

Abstract
Objectives
Even after evolution of computerized tomography and improved surgical measures, treatment of intraarticular calcaneal fractures remains a controversy. Hence this study was carried out to compare functional outcomes of displaced intraarticular calcaneal fractures, treated with operative management with plating and conservative management with cast.
Material and methods
This study was carried out as a prospective, comparative study. Twenty nine (30 fractures) patients with acute, displaced intraarticular fractures of calcaneum aged 18–50 years, were enrolled in the study. Open fractures and fractures older than two weeks were excluded. 30 fractures were divided into two groups (operative and conservative; n = 15 in each). Evaluation in form of post treatment restoration of Bohler's angle, heel varus angle and with Creighton–Nebraska (C–N) score for functional outcome was done at the end of 12 months.
Results
When we consider the clinical evaluation under the C–N score, the results of operatively managed calcaneal fractures are slightly better than those of the conservative group. But this did not have any statistical significance. Also, there was significant difference in pre and post treatment Bohler's angle and heel varus angle in operative group. Three cases of plating suffered from post-operative wound dehiscence.
Conclusion
A relatively better functional outcome was observed in displaced and comminuted fractures in plating, provided that the Bohler's angle was restored. In conservative group, functional outcome of minimally displaced fractures were better than displaced comminuted fractures. Post treatment Bohlers angle has prognostic importance in functional outcome.
Keywords: Intra articular calcaneal fracture, Bohler's angle, Crucial angle of Gissane, Heel varus angle, Creighton–Nebraska health foundation score
1. Introduction
Calcaneal fracture, the most frequently injured tarsal bone, accounts for about 1–2% of all fractures in the human body. Approximately 75% calcaneal fractures are intra-articular, involving the subtalarjoint, mostly caused by a fall from a height with the heel directly hitting the ground.1,2 Fracture of calcaneus leads to considerable morbidity and hence was historically quoted that ‘Ordinarily speaking the man who breaks his heel bone is ‘done’, so far as his industrial future is concerned‘.3 Even after emergence of CT and advanced surgical instrumentations and techniques, the treatment for the intra articular fractures has been a point of debate. Reviews on this subject, have failed to demonstrate indisputable superior results by either operative or conservative approach to the treatment of displaced intra-articular calcaneal fractures.4,5 So, despite the surgeon's extensive experience with this injury, it's a major socio-economic impact with regard to the time lost from work and recreation, and even after attention given to it for many years throughout the world, there is still no method of treatment that yields consistently good results. So we believe such study will attempt to make some valuable contribution to this debate about superiority of operative or conservative treatment.
2. Materials and methods
This prospective comparative study comprised of 30 intra-articular calcaneal fractures in 29 patients from June 2012 to September 2014 (minimum follow up one year). Open fractures, extra articular fractures, fractures presenting after 2 weeks after injury were excluded from the study. Fractures were classified according to Sander's classification.6 The patients were divided into two groups (operative and conservative) with simple randomization technique with chits. 30 chits with 15 labelled conservative and 15 labelled operative were kept in a box, were mixed and one chit was picked whenever the treatment modality of new patient was to be decided. So out of 30 fractures, 15 were managed conservatively and 15 were managed surgically with open reduction and internal fixation with plating. All the results were evaluated by the same senior orthopaedic surgeon in the department who was unaware of the design and model of the study.
Conservative management was in a form of below knee plaster cast initially if there was no gross swelling or else immobilization was done with below knee slab which was later converted into a cast. Cast was removed after 6 weeks & physiotherapy exercises for ankle and sub-talar joints were started after removal of cast. Once the fracture showed appearance of signs of union, partial weight bearing was advised, which was approximately at 7–8 weeks and it was then gradually increased to full weight bearing. The Appearance and progression of signs of union was assessed both clinically and radiologically. Decreased local tenderness at fracture site, reduced pain while weight bearing were considered signs of commencement of union. Radiologically, diminution of visibility of fracture site, appearance of increased bone density (Sclerosis) at fracture margin was seen in both groups. In conservative group, appearance of irritation callus was observed.
