

Abstract
Purpose
To evaluate whether a culturally appropriate campaign using “Black radio” and print media increased awareness and utilization of local mammography screening services provided by the Centers for Disease Control and Prevention’s National Breast and Cervical Cancer Early Detection Program among African American women.
Methods
The evaluation used a quasi-experimental design involving data collection during and after campaign implementation in two intervention sites in GA (Savannah with radio and print media and Macon with radio only) and one comparison site (Columbus, GA). We used descriptive statistics to compare mammography uptake for African American women during the initial months of the campaign (8/08–1/09) with the latter months (2/09–8/09) and a post-campaign (9/09–12/09) period in each of the study sites. Comparisons of monthly mammogram uptake between cities were performed with multinomial logistic regression. We assumed a p value <0.05 to be significant.
Results
We observed an increase of 46 and 20 % in Savannah and Macon, respectively, from the initial period of the campaign to the later period. However, the increase did not persist in the post-campaign period. Analysis comparing monthly mammogram uptake in Savannah and Macon with Columbus showed a significant increase in uptake from the first to the second period in Savannah only (OR 1.269, 95 % CI (1.005–1.602), p = 0.0449).
Conclusions
Dissemination of health promotion messages via a culturally appropriate, multicomponent campaign using Black radio and print media was effective in increasing mammogram uptake in Savannah among low-income, African American women. Additional research is needed to quantify the relative contribution of campaign radio, print media, and community components to sustain increased mammography uptake.
Keywords: African American, Breast cancer, Campaign, Evaluation, Mammography
Introduction
Widespread mammography screening, detection at earlier stage, and improved therapies have resulted in declining breast cancer mortality rates [1]. Yet African American women continue to suffer disproportionate mortality [2, 3] at any stage of diagnosis. Breast cancer deaths among African American women have declined much more slowly, in part, due to late-stage diagnoses and delayed treatment resulting in a persistent disparity in mortality [4]. Although the use of mammography is comparable between African American and white women, women of lower income, uninsured status, or little education are least likely to have had a mammogram within recommended age and frequency guidelines [5]. Given their greater prevalence of late-stage diagnoses and higher mortality [6], timely and regular mammograms using culturally appropriate strategies for African American women are important [7, 8]. In particular, narratives from African American breast cancer survivors have been shown to improve mammography screening among African American women with low education [9].
The National Breast and Cervical Cancer Early Detection Program (NBCCEDP), administered by the Centers for Disease Control and Prevention (CDC), was authorized and implemented specifically to address issues of access to quality screening for low-income, uninsured women [10]. Grantees include all 50 states, the District of Columbia, five US territories, and 11 American Indian/Alaska Native organizations. Although the NBCCEDP has operated nationally for more than two decades, many eligible women are unaware of the availability of local screening services [11, 12].
In an effort to raise community awareness of local screening programs, combat excess breast cancer mortality rates, and help eliminate disparities in cancer outcomes among low-income, African American women, the CDC’s Division of Cancer Prevention and Control designed, implemented, and evaluated the African American Women and Mass Media (AAMM) pilot campaign [12, 13]. The AAMM campaign used Black radio, stations with broad African American listenership. According to Arbitron, about 92 % of Black consumers aged 12 years and over listen to the radio each week, which is a higher penetration rate than that of television, magazines, newspapers, or the Internet [14, 15]. Regardless of age, time of day, or location, Black consumers listen to radio making it a viable health communication channel. Additionally, because radio is an audio channel, it can circumvent the problems associated with low health literacy [15]. In an increasingly Internet-dependent society, Black radio can be accessed via Internet streaming, yet retains its programming, format, and engagement with community. The potential utility of Black radio to reach African American communities with public health messages has been previously discussed [15].
We hypothesized that the dissemination of culturally appropriate breast cancer awareness and screening promotion messages to low-income, African American women using the familiar channel of “Black radio” and placement of supplemental print media in community venues would increase awareness and utilization of local mammography screening services provided by the CDC NBCCEDP. This paper presents the results of an evaluation of a pilot campaign to examine its contribution to increased uptake in the number of mammograms provided through a local screening program [GA Breast and Cervical Cancer Program (BCCP)] among the target audience.
