

Abstract
Purpose of the study
This study seeks to explore methods for conducting economic evaluations alongside multinational trials by conducting a systematic review of the methods used in practice and the challenges that are typically faced by the researchers who conducted the economic evaluations.
Methods
A review was conducted for the period 2002 to 2012, with potentially relevant articles identified by searching the Medline, Embase and NHS EED databases. Studies were included if they were full economic evaluations conducted alongside a multinational trial.
Results
A total of 44 studies out of a possible 2667 met the inclusion criteria. Methods used for the analyses varied between studies, indicating a lack of consensus on how economic evaluation alongside multinational studies should be carried out. The most common challenge appeared to be related to addressing differences between countries, which potentially hinders the generalisability and transferability of results. Other challenges reported included inadequate sample sizes and choosing cost-effectiveness thresholds.
Conclusions
It is recommended that additional guidelines be developed to aid researchers in this area and that these be based on an understanding of the challenges associated with multinational trials and the strengths and limitations of alternative approaches. Guidelines should focus on ensuring that results will aid decision makers in their individual countries.
Introduction
Establishing whether new and existing health technologies provide value for money is becoming important internationally, and many countries now require evidence on cost-effectiveness for resource allocation decisions [1–2]. In the UK, the National Institute for Health and Care Excellence appraises health technologies in terms of their clinical effectiveness and cost-effectiveness [3], and economic evaluation, which is the comparison of alternatives in terms of costs and benefits, is one of the tools used for this purpose [4]. Economic evaluations have been conducted alongside trials mainly because they provide a means for collecting clinical and economic data simultaneously. One type of trial that has seen an increase in its popularity, owing to its ability to recruit participants rapidly and expedite the development of new health technologies, is the multinational trial, which is defined as a study that takes place in more than one country or jurisdiction [5–9].
One of the reasons for pooling/aggregating clinical data from cross-country studies is the belief that clinical and biological effects are homogenous across countries/jurisdictions [10]. However, the same cannot be said about economic data, owing to the vast differences in health systems, practice patterns, resource use and unit prices between countries, all of which need to be accounted for when conducting an economic evaluation [11–14]. Recent reviews of the literature revealed wide variation in the way these differences are addressed [15–16], indicating a lack of consensus among researchers. Availability of economic data in some countries also poses potential problems for researchers. A study conducted alongside a neurologic trial in 15 countries reported a dearth of unit cost information in some participating countries despite the efforts that were made to obtain these costs [17]. Generalisability (applying the results of a study to a number of countries without needing to adjust for interpretation) and transferability (adapting the results of a study to other countries) are other challenges that have been identified in the literature [18]. In principle, because of their very nature, results from cross-country studies should be more generalisable. However, it can be argued that pooled results cannot be applied to a single country owing to the inclusion of data from different jurisdictions [19]. A recent review of national guidelines on the use of data from multinational trials showed that there were vast differences in the data different countries considered to be generalisable or transferable to their settings [1], which indicates a lack of consensus among countries and which potentially limits the usefulness of cost-effectiveness estimates from multinational trials [19–20]. Resource allocation decisions are normally made at a national level [20–22], and thus there is the need to develop and agree on appropriate methods for conducting and interpreting economic analyses based on multinational trials. This would not only make results more useful to decision makers but also avoid the duplication of work in every country/jurisdiction [2].
A number of methods have been developed in response to the challenges outlined, ranging from very simple approaches such as adjusting resource use to very complex statistical approaches such as multilevel modelling [22]. The extent to which these methods have been used in practice is unclear. One study concluded that there is a need for more guidance as a result of the vast variation in methods that are being used to conduct economic analyses alongside multinational trials [15]. It is our belief that a study designed to assess the challenges reported by researchers could lead to a better understanding of the reasons methods vary and also help to develop additional guidance in this area. The objective of this study is to review published economic evaluations that were conducted alongside multinational trials with the aim of exploring methods that have been used and to outline researchers’ challenges i.e. any difficulties associated with the multinational nature of the trial. As far as we are aware, no other review has considered the challenges that have been reported by researchers who have conducted economic evaluations alongside multinational trials.
Materials and Methods
A systematic review was conducted following the guidelines of the Centre for Reviews and Disseminations (CRD) [23].
Inclusion and exclusion criteria
Studies were included if they were full economic evaluations based on multinational trials and reported an incremental cost-effectiveness ratio (ICER) or incremental net benefit. Studies were excluded if they were modelling studies or systematic reviews, did not use patient-level data or were not published in English.
Search strategy
The electronic databases searched were: MEDLINE, EMBASE and the National Health Service economic evaluation database (NHS EED). The search was limited to the period 2002 to 2012 for pragmatic reasons and to capture the most recent studies. The following keywords were used in the search: multinational, cost, cost-effectiveness, cost-utility, cost-benefit, multi-country, multi-centre, trial, economic evaluation, and cross-country (S1 Table). Following an approach used by Roberts and colleagues [24], a three-stage process was used to select relevant papers (S1 Text). The screening of papers was done by all reviewers. Stage one (categorization of studies) was carried out by one reviewer who initially screened titles and abstracts of articles and classified them into 5 groups. Stage 2 (further classification of studies) and stage 3 (application of the inclusion criteria) were carried out independently by all three reviewers (see S1 Text). Results from each reviewer were compared and any differences were resolved through consultation among all reviewers. The quality of the economic evaluations was not assessed because of the study objectives and the need to include as many studies as possible.
Data Extraction
Data were extracted using a predefined data extraction form (S2 Table), and the following data were extracted from the included studies: Type of economic evaluation, health outcomes considered, study perspective, number of countries included, analytical approach to the economic evaluation used and challenges faced.
Results
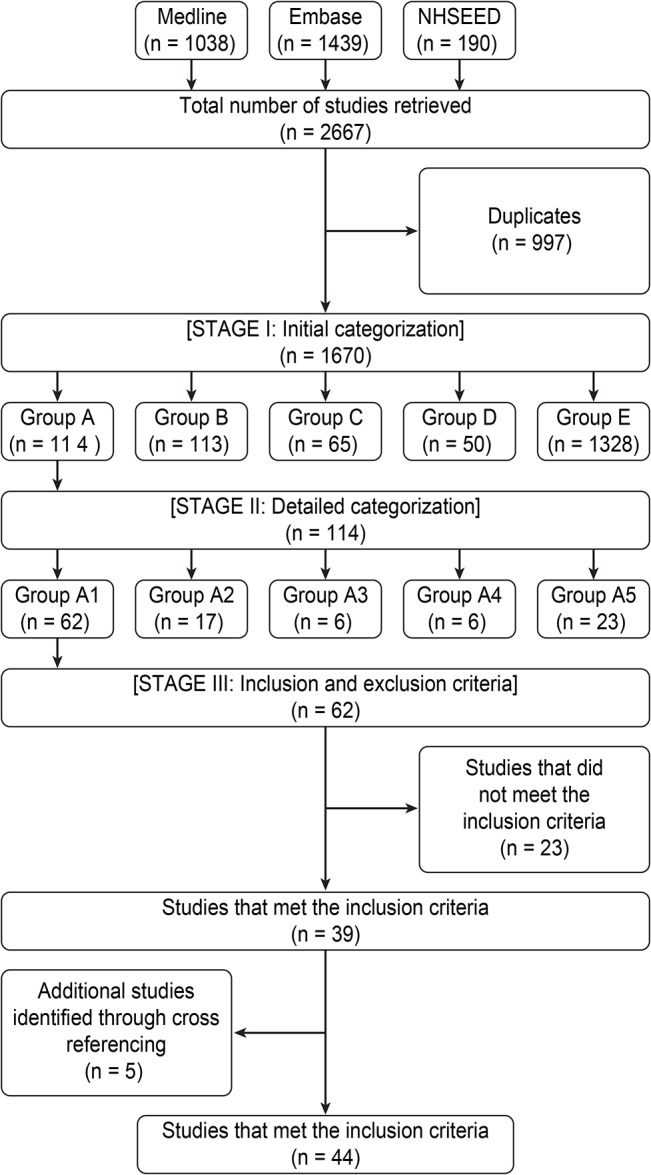
The database searches yielded 2667 articles. After accounting for duplicates, 997 were excluded. Inspecting the titles and abstracts of the remaining papers yielded 114 potentially relevant articles, of which 62 were classified as economic evaluations that reported an ICER or incremental net benefit. Of these, 39 met the inclusion criteria and the remaining 23 were excluded mainly because they were model-based (20 studies) or not relevant (3 studies). An additional 5 studies were identified through cross referencing. Forty-four studies were included in the final sample (Fig 1).
