

Abstract
Content
HIV infections continue to rise in a new generation of young, gay, bisexual and other men who have sex with men (YMSM) despite three decades of HIV prevention and recent biomedical technologies to deter infection.
Objectives
To examine the incidence of HIV and the demographics, behavioral, and structural factors associated with incident infections.
Design
Cohort study.
Participants
600 YMSM who were ages 18-19 at baseline.
Results
At baseline 6 prevalent cases of HIV were detected. Over the course of 36 months and six additional waves of data collection, we identified 43 (7.2%) incident cases of HIV. Incident infections were marginally higher among those residing in neighborhoods with higher rates of HIV prevalence. Using Cox proportional hazards models we detected that hazard ratios for time to HIV seroconversion were significantly higher for Black YMSM (HR = 7.46) and Mixed/Other race YMSM (HR = 7.99), and older age at sexual debut with another man was associated with a lower risk of HIV seroconversion (HR = 0.50), while low perceived familial SES was marginally associated with an increased risk for HIV seroconversion (HR = 2.45).
Conclusions
These findings support the disparities for HIV that exist within the population of sexual minority men and suggest that we attend to behavioral, structural and social conditions to effectively tailor HIV prevention for a new generation of YMSM with a keen eyes to the conditions faced by racial and ethnic minority YMSM which heightened their risk for acquiring HIV.
Keywords: HIV, incidence, gay and bisexual men, YMSM, cohort study, prevention
In the United States, gay, bisexual, and other sexual minority men represent approximately 2% of the general population,1 yet accounted for 63% of estimated incident HIV infections in 2010.2 Moreover, HIV infection rates are particularly high among young men who have sex with men (YMSM). In 2010, YMSM ages 13-24, accounted for 30% of all new infections among MSM and 72% of new infections within this age group.2 Moreover, between 2006-and 2009, YMSM ages 13–24 years had the greatest percentage increase in diagnosed HIV infections of all age groups.2 The burden of HIV is even more pronounced among Black and Hispanic YMSM.2,3 Among all MSM, 36% of new infections in 2010 were among Black men; furthermore, the majority of these infections (45%) occurred among those ages 13 to 24.2 Finally, Hispanic MSM accounted for 22% of new infections in 2010.2
Racial/ethnic disparities in HIV among YMSM have not been explained by differential engagement in sexual behaviors as a number of studies note that Black and Hispanic YMSM do not appear to engage in more or riskier sexual behaviors compared with their White peers.4-6 Recent investigations have considered a broader range of social and contextual determinants for their association with HIV risk among YMSM.6 For example, evidence suggests heightened levels of risk and HIV transmission in newly formed partnerships,7,8 and a higher likelihood of anal sex without condoms among YMSM in formed relationships.9 Additionally, earlier sexual debut, defined as sex before the age of 16, is associated with higher levels of risk behaviors in YMSM 10 and has been associated with the HIV/STI transmission,11; Black and Hispanic YMSM have been show to engage in anal sex without condoms at younger ages than Whites or Asian Pacific Islanders (APIs).6 Finally, socioeconomic status (SES), has been implicated in the spread of HIV in the U.S population.12 In YMSM, familial SES has been shown to be highly associated with anal sex without condoms,13 and SES has been proposed as mediating factor in explaining HIV in this population.14
Given this background in addition to the dearth of longitudinal studies among YMSM, the goal of the present study was to examine risk factors for incident HIV infection among of cohort of racially/ethnically and socioeconomically diverse YMSM.
Methods
Procedures and Participants
Data for this analysis were collected as part of a prospective cohort study of young men who have sex with men (YMSM) known locally as Project 18 (P18). Methods and details of the recruitment and enrollment procedures as well as the baseline study visit have been described in detail previously and are summarized here.9,13,15-19 Briefly, between June 2009 to May 2011, YMSM were recruited for enrollment into the P18 cohort study via both venue and internet-based strategies
At baseline, data were collected via detailed, structured interviews by trained personnel using standardized methods to ensure adherence to all study protocols. Participants provided information on sociodemographics, psychosocial characteristics and behavioral and social factors via audio-computer assisted self-interview (ACASI). Data on recent sexual behaviors were obtained using the Timeline Followback (TLFB) calendar-based measure, a semi-structured, interviewer-administered assessment designed to collect detailed information for the 30 days preceding each study visit.20,21 to report on sexual activity for each day during the past 30 days using a personalized calendar.
Bi-annual follow-up visits for the P18 study were scheduled at 6-, 12-, 18-, 24-, 30-, and 36-months post-baseline visit. For participants who remained in NYC metropolitan area for the entire duration of the cohort follow-up period, all follow-up visit activities included the same protocols and procedures as the baseline visit to ensure consistency of study protocol implementation across all visits. For participants who moved out of the NYC metropolitan region for some period of time during the course of the cohort study, a secure-site, online survey assessment was developed to allow participants to provide information collected in the ACASI assessment. Finally, as on-site HIV testing was not feasible with the sub-sample of participants who completed some or all assessments online, these participants were asked to report if they had been tested for HIV in the previous 3 months and had received their test results. HIV status verification for participants who completed an online assessment and self-reported an HIV seropositive status was conducted at the 36 month assessment. During this follow-up visit, all participants who tested positive (at the P18 site) or self-reported an HIV positive status online were asked to provide details on their HIV treatment uptake and recent HIV-related health care utilization. Among the n=43 incident cases of HIV during the follow-up period, n=8 were among participants who completed assessments online. Finally, as a measure to prevent differential attrition, participant remuneration amounts were the same for participants who completed assessments on-site versus those completing any assessments online.
