

Abstract
Lipomas are benign soft tissue tumours composed mainly of mature adipose tissue. Histological variants of lipomas have been named according to the type of tissue present and they include fibrolipoma, angiolipoma, osteolipoma, chondrolipoma and others. Osteolipoma, a classic lipoma with osseous metaplasia, is a very rare histological variant. Owing to the rarity of oral osteolipomas, we report an uncommon case of osteolipoma located on the floor of the mouth of a 20-year-old female patient and include a review of the literature.
Background
Lipomas are the most common soft tissue mesenchymal neoplasms and represent about 1–5% of all neoplasms of the oral cavity.1 Lipomas can include components other than fat cells; the most recent classification of benign lipomatous tumours includes classic lipoma and lipoma variants such as angiolipoma, fibrolipoma, chondroid lipoma, myolipoma, osteolipoma and spindle cell/pleomorphic lipoma having specific clinical and histological features.2
Osteolipoma is considered to be the rarest subtype encountered, with the osseous change occurring in longstanding and large lipomas. This rarest variant has been addressed by various names such as osteolipoma, lipoma with osseous metaplasia, ossifying lipoma, osseous lipoma, etc, which are used interchangeably with no specific preference over each other.3
A search of the English literature revealed only 21 cases arising in the oral cavity, which have been described in the tongue, sublingual region, buccal sulcus, buccal mucosa and submandibular region.4–6 We present a rare case of osteolipoma occurring on the floor of the mouth in a 20-year-old female patient.
Case presentation
A 20-year-old female patient reported a 3-year history of a growth and enlargement in the floor of the mouth, which interfered with oral functions. It had gradually grown to the present size. On examination, the submucosal mass was light yellowish, well circumscribed, firm and painless, and measured approximately 6×6 cm (figure 1).
Figure 1.

Clinical photograph showing the swelling in the floor of the mouth.
Investigations
CT scan revealed a well-defined, hypodense lesion (−35 to −65 HU) measuring about 6×6 cm within which irregular hyperdense areas (650–850 HU) were noted to be located in the sublingual space (figure 2). Grossly, the specimen measured approximately 5×5 cm2 and displayed outer adipose tissue, lobulated with a small area that was greyish black, firm and gritty (figure 3A). On sectioning, the excised tissue was firm and gritty extending to the inner aspect forming the core of the lesion (figure 3B).
Figure 2.
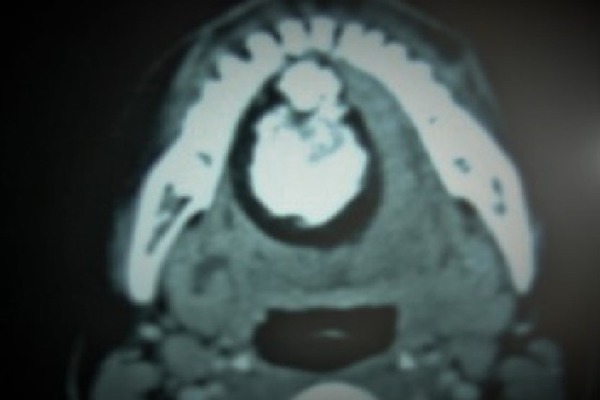
CT scan showing a well-defined hypodense lesion in the sublingual area.
Figure 3.