In operative group, open reduction and internal fixation was done with calcaneal plates. Lateral Seligson's approach was used for all, once oedema subsided and wrinkle sign was seen 7–10 days after injury.5 The incision was started approximately 2 cm above the tip of the lateral malleolus, just lateral to the Achilles tendon till the plantar surface of the heel. It was then slightly curved and was continued along the junction of the lateral foot and the heel pad till calcaneo-cuboid joint. Skin was not incised in layers, but a full thickness subperiosteal flap was elevated to maintain the vascularity especially at the apex of the incision (Fig. 1E). Retraction was done with no touch technique with 3 k-wires.
Fig. 1.
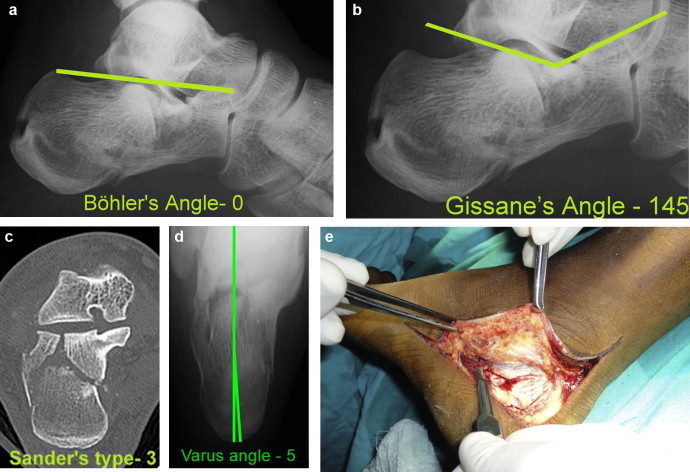
Pre operative radiological assessment and highlights of operative procedure.
Fracture site was exposed. Lateral wall was disimpacted by varus force applied by a transverse stout k wire drilled in tuberosity. Reduction of articular surface was done, along with reduction of the Sustentacular fragment. Hydroxyapatite crystals were filled in 10 out of 15 the cases where there was substantial loss of cancellous bone to support the articular fragments (Fig. 1F). The lateral border was then reduced along with the varus by the k wire, by giving a valgus force. Restoration of angle of Gissane was confirmed, which is the best intra-operative indicator of good restoration of articular surface anatomy.7
The reduction was confirmed by lateral and axial views under image intensifier. The appropriately sized plate was placed on the lateral surface of calcaneum. The complete fixation was again confirmed under image intensifier. Skin was the closed with Allgower-Donati sutures in 9 and by mattress sutures in 6 patients.8 Sterile dressing was given. Suture removal was done after 17–18 days. Post operatively below knee slab was given for 4–5 weeks & Physiotherapy exercises for ankle and sub-talar joints were started on removal of slab with non-weight bearing walking. Once the fracture showed signs of union, partial weight bearing was advised, which was approximately at 7–8 weeks and it was then gradually increased to full weight bearing.
For all patients, the radiological evaluation was carried out initially on weekly basis from 4th week to 8th week. After the 8th week (2 months), the radiological evaluation was repeated on 6th month and 12th month. Minimum follow up of at least one year was completed in each case. Throughout the follow up, X-rays were assessed for progression of union. The Bohler's angle, Heel varus angle and Gissane's angle were measured on 2nd month, 6th month and 12th month in both groups. Criegton-Nebrasaka health foundation scoring system was used to evaluate the patients at the end of 1 year9,10 (Table 1). Pre-treatment and final post treatment (1 year follow up) Bohler's angle, heel varus angle & Gissane's angle were also compared (Figs. 1–4). Finally correlation between C–N score and mean Bohler's angle was evaluated (see Table 2).
Table 1.
Creighton–Nebraska score.
| Summary of Creighton–Nebraska health foundation assessment for fractures of the calcaneum. |
|---|
| Summary of clinical entities considered |
| 1. Pain on activity |
| 2. Pain at rest |
| 3. Activity level |
| 4. Range of inversion/eversion |
| 5. Returning back to work |
| 6. Change of show size |
| 7. Swelling |
| Gradations |
| Excellent – 90–100 points |
| Good – 80–89 points |
| Fair – 65–79 points |
| Poor – 65 or less |
Fig. 2.
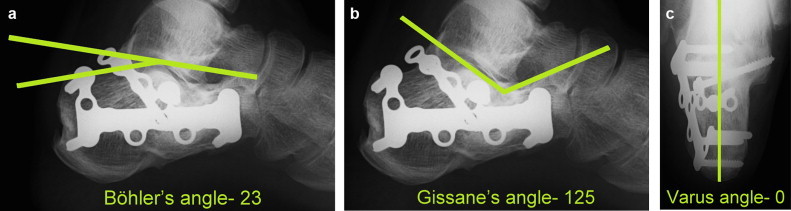
Post operative radiographs at 1 year follow up. All the angles were restored within their normal range.