Individuals were eligible to participate in the P18 cohort study if they were 18-19 years old at screening, born biologically male, reported sexual activity with another man in the 6 months preceding screening, lived in the NYC metropolitan area and self-reported an HIV-negative serostatus. Because a primary objective of the cohort study was to examine racial/ethnic disparities in HIV and related health outcomes, non-probability quota sampling methods were employed to ensure a racially/ethnically diverse study sample. A total of 2,068 individuals were screened for study eligibility; of the n=1,468 ineligible to participate, 49% (n=719) were ineligible due to age >19 years. Among those eligible for the study, n=600 YMSM completed a baseline study visit between July 2009 and May 2011. HIV antibody testing at baseline identified n=6 HIV-seropositive individuals who are excluded from the present analysis.
Careful monitoring and oversight of follow-up reveal high participant retention across completed study visits (86%, 84%, 83%, 83%, 78%, and 81% at 6-, 12-, 18-, 24-, 30- and 36-month follow-up visits for the entire cohort). Next, among the n=600 participants enrolled in P18, n= 456 (76.8%) completed all follow-up assessments onsite whereas n=116 (19.5%) participants utilized a combination of onsite and online modalities to complete the behavioral assessments. Specifically, those who moved out of the New York City metropolitan area for any duration, n=54 (9%), 59 (9.8%), 70 (11.7%), 60 (10%), 53 (8%), and 56 (9%) completed the ACASI assessment online for their 6-, 12-, 18-, 24-, 30- and 36-month follow-up visits, respectively. There were only n=22 (3.6%) participants who completed all follow-up assessments via the online assessment modality.
Measures
Incident HIV Infection
Irrespective of self-reported HIV serostatus at baseline, all participants received pre-test counseling, HIV antibody testing and post-test counseling during the delivery of results. At each follow-up visit, HIV antibody testing and pre- and post-test counseling were conducted following completion of all behavioral assessments. Rapid HIV antibody testing was conducted using the OraQuick ADVANCE® Rapid HIV-1/2 Antibody Test. Pre- and post-test counseling was delivered by trained study staff who received HIV counseling and training certification from the New York State Department of Health's AIDS Institute. Finally, for participants completing an on-line assessment, HIV status, as noted above, was ascertained via self-report and confirmed via data collected at the 36-month visit on treatment uptake and HIV-related health care utilization.
Demographic Characteristics
Participants' self-reported race/ethnicity was categorized as Black, White, Hispanic, and Mixed or another Race (Mixed/Other). The Mixed/Other race category includes participants who identified selected multiple race categories (n=42), who selected ‘other’ as a race category (n=19) and those who selected Asian/Pacific Islander (n=27). Next, perceived familial socioeconomic status (SES) was examined as high, middle or low and used as a proxy for household-level income. The decision to use this measure was due to the fact that YMSM between 18 and 19 years old may be less likely to know or accurately recall their parental household income or have their own household income. School enrollment was based on participant self-report of whether they were currently attending school or not.
Sexual Onset with Male Partners
Participants provided the age at which they first engaged in insertive and receptive anal intercourse with a male partner. Any responses that included an age below 5 years, or were reported as non-consensual, are not included in the present analysis. In addition, participants were asked to report on whether they were currently in a relationship with another man during the 3 months preceding baseline interview as well as whether they had exchanged money for sex (yes/no) during the 3 months preceding baseline interview. Finally, anal intercourse without a condom includes both insertive and receptive anal intercourse during the 30 days preceding interview. In the present analysis, anal intercourse without a condom is examined dichotomously as ‘any’ versus ‘none’.
Residential Neighborhood Characteristics
Valid baseline residential ZIP code data were provided by n=592 participants. The n=509 YMSM from an NYC ZIP code were assigned to one of the United Hospital Fund (UHF) 34 neighborhoods as HIV surveillance data in NYC is readily available for these neighborhoods. The UHF neighborhoods are 34 neighborhoods made up of adjoining ZIP code areas, designated to approximate NYC Community Planning Districts.22 UHF neighborhood poverty rates were determined for New York City and county poverty rates were determined for New York, New Jersey, and Connecticut counties. NYC poverty data were retrieved from the NYC Department of Health and Mental Hygiene's (DHMH) Annual HIV/AIDS Surveillance Report.23 New York State, New Jersey, and Connecticut data were retrieved from the American FactFinder (http://factfinder2.census.gov/) using data from the 2008-2012 American Community Survey 5-Year Estimates. The UHF neighborhood/county poverty variable was categorized into low (<10% of the population living below the federal poverty limit [FPL]), medium (10-<20% living below the FPL), high (20-<30% living below the FPL), and very high poverty (≥30% living below the FPL). Annual HIV diagnosis rates per 100,000 population were determined for and New York City UHF neighborhoods (30) and New York State ZIP codes in 2012 (29). The variable was divided into four categories: 0.0-14.3, 14.4-27.8, 27.9-46.4, and 46.5-174.0 annual HIV diagnoses per 100,000 population.