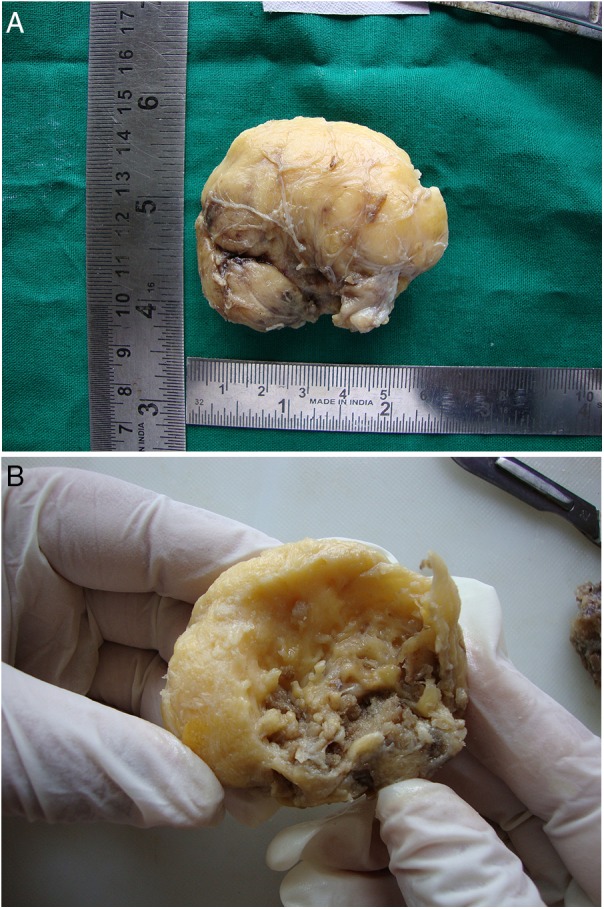
(A) The surgical specimen appearing lobulated, yellowish and soft in consistency, resembling adipose tissue. (B) The cut surface of the specimen showed an irregular round greyish black calcified mass surrounded by yellowish adipose tissue.
Microscopically, the tissue was partly encapsulated and showed a large central area of osseous tissue, characterised by branching and uniting trabeculae of osteoid undergoing varying degrees of mineralisation, and a few mature bony trabeculae with loose fibrocellular and vascular or fatty marrow tissue (figure 4). Lobules of normal mature adipose tissue admixed with areas of bony trabeculae having osteocytes were noted at the periphery (figure 5). The lesion was diagnosed as ‘osteolipoma’.
Figure 4.
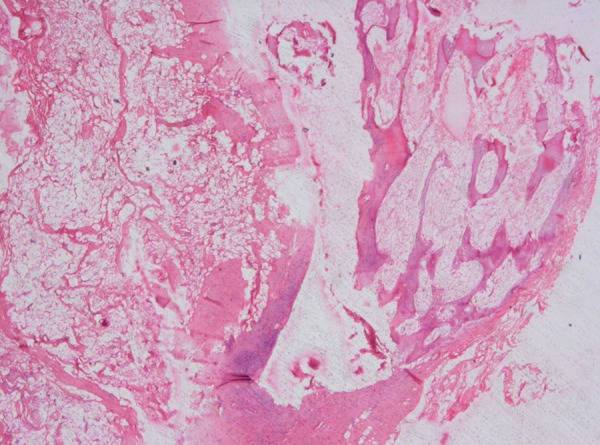
Photomicrograph showing area of trabeculae of osteoid with loose fibrocellular and fatty marrow tissue.
Figure 5.
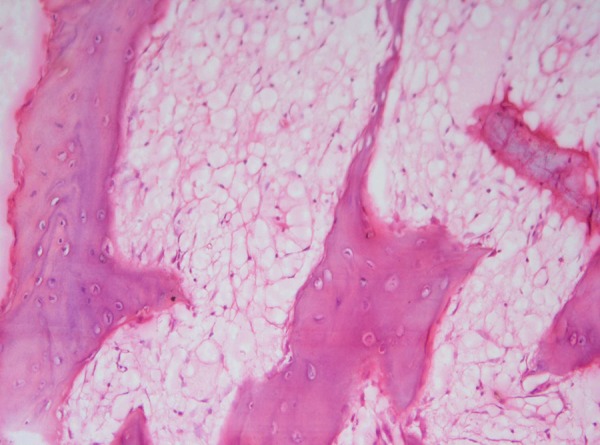
Photomicrograph showing round to oval adipose tissue with bony trabeculae at the periphery.
Treatment
The lesion was completely excised under general anaesthesia and sent for histopathological investigation.
Outcome and follow-up
The patient was kept under follow-up for 1 month; during this period, healing was normal and there was no recurrence or changes during the following year.
