

Abstract
Background:
Multiple sclerosis disorders poses heavy physical and emotional effect on patients who are associated with the disease.
Aim:
This study aimed to compare the effectiveness of individual versus group exercises on fatigue on patients with multiple sclerosis.
Materials and Methods:
In this clinical trial, 85 patients with multiple sclerosis were divided in two groups of individualized exercise and team exercise. The intervention was conducted for 6 weeks and comprised of mild stretching and basic yoga exercises twice a day. The data were collected through demographic questionnaire, standard fatigue scale and self-reported checklist. Data analysis was performed by SPSS software.
Results:
The mean levels of fatigue perception after the intervention in group exercise was 27.9 ± 15.9 and 27.1 ± 17.2 in individual exercise. There was no significant difference between the two groups (P > 0.05). Statistically significant difference was observed in the mean level of perceived fatigue in triplicate measurements (P = 0.013) among patients who completed individual exercise. However, this difference was not significant in the group exercise.
Conclusion:
Performing mild stretching exercises and basic yoga are recommended as a cost-effective method which is easy to perform among patients with mild to moderate disabilities.
Keywords: Exercise, Fatigue, Multiple sclerosis, Rehabilitation
Introduction
Multiple sclerosis (MS) is a non-predictable chronic disease of the central nervous system (CNS).[1] Estimated 57 cases out of 100,000 Iranian people presents MS signs during their life time.[2] Fatigue is normal consequence of every chronic illness especially in MS patients due to high rate of limited physical activity and depression.[3] According to recent results, 75-90% of people with MS complained from fatigue and 60% of patients considered it as the most disabling symptom.[4] Fatigue interferes in daily activities, role playing and quality of life (QOL) and cause or worsen other symptoms of MS.[1]
Clinical practice guidelines suggests pharmacological and non-pharmacological (e. g. exercise, energy or fatigue self-management education and cognitive behavioral therapy) management for fatigue.[5] Due to high complications and cost of medicine, the patients are more interested to engage in non-pharmacological management methods[6] such as exercise,[7] relaxation, counselling, rehabilitation and occupational therapy.[8] A recent available research literature summarized about three types of fatigue management interventions in MS patients which are: Exercise, education and medication. After reviewing 25 studies the results showed that rehabilitation interventions appeared to have stronger and more significant effects on reducing the impact or severity of reported fatigue compared to medication. Pharmacological agents, including fatigue medication, are important but often do not enable people with MS to cope with their existing disabilities.[5]
Stretching exercises and yoga are recommended in patients with MS.[9] The benefits of regular exercise in patients with MS include improvements in mood (state of mind) and the ability to perform daily tasks.[10] Several studies and meta-analysis conducted to show the effectiveness of exercises on patients who involved to chronic disease. Although one fundamental consideration pertaining to any protocol aimed at increasing physical activity what remained to be questioned is if group-based activity is more effective or individually-based? For example, a health-care system may offer group-based educational classes or individual counseling for physical activity. Similarly, a worksite may offer an individually targeted internet intervention or regular fitness classes to promote physical activity.[11] Some reviews recommends that group based exercise is more effective for patients[11] while in contrast other suggested individualized exercises.[12]
Thus, considering the increasing number of MS patients, negative effects of fatigue on quality of life of patients, conflicting results regarding the effect of exercise in alleviating of fatigue in patients with MS, and that no indexed studies regarding the difference in effectiveness of individual with group based exercises in these patients have not been found as researcher knowledge, the researcher performed a study which aimed to compare the effectiveness of group and individual exercises on the level of perception of fatigue in patients with MS. The authors hypothesized the exercise significantly will decrease the fatigue level in MS patients and the level of fatigue in group and individualized exercise group will be significantly different.
Materials and Methods
This study is a randomized clinical trial which was performed after obtaining formal permission from the ethical committee of Mashhad University of Medical Sciences whit code of 87694. Also the participants signed consent form before participation in the study.