Methods
Campaign development
The formative evaluation and pilot campaign development activities have been previously described [13]. An earlier evaluation of the pilot campaign found that it was successful in reaching the target audience and increasing awareness of breast cancer and local screening services as measured by an increase in phone calls to the Cancer Information Service line, 1-800-4CANCER, by uninsured, African American women aged 40–64 in the study sites compared to the comparison location during the campaign implementation period [12]. Hall et al. also presented in this volume, outlines the theoretical underpinnings of the campaign and materials development and demonstrates our use of the Persuasive Health Message framework to design the campaign [16, 17].
Implementation
The AAMM was piloted in Savannah and Macon, GA with Columbus as a comparison site (Fig. 1). These cities were chosen as study sites because they had a similar demographic makeup, do not have any overlap in radio coverage, and had a similar ranking in the top 50 African American Metro Radio market rankings (Arbitron) at the time of study. In three phases, we first conducted a formative evaluation to understand low-income, uninsured African American women’s knowledge and awareness of breast cancer, screening and early detection, message, channel and source preferences. Second, qualitative methods (focus groups) were used to test culturally appropriate campaign concepts, messages, and advertisement-like materials [13]. Finally, an evaluation was conducted to assess the pilot campaign’s ability to increase community awareness of local screening services [12] and to contribute to an increase in utilization of mammography screening through the GABCCP.
Fig. 1.

Study catchment areas defined by specified zip codes in Savannah, Macon, and Columbus, Georgia and surrounding counties
Campaign activities were conducted over a 12-month period (from 8/08 through 7/09). A campaign kickoff reception occurred in Savannah in 7/08, and the airing of radio advertisements commenced in 8/08. Radio advertisements placed on Black radio stations were the primary delivery vehicle for the campaign and implemented in both intervention sites–Savannah and Macon, Georgia (Fig. 2). The development of campaign audio and print materials has been previously described [13].
Fig. 2.
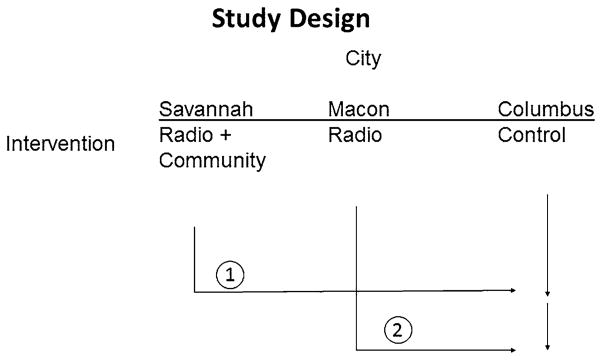
The African American Women and Mass Media (AAMM) campaign was implemented and evaluated in three Georgia cities. The full campaign (radio, print, community) was implemented in Savannah and a radio only component in Macon. Response in each location was compared against Columbus, a control site where no campaign activities were conducted
Four taped radio advertisements aired every month on Black radio stations during the pilot campaign. The radio advertisements were played in equal rotation each month during the campaign. Radio advertisements commonly aired Monday through Friday during morning drive time (6–10 a.m.), afternoon lunch hour (10 a.m.–3 p.m.), and evening drive time (3–7 p.m.); Saturday and Sunday radio spots aired anytime between 6 a.m. and 7 p.m., but normally played in the morning and late afternoon timeslots. The radio advertisements aired included three new 60-s spots developed exclusively for the pilot campaign, and a fourth previously developed State of Georgia radio advertisement. The three new AAMM radio advertisements featured a DJ, health care professional, and breast cancer survivor testimonial. The radio advertisements aired on two radio stations in Savannah and four stations in Macon to ensure that reach and frequency in each location was scheduled to yield similar exposure across sites. In addition to airing the 60-s radio advertisements, live radio shows (30 min to 1 h long) aired 4–5 times in intervention sites on Black radio stations during the Sunday morning public affairs programs (five live shows aired in Savannah; four live shows aired in Macon). The live radio shows featured a discussion between a health care provider and a community breast cancer survivor.
Print materials strategically placed in African American communities supplemented the radio advertising in Savannah, GA only. The materials were placed in a variety of venues throughout the African American community where women reported (during the formative evaluation) that they would notice and access health information (e.g., beauty salons, pharmacies). Print materials were also delivered to Cumulus Media, our partner radio station in Savannah, and several partner organizations in the community including the health department, Daniel’s Communication Group, and the African American Health Information and Resource Center for dissemination. These partners disseminated AAMM print materials at popular community events including street fairs and local community celebrations. Cumulus Media also conducted promotion and outreach activities throughout the campaign implementation including distribution of campaign materials during regular radio remote broadcasts and appearances in and around Savannah. The aim of all activities was to promote no- and low-cost mammogram services through the local GA BCCP to the target audience. Columbus, GA served as a comparison site where no campaign activities were conducted.