Fig 1. Literature search and selection.
Summary of selected studies
The types of economic evaluations were mainly cost-effectiveness analysis (31 studies) and cost-utility analysis (18 studies) (Table 1). Of these, 5 studies conducted both [25–29]. In one study, cost-utility analysis was performed as secondary analysis but an ICER was not estimated [25]. Sixteen studies were related to cardiovascular disease, representing a substantial proportion of the included papers. A total of 21 trials were placebo controlled (Table 2), with a common characteristic being their assessment of drug therapies. The number of countries included in an individual trial ranged from 2 to 48, and approximately 80% of studies included in the review recruited patients from the UK (S3 Table). Using World Bank classifications [30], we identified 38 high-income, 24 upper middle-income, 12 lower middle-income and only 5 low-income countries (S3 Table). Only 2 studies included participants from low-income countries: one that assessed interventions for preeclampsia [31] and another that evaluated a malaria intervention [32]. Studies that recruited patients from lower middle-income countries primarily assessed interventions for chronic obstructive pulmonary disorder and asthma [33–36].
Table 1. Summary of studies that met the inclusion criteria.
| Author/Year | Study aims | Number of countries included (Country EE was carried out) | Type of economic analysis | Health outcomes | EQ-5D Value set used | Study perspective | Analytic approach to the economic evaluation used | Country-specific results presented | Adjustments made to account for country variations | Discussed challenges associated with multinational studies |
|---|---|---|---|---|---|---|---|---|---|---|
| Canoui-Piotrine et al 2009 [25] | Assess the cost-effectiveness of sirolimus-eluting stents compared with bare metal stents. | 15 | Cost-effectiveness analysis and cost-utility analysis | Cost per target vessel revascularization avoided | N/A | Health service perspective | Fully split one-country costing | Yes | No | No |
| Glasziou et al 2010 [26] | Determine the cost-effectiveness of a fixed combination of perindopril and indapamide | 20 | Cost-effectiveness analysis and cost-utility analysis | Cost per death averted at 4.3 years average follow-up, cost per life year gained and cost per QALY | N/A | Healthcare purchaser perspective | Fully pooled one-country costing | Yes | Yes | Yes |
| Marcoff et al 2009 [27] | Examine the cost-effectiveness of enoxaparin compared with unfractioned heparin as adjunctive therapy for fibrinolysis | 48 | Cost-effectiveness analysis and cost utility analysis | Cost per life year gained and cost per QALY gained | N/A | Societal perspective | Fully pooled one-country costing | Yes | Yes Regression approach | Yes |
| Mittman et al 2009 [28] | Assess the cost-effectiveness of cetuximab in metastatic colorectal cancer | 2 | Cost-effectiveness and cost-utility analysis | Cost per life year gained and cost per QALY gained | N/A | Payer perspective (Canadian government) | Fully pooled one-country costing | No | No | Yes |
| Reed et al. 2004 [29] | Estimate the cost-effectiveness of zoledronic acid versus placebo for dressing skeletal complications in men with prostate cancer | 17 | Cost-effectiveness analysis and cost-utility analysis | Cost per skeletal complication avoided; cost per patient free of skeletal-related event and cost per QALY | N/A | Societal perspective | Fully pooled multi-country costing | No | Yesthrough currency conversion | Yes |
| Simon et al 2006 [31] | To assess the cost-effectiveness of using magnesium sulfate to prevent preeclampsia | 33 | Cost-effectiveness analysis | Cost per case of preeclampsia prevented | N/A | Treatment provider perspective (hospital) | Fully pooled multi-country costing | Yes region-/group-specific cost-effectiveness | Yes through currency conversion and country classification | Yes. |
| Lubell et al 2009 [32] | To explore the cost-effectiveness of artesunate versus quinine for the treatment of severe malaria | 4 | Cost-effectiveness analysis | Cost per death averted | N/A | Provider perspective | Fully pooled multi-country costing | Yes | Yes | Yes |
| Sullivan et al. 2003 [33] | Estimate the cost-effectiveness analysis of early intervention with budesonide in mild, persistent asthma | 32 | Cost-effectiveness analysis | Cost per symptom-free day | N/A | Healthcare payer and societal perspective | Fully pooled one-country costing | Yes | ||
| Briggs et al 2006 [34] | Estimate the cost-effectiveness of a single inhaler versus fluticasone proportionate in aiming for total control in asthma patients | 44 | Cost-utility analysis | Cost per QALY gained | Mapping | Health service perspective | Fully pooled one-country costing | Yes | Yes Regression approach | Yes |
| Briggs et al 2010 [35] | Inform decision makers about the cost-effectiveness of alternative COPD treatments | 42 | Cost-utility analysis | Cost per QALY gained | UK tariff | Not clear | Fully split multi-country costing | Yes region-specific | Yes | Yes |
| Lofdal et al 2005 [36] | Compare the healthcare costs and effects of budesonide/formoterol in a single inhaler with those of budesonide and formoterol monotherapies and placebo in patients with COPD | 15 | Cost-effectiveness analysis | Cost per avoided exacerbation | N/A | Healthcare payer perspective | Fully pooled one-country costing | No | Yes Followed study protocol rigorously in all countries | No |
| Bachert et al 2007 [37] | Assess the cost-effectiveness of grass allergen tablet compared with symptomatic medication for preventing seasonal grass pollen-induced rhinoconjunctivitis | 7 | Cost-utility analysis | Cost per QALY gained | UK tariff | Societal perspective | Fully split multi-country costing | Yes | No | Yes |
| Canonica et al 2007 [38] | Assess the cost-effectiveness of GRAZAX for preventing grass pollen-induced rhinoconjunctivitis | 8 | Cost-utility analysis | Cost per QALY gained | UK tariff | Societal perspective | Fully pooled multi-country costing | Yes | No | No |
| Fernandez et al 2005 [39] | Assess the relative cost-effectiveness of escitalopram compared with venlafaxine in patients with major depressive disorder | 8 | Cost-utility analysis | Cost per QALY gained | UK tariff | Payer perspective | Fully pooled multi-country costing | No | Yes Regression approach | Yes |
| Manca et al 2003 [40] | Assess the cost-effectiveness of tension-free vaginal tape compared with open burch colposuspension as a primary treatment for urodynamic stress incontinence | 2 | Cost-utility analysis | Cost per QALY gained | UK tariff | Health service perspective | Fully pooled one-country costing | No | No | |
| Garry et al. 2004 [41] | Evaluate the cost-effectiveness of laparoscopic, abdominal and vaginal hysterectomy | 2 | Cost-utility analysis | Cost per QALY gained | UK | UK NHS perspective | Fully pooled one-country costing | Yes | ||
| Nasser et al. 2008 [42] | To assess the cost-effectiveness of GRAZAX in patients with rhinoconjunctivitis and coexisting asthma | 8 | Cost-utility analysis | Cost per QALY gained | UK tariff | Societal perspective | Fully pooled one-country costing | Yes | No | No |
| Bracco et al 2007 [43] | Assess the cost-effectiveness of tegaserod in treating irritable bowel syndrome | Not stated | Cost-utility analysis | Cost per QALY gained | Appears to be UK tariff | Third-party payer perspective | Fully pooled one-country costing (check) | No | Yes Regression approach | Yes |
| Knapp et al 2008 [44] | Determine the cost-utility of treating schizophrenic patients with olanzapine compared with other antipsychotics | 10 | Cost-utility analysis | Cost per QALY gained | UK tariff | Health service perspective | Fully pooled one-country costing | No | Yes Regression approach | Yes |