Fig. 3.
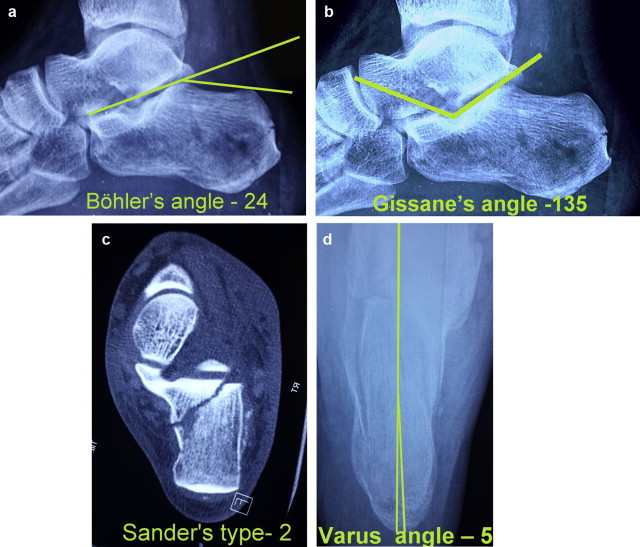
Radiological assessment before cast application.
Fig. 4.
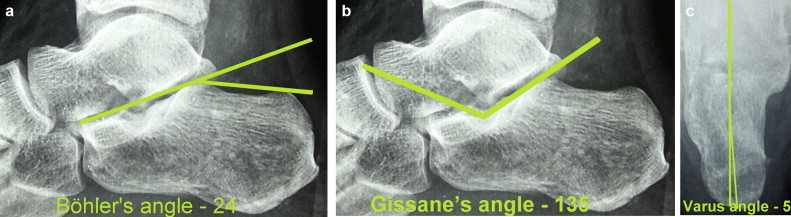
Post treatment radiographs at 1 year follow up. All the angles were maintained within their normal range.
Table 2.
Fracture Classification distribution.
| Treatment | Sander's type |
Total | |||
|---|---|---|---|---|---|
| I | II | III | IV | ||
| Cons | 1 | 7 | 5 | 2 | 15 |
| 6.66% | 46.66% | 33.33% | 13.33% | 100% | |
| Oper | 0 | 5 | 6 | 4 | 15 |
| 0% | 33% | 40% | 26.66% | 100% | |
| Total | 1 | 12 | 11 | 6 | 30 |
| 3.33% | 40% | 36.66% | 20% | 100% | |
Case 3 – Open Reduction and Internal Fixation.
Case 6 – Conservative Management.
3. Results
In our study, 20 patients were males, and 10 were females. The mean age of patients in operative group was 31 years and that of conservative group was 34 years. Majority of calcaneal fractures were caused by fall from height (77% of cases), and 23% were due to road traffic accidents. Out of 30 Fractures, only one patient had bilateral intra-articular calcaneal fractures this series. Nine patients had associated fractures with calcaneal fractures. There were 5 vertebral fractures, 2 lower extremity fractures and 2 fracture of distal radius associated.
The fractures were classified according to Sander's classification based on computerised tomography.6 Most of the fractures were type II and type III fractures, forming almost 76% of the total number. There was only one Type I fracture in our study (Table 2).
The Crucial angle of Gissane was measured in pre and post treatment, in both groups. The improvement of the angle in operative group was found to be statistically significant (Table 3).
Table 3.
Gissane's angle.
| Treatment | Gissane's | N | Mean | Mean diff | P val |
|---|---|---|---|---|---|
| Cons | Pre | 15 | 160.3 | 0.3 | 0.8335 |
| Post | 15 | 160 | |||
| Oper | Pre | 15 | 158.2 | 20.6 | <0.0001 |
| Post | 15 | 137.6 |
In our study we found that the difference between Pre and post treatment values, Bohler's angle in operative group was extremely significant. The mean difference between pre and post treatment values of conservative group was only 1.10 indicating that the restoration of Bohler's angle with conservative method was not possible (Table 4).
Table 4.