Evaluation design and analysis
A quasi-experimental design involving data collection during and after campaign implementation in two intervention sites and one comparison site facilitated a comparison of mammograms obtained by African American women in the intervention and comparison sites. This design allowed assessment of mammogram trends over three time periods including an early campaign period, a later period, and the period after the campaign ended. Collection of data on mammograms obtained in all sites started in 7/08 and continued 5 months beyond the end of the campaign. Data on numbers of mammograms received through the local BCCP were obtained from the Georgia Breast and Cervical Cancer Program, Georgia Department of Community Health (DCH). The DCH program collects data on demographic characteristics of participants, screening outcomes, and payment sources among other variables. Upon submission of a list of zip codes that defined our campaign catchment areas (Fig. 1), DCH provided mammogram data by month and site in selected zip codes, on age (<50, ≥50), race/ethnicity (Black, white, Hispanic, and Asian) of screened participants, and funding source for the mammogram.
Anticipating a delay in hearing or seeing our mass media campaign messages and subsequent behavioral action to obtain a mammogram among women exposed to the campaign, the first 6 months of the campaign (8/08–1/09) were regarded as a period where we expected to build women’s awareness and likely to see little change in mammograms obtained (Campaign period 1). The next 6 months of the pilot campaign (2/09–7/09) were regarded as the period where we expected a greater change in mammograms obtained among African American women. However, we added to this period an additional month (8/09) to allow mammograms scheduled in July to be completed (campaign period 2). Finally, a 4-month (9/09–12/09) post-campaign period (campaign period 3) was used to evaluate whether any increase was sustained. We hypothesized that an increase in mammograms in period 2 indicated that the increase was due, in part, to the existence of the pilot campaign in the community. Similar analyses were conducted for non-African American women to assess secular trends in each location.
In order to assess whether the campaign contributed to motivating women to get a mammogram through the GA BCCP, we calculated a percentage change in the average number of mammograms from periods 1 to 2 and periods 1 to 3 in each site. We also computed percentage change from period 2 to period 3 to examine sustainability of mammogram uptake after the campaign ended.
We used a multinomial logistic regression model (generalized logit) appropriate for modeling the association between a multicategory outcome and independent variables [18]. It uses simultaneous separate binary logit models for different pairs of a response category. Our model simultaneously describes the association between the periods (period 1 vs. 2, period 1 vs. 3, and period 2 vs. 3) and mammography uptake in the different cities (Savannah vs. Columbus and Macon vs. Columbus) for each race/ethnicity group. We assessed the association with the Wald Chi-square test. A p value <0.05 was considered statistically significant.
Results
Figure 3 presents the number of mammograms obtained by African American women through the local BCCP in the three campaign sites by month and period. The monthly number of mammograms in the first period ranged from 98 to 194 in Savannah, 48 to 65 in Macon, and 19 to 33 in Columbus. The monthly mammography uptake in period 2 ranged from 163 to 216 in Savannah, 61 to 85 in Macon, and 23 to 36 in Columbus. Monthly mammogram uptake in period 3 ranged from 128 to 177 in Savannah, 49 to 53 in Macon, and 17 to 36 in Columbus. Table 1 presents the results of mammography utilization among African American women in the three periods. The average number of mammograms in Savannah increased from 125 in period 1 to 183 in period 2. Macon had an increase from 59 to 71, and Columbus from 24 to 28. However, the monthly average dropped in period 3 to 150, 51, and 29 in Savannah, Macon, and Columbus, respectively. The percent change in the average number of mammograms obtained by African American women in each city, comparing periods 1 and 2, was 46.3, 20.2, and 15.3 %, respectively. However, there was a decrease in mammography uptake from periods 2 to 3 in both Savannah and Macon (data not shown). Percent change in mammography uptake among non-African American women in intervention cities ranged from 11.1 to 24.5 % from the first to second period and from 11.1 to 17.9 % from the first to the third period.
Fig. 3.