| Buxton et al 2004 [46] | Assess the cost-effectiveness of early intervention with budesonide in mild asthma | 32 (Mentioned 8 in paper) | Cost-effectiveness analysis | Cost per symptom free day | N/A | Healthcare payer perspective and societal perspective | Partially split multi-country costing | Yes | Yes Used country-specific costs | Yes |
| Rutten Von Molken et al 2007 [47] | Assess the cost-effectiveness analysis of roflumilast for treating patients with severe chronic obstructive pulmonary disease | 14 | Cost-effectiveness analysis | Cost per exacerbation avoided | N/A | Societal and NHS perspectives | Fully pooled one-country costing | No | Yes through currency conversion | Yes |
| Willan et al 2006 [48] | Assess the cost-effectiveness of rivastigmine in patients with Parkinson’s disease dementia | 12 | Cost-utility analysis | Cost per QALY gained | N/A | Societal perspective | Fully pooled multi- country costing | Yes Regression approach | Yes | |
| Radeva et al 2005 [49] | Determine the cost-effectiveness of everolimus compared with azathioprine one year after de novo heart transplantation | 14 | Cost-effectiveness analysis | Cost per additional patient free of efficacy failure | N/A | Societal perspective | Fully pooled multi-country costing | No | Yes Regression approach | No |
| Edbrooke et al 2011 [50] | To assess the implications of intensive care unit triage decisions on patient mortality | 7 | Cost-effectiveness analysis | Cost per life-year saved and cost per life year | N/A | Not clear | Fully pooled multi-country costing | No | Yes Regression approach | Yes |
| Lamy et al 2004 [51] | Assess the cost-effectiveness of the use of clopidogrel in acute coronary syndromes | 28 | Cost-effectiveness analysis | Cost per CV death prevented | N/A | Societal perspective | Fully pooled multi-country costing | Yes | Yes Regression approach and event costs | Yes |
| Drummond et al 2003 [52] | Determine the cost-effectiveness of sequential i.v./po moxifloxacin therapy compared with i.v./po co-amoxiclav with or without clarithromycin in treating community-acquired pneumonia | 10 | Cost-effectiveness analysis | Cost per additional patient cured | N/A | Health service perspective | Fully pooled one country costing | Yes | Yes Regression approach | Yes |
| Gomes et al. 2010 [53] | Assess the cost-effectiveness of general versus local anesthesia for carotid surgery | 24 | Cost-effectiveness analysis | Cost per event-free day | N/A | Health service and personal social services | Fully pooled one-country costing | Yes | No | Yes |
| Lorgelly et al 2010 [55] | Assess the cost-effectiveness of rosuvastatin treatment in systolic heart failure | 21 | Cost-effectiveness analysis | Cost per major CV event avoided | N/A | Healthcare perspective | Fully pooled one-country costing | No | Yes Used event cost | Yes |
| Price et al 2002 [57] | Assess the cost-effectiveness of chlorofluorocarbon-free beclomethasone dipropionate in treating chronic asthma | 4 | Cost-effectiveness analysis | Cost per symptom free day | N/A | Healthcare provider | Fully pooled one-country costing | Yes appeared to be UK | Yes Adjusted resource use | Yes |
| Weintraub et al 2005 [58] | Assess the long-term cost-effectiveness of clopidogrel in patients with acute coronary syndromes | 28 | Cost-effectiveness analysis | Cost per life year gained | N/A | Societal perspective | Fully polled one-country costing | Yes | No | Yes |
| Wade et al 2008 [59] | Evaluate the cost-effectiveness of escitalopram versus duloxetine in treating major depressive disorder | 9 | Cost-effectiveness analysis | Change in Sheehan Disability Scale | N/A | Societal perspective | Fully pooled one-country costing | No | Yes Regression approach | Yes |
| Kolm 2007 [60] | Assess the cost-effectiveness of clopidogrel in acute coronary syndromes | 28 | Cost-effectiveness analysis | Cost per life year gained | N/A | Canadian health system | Fully pooled one-country costing | Yes | Yes | Yes |
| Jowett et al 2009 [61] | Assess the cost-effectiveness of computer-assisted anticoagulant dosage versus manual dosing in patients on long- or short-term oral anticoagulant therapy | 13 | Cost-effectiveness analysis | Cost per clinical event avoided | N/A | Healthcare perspective | Fully pooled one-country costing | No | No | Yes |
| Dukhovny et al 2011 [62] | Evaluate the cost-effectiveness of caffeine for apnea of prematurity | 9 | Cost-effectiveness analysis | Survival without bronchopulmonary dysplasia (BPD) or neurodevelopmental impairment (NDI) | N/A | Third-party payer perspective | Fully pooled one-country costing | No | Yes Regression approach | Yes |
| Annemans et al 2003 [81] | Assess the cost-effectiveness of recombinant urate oxidase in hematological cancer patients | 4 | Cost-effectiveness analysis | Cost per life year saved | N/A | Healthcare payer | Fully pooled multi-country costing | Yes | No | |
| Aspelin et al 2005 [82] | Assess the cost-effectiveness of iodixanol in patients at high risk of contrast-induced nephropathy | 5 | Cost-effectiveness analysis | Cost per adverse drug reaction avoided | N/A | Hospital perspective | Fully pooled one-country costing | Yes | No | |
| Bakhai et al. 2003 [83] | Evaluate the cost-effectiveness of coronary stenting and abciximab for patients with acute myocardial infarction | 9 | Cost-utility analysis | Cost per QALY gained | N/A | Third-party payer perspective | Fully split one-country costing | Yes | No | No |
| Brown et al. 2003 [84] | Establish the cost-effectiveness of eptifibatide treatment for acute coronary syndrome patients | 28 | Cost-effectiveness analysis | Cost per life year gained | N/A | Fully split one-country costing | Yes | No | No | |
| Janzon et al 2003 [85] | Assess the cost-effectiveness of extended treatment with low molecular weight heparin (dalteparin) in unstable coronary artery disease | 3 | Cost-effectiveness analysis | Cost per avoided death or myocardial infarction | N/A | Healthcare provider perspective | Fully pooled one-country costing | No | Yes Tested the impact of price differences between countries | No |
| Lamy et al 2003 [86] | Assess the cost implication of using ramipril in high-risk patients based on the heart outcomes prevention evaluation (HOPE) study | 19 | Cost-effectiveness analysis | Cost per primary event saved | N/A | Third-party payer perspective | Fully pooled one-country costing | Yes | No | No |
| Lindgren et al. 2005 [87] | Assess the cost-effectiveness of formoterol and salbutamol in patients with asthma | 24 | Cost-effectiveness analysis | Cost per avoided severe exacerbation | N/A | Healthcare payer perspective | Fully pooled multi-country costing | Yes | No | No |
| Martin et al 2003 [88] | Determine the cost-effectiveness of epoetin-Alfa versus placebo in stage IV breast cancer. | 15 | Cost-utility analysis | Cost per QALY gained | N/A | Health service perspective | Fully pooled one-country costing (Not clear) | No | No | No |
| Reed et al 2004 [89] | Assess the cost-effectiveness of valsartan in patients with chronic heart failure | 16 | Cost-effectiveness analysis | Cost per life year saved | N/A | Societal perspective | Fully pooled multi-country costing | No | Yes Used country-specific costing and other approaches | Yes |
| Welsch et al 2009 [90] | Cost-effectiveness of enoxaparin compared with unfractionated heparin in ST elevation myocardial infarction patients | 48 | Cost-effectiveness analysis | Cost per life year gained | NA | Fully pooled one-country costing | Yes | No | Yes |
I A fully pooled analysis is a study that relies on resource use and effectiveness data from all participating countries II A fully split analysis is one that relies on resource use and effectiveness from one or a subset of countries. III Partially split analysis relies on effectiveness data from all participating countries but relies on resource use data from one or a subset of countries. IV One-country costing applies the unit cost from one country V Multi-country costing applies unit costs from two or more participating countries.