Bohler's angle.
| Treatment | BOA | N | Mean0 | Mean diff | P val |
|---|---|---|---|---|---|
| Cons | Pre | 15 | 14.066 | 1.134 | 0.391 |
| Post | 15 | 15.2 | |||
| Oper | Pre | 15 | 11 | 12.66 | <0.0001 |
| Post | 15 | 23.66 |
Similarly, the heel varus angulation, which ultimately leads to loss of heel height, was found to be correctable only by operative method. The mean values of both pre-operative groups were almost similar, but in operative group the varus angulation could almost completely be corrected with mean value being only 0.20 (Table 5).
Table 5.
Heel varus angle.
| Treatment | Varus | N | Mean0 | Mean diff | P val |
|---|---|---|---|---|---|
| Cons | Pre | 15 | 9 | 0.2 | 0.9139 |
| Post | 15 | 8.8 | |||
| Oper | Pre | 15 | 9.1 | 8.7 | <0.0001 |
| Post | 15 | 0.4 |
Evaluation of functional outcome was done according to C–N score at the end of 1 year. It was observed that almost 63% patients, i.e. 19 patients out of 30 had good results. 10% i.e. 3 patients had excellent results at the end of 1 year. 16.6% patients had fair outcomes and only 3 patients had poor outcome. Both groups had almost similar outcomes without taking the fracture type into consideration (Table 6).
Table 6.
Functional outcome.
| Treatment | C–N score |
Total | |||
|---|---|---|---|---|---|
| Poor | Fair | Good | Excellent | ||
| Cons | 2 | 3 | 9 | 1 | 15 |
| 13.33% | 20% | 60% | 6.66% | 100% | |
| Oper | 1 | 2 | 10 | 2 | 15 |
| 6.66% | 13.33% | 66.66% | 13.33% | 100% | |
| Total | 3 | 5 | 19 | 3 | 30 |
| 10% | 16.66% | 63.33% | 10% | 100% | |
4. Discussion
The treatment of calcaneal fractures remains controversial. In this study the outcomes of operatively managed and conservatively managed calcaneal fractures was compared in order to find out the better method for different type of fracture. Two different parameters were used to compare the outcome and finally correlation between the two parameters was evaluated. The results of present study are compared with those of previous similar studies.
It can be seen from Table 7 that the results of operatively managed calcaneal fractures are slightly better than those of the conservative group when comparison is done irrespective of the fracture type. But this does not have any statistical significance, as proved by chi square test. Compared to a similar study (Thordarson11), the results of our study in conservative group are better. This may be due to weight bearing after one and a half month, proper immobilization for the required time or due to good compliance of patients. The outcomes in both conservative and operative groups in this study are comparable with all other (Griffin,12 Argen,13 Buckley5) studies (Table 7).
Table 7.
Overview and comparison with previous studies.
| Rx | Year | Series | Cases | Mean score | Interpretation | Scoring system |
|---|---|---|---|---|---|---|
| CONS | 1996 | Thordarson | 15 | 55.5 | Poor | Questionnaire |
| 2013 | Argen | 40 | 75.5 | Good | AFOS | |
| 2014 | Griffin | 74 | 65.7 | Good | Kerr–Atkins Score | |
| 2002 | Buckley | 218 | 64.7 | Good | SF – 36 | |
| 2014 | Present | 15 | 78.7 | Good | C–N Score | |
| OPER | 1996 | Thordarson | 15 | 86.7 | Excellent | Questionnaire |
| 2013 | Argen | 42 | 72.5 | Good | AFOS | |
| 2014 | Griffin | 69 | 69.8 | Good | Kerr–Atkins Score | |
| 2002 | Buckley | 206 | 68.7 | Good | SF – 36 | |
| 2014 | Present | 15 | 82.4 | Good | C–N Score | |
Randle et al.14 performed a meta-analysis of articles between 1980 and 1996 dealing with calcaneal fractures. Of the 1845 articles, 6 compared operative and non operative treatment for displaced calcaneal fractures. A statistical summary of information across the 6 articles revealed a trend for surgically treated patients to be more likely to return to the same type of work as compared with non operatively treated individuals. There was also a trend for non-operatively treated patients to have a higher risk of experiencing severe foot pain.