Analytic Plan
Using descriptive statistics, we examined the distributions of all covariates examined across each wave of data collection. To examine differences in sociodemographic characteristics between those who were active study participants versus those loss-to-follow upin this study sample, chi-square tests and ANOVA were used. Estimates for time to an HIV seropositive test result was measured in number of years from the baseline visit date to the midpoint between the last study visit date at which an individual was tested as HIV seronegative, or reported a HIV seronegative status via on-line assessment, and the first visit date at which a participant received or reported a HIV seropositive test result. Participants who remained HIV seronegative were right censored at the date of their last follow-up visit. Next, we calculated Kaplan–Meier probabilities of testing HIV seropositive, stratified by race/ethnicity and by perceived familial SES, and compared survival distributions using the log-rank test which gives equal weight to all time points. Cox proportional hazards models were employed to formally test for significant differences in time to an HIV seropositive test result.24 First, univariable Cox proportional hazards models were fitted to estimate hazard ratios and 95% confidence intervals (CI) for the probability of progressing to an HIV seropositive event. Multivariable models were fitted to examine the influence of race/ethnicity and perceived familial SES on the probability of seroconversion after adjusting for baseline sociodemographic characteristics and other covariates found to be significant in univariable models. Statistical and graphical approaches were used to test the proportional hazards assumption.25 All analyses were conducted using SPSS (version 21.0).
Results
Sample Characteristics
In order to assess the presence and extent of differential loss-to-follow up, we first examined sample sociodemographic characteristics and sexual behaviors between those who were active study participants, defined as having completed baseline and 2 or more follow-up visits (n=531) and those lost to follow-up, defined as completing only the baseline (n=47) or baseline plus 1 follow-up visit (n=63). There were no statistically significant differences between any sociodemographic or sexual behavior related characteristics among those who were retained in this cohort study versus those who were lost-to-follow up (Table 1). Next, we compared participants who completed all visit onsite versus those who took part in all or some follow-up assessments online. These comparisons indicate that participants who completed some or all assessments online were more likely to be White YMSM compared to other race/ethnicities and also more likely to be of higher perceived SES (Table 1). In addition, these participants were more likely to report still being enrolled in school and to have been older, on average, at age of sexual debut. However, there were no statistically significant differences with regard to recent anal intercourse without a condom, area level poverty or HIV prevalence between the two groups.
Table 1. Comparison of sociodemographic characteristics, sexual behavior and social factors by participant retention and assessment modality for the P18 Cohort Study, n=594.
| Total Sample %(n=594) | Returned for >2 visits %(n=531) | Baseline+1 follow-up visit %(n=63) | p-value | Completed all visits onsite %(n=456) | Completed some or all visits online %(n=138) | p-value | ||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Race/ethnicity | ||||||||
| Black | 15 (88) | 16 (82) | 10 (6) | 0.215 | 16 (73) | 11 (15) | <0.001 | |
| Hispanic | 38 (225) | 38 (199) | 41 (26) | 41 (186) | 28 (39) | |||
| White | 29 (173) | 30 (158) | 24 (15) | 25 (115) | 42 (58) | |||
| Mixed/Other | 18 (106) | 17 (90) | 25 (16) | 18 (80) | 19 (26) | |||
|
| ||||||||
| Perceived familial SES | ||||||||
| Low | 33 (198) | 34 (179) | 30 (19) | 0.764 | 34 (154) | 32 (44) | 0.007 | |
| Middle | 37 (218) | 37 (195) | 37 (23) | 39 (179) | 28 (39) | |||
| High | 30 (176) | 29 (155) | 33 (21) | 27 (121) | 40 (55) | |||
|
| ||||||||
| Enrolled in school (yes) | 86 (509) | 87 (459) | 79 (50) | 0.110 | 84 (384) | 92 (128) | 0.013 | |
|
| ||||||||
| Age at sexual debut, mean (SE) | ||||||||
| Receptive anal intercourse | 16.16 (1.8) | 16.16 (1.8) | 16.22 (1.7) | 16.06 (1.9) | 16.54 (1.5) | 0.022 | ||
| Insertive anal intercourse | 16.41 (1.6) | 16.42 (1.6) | 16.33 (1.4) | 0.724 | 16.31 (1.7) | 16.76 (1.4) | 0.020 | |
|
| ||||||||
| Anal Intercourse without a condom (last 30 days) | 20 (119) | 20 (107) | 19 (12) | 0.825 | 19 (88) | 23 (31) | 0.429 | |
|
| ||||||||
| Area-level HIV prevalence (per 100,000 population) | ||||||||
| 0.0-14.3 | 17 (84) | 16 (74) | 19 (10) | 0.358 | 16 (63) | 20 (21) | 0.581 | |
| 14.4-27.8 | 12 (60) | 11 (51) | 17 (9) | 12 (50) | 9 (10) | |||
| 27.9-46.4 | 32 (163) | 33 (151) | 23 (12) | 32 (127) | 34 (36) | |||
| 46.5-174.0 | 40 (202) | 40 (180) | 42 (22) | 40 (163) | 37 (39) | |||
|
| ||||||||
| Area level poverty | ||||||||
| Low | 25 (140) | 24 (120) | 33 (20) | 0.246 | 22 (99) | 32 (41) | 0.005 | |
| Medium | 39 (221) | 39 (199) | 36 (22) | 37 (164) | 44 (57) | |||
| High | 21 (119) | 22 (111) | 13 (8) | 23 (100) | 15 (19) | |||
| Very high | 16 (92) | 16 (81) | 18 (11) | 18 (80) | 9 (12) | |||
On average, participants completed at least 6 study visits (mean = 6 visits; median = 7 visit) over an average of 2.54 years (median= 2.99 years) of follow-up. Overall, the YMSM participating in this study contributed a total of 1,508.90 person-years of observation, during which time n=43 HIV seroconversions occurred. This yielded an HIV incidence rate of 2.85 per 100 person-years over the follow-up period for this cohort study and accumulative incidence of 7.2%. This excludes the 6 prevalent cases detected at baseline, and thus analyses are based on n=594.