Table 2. Specific characteristics of studies included in the review.
| Author | Placebo controlled trial | Provided sources of unit costs in each country | Currency used | |||
|---|---|---|---|---|---|---|
| Pounds | Euro | US dollar | Other | |||
| Canoui-Piotrine et al 2009 [25] | ✗ | ✗ | ✓ | |||
| Glasziou et al 2010 [26] | ✓ | ✗ | ✓ | |||
| Marcoff et al 2009 [27] | ✗ | ✗ | ✓ | |||
| Mittman et al 2009 [28] | ✗ | ✗ | ✓ | |||
| Reed et al 2004 [29] | ✓ | ✗ | ✓ | |||
| Simon et al 2006 [31] | ✓ | ✗ | ✓ | |||
| Lubell et al 2009 [32] | ✗ | ✗ | ✓ | |||
| Sullivan et al. 2003 [33] | ✗ | ✗ | ✓ | |||
| Briggs et al 2006 [34] | ✗ | ✗ | ✓ | |||
| Briggs et al 2010 [35] | ✓ | ✗ | ✓ | |||
| Lofdal et al 2005 [36] | ✓ | ✗ | ✓ | |||
| Bachert et al 2007 [37] | ✓ | ✓ | ✓ | |||
| Canonica et al 2007 [38] | ✓ | ✓ | ✓ | |||
| Fernandez et al 2005 [39] | ✗ | ✗ | ✓ | |||
| Manca et al 2003 [40] | ✗ | ✗ | ✓ | |||
| Garry et al. 2004 [41] | ✗ | ✗ | ✓ | |||
| Nasser et al. 2008 [42] | ✓ | ✗ | ✓ | |||
| Bracco et al 2007 [43] | ✓ | ✗ | ✓ | |||
| Knapp et al 2008 [44] | ✗ | ✗ | ✓ | |||
| Buxton et al 2004 [46] | ✓ | ✓ | ✓ | |||
| Rutten Von Molken et al 2007 [47] | ✓ | ✗ | ✓ | |||
| Willan et al 2006 [48] | ✓ | ✓ | ✓ | ✓ | ||
| Ra✓deva et al 2005 [49] | ✗ | ✗ | ✓ | |||
| Edbrooke et al 2011 [50] | ✗ | ✗ | ✓ | |||
| Lamy et al 2004 [51] | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ |
| Drummond et al 2003 [52] | ✗ | ✗ | ✓ | |||
| Gomes et al. 2010 [53] | ✗ | ✗ | ✓ | |||
| Lorgelly et al 2010 [55] | ✗ | ✗ | ✓ | |||
| Price et al 2002 [57] | ✗ | ✗ | ✓ | |||
| Weintraub et al 2005 [58] | ✓ | ✗ | ✓ | |||
| Wade et al 2008 [59] | ✗ | ✗ | ✓ | |||
| Kolm 2007 [60] | ✓ | ✗ | ✓ | |||
| Jowett et al 2009 [61] | ✗ | ✗ | ✓ | |||
| Dukhovny et al 2011 [62] | ✓ | ✗ | ✓ | |||
| Annemans et al 2003 [81] | ✗ | ✗ | ✓ | |||
| Aspelin et al 2005 [82] | ✗ | ✗ | ✓ | |||
| Bakhai et al. 2003 [83] | ✗ | ✗ | ✓ | |||
| Brown et al. 2003 [84] | ✗ | ✗ | ✓ | |||
| Janzon et al 2003[85] | ✓ | ✗ | ✓ | ✓ | ||
| Lamy et al 2003 [86] | ✓ | ✗ | ✓ | |||
| Lindgren et al. 2005 [87] | ✗ | ✗ | ✓ | |||
| Martin et al 2003 [88] | ✓ | ✗ | ✓ | |||
| Reed et al. 2004 [89] | ✓ | ✗ | ✓ | |||
| Welsch et al 2009 [90] | ✓ | ✗ | ✓ | |||
Health outcomes
Studies that adopted the CEA approach reported general outcomes such as cost per life year gained or used disease-specific outcome measures such as cost per cardiovascular event avoided. The quality adjusted life year (QALY) was the main outcome measure for those that used CUA; however, different methods were used to estimate QALYs. The main approach was to obtain responses to the EQ-5D questionnaire and use them to obtain health utilities (Table 1). Nine studies gave an indication of how they generated EQ-5D index scores [35, 37–44], and in all cases, the UK tariff [45] was used, mainly because it was well established [43], recommended [35] and readily available [44]. Only one study used the Health Utility Index to obtain QALYs [28]. Mapping was another approach used for this purpose; one study used a mapping algorithm to obtain QALYs from the Asthma Quality of Life Questionnaire [34].
Costing and study perspective
Twenty-eight studies applied unit costs from only one country to the data; the others applied unit costs from all or a subset of countries (Table 1). The average number (range) of countries per study was 17 (2 to 48) and 16 (4 to 42) for studies that adopted the one-country and multi-country approaches, respectively. One reason for adopting a one-country costing approach was the availability of good-quality data in countries such as the UK [44]. Most studies presented results from one perspective (health service/healthcare or societal) (Table 1), although three adopted multiple perspectives for the purpose of comparison [33,46–47]. The results obtained from the different perspectives were comparable [33,47], although one study had results that were sensitive to the perspective adopted [46]. In terms of what was considered societal costs, most studies included productivity losses using human capital [33, 37, 38, 42, 46] or friction costs approaches [47]. One study included caregiver time [48], whereas others were not explicit about what was included.
The level of detail given about the sources of unit costs varied from simply stating that official tariffs and retail prices in each country had been used [37] to providing detailed references of each country’s unit costs [25,46,48]. In most cases, it was unclear how costs had been obtained (Table 2). One approach to costing when unit costs were unavailable was to assume that countries were similar in terms of geographic proximity and level of development and apply the mean cost from countries that were assumed to be similar to the countries for which costs were not available [31,49]. In contrast, the market basket approach, which involves developing an index that reflects the relative costs of a basket of resources used in a pair of countries [17], was used in two studies [29,49]. Other approaches included using recognized international databases such as the WHO-CHOICE database [32], contacting local health economists and researchers through surveys that elicited unit cost information [29,49] and the top-down/macro-costing approach, which considers costs at an aggregate level [50]. This approach has been shown to be effective in cases when obtaining unit costs is not feasible [4]. Some studies used a combination of methods, such as using the market basket approach and contacting local researchers [29, 49]. In terms of presenting costs, the most common currencies used were the US dollar, the Euro and the UK pound, with one study [51] presenting its results using more than one currency (Table 2).
Analytical approach to economic evaluation
Based on a well-known classification system (S2 Text) [19], 26 studies were classified as fully pooled one-country costing, and 13 were fully pooled multi-country costing studies. Some studies adopted the fully split approach, with 60% of these using one-country costing. One study was classified as a partially split multi-country costing study (S4 Table). The justification for pooling data was that the sample size in some participating countries was too small [37,38], but only one study tested whether it was appropriate to pool data across countries [52].
Methods for addressing the multinational nature of the data and ensuring the generalisability and transferability of results
Estimating country-specific cost-effectiveness
Two studies used subgroup analysis within sensitivity analysis to estimate ICERs using only data from the country of interest [26,53], and in both cases, the results were similar to the main (pooled) analysis. A third study ignored data from all other countries and used data from only the country of interest [25]. Empirical Bayesian shrinkage, a method that involves borrowing strength from the overall trial to estimate country-specific cost-effectiveness [54], was used by only one study; however, the authors did not present the country-specific estimates [27]. The simplest approach was to state that the perspective of the analysis was related to a particular country and to apply unit costs from that country to the trial-wide data [34, 36, 37, 46, 52]. With regard to reporting the country-specific results, one study [51] reported the cost-effectiveness results in the country’s own currency, whereas other studies presented their results in currencies such as US dollars or Euros.
Regression methods
Multilevel modelling was used in three studies to account for the clustered nature of the data [27, 49, 50]. Other regression approaches such as controlling for country when estimating outcomes such as the QALY [43], adjusting for length of stay and costs within countries [51] and including interaction terms and country dummy variables [34,39,44,52] were also used. In one of the studies, the authors went further to test whether the country dummy variables were significant [39].
Other approaches
Event rather than daily costs were used to eliminate effects such as differences in lengths of stay across countries [51,55]. Close adherence to the study protocol [56] was also used to eliminate differences in practice patterns and resource use in different countries [36]. One study made assumptions about the number of visits per patient to reflect current guidelines and the UK Department of Health’s recommendations for the management of asthma [57].
Challenges associated with the economic evaluation of multinational trials
Potential challenges were discussed in 29 studies (Table 1), including:
Differences between countries
It was noted that there are numerous differences between countries but no accepted guidance on how to account for them [35, 46, 53]. These differences include: differences in resource use, prices, health systems and practice patterns [27–29,31,39,46,47,52,54,58–60]. Estimating country-specific cost-effectiveness was another area in which there is no consensus amongst researchers [35,46]. One study acknowledged this and outlined the advantages and disadvantages of some of the approaches that had been suggested in the literature [35].
Sample size and lack of data
Sample size problems were mentioned by some researchers, who noted that uneven recruitment across countries could potentially lead to unreliable cost-effectiveness estimates, especially in cases in which pooling data across all countries is not an option [31, 32, 35, 37, 46]. The lack of country-specific price weights/costs and the challenges associated with collecting data in multi-country studies were also highlighted in some studies [49, 59, 61]. Most often, the researchers conducting the economic analysis were based in one country and were unlikely to know the sources of unit costs in other countries. In addition, there is also a lack of good-quality data in some participating countries, particularly in developing countries [29, 44, 62]. One study was aware of the advantage of using country-specific price weights but went on to use price weights from only one country [62].