Sampling
The research population comprised the patients with MS referred to the neurology clinic of Mashhad University during 2013-2014. Inclusion criteria were according diagnosis of MS based on McDonald criteria, the level of disability less than seven using Expanded Disability Status Scale (EDSS),[13] no history of recurrence in the last month, and lack of physical and psychological trauma in the recent 6 months. Only relapsing-recovery and secondary progressive MS patients included. Eighty five cases selected through purposive sampling method according inclusion and exclusion criteria and were administered in two groups randomly (through check list) that is 41 cases in individual exercise group and 44 patients in team exercise group. Totally 28 cases lost during study (eight cases due to irregular exercise, three patients due to disease recurrence and 17 cases decline to participate in the study). The final analysis sample were comprised 28 cases in individual exercise group and 29 in team exercise group.
Exercise
The exercise performed twice a day 10-15 minutes for 6 weeks. In the first session fundamental information and objectives presented for all participants and patients in both groups were trained in term of performing exercises.
During next sessions a video CD was displayed step by step (mild stretching intervention). The patients trained with experienced coach. A booklet with full details of the exercise was prepared by the researcher. The prepared VCD and booklet provided for individualized group. The group based exercise program followed by phone contact twice a week by researcher. Group based exercise performed the exercises at the gym and VCD with booklet provided for group based exercise in the end of each sessions also.
Tools for measurement
The fatigue level of patients was evaluated in both groups at three time frame before, 3 and 6 weeks after the intervention. Data collection tools in this study consisted three parts as following:
Demographic and disease-related information.
Modified Fatigue Impact Scale (MFIS), which was originally developed to assess the effects of fatigue on quality of life of patients with chronic diseases specifically MS. The total score of the MFIS ranges from 0-84. The ranges of scores for each subscale are as follows: physical, 0-36; cognitive, 0-40; and psychosocial, 0-8.[14] The reliability of MFIS has been confirmed in Mashhad Nursing and Midwifery faculty using the test-retest method with a coefficient of 0.812, and to determine the internal relationship between the answers the Cronbach alpha had coefficient of 0.91.[15]
Severity of disability was measured using the EDSS tools.[13]
Validity of demographic questionnaire, checklist and Modified Fatigue Impact questionnaire was confirmed by content validity.
Statistics
Data were analyzed with SPSS software using independent t-test, Mann-Whitney, ANOVA with repeated measurements, chi-square.
Chi-square used to test the difference of level of fatigue before intervention. Independent t-test used to compare group and individualized exercise in term of fatigue in third week and sixth week. ANOVA and man Whitney used to compare difference of fatigue levels in three assessment time intergroup and between groups.
Results
Descriptive results
The mean age of subjects was 32.2 ± 8.4 years, and 61.4% of subjects pertaining age group of 25-40 years. 93% of subjects were female, 4.47% were married, and 8.8% were divorced. Regarding education, 47.4% of subjects hold diploma, 12% were illiterate and rest were literate up to high school. 61.4% of patients had a monthly income between 80-150 US dollar and rest reported income higher than 150 US dollar.
Mean interval from the onset of symptoms to diagnosis of MS was 13.5 ± 28.6 months. 31.6% of subjects used Betaferon, 21.1% Rebif, 17.5% synovex, 8.8% anovex, 8.8% Recigen and 12.3% didn′t use moderator drugs.
The first symptom of MS in 38.6% of subjects comprised visual defect. 38.6% of patients reported fatigue as the most debilitating problem. 56.1% of subjects had no history of recurrence during one recent year and number of recurrence in 38.9% of patients were one or two times.
Comparative results
Figure 1.