Monthly BCCP mammograms by African American women, by site, 7/2008–12/2009
Table 1.
Mammography uptake in the three periods of the study among African American and other (non-African American) women in Savannah, Macon, and Columbus, GA
| City | Race/ethnicity | Average number of mammograms
|
% change from P1 to P2b | % change from P1 to P3b | ||
|---|---|---|---|---|---|---|
| P1a | P2a | P3a | ||||
| Savannah (radio and print material) | AA | 125.2 | 183.1 | 150.2 | 46.3 | 20.0 |
| Other | 126.0 | 140.0 | 140.0 | 11.1 | 11.1 | |
| Macon (radio only) | AA | 59.2 | 71.1 | 50.7 | 20.2 | −14.2 |
| Other | 33.5 | 41.7 | 39.5 | 24.5 | 17.9 | |
| Columbus (comparison site) | AA | 24.2 | 27.9 | 28.5 | 15.3 | 17.9 |
| Other | 12.0 | 13.1 | 13.0 | 9.5 | 8.3 | |
P1 = period 1 (8/08–1/09); P2 = period 2 (2/09–8/09); P3 = period 3 (9/09–12/09)
AA African American
Monthly average of mammograms across a specified period. Averages are rounded to one decimal
Percent change (increase or decrease) relative to P1, eg., (P2–P1)/P1
To determine whether the Savannah campaign had a differential effect by age, an additional examination of the change in average mammography uptake among African American women between the first two periods for each age group (<50 years and ≥50 years, Fig. 4) revealed that younger women in Savannah had an increase in average number of mammograms from 53 to 78 (percentage change of 46.5 %) and the older group from 72 to 105 (percentage change of 46.2 %).
Fig. 4.

Total BCCP mammograms by African American women in Savannah, by month, and age (<50 vs. 50+)
Results from the multinomial regression analysis comparing mammography uptake in the first and second periods of the campaign and the first and post-campaign (third) periods in Savannah and Macon each versus Columbus for African American and non-African American women are presented in Table 2. The effect of moving from the first period of the campaign to the second period resulted in a significant increase in mammography uptake among African American women in Savannah compared with the uptake in Columbus (OR 1.269, 95 % CI (1.005–1.602), p = 0.0449). However, no significant difference in mammography uptake was observed between the first period of the campaign and the post-campaign period. A comparison of mammography uptake between Macon and Columbus in the first and second periods of the campaign showed that the campaign had no effect on the uptake among African American women. However, comparing the first and post-campaign periods revealed that Macon was less likely to sustain mammography uptake than Columbus (OR 0.73, 95 % CI (0.539–0.982), p = 0.0375). Additional results from the analyses comparing each of the two campaign cities with Columbus showed no significant difference in mammography uptake between the second period of the campaign and post-campaign in Savannah, but an odds ratio of 0.7 (95 % CI (0.525–0.925), p = 0.0125) in Macon. We did not observe any difference in mammography uptake between Savannah and Columbus and between Macon and Columbus for non-African American women during the campaign and post-campaign periods.
Table 2.
Odds ratio estimates of campaign effect on mammography uptake in the cities of Savannah and Macon compared with Columbus in the three campaign periods among African American and other (non-African American) women
| Race/ethnicity | City | Period | Point estimate (OR) | 95 % CI | p value |
|---|---|---|---|---|---|
| AA | Savannah versus Columbus | 2 versus 1 | 1.269 | (1.005–1.602) | 0.0449 |
| 3 versus 1 | 1.018 | (0.779–1.330) | 0.8968 | ||
| 3 versus 2 | 0.802 | (0.624–1.030) | 0.0842 | ||
| Macon versus Columbus | 2 versus 1 | 1.043 | (0.809–1.345) | 0.7450 | |
| 3 versus 1 | 0.727 | (0.539–0.982) | 0.0375 | ||
| 3 versus 2 | 0.697 | (0.525–0.925) | 0.0125 | ||
| Other | Savannah versus Columbus | 2 versus 1 | 1.014 | (0.735–1.401) | 0.9304 |
| 3 versus 1 | 1.026 | (0.706–1.489) | 0.8942 | ||
| 3 versus 2 | 1.011 | (0.709–1.443) | 0.9519 | ||
| Macon versus Columbus | 2 versus 1 | 1.137 | (0.796–1.625) | 0.4810 | |
| 3 versus 1 | 1.088 | (0.720–1.645) | 0.6877 | ||
| 3 versus 2 | 0.958 | (0.648–1.416) | 0.8281 |
P1 = period 1 (8/08–1/09); P2 = period 2 (2/09–8/09); P3 = period 3 (9/09–12/09)
AA African American
Discussion
The AAMM pilot campaign was conceived to increase public awareness and utilization of mammography screening services among African American women at the community level through radio, with or without other small media components, to assess whether it ultimately helps reduce cancer mortality disparities in low income or minority groups [8, 19]. After 1 year of implementation, as hypothesized, percent change in mammography uptake among African American women was higher in Savannah and Macon from period 1 to period 2 than that in Columbus. Thus, the goal of increasing the number of mammograms scheduled and obtained through the local BCCP by African American women was realized. However, after examining the effect of the campaign with multinomial regression modeling, controlling for screening in the comparison site, the campaign effect was only significant in Savannah. The increase in screening did not persist following the end of the campaign. We observed a sharp decrease from period 2 to period 3 in mammography uptake in Macon and less so in Savannah. The change in screening behavior argues for sustaining breast cancer screening messages year-round as opposed to the current October focus for Breast Cancer Awareness Month.