Additional challenges
The cost-effectiveness threshold, which represents society’s willingness to pay for an additional unit of benefit, is often used to determine whether an intervention is cost-effective [63]. However, with regard to analyzing multinational trials, researchers are faced with the problem of how to determine and choose the appropriate threshold [28, 34, 43, 46]. One study adopted a threshold of €50,000 per QALY but stated that the decision was based on what other studies had done in the past [43]. Another important issue relates to the generalisability of study findings. Two studies noted that owing to the multinational nature of the data, decision makers in various countries might face problems with making judgments about the cost-effectiveness of interventions in their own country/jurisdiction [29, 35]. Finally, only one study mentioned the choice of the EQ-5D tariff as a challenge [44].
Discussion
Summary of main findings
This review has assessed published economic evaluations that were conducted alongside multinational trials. The results indicate that most studies applied costs from one country but resource use from all countries, possibly owing to a lack of cost data in some countries or to the fact that researchers sought to inform decisions in a particular country. However, of the studies that reported results from a single country, 50% of them applied one-country costing. The major problem that has been associated with this approach is the possibility of overestimating or underestimating costs [19, 22, 64].
Most studies did not give reasons for having pooled resource use and effectiveness data, although it can be inferred that increasing sample size is a possible motivation for this. One study did test for heterogeneity and homogeneity before pooling data [53]. With regard to pooling resource use, unless the study protocol is followed rigidly, issues related to practice patterns across countries could potentially affect the analysis [19]. However, it should be noted that although protocols have the potential to reduce differences in treatment patterns across countries, they do not necessarily dictate all care provided.
The UK tariff was used in all studies that used the EQ-5D questionnaire to elicit information on health-related quality of life, and although its widespread use can be attributed to its availability [35, 43, 44], it is also possible that other tariffs such as the EU tariff, which was derived from 6 countries, were not used because they are based on the visual analogue scale (VAS). Although some researchers believe that the VAS should not be used in resource allocation decisions because the values obtained are not considered to be utilities [65–67], current research is exploring the predictive value of the EQ-VAS for EQ-5D utilities [68]. In addition to this, most of the studies that used the UK tariff over the EU tariff were published after 2003, the year the EU tariff was published. This supports the findings from other research papers that the UK tariff is most often used [67]. The choice of the EQ-5D tariff is important because different tariffs could lead to conflicting results [69], and the EuroQol group’s current guidance states that the most relevant should be used [70]. However, when the study is multinational, it is difficult to determine the most relevant tariff, and thus, there is a need for further research. A recent study has suggested that researchers explore the potential for different results using all appropriate tariffs within sensitivity analyses [71].
A number of studies made some form of adjustment to the data to account for the multinational nature; however, the methods used varied, indicating that methods have not been standardized in this area. With regard to studies that looked at country-specific results, only one study explicitly stated that the reason for doing this was the important role of health economics in policy making [46]. The most common method of obtaining country-specific estimates was fully pooled one-country costing. Current recommendations by the ISPOR taskforce suggest that the more complex methods such as hierarchical modeling should be used for the analysis of multinational trial data [18] and a recent study also concluded that Bayesian hierarchical models are the most appropriate for estimating country-specific cost-effectiveness [22]; however, only one study in this review used this approach [27], suggesting that researchers are not adhering to existing guidelines, possibly because of the complexity associated with implementing this approach. Bayesian hierarchical models have been challenged because it assumes that differences between countries are random, whereas in reality, these differences are systematic [72].
The multinational nature of the data was acknowledged by most studies, but not all listed the countries that were included, and some merely reported the number of countries in the trial. This may be attributable to word limits imposed by journals. In most cases, it was not clear whether the study was attempting to estimate general or country-specific results, primarily as a result of inadequate reporting. With respect to unit costs, we found that the sources of the costs were not stated in most cases. This is of great concern because this information would enable researchers and decision makers to judge the validity of the study and whether it was applicable to their own settings and also help other researchers identify unit cost sources. It is therefore advisable that future multinational studies include unit cost sources, and if assumptions about the unit costs were made, this should also be made explicit. This review also found that recruitment is biased towards developed countries, which may reflect the difficulties associated with recruiting patients and the lack of high-quality data in low-income countries [44].
Comparison with other studies
Other reviews have looked at economic evaluations alongside multinational trials and obtained results similar to what was found in our study. One study found that reporting on economic evaluations of multinational trials is inadequate [16], another found that methods of analysis differed between studies [15] and a recent review reported that the uptake of the more complicated methods for estimating country-specific cost-effectiveness is slow [73].
Strengths and limitations of the study
As with any systematic review, there is the possibility that some articles may have been missed. However, we made the best attempt to identify all possible studies by developing the search strategy with advice from an information specialist. The key strength of this study is that it documented the challenges that have been reported by researchers who have conducted economic evaluations of clinical trials, and no other systematic review of multinational trials has done this.
Implications for current practice and future research
The most frequently mentioned challenge was the differences between countries, which could possibly affect the generalisability of study findings. Most clinical results from multinational trials are generalisable to the countries that participated in the study. However, results from economic evaluations are not easily generalisable [1] because there are differences in economic circumstances and differences in health systems across various countries. Hence, there is the need to consider these issues when countries are being included in trials. However, the requirements for economic evaluation/analysis are not given prominence when countries are being chosen for inclusion in multinational trials, and country selection is based on factors such as convenience [2,22]. Research is ongoing regarding selecting centres for multi-centre clinical trials [74], but this research needs to be extended to selecting countries in multinational trials as well because the countries included in a study could potentially determine the extent to which the study results are generalisable. In addition, a very important finding is that different methods were used by different studies for costing and addressing differences between countries. This is an indication that guidance similar to that which has been developed for standard economic evaluations needs to be developed. Although it can be argued that data from multinational trials may only serve as inputs into decision models which are used in resource allocation decisions at the national level, there is still the need to develop methods that would ensure that these inputs can be made more generalisable and transferable to individual country contexts when the need arises.
A possible solution to the problem of generalisability and transferability is the use of checklists to ensure that the results meet the required standards [75–78]. However, a possible limitation is the fact that individual items on checklists are sometimes equally weighted [79]. Another suggestion is for researchers to conduct economic evaluations using multiple perspectives. For example, the results of a study that considers both a health service and societal perspective may be useful for decision making in both the UK and the Netherlands.
There is evidence from this study that most researchers are aware of some of the issues surrounding economic evaluation alongside multinational trials, but they did not offer solutions to these challenges in most cases. Researchers should therefore endeavor to document the challenges they face to guide future research. The main challenge we identified was how to address the differences between countries, which could be attributed to a lack of consensus on many aspects such as how to estimate country-specific cost-effectiveness. Future research should therefore focus on reaching a consensus about how to address the challenges associated with multinational trials.
Conclusion
Despite the difficulties associated with multinational studies, their frequency will increase [80]. It is clear that conducting an economic evaluation in every country/jurisdiction is not feasible or efficient, and decision makers are likely to have to resort in some cases to considering results from other countries/jurisdictions to inform their local decision making despite the obvious limitations. Conducting economic evaluations alongside multinational trials is not trivial, and there should be a conscious effort by all stakeholders to constantly improve methodology in this area. We suggest that additional guidelines be developed to aid in using a consistent approach in this area, and this should be based on understanding the challenges associated with multinational trials and comparing alternative approaches. The guidelines should also be focused on ensuring that results can be useful to decision makers in individual countries.
Supporting Information
(DOCX)
(DOCX)
(DOCX)
(DOCX)
(DOCX)
(DOCX)
(DOCX)
Data Availability
All relevant data are within the paper and its Supporting Information files.
Funding Statement
The authors have no support or funding to report.