Factors Associated with HIV Infection Incidence
When comparing YMSM who remained HIV seronegative over the course of the follow-up period to those who seroconverted, race/ethnicity was strongly associated with HIV seroconversion (Table 2). Specifically, the smallest proportion of seroconversions occurred among White YMSM (7%) compared with Black (33%), Hispanic (30%) and Mixed/Other YMSM (30%, p < 0.001). We were able to disaggregate 29 APIs from the Mixed/Other group and note that there were no seroconversions among the APIs, while n=7 infections were among those who identified as Mixed Race and n=6 among those who identified an Other Race. With regard to perceived familial SES, YMSM who indicated a low and middle/average perceived SES were more likely to seroconvert (49% and 40%, respectively) compared with their peers who reported a higher perceived SES (12%, p = 0.014). Next, a younger average age at sexual debut with another man (13.4 years vs. 14.7 years, p-value = 0.045) was also associated with greater seroconversion likelihood.
Table 2. Comparison sociodemographics characteristics by HIV seroconversion status in the P18 Cohort Study, n=594.
| Total (n=594) | HIV seronegative (n=551)* % (n) | HIV seroconvert (n=43) % (n) | p-value | |
|---|---|---|---|---|
|
| ||||
| Race/ethnicity | ||||
| Black | 15 (88) | 14 (74) | 33 (14) | <0.001 |
| Hispanic | 38 (225) | 39 (212) | 30 (13) | |
| White | 29 (173) | 31 (170) | 7 (3) | |
| Mixed/Other | 18 (106) | 17 (93) | 30 (13) | |
|
| ||||
| Perceived familial SES | ||||
| Low | 33 (198) | 32 (177) | 49 (21) | 0.014 |
| Middle | 37 (218) | 37 (201) | 40 (17) | |
| High | 30 (176) | 31 (171) | 12 (5) | |
|
| ||||
| Enrolled in school (yes) | 86 (509) | 86 (473) | 84 (36) | 0.658 |
|
| ||||
| Age at sexual debut with a man, years, mean (SE) | 14.6 (0.11) | 14.7 (0.11) | 13.4 (0.50) | 0.045 |
|
| ||||
| Ever exchanged sex for money (yes) | 16 (95) | 15 (84) | 26 (11) | 0.077 |
|
| ||||
| Anal Intercourse without a condom: baseline (last 30 days) | 26 (119) | 19 (106) | 30 (13) | 0.085 |
|
| ||||
| Anal Intercourse without a condom: any follow-up visit (last 30 days) | 62 (368) | 62 (342) | 61 (26) | 0.835 |
|
| ||||
| Area-level HIV prevalence (100,000 population)** | ||||
| 0.0-14.3 | 17 (84) | 17 (78) | 15 (6) | 0.067 |
| 14.4-27.8 | 12 (60) | 13 (60) | 0 (0) | |
| 27.9-46.4 | 32 (163) | 32 (151) | 31 (12) | |
| 46.5-174.0 | 40 (202) | 39 (181) | 54 (21) | |
|
| ||||
| Area level poverty** | ||||
| Low | 25 (140) | 25 (132) | 20 (9) | 0.439 |
| Medium | 39 (221) | 39 (208) | 32 (8) | |
| High | 21 (119) | 20 (108) | 27 (13) | |
| Very high | 16 (92) | 16 (83) | 22 (9) | |
Includes n=551 YMSM who remained HIV seronegative over the follow-up period.
Complete and accurate zip code data only available for n=509 and n=572 participants, respectively.