Discussion
Lipomas are rare benign soft tissue mesenchymal neoplasms in the oral cavity, representing 1% of all benign oral tumours.7 The first description of an oral lipoma was given by Roux8, who referred to it as a ‘yellow epulis’. The origin of lipomas remains uncertain. Several pathogenic mechanisms such as chronic irritation, trauma, spontaneous development,9 lipoblastic embryonic cell nest origin, metaplasia of muscle cells and fatty degeneration have been proposed.10 11 Variants of lipomas exist that are admixed with other mesoderm-derived tissues, and are designated accordingly (fibrolipoma, angiolipoma, chondrolipoma and osteolipoma).
Osteolipomas are rare variants of lipomas, first described by Plaut and his partners in 1958.5 Various theories have been suggested for the genesis of osteolipoma, and include metaplasia of fibroblasts from within the lipoma, origination of the adipocytes and osseous components from a multipotent stem cell, repetitive external microtrauma and ischaemia secondary to outgrowth of the tumour's blood supply.3 According to Ohno et al,12 the fibrous tissue is the origin of osseous changes in lipomas.
A search of the English literature revealed 21 cases of lipomas with osseous metaplasia occurring in the oral cavity, and head and neck region. As per a recent literature review by Saghafi et al,3 only eight cases of osteolipoma arising in the oral cavity and two pharyngeal cases having some oral manifestations were shown. For lucidity, we performed an English literature search, which revealed a total of 12 cases of osteolipoma only occurring/presenting in the oral cavity since the first case report by Godby et al in 1961.4 6 The details of those cases are presented in table 1.6 13
Table 1.
Details of previously reported cases of osteolipoma in the oral cavity*
| Serial No | Authors | Year | Age | Gender | Site of the lesion | Clinical presentation |
|---|---|---|---|---|---|---|
| 1. | Godby et al | 1961 | 54 | M | Floor of the mouth | – |
| 2. | Hughes | 1966 | 69 | M | Mandibular buccal vestibule | Facial asymmetry |
| 3. | Allard et al | 1982 | 81 | F | Mandibular buccal vestibule | Facial asymmetry |
| 4. | Piattelli et al | 2001 | 49 | F | Tongue | Asymptomatic |
| 5. | Castilho et al | 2004 | 65 | F | Buccal mucosa | Asymptomatic |
| 6. | Durmaz et al | 2007 | 21 | M | Nasopharynx, left soft palate defect | Hypoacousia |
| 7. | Saghaphi et al | 2008 | 68 | M | Mandibular alveolar mucosa | Asymptomatic |
| 8. | Gokul et al | 2009 | 6 | M | Hard palate | Congenital cleft palate |
| 9. | Juliasse et al | 2010 | – | – | Buccal sulcus | – |
| 10. | de Castro et al | 2010 | 47 | F | Buccal mucosa | Facial asymmetry |
| 11. | Adebiyi et al | 2011 | 37 | F | Palate | Asymptomatic |
| 12. | Hsu et al | 2012 | 71 | M | Buccal mucosa | Asymptomatic |
| 13. | Present case | 2015 | 20 | F | Floor of the mouth | Asymptomatic |
Of the 21 cases of osteolipoma in the oral cavity and head and neck, only 12 were reported in the oral tissues. Excluding the present case, the age range of patients was from 6 to 81 years, six were males and five were females, with a mean age of 51.7 years. The male to female ratio was almost equal (54.5% to 45.5%) with a slight increase in males. The majority of the cases were asymptomatic and few showed facial asymmetry. Two cases have been reported without details about the nature of the disease. The present case is the 13th case of osteolipoma, and the second case to be noted in the floor of the mouth.
A wide range of differential diagnoses for osteolipoma may be included and mainly depends on the location of the lesion. Lesions such as teratoma, dermoid cyst, osteoma, ossifying fibroma, myositis ossificans, osteocartilaginous choristoma, metastatic chondrosarcoma or osteosarcoma and liposarcoma with metaplasia are considered.3 9 However, many believe that imaging and biopsy help in the diagnosis, since the usually diffuse fin pattern of mature ossification and bland mature fatty tissue is unique to ossifying lipoma.14 Treatment is complete surgical excision, which shows no recurrences, and prognosis is similar to that of the other lipomas.3 9
Learning points.