References
- 1. Barbieri M, Drummond M, Rutten F, Cook J, Glick H, Lis J, et al. (2010) What do international pharmacoeconomic guidelines say about economic data transferability? Value Health 13: 1028–1037 10.1111/j.1524-4733.2010.00771.x [DOI] [PubMed] [Google Scholar]
- 2. Drummond M, Manca A, Sculpher M (2005) Increasing the generalizability of economic evaluations: recommendations for the design, analysis, and reporting of studies. Int J Technol Assess Health Care 21: 165–171 [PubMed] [Google Scholar]
- 3.National Institute for Health and Care Excellence Guide to the methods of technology appraisal 2013 Available: http://www.nice.org.uk/media/D45/1E/GuideToMethodsTechnologyAppraisal2013.pdf [PubMed]
- 4. Morris S, Devlin N, Parkin D (2007) Economic analysis in health care Chichester; John Wiley and Sons; [Google Scholar]
- 5. Marschner IC (2010) Regional differences in multinational clinical trials: anticipating chance variation. Clin Trials 7: 147–156 10.1177/1740774510361974 [DOI] [PubMed] [Google Scholar]
- 6. Cook JR, Drummond M, Glick H, Heyse JF (2003) Assessing the appropriateness of combining economic data from multinational clinical trials. Stat Med 22: 1955–1976 [DOI] [PubMed] [Google Scholar]
- 7. Drummond M, Pang F (2001) Transferability of economic evaluation results; Drummond M, McGuire A. Economic evaluation in health care: merging theory with practice New York; Oxford University Press. [Google Scholar]
- 8. Mulligan JA, Fox-Rushby J. (2005) Transferring cost-effectiveness data across space and time Fox-Rushby J and Cairns J, Economic Evaluation (Understanding Public Health) London; Open University Press. [Google Scholar]
- 9. Wild D, Eremenco S, Mear I, Martin M, Houchin C, Gawlicki M, et al. (2009) Multinational trials-recommendations on the translations required, approaches to using the same language in different countries, and the approaches to support pooling the data: the ISPOR patient-reported outcomes translation and linguistic validation good research practices task force report. Value Health 12: 430–440 10.1111/j.1524-4733.2008.00471.x [DOI] [PubMed] [Google Scholar]
- 10. Yusuf S, Collins R, Peto R (1984) Why do we need some large simple randomized trials? Statistics in Medicine 3: 409–422 [DOI] [PubMed] [Google Scholar]
- 11. Koopmanscap MA, Touw KCR, Rutten FFH (2001). Analysis of cost and cost-effectiveness in multinational trials. Health Policy 58: 175–186 [DOI] [PubMed] [Google Scholar]
- 12. Knies S, Evers SMMA, Candel MJJM, Severens JL, Ament AJHA (2009) Utilities of the EQ-5D transferable or not? Pharmacoeconomics 27: 767–779 10.2165/11314120-000000000-00000 [DOI] [PubMed] [Google Scholar]
- 13. Magnell C, Brown L, Moskowitz A, Gelijns A (2005) Health care evaluation: issues in transferability In: Project TOH, eds. Health technologies and decision making. Paris: OECD; [Google Scholar]
- 14. Thompson SG, Nixon RM, Grieve R (2006). Addressing the issues that arise in analysing multicentre cost data, with application to a multinational study. Journal of Health Economics, 25: 1015–1028 [DOI] [PubMed] [Google Scholar]
- 15. Torti FM Jr, Reed SD, Schulman KA (2006) Analytic considerations in economic evaluations of multinational cardiovascular clinical trials. Value Health, 9: 281–291 [DOI] [PubMed] [Google Scholar]
- 16. Rivero-Arias O, Gray A (2010) The multinational nature of cost-effectiveness analyses alongside multinational clinical trials. Value Health, 13: 34–41 10.1111/j.1524-4733.2009.00582.x [DOI] [PubMed] [Google Scholar]
- 17. Schulman K, Burke J, Drummond M, Davies L, Carlsson P, Gruger J, et al. (1998) Resource costing for multinational neurologic clinical trials: Methods and results Health Econ 7: 629–638 [DOI] [PubMed] [Google Scholar]
- 18. Drummond M, Barbieri M, Cook J, Glick HA, Lis J, Farzana M (2009) Transferability of economic evaluations across jurisdictions: ISPOR Good Research Practices Task Force report. Value Health, 12: 409–418 10.1111/j.1524-4733.2008.00489.x [DOI] [PubMed] [Google Scholar]
- 19. Reed SD, Anstrom KJ, Bakhai A, Briggs AH, Califf RM, Cohen DJ, et al. (2005) Conducting economic evaluations alongside multinational clinical trials: toward a research consensus. Am Heart J, 149: 434–443 [DOI] [PubMed] [Google Scholar]
- 20. Reinhold T, Bruggenjurgen B, Schlander M, Rosenfeld S, Hessel F, Willich SN, et al. (2010). Economic analysis based on multinational studies: methods for adapting findings to national contexts. J Publ Health 18: 327–335 [Google Scholar]
- 21. Willke RJ, Glick HA, Polsky D, Schulman K (1998). Estimating country specific cost-effectiveness from multinational clinical trials. Health Econ, 7: 481–493 [DOI] [PubMed] [Google Scholar]
- 22. Manca A, Sculpher MJ, Goeree R (2010) The analysis of multinational cost-effectiveness data for reimbursement decisions: a critical appraisal of recent methodological developments. PharmacoEconomics, 28: 1079–1096 10.2165/11537760-000000000-00000 [DOI] [PubMed] [Google Scholar]
- 23. Centre for Reviews and Dissemination University of York. Systematic reviews: CRD's guidance for undertaking reviews in health care Centre for Reviews and Dissemination, University of York, 2009. Available: http://www.york.ac.uk/inst/crd/pdf/Systematic_Reviews.pdf [Google Scholar]
- 24. Roberts T, Henderson J, Mugford M, Bricker L, Neilson J (2002) Antenatal ultrasound screening for fetal abnormalities: a systematic review of studies of cost and cost effectiveness. Br J Obstet Gynaecol, 109: 44–56 [DOI] [PubMed] [Google Scholar]
- 25. Canoui-Poitrine F, Jeanblanc G, Alberti C, Armoogum P, Cebrian A (2009) Cost effectiveness of sirolimus-eluting stents compared with bare metal stents in acute myocardial infarction: insights from the TYPHOON trial. Appl Health Econ Health Policy 7: 19–29 10.2165/00148365-200907010-00003 [DOI] [PubMed] [Google Scholar]
- 26. Glasziou PP, Clarke P, Alexander J, Rajmokan M, Beller E (2010) Cost-effectiveness of lowering blood pressure with a fixed combination of perindopril and indapamide in type 2 diabetes mellitus: an ADVANCE trial-based analysis. Med J Aust 193: 320–324 [DOI] [PubMed] [Google Scholar]
- 27. Marcoff L, Zhang Z, Zhang W, Ewen E, Jurkovitz C (2009) Cost effectiveness of enoxaparin in acute ST-segment elevation myocardial infarction: the ExTRACT-TIMI 25 (Enoxaparin and Thrombolysis Reperfusion for Acute Myocardial Infarction Treatment-Thrombolysis In Myocardial Infarction 25) study. J Am Coll Cardiol, 54: 1271–1279 10.1016/j.jacc.2009.05.060 [DOI] [PubMed] [Google Scholar]
- 28. Mittmann N, Au HJ, Tu D, O'Callaghan CJ, Isogai PK, Karapetis CS, et al. (2009). Prospective cost-effectiveness analysis of cetuximab in metastatic colorectal cancer: evaluation of National Cancer Institute of Canada Clinical Trials Group CO. 17 trial. J Natl Cancer Inst, 101: 1182–1192 10.1093/jnci/djp232 [DOI] [PubMed] [Google Scholar]
- 29. Reed SD, Radeva IJ, Glendenning GA, Saad F, Schulman KA (2004). Cost-effectiveness of zoledronic acid for the prevention of skeletal complications in patients with prostate cancer. Journal of Urology, 171: 1537–1542 [DOI] [PubMed] [Google Scholar]
- 30.The World Bank Data (2012). Available: http://data.worldbank.org/news/newest-country-classifications-released
- 31. Simon J, Gray A, Duley L, & Magpie Trial Collaborative Group (2006) Cost-effectiveness of prophylactic magnesium sulphate for 9996 women with pre-eclampsia from 33 countries: economic evaluation of the Magpie Trial. Br J Obstet Gynaecol 113: 144–151 [DOI] [PubMed] [Google Scholar]