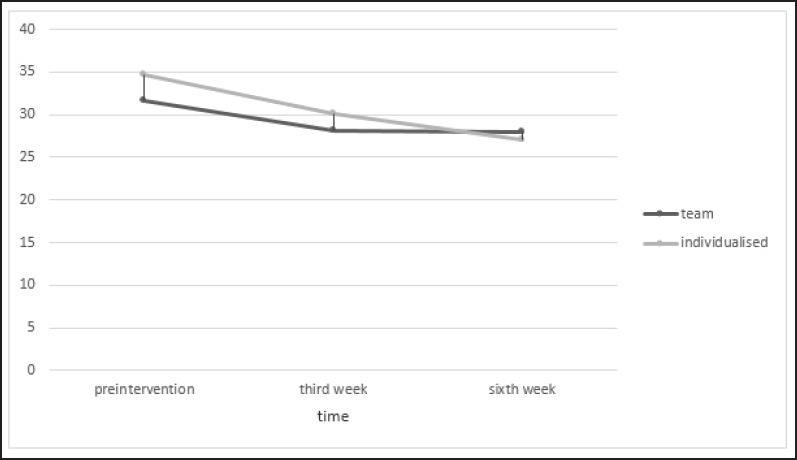
Mean scores of perceived fatigue before intervention, three weeks, and six weeks after the intervention in two groups of group based exercises and individual exercises
The mean of perceived fatigue in the group exercise was decreased 3 weeks after the intervention 11.3% and 6 weeks after the intervention 21%. In the individual exercise the mean score of fatigue was 13.2% three weeks after the intervention and it was 21.9% 6 weeks after the intervention.
According to the results of the independent t-test, there was no statistically significant difference before intervention between two groups and individual exercises before intervention (P = 0.554). Also the mean of perceived fatigue was not significantly different after 3 weeks (P = 0.669) and 6 weeks (P = 0.858) after intervention between two groups. Difference of fatigue level was not significant in subscales that is, physical, cognitive and psychosocial dimensions after the intervention in two groups (P = 0.675, P = 0.761, P = 0.877) respectively.
The results of ANOVA indicated that the scores of perceived fatigue before the intervention and after intervention was significant (P = 0.013). The mean perceived fatigue before intervention with after sixth week was statistically significant (P = 0.024). While the difference was not significant when comparing pre-intervention with third week (P = 0.053) and third week with sixth week (P = 0.759).
In individualized group the mean perceived fatigue in the physical and cognitive subscales in the group of individual exercises in all three times of assessment were significantly different (P = 0.011, P = 0.017 respectively), but the mean perceived fatigue in the psychosocial level at three times of assessment was not statistically significantly different (P = 0.131).
In group based exercise the mean perceived fatigue in at three time measurements was not significantly different (P = 0.160). The mean perceived fatigue in physical, cognitive and psychosocial levels at three measurements was not significantly different (P = 0.160, P = 0.584, P = 0.533, respectively) also.
Discussion
The results showed two groups were similar term of mean perceived fatigue before intervention. Therefore difference in fatigue after the intervention may be related to the effect of mild stretching exercises and basic yoga exercises in both group and individual exercises.
The results of present study showed that the mean perceived fatigue was decreased in compare to pre-intervention in the group exercise 11.35% in third week, and sixth week 11.98%, respectively, but, this difference was not statistically significant (P = 0.160).
In individual exercise group the fatigue level was decreased 13.2% at third week and 21.9% at sixth weeks after the intervention. In the study conducted with Plow et al., (2009) comparing two individual rehabilitation and group health (seven training sessions) to promote physical activity and health in 50 patients with MS. The results showed no significant difference between the two groups in terms of QOL, perceived fatigue, mental health and physical assessment. But fatigue, resting heart rate and physical activity were improved in both groups[16] which is in harmony with our results, although the type of intervention was different in both groups. In findings of Veliconja and colleagues revealed that yoga was not effective on fatigue.[7] Although this difference is explainable with different sample size and sessions in two study.
Freeman and Allison (2004) delivered 10 weeks exercise program with a counseling session at the end of each exercise session and their findings indicated that the mean perceived fatigue was decreased as 21.6%.[17] In their study the percentage of decrease in perceived fatigue was reported higher than the present study. This difference can be due to small sample size of their study (10 patients) also the patients received longer exercise sessions plus counselling in the end of each session.
The study of Rasova et al., (2006) showed that after two months of intervention, one hour twice a week, perceived fatigue was in the aerobic exercise group 11.10% (P < 0.05) and in the combination group of neurophysiological and aerobic exercise 8.67% (P < 0.05). They believed that the reason of difference between the four groups is related to the disability levels.[18] In the present study a decrease of about 12% in perception of fatigue was observed which is in consistent with the study of Razova et al., in the aerobic exercise group.
Kargarfard and colleagues[19] showed that 8 weeks of exercise in water, three times a week significantly decreased perceived fatigue of patients significantly (P = 0.002). These differences may be is related to the nature of exercises (exercise in water), the frequency and duration of exercise in a week and used different tools to measure the fatigue.