Osteolipoma is considered to be the rarest subtype of lipomas, the nature and origin of lipomas remain uncertain.
A literature review showed only 12 cases of intraoral osteolipoma, due to the rarity of this lesion in regard to its clinical behaviour and prognosis; a long-term follow-up is advised.
Even though these are benign in nature, various lesions are considered in the differential diagnosis depending on the anatomical site of the lesion.
Hence we reported this rare case of osteolipoma in a 20-year-old female patient along with a review of the literature.
Footnotes
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Fregnani ER, Pires FR, Falzoni R et al. . Lipomas of the oral cavity: clinical findings, histological classification and proliferative activity of 46 cases. Int J Oral Maxillofac Surg 2003;32:49–53. 10.1054/ijom.2002.0317 [DOI] [PubMed] [Google Scholar]
- 2.Nielsen G, Mandahl N. Adipocytic tumours. In: Fletcher CDM, Unni KK, Mertens F, eds. World Health Organization classification of tumours: pathology & genetics tumours of soft tissue and bone. Lyon: WHO Press, 2002:19–20. [Google Scholar]
- 3.Saghafi S, Mellati E, Sohrabi M et al. . Osteolipoma of the oral and pharyngeal region: report of a case and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:e30–4. 10.1016/j.tripleo.2008.02.018 [DOI] [PubMed] [Google Scholar]
- 4.Castilho RM, Squarize CH, Nunes FD et al. . Osteolipoma: a rare lesion in the oral cavity. Br J Oral Maxillofac Surg 2004;42:363–4. 10.1016/j.bjoms.2004.04.001 [DOI] [PubMed] [Google Scholar]
- 5.de Castro AL, de Castro EV, Felipini RC et al. . Osteolipoma of the buccal mucosa. Med Oral Patol Oral Cir Bucal 2010;15:e347–9. 10.4317/medoral.15.e347 [DOI] [PubMed] [Google Scholar]
- 6.Kavusi S, Farahmand V, Davidson TM et al. . Osteolipoma presenting as a submandibular mass: a rare presentation. Head Neck Pathol 2013;7:93–6. 10.1007/s12105-012-0384-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Manjunatha BS, Pateel GS, Shah V. Oral fibrolipoma-a rare histological entity: report of 3 cases and review of literature. J Dent (Tehran) 2010;7:226–31. [PMC free article] [PubMed] [Google Scholar]
- 8.Roux M. On exostoses: there character. Am J Dent Sci 1848;9:133–4. [PMC free article] [PubMed] [Google Scholar]
- 9.Gokul S, Ranjini KV, Kirankumar K et al. . Congenital osteolipoma associated with cleft palate: a case report. Int J Oral Maxillofac Surg 2009;38:91–3. 10.1016/j.ijom.2008.09.005 [DOI] [PubMed] [Google Scholar]
- 10.Kuyama K, Fifita SF, Komiya M et al. . Rare lipomatous tumors with osseous and/or chondroid differentiation in the oral cavity report of two cases and review of the literature. Int J Dent 2009;2009:143460 10.1155/2009/143460 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Epivatianos A, Markpoulos AK, Papanayotou A. Benign tumors of adipose tissue of the oral cavity: a clinicopathologic study of 13 cases. J Oral Maxillofac Surg 2000;58:1113–17. 10.1053/joms.2000.9568 [DOI] [PubMed] [Google Scholar]
- 12.Ohno Y, Muraoka M, Ohashi Y et al. . Osteolipoma in the parapharyngeal space. Eur Arch Otorhinolaryngol 1998;255:315–17. 10.1007/s004050050067 [DOI] [PubMed] [Google Scholar]
- 13.Hsu HH, Lee LY, Chang KP. Pathology quiz case 2. Osteolipoma of the buccal space. Arch Otolaryngol Head Neck Surg 2012;138:97–8. 10.1001/archoto.2011.219-a [DOI] [PubMed] [Google Scholar]
- 14.Obermann EC, Bele S, Brawanski A et al. . Ossifying lipoma. Virchows Arch 1999;434:181–3. 10.1007/s004280050324 [DOI] [PubMed] [Google Scholar]