- 32. Lubell Y, Yeung S, Dondorp AM, Day NP, Nosten F, Tjitra E, et al. (2009) Cost-effectiveness of artesunate for the treatment of severe malaria. Trop Med Int Health, 14: 332–337 10.1111/j.1365-3156.2009.02227.x [DOI] [PubMed] [Google Scholar]
- 33. Sullivan SD, Buxton M, Andersson LF, Lamm CJ, Liljas B (2003) Cost-effectiveness analysis of early intervention with budesonide in mild persistent asthma. J Allergy Clin Immunol 112: 1229–1236 [DOI] [PubMed] [Google Scholar]
- 34. Briggs AH, Bousquet J, Wallace MV, Busse WW, Clark TJ, Pedersen SE, et al. (2006) Cost-effectiveness of asthma control: an economic appraisal of the GOAL study. Allergy 61: 531–536 [DOI] [PubMed] [Google Scholar]
- 35. Briggs AH, Glick HA, Lozano-Ortega G, Spencer M, Calverley PMA, Jones PW, et al. (2010) Is treatment with ICS and LABA cost-effective for COPD? Multinational economic analysis of the TORCH study. Eur Respir J 35: 532–539 10.1183/09031936.00153108 [DOI] [PubMed] [Google Scholar]
- 36. Lofdahl CG, Ericsson A, Svensson K, Andreasson E (2005) Cost effectiveness of budesonide/formoterol in a single inhaler for COPD compared with each monocomponent used alone. PharmacoEconomics, 23: 365–375 [DOI] [PubMed] [Google Scholar]
- 37. Bachert C, Vestenbaek U, Christensen J, Griffiths UK, Poulsen PB,(2007) Cost-effectiveness of grass allergen tablet (GRAZAX) for the prevention of seasonal grass pollen induced rhinoconjunctivitis—A Northern European perspective. Clin Exp Allergy 37: 772–779 [DOI] [PubMed] [Google Scholar]
- 38. Canonica GW, Poulsen PB, Vestenbaek U (2007) Cost-effectiveness of GRAZAX for prevention of grass pollen induced rhinoconjunctivitis in Southern Europe. Respir Med 101: 1885–1894 [DOI] [PubMed] [Google Scholar]
- 39. Fernandez JL, Montgomery S, Francois C (2005) Evaluation of the cost effectiveness of escitalopram versus venlafaxine XR in major depressive disorder. PharmacoEconomics, 23: 156–167 [DOI] [PubMed] [Google Scholar]
- 40. Manca A, Sculpher MJ, Ward K, Hilton P (2003) A cost-utility analysis of tension-free vaginal tape versus colposuspension for primary urodynamic stress incontinence. Br J Obstet Gynaecol 110: 255–262 [PubMed] [Google Scholar]
- 41. Garry R, Fountain J, Brown J, Manca A, Mason S (2004) EVALUATE hysterectomy trial: a multicentre randomised trial comparing abdominal, vaginal and laparoscopic methods of hysterectomy. Health Technol Assess (Winchester, England), 8: 1–154 [DOI] [PubMed] [Google Scholar]
- 42. Nasser S, Vestenbaek U, Beriot-Mathiot A, Poulsen PB (2008) Cost-effectiveness of specific immunotherapy with Grazax in allergic rhinitis co-existing with asthma. Allergy 63: 1624–1629 10.1111/j.1398-9995.2008.01743.x [DOI] [PubMed] [Google Scholar]
- 43. Bracco A, Jonsson B, Ricci JF, Drummond M, Nyhlin H (2007) Economic evaluation of tegaserod vs placebo in the treatment of patients with irritable bowel syndrome: an analysis of the TENOR study. Value Health 10: 238–246 [DOI] [PubMed] [Google Scholar]
- 44. Knapp M, Windmeijer F, Brown J, Kontodimas S, Tzivelekis S (2008) Cost-utility analysis of treatment with olanzapine compared with other antipsychotic treatments in patients with schizophrenia in the pan-European SOHO study. PharmacoEconomics 26: 341–358 [DOI] [PubMed] [Google Scholar]
- 45.Dolan P. Modeling valuations for EuroQol health states. Med Care 1997; 1095–108 [DOI] [PubMed]
- 46. Buxton MJ, Sullivan SD, Andersson LF, Lamm C, Liljas B, Busse WW, et al. (2004) Country-specific cost-effectiveness early intervention with budesonide in mild asthma. Eur Respir J 24: 568–574 [DOI] [PubMed] [Google Scholar]
- 47. Rutten-van Molken MP, Van Nooten FE, Lindemann M, Caeser M, Calverley PM (2007) A 1-year prospective cost-effectiveness analysis of roflumilast for the treatment of patients with severe chronic obstructive pulmonary disease. PharmacoEconomics, 25: 695–711 [DOI] [PubMed] [Google Scholar]
- 48. Willan AR, Goeree R, Pullenayegum EM, McBurney C, Blackhouse G (2006) Economic evaluation of rivastigmine in patients with Parkinson's disease dementia. PharmacoEconomics, 24: 93–106 [DOI] [PubMed] [Google Scholar]
- 49. Radeva JI, Reed SD, Kalo Z, Kauf TL, Cantu E, Cretin N, et al. (2005) Economic evaluation of everolimus vs azathioprine at one year after de novo heart transplantation. Clin Transplant 19: 122–129 [DOI] [PubMed] [Google Scholar]
- 50. Edbrooke DL, Minelli C, Mills GH, Iapichino G, Pezzi A, Corbella D, et al. (2011) Implications of ICU triage decisions on patient mortality: a cost-effectiveness analysis. Crit Care, 15: R56 10.1186/cc10029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Lamy A, Jonsson B, Weintraub WS, Zhao F, Chrolavicius S, Bakhai A, et al. (2004) The cost-effectiveness of the use of clopidogrel in acute coronary syndromes in five countries based upon the CURE study. Eur J Cardiovas Prevent Rehab, 11: 460–465 [DOI] [PubMed] [Google Scholar]
- 52. Drummond MF, Becker DL, Hux M, Chancellor JV, Duprat-Lomon I, Kubin R, et al. (2003) An economic evaluation of sequential i.v./po moxifloxacin therapy compared to i.v./po co-amoxiclav with or without clarithromycin in the treatment of community-acquired pneumonia. Chest, 124: 526–535 [DOI] [PubMed] [Google Scholar]
- 53. Gomes M, Soares MO, Dumville JC, Lewis SC, Torgerson DJ, Bodenham AR, et al. (2010) Cost-effectiveness analysis of general anaesthesia versus local anaesthesia for carotid surgery (GALA Trial). Br J Surg 97: 1218–1225 10.1002/bjs.7110 [DOI] [PubMed] [Google Scholar]
- 54. Manca A, Lambert PC, Sculpher M, Rice N (2007) Cost-effectiveness analysis using data from multinational trials: The use of bivariate hierarchical modelling Med Decis Making 27: 471–490 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Lorgelly PK, Briggs AH, Wedel H, Dunselman P, Hjalmarson A, Kjekshus J, et al. (2010) An economic evaluation of rosuvastatin treatment in systolic heart failure: evidence from the CORONA trial. Eur J Heart Failure, 12: 66–74 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Grieve R, Nixon R, Thompson SG, Normand C (2005) Using multilevel models for assessing the variability of multinational resource use and cost data Health Econ 14: 185–196 [DOI] [PubMed] [Google Scholar]
- 57. Price D, Haughney J, Duerden M, Nicholls C, Moseley C (2002) The cost effectiveness of chlorofluorocarbon-free beclomethasone dipropionate in the treatment of chronic asthma: a cost model based on a 1-year pragmatic, randomised clinical study. PharmacoEconomics, 20: 653–664 [DOI] [PubMed] [Google Scholar]
- 58. Weintraub WS, Mahoney EM, Lamy A, Culler S, Yuan Y, Caro J (2005). Long-term cost-effectiveness of clopidogrel given for up to one year in patients with acute coronary syndromes without ST-segment elevation. J Am Coll Cardiol 45: 838–845 [DOI] [PubMed] [Google Scholar]
- 59. Wade AG, Fernandez JL, Francois C, Hansen K, Danchenko N, Despiege N, et al. (2008) Escitalopram and duloxetine in major depressive disorder: a pharmacoeconomic comparison using UK cost data. PharmacoEconomics, 26: 969–981 [DOI] [PubMed] [Google Scholar]
- 60. Kolm P, Yuan Y, Veledar E, Mehta SR, O'Brien JA, Weintraub WS, et al. (2007) Cost-effectiveness of clopidogrel in acute coronary syndromes in Canada: a long-term analysis based on the CURE trial. Can J Cardiol 23: 1037–1042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Jowett S, Bryan S, Poller L, van den Besselaar AM, van derMeer FJM Palareti G, et al. (2009) The cost-effectiveness of computer-assisted anticoagulant dosage: results from the European Action on Anticoagulation (EAA) multicentre study. J Thrombosis and Haemostasis, 7: 1482–1490 [DOI] [PubMed] [Google Scholar]