Mean perceived fatigue had statistically significant difference in individual exercise group at the third and sixth weeks after the intervention (P = 0.013), although there was no significant difference in the group exercise (P = 0.160). This result may explainable with considering the mean number of exercise sessions in individual group (10.6 ± 1.5) which was more than group exercise (9.5 ± 1.3), and according to self-report checklist, more subjects in individual exercise group (57.14%) regularly performed 12 sessions of exercises while in the group exercise only 34.48% were regular.
As a result, increasing self-efficacy and activity of patients leads to further decrease of fatigue perception in individual exercise group. This result is similar to the reported results in review conducted with Atienza,[12] While it is in contrast with Shauna et al.’s findings.[11] In this study, the group exercise had to join to each session at certain time and in a certain sport gym which can be one of the reasons for the high rate of drop and the lack of significances in the effect of exercise on fatigue perception. The participants of individual exercise group was not involved with this kind of limitations and they could perform the exercise at home whenever they can.
Another reason could be due to the nature of MS symptoms. In this study, the samples were vary about the levels of MS and also both types of recurrence included. Due to the nature of the disease, being in a group and observing the problems of people during exercise, creates a negative impact on the morale of the patients.
The nature of exercises in this study was mild stretching and preliminary yoga, the exercises were safe for all levels of disability in these patients and caused satisfied feeling in the patients after exercise. The results also indicated a positive effect of the nature of this type of exercise in MS patients and despite of the negative consequences of being in a group the effect of exercise was significant in group exercise also.
In summary, according to the obtained results, the period of 6-weeks exercises is the minimum required time and longer time expected to show more significant results. Based on our findings, stretching exercises and selected preliminary yoga is a beneficial method to reduce fatigue in MS patients. Despite the perception of fatigue in both groups showed a significant decreases in fatigue of patients in compare to pre-intervention, this difference was not significant in team exercise group. Further studies needs to be performed among patients with MS considering the level of disability progression and separate exercise classes should be hold for each group.
Holding the group exercise sessions in different times give them to choose sessions according daily program. So that the patients attend for exercise when they are willing. Also, the long term effect of these interventions can be assessed by a follow-up program. Considering the effect of these exercises in reducing fatigue, survey on effectiveness of exercise on other signs of MS recommended.
This study involved with some limitations such as lack of control on physical activities of the subjects, selecting the samples with different level of disability, factors influencing on fatigue such as mental-psychological status, nutrition, etc.
Acknowledgement
This study is result of a research thesis submitted to Mashhad University of Medical Sciences whit code of 87694. We appreciate the Deputy of Research of Mashhad University of Medical Sciences for their financial support, the faculty of Mashhad Midwifery and Nursing school, and all patients who participated in this study.
Footnotes
Source of Support: Nil.
Conflict of Interest: This study supported financially by Deputy of Research of Mashhad University of Medical Sciences.