Black radio is an established communication channel that reaches a broad and diverse cross section of the African American community that includes African Americans, Haitians, Africans, and people from the Caribbean. Marketing studies indicate that African Americans, in particular, often listen to the radio at home, at work, in the car, in stores and restaurants, online, and on cell phones [14] making Black radio an attractive and valuable health communication resource to tap to reach African Americans with important health messages necessary to reduce health disparities in this population.
The increase in mammography uptake during the campaign period in Savannah suggests possible benefits of a campaign using radio as a multimedia component with culturally appropriate messages in diverse materials directed at low-income, African American women. This campaign used the images and voices of Black women (which resonated with the target audience), and a clear call to action by engaging breast cancer survivors to be the featured voice in the campaign’s radio spots as was suggested by respondents in the formative evaluation [12]. In a brief mid-campaign listener survey, respondents intimated that hearing the voices and stories of breast cancer survivors was important in motivating African American women to call the 1-800-4CANCER number, schedule, and ultimately obtain mammograms through the GA BCCP. These findings are consistent with other study findings that radio advertisements are effective media [20, 21].
A number of past studies have utilized, fielded, and evaluated radio as an element of multicomponent community-based efforts to improve cancer screening rates among underserved women [22–26]. These studies, which utilized intervention and comparison communities, observed an increase in self-reported mammography screening in the target audiences and reported intervention effects that ranged from 8 to 18 %, although some studies reported no intervention effect [27, 28]. In comparison, our data showed a 27 % increase in the odds of screening among our desired audience in Savannah compared with the odds of screening in Columbus. Additionally, no significant change was observed among groups of women not targeted.
A key strength of this campaign’s implementation is that study sites were geographically distinct. Sites were sufficiently separated so that there was no contamination of radio or print interventions (e.g., there was no airing of radio messages from the study sites in the comparison site). A second strength of the study is its use of a quasi-experimental, three-period design allowing us to evaluate the benefits of the intervention, detect secular trends in mammography utilization over time, and make comparisons between outcomes in sites exposed and unexposed to the pilot campaign to suggest campaign contribution. Finally, our evaluation used actual mammograms obtained as an outcome measure of mammography utilization rather than women’s self-reported receipt of screening or their intention to screen and avoids potential overreporting [29].