- 62. Dukhovny D, Lorch SA, Schmidt B, Doyle LW, Kok JH, Roberts RS, et al. (2011) Economic evaluation of caffeine for apnea of prematurity. Pediatrics, 127: e146–e155 10.1542/peds.2010-1014 [DOI] [PubMed] [Google Scholar]
- 63. Appleby J, Devlin N, Parkin D (2007) NICE's cost effectiveness threshold. BMJ, 335: (7616) 358 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Glick HA, Doshi JA, Sannad SS, Polsky D (2007) Economic evaluation in clinical trials Oxford: University Press Oxford; [Google Scholar]
- 65. Torrance GW (1986) Measurement of health state utilities for economic appraisal: a review. J Health Econ, 5: 1–30 [DOI] [PubMed] [Google Scholar]
- 66. King JT, Tsevat J, Lave JR, Roberts MS (2005) Willingness to pay for a quality-adjusted life year: implications for societal health care resource allocation. Med Decis Making 25: 667–677 [DOI] [PubMed] [Google Scholar]
- 67. Sakthong P, Charoenvisuthiwongs R, Shabunthom R (2008) A comparison of EQ-5D index scores using the UK, US, and Japan preference weights in a Thai sample with type 2 diabetes. Health Qual Life Outcomes, 6: 71 10.1186/1477-7525-6-71 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. Feng Y, Parkin D, Devlin NJ (2014) Assessing the performance of the EQ-VAS in the NHS PROMs programme. Quality of Life Research, 23(3) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Bernert S, Fernandez A, Haro JM, Konig HH, Alonso J, Vilagut G (2009) Comparison of different valuation methods for population health status measured by the EQ-5D in three European countries. Value Health, 12: 750–758 10.1111/j.1524-4733.2009.00509.x [DOI] [PubMed] [Google Scholar]
- 70. Szende A, Oppe M, de Charro F (2007) Comparative review of time trade-off value sets Szende A, Oppe M, Devlin N EQ-5D value sets comparative review and user guide Springer; 2007. [Google Scholar]
- 71. Oppong R, Kaambwa B, Nuttall J, Hood K, Smith RD, Coast J (2013) The impact of using different tariffs to value EQ-5D health state descriptions: an example from a study of acute cough/lower respiratory tract infections in seven countries. The Eur J Health Econ 14: 197–209 [DOI] [PubMed] [Google Scholar]
- 72. Manca A, Rice N, Sculpher MJ, Briggs AH (2005) Assessing generalisability by location in trial-based cost-effectiveness analysis: The use of multilevel models Health Econ 2005; 14: 471–485 [DOI] [PubMed] [Google Scholar]
- 73. Vemer P, Rutten-van Molken (2013) The road not taken: transferability issues in multinational trials PharmacoEconomics 31: 863–876 10.1007/s40273-013-0084-z [DOI] [PubMed] [Google Scholar]
- 74. Gheorghe A, Roberts TE, Ives JC, Fletcher BR, Calvert M (2013) Centre selection for clinical trials and the generalisability of results: A mixed methods study PLoS ONE 8: e56560 10.1371/journal.pone.0056560 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Heyland DK, Kernerman P, Gafni A, Cook DJ (1996) Economic evaluations in the critical care literature: do they help us improve the efficiency of our unit? Crit Care Med, 24: 1591–1598 [DOI] [PubMed] [Google Scholar]
- 76. Spath HM, Carrere MO, Fervers B, Philip T (1999) Analysis of the eligibility of published economic evaluations for transfer to a given health care system: methodological approach and application to the French health care system. Health Policy, 49: 161–177 [DOI] [PubMed] [Google Scholar]
- 77. Welte R, Feenstra T, Jager H, Leidl R (2004) A decision chart for assessing and improving the transferability of economic evaluation results between countries. PharmacoEconomics, 22: 857–876 [DOI] [PubMed] [Google Scholar]
- 78. Antonanzas F, Rodriguez-Ibeas R, Juarez C, Hutter F, Lorente R, Pinillos M (2009) Transferability indices for health economic evaluations: methods and applications. Health Econ, 18: 629–643 10.1002/hec.1397 [DOI] [PubMed] [Google Scholar]
- 79. Nixon J, Rice S, Drummond M, Boulenger S, Ulmann P, de Pouvourville G (2009) Guidelines for completing the EURONHEED transferability information checklists. The Eur J Health Econ 10: 157–165 [DOI] [PubMed] [Google Scholar]
- 80. Pang F (2002) Design, analysis and presentation of multinational economic studies: The need for guidance. PharmacoEconomics, 20: 75–90 [DOI] [PubMed] [Google Scholar]
- 81. Annemans L, Moeremans K, Lamotte M, Garcia CJ, van den Berg H, Myint H, et al. (2003) Pan-European multicentre economic evaluation of recombinant urate oxidase (rasburicase) in prevention and treatment of hyperuricaemia and tumour lysis syndrome in haematological cancer patients. Support Care Cancer, 11: 249–257 [DOI] [PubMed] [Google Scholar]
- 82. Aspelin P, Aubry P, Fransson SG, Strasser R, Willenbrock R, Lundkvist J (2005) Cost-effectiveness of iodixanol in patients at high risk of contrast-induced nephropathy. Am Heart J 149: 298–303 [DOI] [PubMed] [Google Scholar]
- 83. Bakhai A, Stone GW, Grines CL, Murphy SA, Githiora L, Berezin RH, et al. (2003) Cost-effectiveness of coronary stenting and abciximab for patients with acute myocardial infarction: results from the CADILLAC (Controlled Abciximab and Device Investigation to Lower Late Angioplasty Complications) trial. Circulation, 108: 2857–2863 [DOI] [PubMed] [Google Scholar]
- 84. Brown R, Armstrong P (2003) Cost effectiveness in Canada of eptifibatide treatment for acute coronary syndrome patients using PURSUIT subgroup analysis. Can J Cardiol 19: 161–166 [PubMed] [Google Scholar]
- 85. Janzon M, Levin LA, Swahn E (2003) Cost effectiveness of extended treatment with low molecular weight heparin (dalteparin) in unstable coronary artery disease: results from the FRISC II trial. Heart, 89: 287–292 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Lamy A, Yusuf S, Pogue J, Gafni A (2003) Cost implications of the use of ramipril in high-risk patients based on the Heart Outcomes Prevention Evaluation (HOPE) study. Circulation, 107: 960–965 [DOI] [PubMed] [Google Scholar]
- 87. Lindgren B, Sears MR, Campbell M, Villasante C, Huang S., Lindh A, et al. (2005) Cost-effectiveness of formoterol and salbutamol as asthma reliever medication in Sweden and in Spain. Int J Clin Pract, 59: 62–68 [DOI] [PubMed] [Google Scholar]
- 88. Martin SC, Gagnon DD, Zhang L, Bokemeyer C, Van Marwijk KM, van Hout B (2003) Cost-Utility Analysis of Survival with Epoetin-Alfa versus Placebo in Stage IV Breast Cancer. PharmacoEconomics, 21: 1153–1169 [DOI] [PubMed] [Google Scholar]
- 89. Reed SD, Friedman JY, Velazquez EJ, Gnanasakthy A, Califf RM, Schulman KA (2004) Multinational economic evaluation of valsartan in patients with chronic heart failure: results from the Valsartan Heart Failure Trial (Val-HeFT). Am Heart J 148: 122–128 [DOI] [PubMed] [Google Scholar]
- 90. Welsh RC, Sauriol L, Zhang Z, Kolm P, Weintraub WS, Theroux P (2009) Cost-effectiveness of enoxaparin compared with unfractionated heparin in ST elevation myocardial infarction patients undergoing = pharmacological reperfusion: a Canadian analysis of the Enoxaparin and Thrombolysis Reperfusion for Acute Myocardial Infarction Treatment Thrombolysis in Myocardial Infarction (ExTRACT-TIMI) 25 trial. Can J Cardiol 25: e399–e405 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOCX)
(DOCX)
(DOCX)
(DOCX)
(DOCX)
(DOCX)
(DOCX)
Data Availability Statement
All relevant data are within the paper and its Supporting Information files.