References
- 1.Matuska K, Mathiowetz V, Finlayson M. Use and perceived effectiveness of energy conservation strategies for managing multiple sclerosis fatigue. Am J Occup Ther. 2007;61:62–9. doi: 10.5014/ajot.61.1.62. [DOI] [PubMed] [Google Scholar]
- 2.Abediani M, Habibi Saravi R, Zarvani A, Farahmand M. Epidemiology of multiple sclerosis in the Mazandaran province in 2006. J Mazandaran Univ Med Sci. 2007;18:82–7. [Google Scholar]
- 3.Taylor KL, Hadgkiss EJ, Jelinek GA, Weiland TJ, Pereira NG, Marck CH, et al. Lifestyle factors, demographics and medications associated with depression risk in an international sample of people with multiple sclerosis. BMC Psychiatry. 2014;14:327. doi: 10.1186/s12888-014-0327-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Plow M, Finlayson M, Motl RW, Bethoux F. Randomized controlled trial of a teleconference fatigue management plus physical activity intervention in adults with multiple sclerosis: Rationale and research protocol. BMC Neurol. 2012;12:122. doi: 10.1186/1471-2377-12-122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Asano M, Finlayson ML. Meta-analysis of three different types of fatigue management interventions for people with multiple sclerosis: Exercise, education, and medication. Mult Scler Int. 2014;2014:798285. doi: 10.1155/2014/798285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Neill J, Belan I, Ried K. Effectiveness of non-pharmacological interventions for fatigue in adults with multiple sclerosis, rheumatoid arthritis, or systemic lupus erythematosus: A systematic review. J Adv Nurs. 2006;56:617–35. doi: 10.1111/j.1365-2648.2006.04054.x. [DOI] [PubMed] [Google Scholar]
- 7.Velikonja O, Curic’ K, Ozura A, Jazbec SS. Influence of sports climbing and yoga on spasticity, cognitive function mood and fatigue in patients with multiple sclerosis. Clin Neurol Neurosurg. 2010;112:597–601. doi: 10.1016/j.clineuro.2010.03.006. [DOI] [PubMed] [Google Scholar]
- 8.Ghaffari S, Ahmadi F, Nabavi M, Memarian R, Kazemnejad A. Technique of progressive muscle relaxation on fatigue investigation in patients with multiple sclerosis. JSKUMS. 2007;10:61–8. [Google Scholar]
- 9.Jafarian N, Sadeghi A. Multiple sclerosis and care. In: Jafarian M, editor. Vol. 1. Jame-e-Negar, Tehran: Salemi Publication; 2005. [Google Scholar]
- 10.White LJ, McCoy SC, Castellano V, Gutierrez G, Stevens JE, Walter GA, et al. Resistance training improves strength and functional capacity in persons with multiple sclerosis. Mult Scler. 2004;10:668–74. doi: 10.1191/1352458504ms1088oa. [DOI] [PubMed] [Google Scholar]
- 11.Burke SM, Carron AV, Eys MA, Ntoumanis N, Estabrooks PA. Group versus individual approach? A meta-analysis of the effectiveness of interventions to promote physical activity. Sport Exerc Psy Rev. 2006;2:2–39. [Google Scholar]
- 12.Atienza AA. Home-based physical activity programs for middle-aged and older adults: Summary of empirical research. J Aging Phys Activity. 2001:38–58. [Google Scholar]
- 13.Kurtzke JF. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS) Neurology. 1983;33:1444–52. doi: 10.1212/wnl.33.11.1444. [DOI] [PubMed] [Google Scholar]
- 14.Larson RD. Psychometric properties of the modified fatigue impact scale. Int J MS Care. 2013;15:15–20. doi: 10.7224/1537-2073.2012-019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Motle RW, Arnett PA, Smith MM, Barwick FH, Ahlstrom B, Stover EJ. Worsening of symptoms is associated with lower physical activity level in individuals with multiple sclerosis. Mult Scler. 2008;14:140–2. doi: 10.1177/1352458507079126. [DOI] [PubMed] [Google Scholar]
- 16.Plow MA, Mathiowetz V, Lowe DA. Comparing individualized rehabilitation to a group wellness intervention for persons with multiple sclerosis. Am J Health promot. 2009;24:23–6. doi: 10.4278/ajhp.071211128. [DOI] [PubMed] [Google Scholar]
- 17.Freeman J, Allison R. Group exercise classes in people with multiple sclerosis: A pilot study. Physiother Res Int. 2004;9:104–7. doi: 10.1002/pri.307. [DOI] [PubMed] [Google Scholar]
- 18.Rasova K, Havrdova E, Brandejsky P, Zalisova M, Foubikova B, Martinkova P. Comparison of the influence of different rehabilitation programmes on clinical, spirometric and spiroergometric parameters in patients with multiple sclerosis. Mult Scler. 2006;12:227–34. doi: 10.1191/135248506ms1248oa. [DOI] [PubMed] [Google Scholar]
- 19.Kargarfard M, Etemadifar M, Baker P, Mehrabi M, Hayatbakhsh R. Effect of aquatic exercise training on fatigue and health-related quality of life in patients with multiple sclerosis. Arch Phys Med Rehabil. 2012;93:1701–8. doi: 10.1016/j.apmr.2012.05.006. [DOI] [PubMed] [Google Scholar]