A key limitation of this evaluation is that due to HIPAA privacy regulations, the study team was unable to track individuals who responded to campaign materials through appointment setting and screening completion. Therefore, we cannot confirm that women who called the 1-800-4CANCER phone number, prominently featured on all AAMM pilot campaign materials, were those who later obtained screening in either campaign period. A second limitation is the possibility that there were other breast cancer awareness and mammography promotion activities in our study communities influencing an uptake in mammography utilization. The study team endeavored to offset this shortcoming by conducting regular environmental scans of breast cancer and mammography promotion campaigns and activities in the study sites; this included querying study site health departments on a monthly basis about breast cancer and/or mammography awareness activities in each community. Our environmental scan and discussions with health department staff did not yield any information about any breast cancer and mammography campaign or activities other than the expected activities during October’s Breast Cancer Awareness Month. Further, none of the health department staff reported any organized efforts to promote mammography utilization that targeted NBCCEDP-eligible African American women. In addition, any state or national campaigns would have affected all sites and would have been reflected in the screening trends observed in the comparison site. Third, print materials were used as a supplement to the primary radio focus in Savannah. As a result, our evaluation design did not capture information on print media alone, and we cannot quantify the relative impact of campaign radio and print components. Finally, given that radio messages are heard throughout African American communities, it is possible that the campaign motivated non-BCCP-eligible women to get mammograms which would suggest that the campaign widely contributed to an uptake in mammograms in the broader African American community. In fact health departments in our study sites reported that they received calls from ineligible women whose mammograms were paid through other funding sources or who were referred to other screening resources. However, our data collection activities did not capture data on mammograms performed outside of the NBCCEDP. In addition, it may have been possible for BCCP-eligible women to identify and receive a mammogram through screening services outside of the BCCP. In either scenario, estimates of the pilot campaign’s contribution to mammogram uptake in the community are likely conservative. Future studies of AAMM could be strengthened if we were able to track women from the time they call in response to campaign prompts, through appointment setting, and receipt of screening to show a direct link between campaign exposure and mammography uptake.
The increase in mammography utilization at the Savannah site reported during the study’s pilot campaign demonstrates that a culturally appropriate, multicomponent campaign promoting breast cancer awareness and utilization of low- and no-cost screening services for low-income, African American women, using Black radio as the primary channel for dissemination, contributed to an increase in mammography utilization among younger and older underserved African American women of screening age. Although the radio only campaign reached our target in Macon (11), its individual contribution to the overall campaign effectiveness remains uncertain, as previously noted (8). Few studies have successfully teased out the effect of a single component of a multicomponent campaign. Our results show that the AAMM pilot campaign can reach and promote breast cancer awareness and mammogram utilization with underserved audiences. Most importantly, our findings indicate that Black radio is an important communication channel in African American communities [30–32] and valuable, particularly when used in conjunction with other communication channels, to contribute to desired behavior change [33] and may impact elimination of cancer disparities in vulnerable populations. The approach, if scaled-up and sustained in communities, shows promise to motivate mammography usage and ultimately may be effective in contributing to a reduction in breast cancer disparities and mortality among low-income, African American women.
Acknowledgments
This work was supported in part by Centers for Disease Control and Prevention, Division of Cancer Prevention and Control (Contract No. 200-2002-00574 to ICF International).