Note: Column totals may not add to 100% due to missing data
Figure 1 shows the Kaplan Meier Curves for time to HIV seroconversion by race/ethnicity and perceived familial SES. First, survival probability for time to HIV seroconversion was significantly different across racial/ethnic groups. Specifically, Black YMSM were more likely to seroconvert more rapidly compared with all other racial/ethnic groups (log rank test, p < 0.001). In addition, survival probabilities for HIV seroconversion by perceived familial SES indicate a greater likelihood of progression among those with lower perceived SES compared to middle and upper levels (log rank test, p < 0.001).
Figure 1.
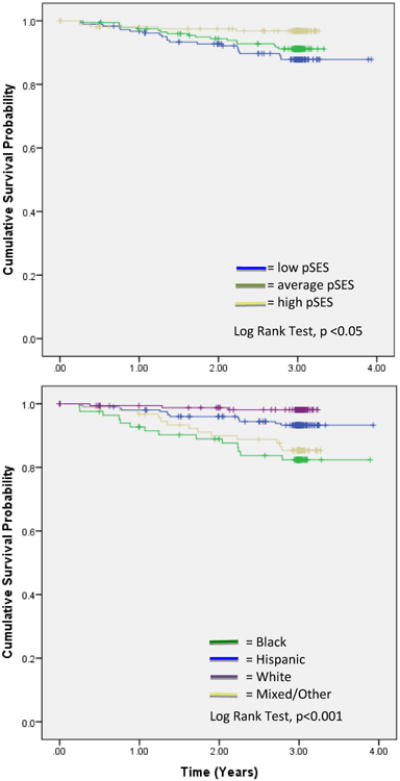
Kaplan Meier survival probability curves showing time to HIV seroconversion by (A) perceived familiar SES and (B) race/ethnicity.
In univariable models, YMSM of color (Black, Hispanic and Mixed/Other YMSM, those from a lower and middle/average perceived familial SES were at an increased risk for HIV seroconversion. And while engaging in anal intercourse without a condom (p=0.091) and having exchanged sex for money (p=0.067) were both marginally associated with an increased risk for HIV seroconversion, YMSM reporting an older, on average, age of sexual debut with another man were less likely to seroconvert (p=0.058). In the final multivariable model, hazard ratios for time to HIV seroconversion were significantly higher for Black YMSM (HR = 7.46; 95% CI 2.06, 27.02) Mixed/Other YMSM (HR = 7.99; 95% CI 2.25, 28.48). Low perceived familial SES was marginally associated with an increased risk for HIV seroconversion (HR = 2.45, 95% CI 0.89, 6.77). However, older age at sexual debut with another man was associated with a lower risk of HIV seroconversion (HR = 0.50; 95% CI 0.27, 0.94).
Discussion
In this diverse sample of young gay, bisexual, and other men who have sex with men (YMSM), we observed an incidence rate of 2.85 per 100 person-years over the course of the follow-up period. In the cross-sectional National HIV Behavioral Surveillance (NHBS) study, Neaigus and colleagues estimated HIV incidence among NYC MSM aged 18 and older based upon self-reported seronegative status within the past 24 months followed by laboratory confirmed seropositive status reported an HIV incidence rates of 5.67 per 100 person-years.26 The lower incidence rate observed in the P18 cohort is likely to be a reflection of the young age of the sample; YMSM were aged 18 or 19 at study entry and up to age 21 or 22 at the end of follow-up. Furthermore, prior analysis of sexual behavior in this cohort9 revealed low levels of risky sexual behavior at baseline, with 19% reporting anal intercourse without a condom in the past 30 days.
There were significant differences across racial lines Black and Mixed/Other YMSM having more than a 7-fold increased risk for HIV seroconversion compared to their White counterparts. The Black-White inequities are consistent with other research documenting the substantial burden of HIV noted in the population of Black MSM, and in particular, YMSM.26-29 Among all MSM ages 18 and older in the NHBS, Blacks were significantly more likely to seroconvert relative to Whites (21). Also consistent with the New York NHBS, there were no significant differences in HIV seroconversion between Hispanic and White YMSM.26 Our findings are therefore consistent with the epidemiological patterns noted throughout the United States, and point to the enormous burden being experienced by young Black sexual minority men, for whom HIV may be but one of the challenges that they face.
Mixed/Other YMSM had a significant 8-fold increased risk for HIV relative to Whites. Since there were no seroconversions among the API subsample, this result was not driven by API men in that aggregated race category. The literature, however, is inconsistent with respect to HIV risk among mixed and other race individuals. In the New York NHBS, 26 other race MSM (included groups not defined) were less likely to be HIV positive but in the pooled analysis of the NHBS and Young Mens' Study found that other race MSM (American Indian/Alaska Native, Asian, Native Hawaiian or Other Pacific Islander, other race, and multiple races) were more likely to be HIV positive.28 A pooled analysis of the HIV Network for Prevention Trials Vaccine Preparedness Study, EXPLORE behavioral efficacy trial, and VAX004 vaccine efficacy trial 29 found no increased risk for HIV among other race individuals (included groups not defined). Who is included in mixed and racial categories varies across studies, is often not precisely; such categories are quite heterogeneous which, coupled with small sample sizes, makes interpretation impossible. However, exclusion of these populations from analyses is also problematic as it results in the systematic exclusion of some minority communities. In the 2000 US Census, more than 6.3 million, or 2.4% of the US population identified as two or more races.30 By the 2010 US Census, that number had grown to more than 8.2 million or 2.9% of the population.31 This was a 32% increase in the number of people identifying as two or more races.