The tuber angle of Böhler is composed of a line drawn from the highest point of the anterior process of the calcaneus to the highest point of the posterior facet and a line drawn tangential to the superior edge of the tuberosity. The angle is normally between 20 and 40°; a decrease in this angle indicates that the weight-bearing posterior facet of the calcaneus has collapsed, thereby shifting body weight anteriorly. Table 4 shows that there was a more statistically significant difference in pre and post treatment Bohler's angle in operative group in comparison to conservative group. This shows that restoration of the Bohler's angle is possible with operative management.15 When calculated with Pearson's correlation, our study shows a good correlation between post treatment Bohler's angle and C–N score for conservative group and very significant correlation in operative group. There is also an overall good correlation between post treatment Bohler's angle and C–N score which is statistically significant. D Makki et al16 carried out a retrospective review of 47 intra-articular fractures of the calcaneum treated by open reduction and internal fixation in 45 patients by a single surgeon. They concluded that restoration of Bohler's angle was associated with a better outcome and that prompt osteosynthesis should be considered for intra-articular fractures of the calcaneum in order to restore the shape of the hindfoot and Bohler's angle. This indicated that with the restoration of Bohler's angle, the functional outcome is much better and if post treatment Bohler's angle is not restored then the outcome will be poor.
The varus angulation correction is very important to prevent the malunion and its related complications, and most importantly, to maintain the height of the heel. Table 4 shows that the essential varus correction can be achieved by open reduction of the fracture to maximum extent. With similar mean values pre and post treatment, it was seen that conservative management couldn't correct the varus deformity of heel, and it was proved statistically. Like Bohler's angle, the correction of heel varus too is difficult to achieve by conservative method. Similar opinion was given by Zwipp17 in his study of operative treatment in 123 patients about feasibility of varus correction in treatment by open reduction.
With conservative management, in the only patient there was excellent outcome with type I fracture, good outcomes with type II and III fractures. There were fair to poor outcomes type IV fracture. There was no type I fracture treated with plating. With operative management in patients with type II fractures, one patient had excellent result and other 4 had good results. With type III fracture, 1 patient had excellent result and 4 had good results. With type IV fracture 3 of them had good results but one patient had a poor result.L.A.Crosby9 et al. compared outcomes of 30 intra articular calcaneum fractures according to fracture type, treated by conservative treatment. They classified the fractures on CT almost similar to Sander's, with type 1 being small fracture fragments or undisplaced fracture, type 2 being displaced fractures and type 3 being comminuted displaced fractures. They concluded that it was possible to predict which fractures will do well with closed reduction, with results progressing from excellent to poor with increased comminution. Our study showed similar trend. In our study the results of the only type I fractures managed conservatively had an excellent outcome. Also type II and type III fractures had almost similar outcome with operative and conservative management. The difference was not statistically significant. But in type IV fractures operative management was comparatively better than conservative management with one poor and one fair result in conservative group.
Wound dehiscence was seen in 3 cases of operative group. All of them occurred at the area where two limbs of incision met, and were typically late on onset, occurring around 12th to 15th day post operatively (Fig. 5). The wound healed with regular dressings within average period of 2 weeks from time of dehiscence. Use of vacuum assisted closure or soft tissue muscle flap was not needed. No other complications like sural nerve injury, peroneal tendons dislocation, and implant failure were encountered in our study.
Fig. 5.

Wound dehiscence at apex of the incision.
Our study has a few limitations. The sample of our study is small, that makes it difficult to make any concrete recommendations. Also, in our study the average period of follow up is 1 year. Hence long term problem of subtalar arthritis has not been taken into consideration.
Hence we conclude, that displaced and comminuted fractures managed surgically have a relatively better functional outcome as compared to those managed conservatively, provided Bohler's angle is restored. Although, the superiority of functional outcomes in operative group couldn't be proved statistically. The outcomes of both surgically and conservatively managed cases are comparable to the results in other studies. But the size of the present study group is small to come to a concrete conclusion. In case of displaced and comminuted calcaneal fractures, the aim of the treatment should be anatomical reduction and restoration of Bohler's angle surgically. Wound dehiscence with infection is a major risk in operative group.
Conflicts of interest
All authors have none to declare.