Footnotes
The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Contributor Information
Ingrid J. Hall, Email: ihall@cdc.gov, Division of Cancer Prevention and Control, Centers for Disease Control and Prevention, 4770 Buford Highway, Atlanta, GA 30341, USA
Ashani Johnson-Turbes, ICF International, Atlanta, GA 30329, USA.
Zahava Berkowitz, Division of Cancer Prevention and Control, Centers for Disease Control and Prevention, 4770 Buford Highway, Atlanta, GA 30341, USA.
Yasmine Zavahir, Hollywood, Health and Society, Los Angeles, CA, USA.
References
- 1.Edwards BK, Noone AM, Mariotto AB, Simard EP, Boscoe FP, Henley SJ, Jemal A, Cho H, Anderson RN, Kohler BA, Eheman CR, Ward EM. Annual report to the nation on the status of cancer, 1975–2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer. 2014;120:1290–1314. doi: 10.1002/cncr.28509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Howlader N, Noone AM, Krapcho M, Garshell J, Miller D, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA, editors. SEER Cancer Statistics Review, 1975–2011. National Cancer Institute; Bethesda, MD: Apr, 2014. http://seer.cancer.gov/csr/1975_2011/, based on November 2013 SEER data submission, posted to the SEER web site. [Google Scholar]
- 3.Whitman S, Orsi J, Hurlbert M. The racial disparity in breast cancer mortality in the 25 largest cities in the United States. Cancer Epidemiol. 2012;36:147–151. doi: 10.1016/j.canep.2011.10.012. [DOI] [PubMed] [Google Scholar]
- 4.Hunt BR, Whitman S, Hurlbert MS. Increasing black: white disparities in breast cancer mortality in the 50 largest cities in the United States. Cancer Epidemiol. 2014;38:118–123. doi: 10.1016/j.canep.2013.09.009. [DOI] [PubMed] [Google Scholar]
- 5.Centers for Disease Control and Prevention (CDC) . Cancer screening—United States, 2010. MMWR Morb Mortal Wkly Rep. 2012;61:41–45. [PubMed] [Google Scholar]
- 6.Centers for Disease Control and Prevention (CDC) . Vital signs: racial disparities in breast cancer severity–United States, 2005–2009. MMWR Morb Mortal Wkly Rep. 2012;61:922–926. [PubMed] [Google Scholar]
- 7.Kreuter MW, Strecher VJ, Glassman BN. One size does not fit all: the case for tailoring print materials. Ann Behav Med. 1999;21:276–283. doi: 10.1007/BF02895958. [DOI] [PubMed] [Google Scholar]
- 8.Baron RC, Rimer BK, Breslow RA, Coates RJ, Kerner J, Melilo S, et al. Client-directed interventions to increase community demand for breast, cervical, and colorectal cancer screening a systematic review. Am J Prev Med. 2008;32:1784–1792. doi: 10.1016/j.amepre.2008.04.002. [DOI] [PubMed] [Google Scholar]
- 9.Kreuter MW, Holmes K, Alcaraz K, Kalesan B, Rath S, Richert M, McQueen A, Caito N, Robinson L, Clark EM. Comparing narrative and informational videos to increase mammography in low-income African American women. Patient Educ Couns. 2010;81(Suppl):S6–S14. doi: 10.1016/j.pec.2010.09.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.National Breast and Cervical Cancer Early Detection Program (NBCCEDP) [Accessed 12 May 2014]; http://www.cdc.gov/cancer/nbccedp/about.htm.
- 11.Parker DM. Georgia’s cancer awareness and education campaign: combining public health models and private sector communications strategies. [Accessed 13 May 2014];Prev Chronic Dis [serial online] 2004 Jul;2004 Available from: http://www.cdc.gov/pcd/issues/2004/jul/04_0030.htm. [PMC free article] [PubMed] [Google Scholar]
- 12.Hall IJ, Rim SH, Johnson-Turbes CA, Vanderpool R, Kamalu NN. The African American Women and Mass Media Campaign: a CDC breast cancer screening project. J Women’s Health. 2012;21:1107–1113. doi: 10.1089/jwh.2012.3903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Leeks KD, Hall IJ, Johnson-Turbes CA, Kamalu NK, Zavahir Y. Formative development of a culturally appropriate mammography screening campaign for low-income African-American women. J Health Dispar Res Pract. 2012;5:42–61. [Google Scholar]
- 14.Arbitron. Black Radio Today. [Accessed 12 May 2014];Executive summary. 2013 http://www.arbitron.com/downloads/Black_Radio_Today_2013_execsum.pdf.
- 15.Hall IJ, Johnson-Turbes CA, Williams KN. The potential of black radio to disseminate health messages and reduce disparities. Prev Chronic Dis. 2010;7(4):A87. [PMC free article] [PubMed] [Google Scholar]
- 16.Witte K. Fishing for success using the Persuasive Health Message Framework to generate effective campaign messages. In: Maibach E, Parrott RL, editors. Designing health messages: approaches from communication theory and public health practice. Sage; Thousand Oaks: 1994. [Google Scholar]