Perceived familial SES at baseline was significantly associated with HIV seroconversion in bivariable analyses but not in the final multivariable models, although low SES YMSM were marginally more likely to seroconvert. UHF neighborhood/county-level poverty was not significantly associated with HIV seroconversion. SES is an important determinant of health and is strongly related to race in the US. In this analysis, perceived familial SES likely attenuated the association between race and HIV seroconversion, but did not eliminate it as evidenced by the attenuated race/ethnicity HRs in the final adjusted model. Low SES YMSM are more likely to reside in neighborhoods with higher levels of poverty, environments associated with lower access to effective health services, and higher level of untreated sexually transmitted infections (STIs) including HIV, conditions which have been shown to be inextricably connected.32 As result of such conditions, HIV tends to cluster in neighborhoods,33 and for Black and Hispanic YMSM, experiences of poverty are contextual factors shown to heighten susceptibility to HIV.34 In this sample, perceived familial SES was significantly associated with both race/ethnicity and UHF neighborhood/county-level poverty. More granular measures of area-level poverty (i.e., census-tract) are needed to further explore the relationship between area-level poverty and HIV incidence.
Age at sex debut was an important predictor of HIV seroconversion. YMSM who initiated sex with another man at after the age of 14 were substantially less likely to seroconvert, indicating the delay of sexual debut may be protective for HIV in sexual minority men. Previous studies have indicated that YMSM who begin to engage in sex at a young age have heightened risk fir HIV infection because there is a high likelihood of engaging in condomless sex and engaging in sex with older partners; these young men also have more limited ability to negotiate safer sex, etc.6,10,35,36. These findings suggest that delaying sexual debut is a key target for HIV prevention among adolescent and emerging adult YMSM. Kubicek et al. 36 note that YMSM have had limited access to comprehensive sexuality education prior to initiation of anal sex and often remain in the dark since such information is not made available from family, friends, or schools. As a result, YMSM have limited information about STIs, including HIV, an infection to which young sexual minority men are more vulnerable than their heterosexual peers. Given that earlier sexual debut is associated with a higher likelihood of HIV seroconversion for YMSM, and given that sexual minority men are themselves often raised by heterosexual parents who themselves may not be equipped to educate their children, it is imperative that sex education be provided in schools, be initiated at the onset of adolescence, and also include comprehensive information abut sexuality and safer sex practices for sexual minority men.
Limitations
Several limitations should be considered. The past 30 day referent period for sexual activity captured via the TLFB is somewhat short; however, it provides more accurate and comprehensive data for the time period under study. In this study, 23% of the sample completed at least one follow-up visit online, meaning HIV screening tests were not completed and HIV incidence may be underestimated. However, because these trends reflect NYC and national trends, we do not believe these results are invalid.
Conclusions
Future studies are needed disentangle the drivers of the racial inequities observed in this cohort study of racially/ethnically and socioeconomically diverse YMSM. A critical element of such work is to document and delineate the relative contributions of economic, social, psychosocial, and structural factors that place young racial minority YMSM at such high risk for HIV infections. Such understandings also will aid in the strategic scale-up of existing interventions and the uptake and effectiveness of new biomedical interventions, including Pre-Exposure Prophylaxis (PrEP), aimed at addressing these HIV disparities. Knowledge, which delineates the social and structural factors, in addition to behavioral factors such as sexual debut, that place young Black sexual minority men at risk for HIV, will ultimately be more helpful in addressing the epidemic, through the development of programs and policies targeting inequities, and by shifting the dialogue away from one that simply focuses on race.
Table 3. Univariable and Multivariable hazard ratios (HRs) for HIV seroconversion among YMSM in the P18 Cohort study, n=594.
| Unadjusted HR (95% CI) | p-value | Adjusted HR (95% CI) | p-value | |
|---|---|---|---|---|
|
| ||||
| Race/ethnicity | ||||
| Black | 10.10 (2.90,35.13) | <0.001 | 7.46 (2.06,27.02) | 0.002 |
| Hispanic | 3.59 (1.02, 12.56) | 0.047 | 2.63 (0.72, 9.55) | 0.143 |
| Mixed/Other | 8.05 (2.29, 28.24) | 0.001 | 7.99 (2.25, 28.48) | 0.001 |
| White | 1.00 | 1.00 | ||
|
| ||||
| Perceived familial SES | ||||
| Low | 3.80 (1.43, 10.08) | 0.007 | 2.45 (0.89, 6.77) | 0.083 |
| Middle | 2.72 (1.01, 7.37) | 0.049 | 2.18 (0.79, 5.98) | 0.132 |
| High | 1.00 | 1.00 | ||
|
| ||||
| Age at sexual debut with a man (>14 yo) | 0.55 (0.29, 1.02) | 0.058 | 0.50 (0.27, 0.94) | 0.032 |
|
| ||||
| Anal intercourse without a condom (last 30 days) | 1.75 (0.91, 3.36) | 0.091 | -- | |
|
| ||||
| Ever exchanged sex for money (yes) | 1.90 (0.96, 3.77) | 0.067 | -- | |
Acknowledgments
Sources of Funding: NIH, 1R01DA025537
Footnotes
Conflicts of Interest: None to report
References
- 1.Chandra A, Mosher WD, Copen C, Sionean C. Sexual behavior, sexual attraction, and sexual identity in the United States: data from the 2006-2008 National Survey of Family Growth. National health statistics reports. 2011;(36):1–36. [PubMed] [Google Scholar]
- 2.Centers for Disease Control and Prevention. Estimated HIV incidence in the United States, 2007-2010. 2012 Available at: http://www.cdc.gov/hiv/pdf/statistics_hssr_vol_17_no_4.pdf.