References
- 1.Atkins R.M., Allen P.E., Livingstone J.A. Demographic features of intra-articular fractures of the calcaneum. Foot Ankle Surg. 2001;7:77–84. [Google Scholar]
- 2.Bremner A.E., Warrick C.K. Fractures of the calcaneus. J Fac. 1951;2:235–241. doi: 10.1016/s0368-2242(51)80016-2. [DOI] [PubMed] [Google Scholar]
- 3.Cotton F.J. Fractures of the oscalcis. Boston Med Surg J. 1908;18:559–565. [Google Scholar]
- 4.Parmar H.V., Triffitt P.D., Gregg P.J. Intraarlicular fractures of calcaneus treated operatively or conservatively: a prospective study. J Bone Jt Surg. 1993;75B:932–943. doi: 10.1302/0301-620X.75B6.8245085. [DOI] [PubMed] [Google Scholar]
- 5.Buckley R., Tough S., McCormack R. Operative compared with non operative treatment of displaced intraarticular calcaneal fractures. J Bone Jt Surg. 2002;84A:1733–1740. doi: 10.2106/00004623-200210000-00001. [DOI] [PubMed] [Google Scholar]
- 6.Sanders R., Fortin P., DiPasquale T., Walling A. Operative treatment in 120 displaced intraarticular calcaneal fractures results using a prognostic Computed Tomography scan classification. Clin Res. 1993;290:87–95. [PubMed] [Google Scholar]
- 7.Swanson A., Clare Michael P., Sanders Roy W. Management of intra-articular fractures of the calcaneus Scott. Foot Ankle Clin. 2008;13 doi: 10.1016/j.fcl.2008.09.006. [DOI] [PubMed] [Google Scholar]
- 8.Sagi H Claude, Papp Steven, DiPasquale Thomas DO. The effect of suture pattern and Tension on cutaneous blood flow as assessed by laser Doppler flowmetry in a pig model. J Orthop Trauma. March 2008;22:171–175. doi: 10.1097/BOT.0b013e318169074c. [DOI] [PubMed] [Google Scholar]
- 9.Crosby L.A., Fitzgibbons T. Computerized Tomography scanning of acute intraarticular fractures of the calcaneus. J Bone Jt Surg. 1990;72:852–859. [PubMed] [Google Scholar]
- 10.Schepers Tim, Heetveld Martin J., Mulder Paul G.H., Patka Peter. Clinical outcome scoring of intra-articular calcaneal fractures. J Foot Ankle Surg. 2008;47:213–218. doi: 10.1053/j.jfas.2008.02.014. [DOI] [PubMed] [Google Scholar]
- 11.Thordarson David. Operative vs. nonoperative treatment of intra-articular fractures of the calcaneus: a prospective randomized trial. Foot Ankle Int. January 1996;17:2–9. doi: 10.1177/107110079601700102. [DOI] [PubMed] [Google Scholar]
- 12.Griffin Damian. Operative versus non-operative treatment for closed, displaced, intra-articular fractures of the calcaneus: randomised controlled trial. BMJ. 2014;349:g4483. doi: 10.1136/bmj.g4483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ågren Per-Henrik. Operative versus nonoperative treatment of displaced intra-articular calcaneal fractures. J Bone Joint Surg Am. 2013 Aug 07;95:1351–1357. doi: 10.2106/JBJS.L.00759. [DOI] [PubMed] [Google Scholar]
- 14.Randle J.A., Kreder H.J., Stephen D. Should calcaneal fractures be treated surgically? A meta-analysis. Clin Orthop. 2000;377:217–227. doi: 10.1097/00003086-200008000-00029. [DOI] [PubMed] [Google Scholar]
- 15.Su Yanling, Chen Wei, Zhang Tao, Wu Xingwang, Wu Zhanpo, Zhang Yingze. Bohler's angle's role in assessing the injury severity and functional outcome of internal fixation for displaced intra-articular calcaneal fractures: a retrospective study. BMC Surg. 2013;13:40. doi: 10.1186/1471-2482-13-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Makki D., Alnajjar H.M., Walkay S., Ramkumar U., Watson A.J., Allen P.W. Osteosynthesis of displaced intra-articular fractures of the calcaneum. J Bone Jt Surg Br. 2010;92-B:693–700. doi: 10.1302/0301-620X.92B5.23542. [DOI] [PubMed] [Google Scholar]
- 17.Zwipp H, Tscherne H, Thermann, H, Osteosynthesis of displaced intraarticular fractures of the calcaneus results in 123 cases. Clin Orthop Relat Res 290:76–86. [PubMed]