US. J Korean Radiol Soc. 2003;48:53–58. [Google Scholar]
- 9.Kement M, Ozlem N, Colak E, Kesmer S, Gezen C, Vural S. Synergistic effect of multiple predisposing risk factors on the development of bezoars. World J Gastroenterol. 2012;18:960–964. doi: 10.3748/wjg.v18.i9.960. [DOI] [PMC free article] [PubMed] [Google Scholar]