- 3.Hall HI, Song R, Rhodes P, et al. Estimation of HIV incidence in the United States. JAMA. 2008;300(5):520–529. doi: 10.1001/jama.300.5.520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Millett GA, Flores SA, Peterson JL, Bakeman R. Explaining disparities in HIV infection among black and white men who have sex with men: a meta-analysis of HIV risk behaviors. AIDS. 2007;21(15):2083–2091. doi: 10.1097/QAD.0b013e3282e9a64b. [DOI] [PubMed] [Google Scholar]
- 5.Millett GA, Peterson JL, Wolitski RJ, Stall R. Greater risk for HIV infection of black men who have sex with men: a critical literature review. Am J Public Health. 2006;96(6):1007–1019. doi: 10.2105/AJPH.2005.066720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Halkitis PN, Brockwell S, Siconolfi DE, et al. Sexual behaviors of adolescent emerging and young adult men who have sex with men ages 13-29 in New York City. J Acquir Immune Defic Syndr. 2011;56(3):285–291. doi: 10.1097/QAI.0b013e318204194c. [DOI] [PubMed] [Google Scholar]
- 7.Santos-Hövener C, Zimmermann R, Kucherer C, et al. Conversation about Serostatus decreases risk of acquiring HIV: results from a case control study comparing MSM with recent HIV infection and HIV negative controls. BMC Public Health. 2014;14:453. doi: 10.1186/1471-2458-14-453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Goodreau SM, Carnegie NB, Vittinghoff E, et al. What drives the US and Peruvian HIV epidemics in men who have sex with men (MSM)? PLoS One. 2012;7(11):e50522. doi: 10.1371/journal.pone.0050522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Halkitis PN, Kapadia F, Siconolfi DE, et al. Individual, psychosocial, and social correlates of unprotected anal intercourse in a new generation of young men who have sex with men in New York City. Am J Public Health. 2013;103(5):889–895. doi: 10.2105/AJPH.2012.300963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Outlaw AY, Phillips G, Hightow-Weidman LB, et al. Age of MSM sexual debut and risk factors: results from a multisite study of racial/ethnic minority YMSM living with HIV. AIDS Patient Care STDS. 2011;25(Suppl 1):S23–S29. doi: 10.1089/apc.2011.9879. [DOI] [PubMed] [Google Scholar]
- 11.Albert B, Brown S, Flanigan CM. 14 and Younger: The Sexual Behavior of Young Adolescents Summary. Washington, DC: National Campaign to Prevent Teen Pregnancy; 2003. Available at: [Google Scholar]
- 12.Centers for Disease Control and Prevention. Characteristics associated with HIV infection among heterosexuals in urban areas with high AIDS prevalence --- 24 cities, United States, 2006-2007. MMWR Morbidity and mortality weekly report. 2011;60(31):1045–1049. [PubMed] [Google Scholar]
- 13.Halkitis PN, Figueroa RP. Sociodemographic characteristics explain differences in unprotected sexual behavior among young HIV-negative gay, bisexual, and other YMSM in New York City. AIDS Patient Care STDS. 2013;27(3):181–190. doi: 10.1089/apc.2012.0415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Santelli JS, Lowry R, Brener ND, Robin L. The association of sexual behaviors with socioeconomic status, family structure, and race/ethnicity among US adolescents. Am J Public Health. 2000;90(10):1582–1588. doi: 10.2105/ajph.90.10.1582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Storholm ED, Siconolfi DE, Halkitis PN, Moeller RW, Eddy JA, Bare MG. Sociodemographic Factors Contribute to Mental Health Disparities and Access to Services Among Young Men Who Have Sex with Men in New York City. J Gay Lesbian Ment Health. 2013;17(3):10. doi: 10.1080/19359705.2012.763080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kapadia F, Siconolfi DE, Barton S, Olivieri B, Lombardo L, Halkitis PN. Social support network characteristics and sexual risk taking among a racially/ethnically diverse sample of young, urban men who have sex with men. AIDS Behav. 2013;17(5):1819–1828. doi: 10.1007/s10461-013-0468-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Siconolfi DE, Kapadia F, Halkitis PN, et al. Sexual health screening among racially/ethnically diverse young gay, bisexual, and other men who have sex with men. J Adolesc Health. 2013;52(5):620–626. doi: 10.1016/j.jadohealth.2012.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Halkitis PN, Moeller RW, Siconolfi DE, Storholm ED, Solomon TM, Bub KL. Measurement model exploring a syndemic in emerging adult gay and bisexual men. AIDS Behav. 2013;17(2):662–673. doi: 10.1007/s10461-012-0273-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Halkitis PN, Kapadia F, Bub KL, Barton S, Moreira AD, Stults CB. A Longitudinal Investigation of Syndemic Conditions Among Young Gay, Bisexual, and Other MSM: The P18 Cohort Study. AIDS Behav. 2014 doi: 10.1007/s10461-014-0892-y. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sobell LC, Sobell MB. Alcohol Timeline Followback Users' Manual. Toronto: Addiction Research Foundation; 1995. [Google Scholar]
- 21.Sobell LC, Agrawal S, Sobell MB, et al. Comparison of a quick drinking screen with the timeline followback for individuals with alcohol problems. J Stud Alcohol. 2003;64(6):858–861. doi: 10.15288/jsa.2003.64.858. [DOI] [PubMed] [Google Scholar]
- 22.New York City Department of Health and Mental Hygiene. NYC UHF Neighborhoods. Available at: http://www.nyc.gov/html/doh/downloads/pdf/tracking/neighborhoods.pdf.