- 17.Hall IJ, Johnson-Turbes A. Use of the Persuasive Health Message Framework in Development of a Community-based Mammography Promotion Campaign. Canc Causes Control. 2015 doi: 10.1007/s10552-015-0537-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Stokes ME, Davis CS, Koch GG. Categorical data analysis using the SAS system. 2. SAS Institute Inc; Cary: 2000. [Google Scholar]
- 19.Sabatino SA, Lawrence B, Elder R, Mercer SL, Wilson KM, DeVinney B, Melillo S, Carvalho M, Taplin S, Bastani R, Rimer BK, Vernon SW, Melvin CL, Taylor V, Fernandez M, Glanz K Community Preventive Services Task Force . Effectiveness of interventions to increase screening for breast, cervical, and colorectal cancers: nine updated systematic reviews for the guide to community preventive services. Am J Prev Med. 2012;43:97–118. doi: 10.1016/j.amepre.2012.04.009. [DOI] [PubMed] [Google Scholar]
- 20.Farrelly MC, Hussin A, Bauer UE. Effectiveness and cost effectiveness of television, radio and print advertisements in promoting the New York smokers’ quitline. Tob Control. 2007;16(Suppl 1):i21–i23. doi: 10.1136/tc.2007.019984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bronar C, MA, Saul J., PhD NAQC. Increasing reach of tobacco cessation quitlines: a review of the literature and promising practices. Phoenix, AZ: 2009. [Google Scholar]
- 22.McAlister AL, Fernandez-Esquer ME, Ramirez AG, Trevino F, Gallion KJ, Villarreal R, Pulley LV, Hu S, Torres I, Zhang Q. Community level cancer control in a Texas barrio: part II–base-line and preliminary outcome findings. J Natl Cancer Inst Monogr. 1995;18:123–126. [PubMed] [Google Scholar]
- 23.Paskett ED, Tatum CM, D’Agostino R, Jr, Rushing J, Velez R, Michielutte R, Dignan M. Community-based interventions to improve breast and cervical cancer screening: results of the Forsyth county cancer screening (FoCaS) project. Cancer Epidemiol Biomarkers Prev. 1999;8:453–459. [PubMed] [Google Scholar]
- 24.Dignan M, Michielutte R, Wells HB, Bahnson J. The forsyth county cervical cancer prevention project—I. Cervical cancer screening for black women. Health Educ Res. 1994;9:411–420. doi: 10.1093/her/9.4.411. [DOI] [PubMed] [Google Scholar]
- 25.Fletcher SW, Harris RP, Gonzalez JJ, Degnan D, Lannin DR, Strecher VJ, Pilgrim C, Quade D, Earp JA, Clark RL. Increasing mammography utilization: a controlled study. J Natl Cancer Inst. 1993;85:112–120. doi: 10.1093/jnci/85.2.112. [DOI] [PubMed] [Google Scholar]
- 26.Blumenthal DS, Fort JG, Ahmed NU, Semenya KA, Schreiber GB, Perry S, Guillory J. Impact of a two-city community cancer prevention intervention on African Americans. J Natl Med Assoc. 2005;97:1479–1488. [PMC free article] [PubMed] [Google Scholar]
- 27.Suarez L, Roche RA, Pulley LV, Weiss NS, Goldman D, Simpson DM. Why a peer intervention program for Mexican-American women failed to modify the secular trend in cancer screening. Am J Prev Med. 1997;13:411–417. [PubMed] [Google Scholar]
- 28.Zapka JG, Costanza ME, Harris DR, Hosmer D, Stoddard A, Barth R, Gaw V. Impact of a breast cancer screening community intervention. Prev Med. 1993;22:34–53. doi: 10.1006/pmed.1993.1003. [DOI] [PubMed] [Google Scholar]
- 29.McPhee SJ, Nguyen TT, Shema AJ, Nguyen B, Somkin C, Vo P, Pasick R. Validation of recall of breast and cervical cancer screening by women in an ethnically diverse population. Prev Med. 2002;35:463–473. doi: 10.1006/pmed.2002.1096. [DOI] [PubMed] [Google Scholar]
- 30.Alexander J, Kwon HT, Strecher R, Bartholomew J. Multicultural media outreach: increasing cancer information coverage in minority communities. J Canc Educ. 2013;28:744–747. doi: 10.1007/s13187-013-0534-5. [DOI] [PubMed] [Google Scholar]
- 31.Stockton MB, McClanahan BS, Lanctot JQ, Klesges RC, Beech BM. Identification of facilitators and barriers to participation in weight gain prevention research by African American girls. Contemp Clin Trials. 2012;33:38–45. doi: 10.1016/j.cct.2011.08.010. [DOI] [PubMed] [Google Scholar]
- 32.Jedele JM, Ismail AI. Evaluation of a multifaceted social marketing campaign to increase awareness of and screening for oral cancer in African Americans. Community Dent Oral Epidemiol. 2010;38:371–382. doi: 10.1111/j.1600-0528.2010.00545.x. [DOI] [PubMed] [Google Scholar]
- 33.Kennedy MG, Genderson MW, Sepulveda AL, Garland SL, Wilson DB, Stith-Singleton R, Dubuque S. Increasing tobacco quitline calls from pregnant African American women: the “one tiny reason to quit” social marketing campaign. J Womens Health (Larchmt) 2013;22:432–438. doi: 10.1089/jwh.2012.3845. [DOI] [PMC free article] [PubMed] [Google Scholar]