- 23.New York City Department of Health and Mental Hygiene. New York City HIV/AIDS Annual Surveillance Statistics 2012. 2014 Available at: http://www.nyc.gov/html/doh/downloads/pdf/ah/surveillance2012-table-all.pdf.
- 24.Cox DR, Oakes D. Analysis of Survival Data. London: Chapman & Hall; 1984. [Google Scholar]
- 25.Hess KR. Graphical methods for assessing violations of the proportional hazards assumption in Cox regression. Stat Med. 1995;14(15):1707–1723. doi: 10.1002/sim.4780141510. [DOI] [PubMed] [Google Scholar]
- 26.Neaigus A, Jenness SM, Hagan H, et al. Estimating HIV incidence and the correlates of recent infection in venue-sampled men who have sex with men in New York City. AIDS Behav. 2012;16(3):516–524. doi: 10.1007/s10461-011-0050-8. [DOI] [PubMed] [Google Scholar]
- 27.Neaigus A, Reilly KH, Jenness SM, Wendel T, Marshall DM, Hagan H. Multilevel risk factors for greater HIV infection of black men who have sex with men in New York City. Sex Transm Dis. 2014;41(7):433–439. doi: 10.1097/OLQ.0000000000000144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Oster AM, Johnson CH, Le BC, et al. Trends in HIV prevalence and HIV testing among young MSM: five United States cities, 1994-2011. AIDS Behav. 2014;18(Suppl 3):S237–S247. doi: 10.1007/s10461-013-0566-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Scott HM, Vittinghoff E, Irvin R, et al. Age, race/ethnicity, and behavioral risk factors associated with per contact risk of HIV infection among men who have sex with men in the United States. J Acquir Immune Defic Syndr. 2014;65(1):115–121. doi: 10.1097/QAI.0b013e3182a98bae. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Bureau of the Census, US Department of Commerce. US Census 2000. 2014 Sep 20; 2000. Available at: www.infoshare.org.
- 31.Bureau of the Census, US Department of Commerce. US Census 2010. 2014 Sep 20; 2010. Available at: www.infoshare.org.
- 32.Castel AD, Befus M, Willis S, et al. Use of the community viral load as a population-based biomarker of HIV burden. AIDS. 2012;26(3):345–353. doi: 10.1097/QAD.0b013e32834de5fe. [DOI] [PubMed] [Google Scholar]
- 33.Nunn A, Yolken A, Cutler B, et al. Geography should not be destiny: focusing HIV/AIDS implementation research and programs on microepidemics in US neighborhoods. Am J Public Health. 2014;104(5):775–780. doi: 10.2105/AJPH.2013.301864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Williams JK, Wyatt GE, Resell J, Peterson J, Asuan-O'Brien A. Psychosocial issues among gay- and non-gay-identifying HIV-seropositive African American and Latino MSM. Cultur Divers Ethnic Minor Psychol. 2004;10(3):268–286. doi: 10.1037/1099-9809.10.3.268. [DOI] [PubMed] [Google Scholar]
- 35.Warren JC, Fernandez MI, Harper GW, Hidalgo MA, Jamil OB, Torres RS. Predictors of unprotected sex among young sexually active African American, Hispanic, and White MSM: the importance of ethnicity and culture. AIDS Behav. 2008;12(3):459–468. doi: 10.1007/s10461-007-9291-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kubicek K, Beyer WJ, Weiss G, Iverson E, Kipke MD. In the dark: young men's stories of sexual initiation in the absence of relevant sexual health information. Health Educ Behav. 2010;37(2):243–263. doi: 10.1177/1090198109339993. [DOI] [PMC free article] [PubMed] [Google Scholar]